
Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
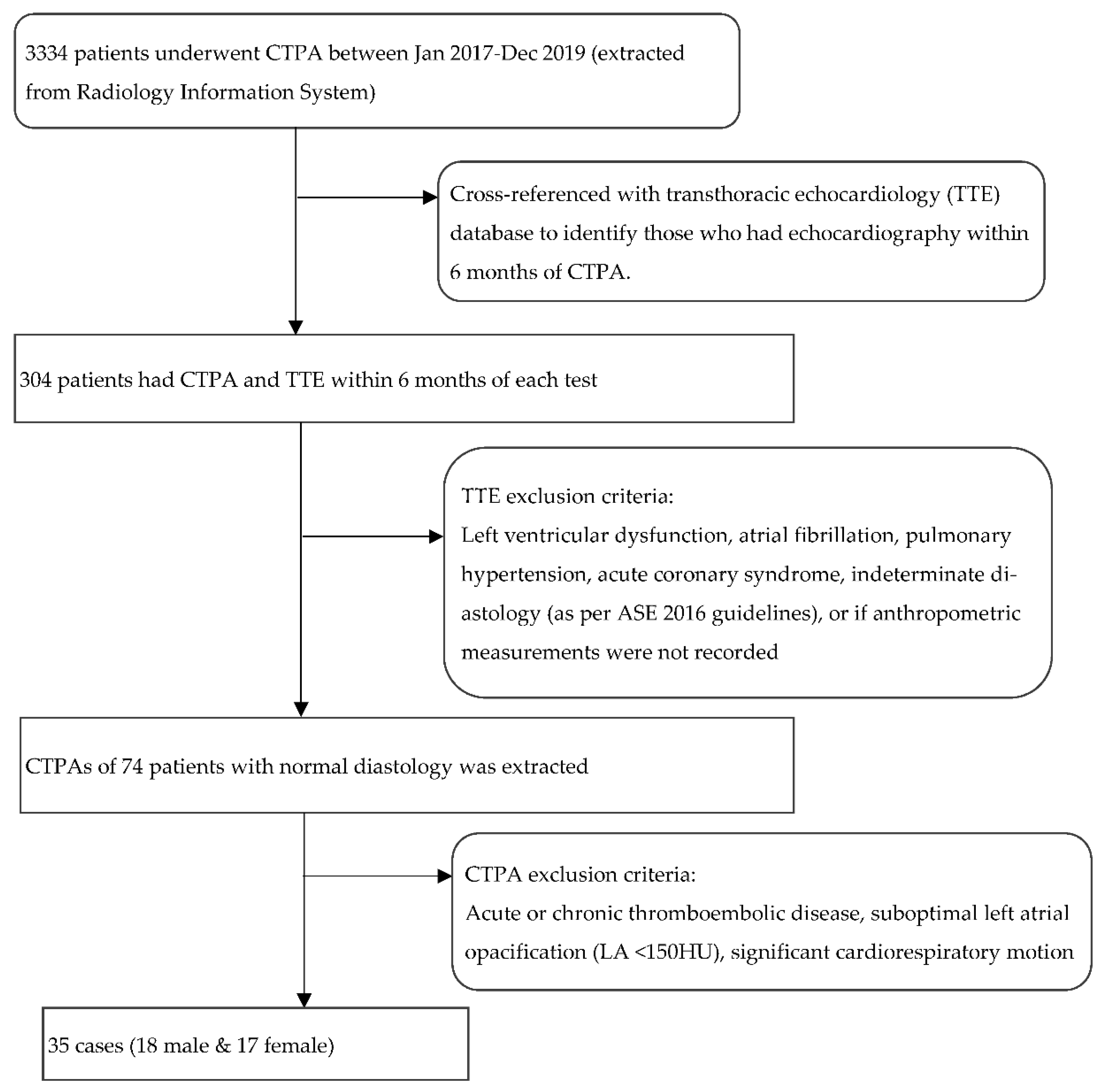
2.1. Patient Population
2.2. CT Acquisition
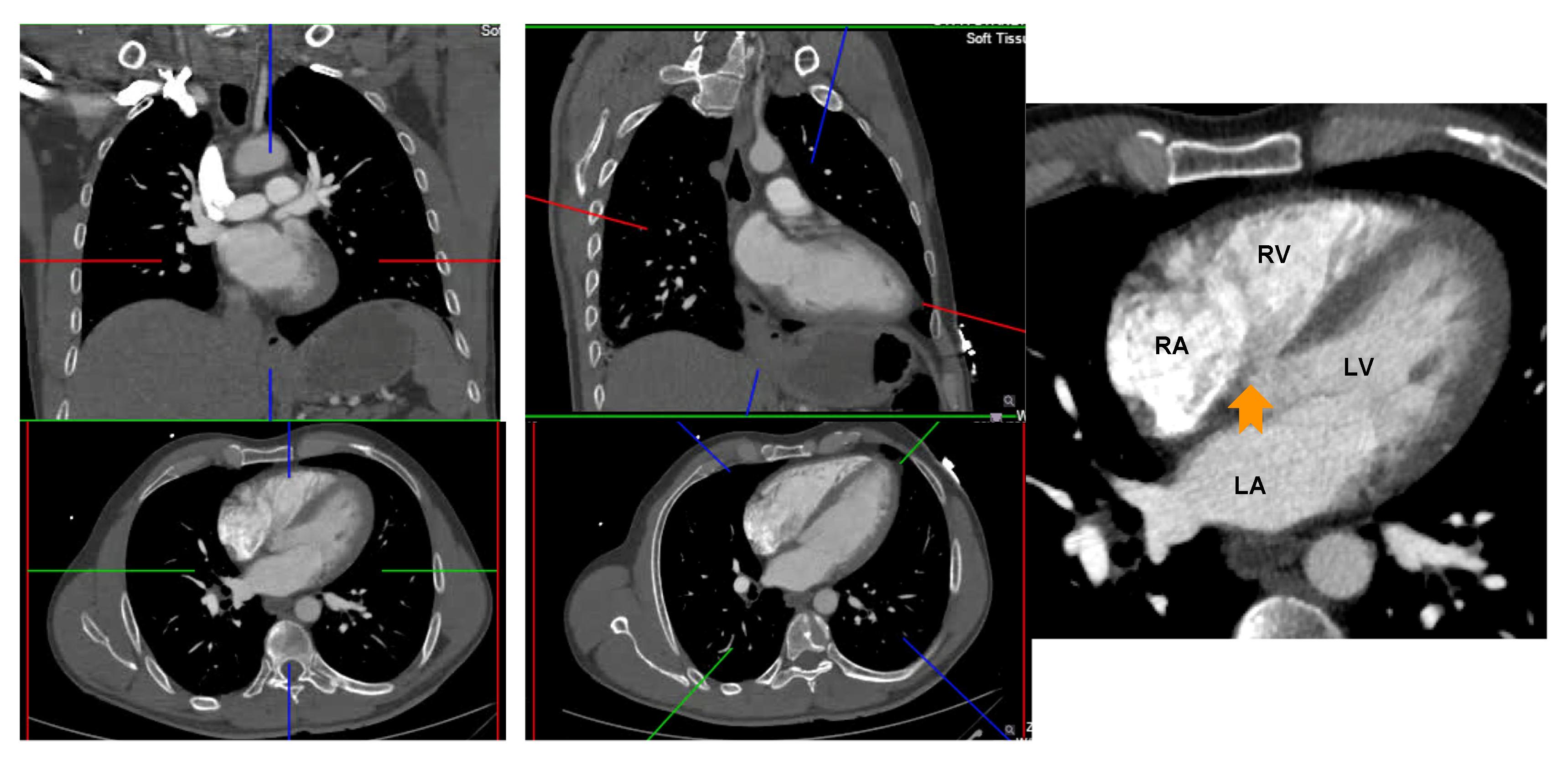
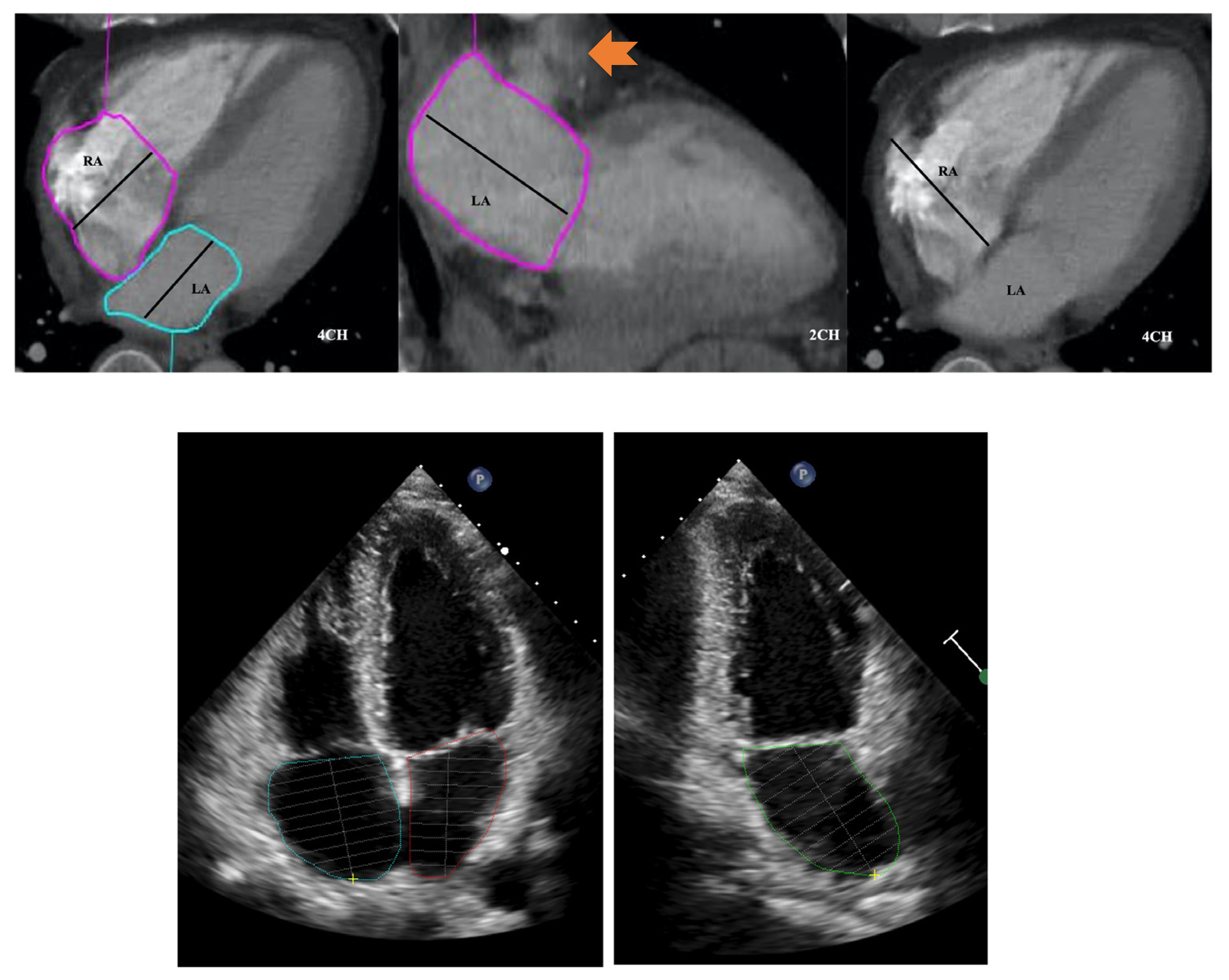
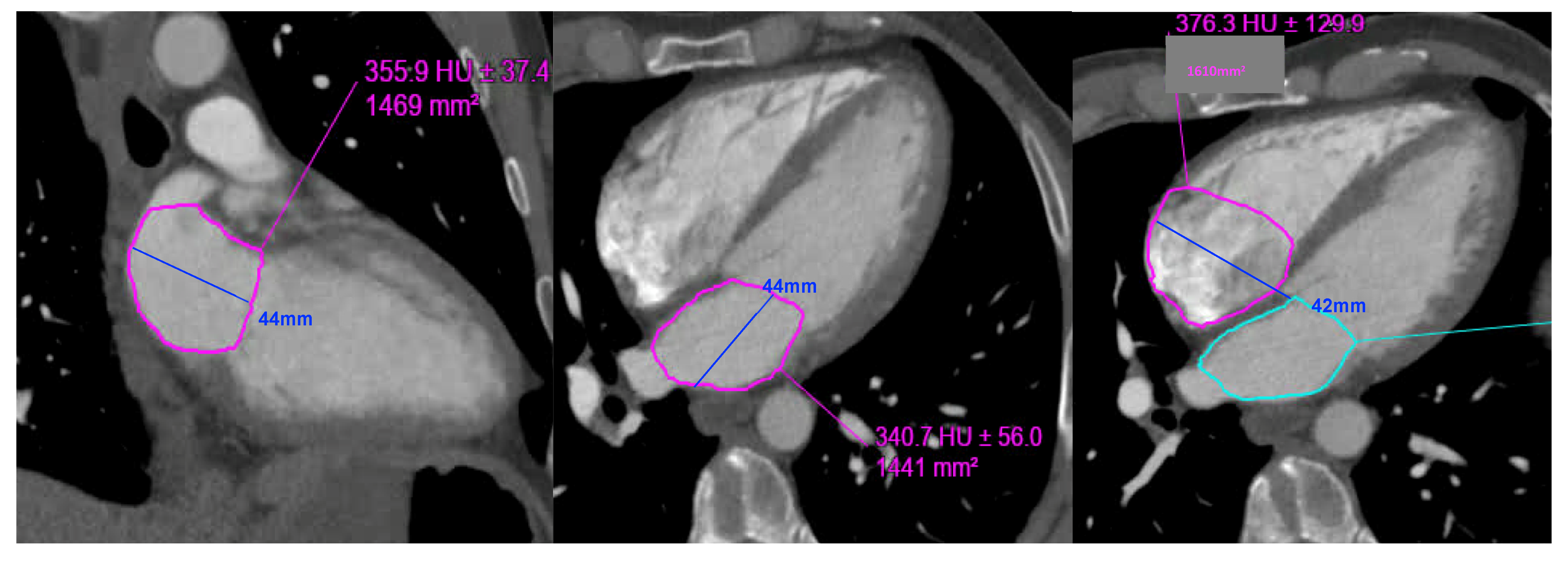
2.3. CT Biatrial Measurement
| Left atrial volume: (0.85 × area 1 (2 chamber) × area 2 (4 chamber)) ÷ shortest LA long axis length: |
| 0.85 × 14.7 × 14.4 ÷ 4.4 = 40.8 mL. LAVi = 21.4 mL/m2 |
| Right atrial volume: (0.85 × (RA 4 chamber area)2) ÷ RA long axis length: |
| 0.85 × (16.1) 2) ÷ 4.2 = 52.45 mL. RAVi: 27.6 mL/m2 |
2.4. Statistical Analysis
3. Results
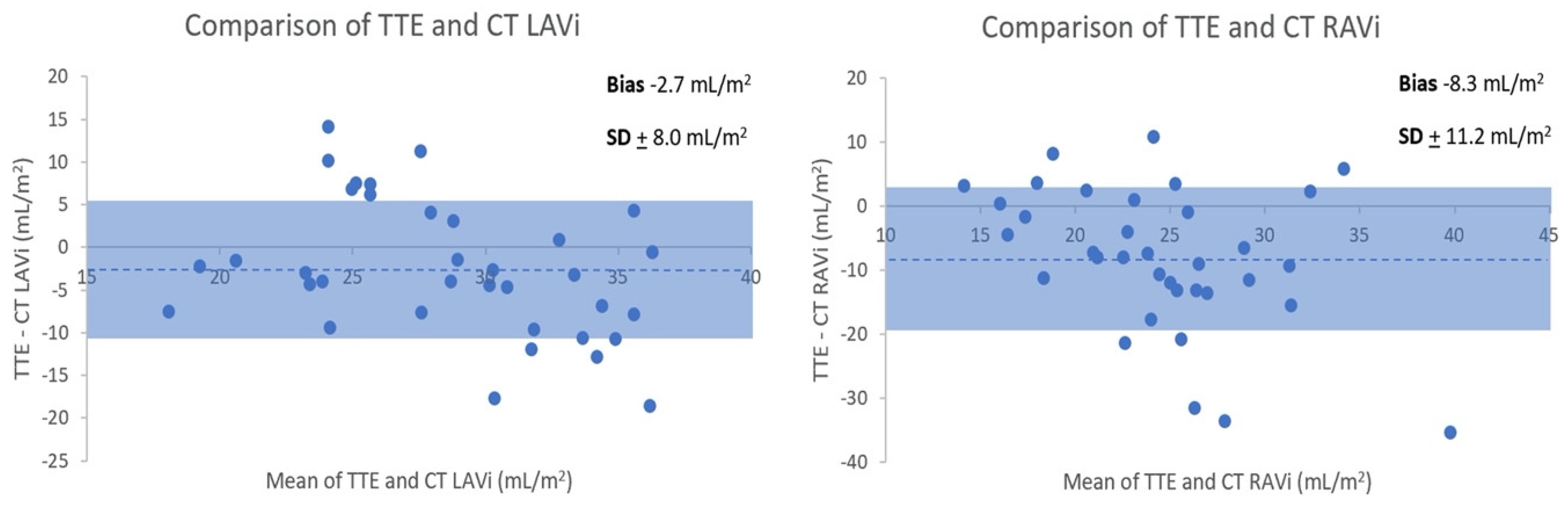
3.1. TTE versus CT Biatrial Volumes
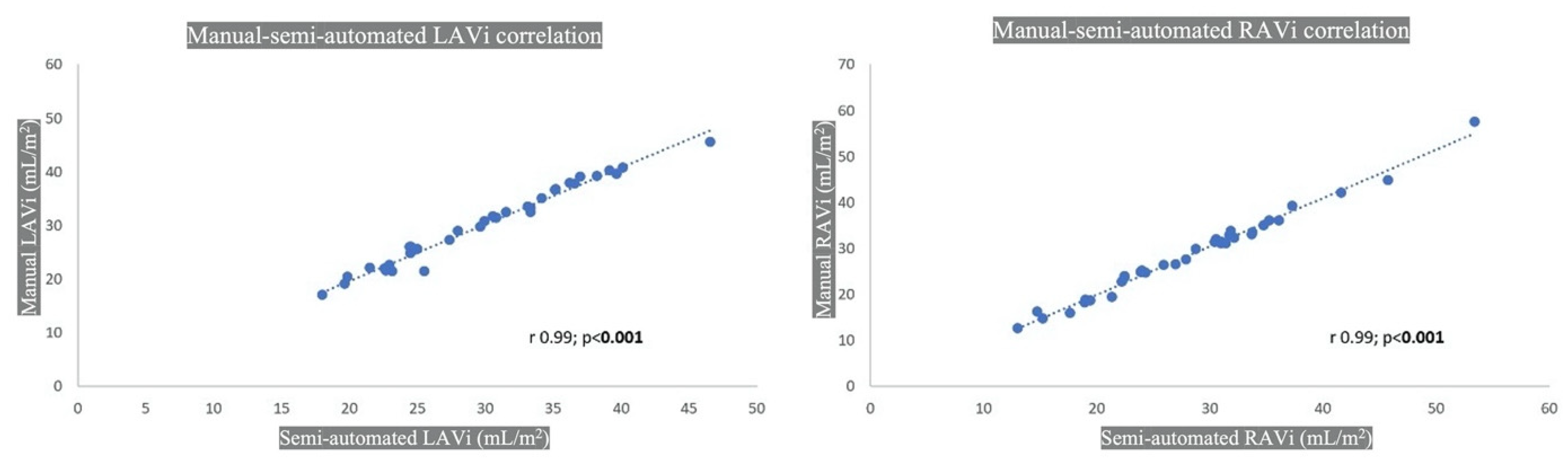
3.2. Manual versus Semiautomated CT Biatrial Volumes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoit, B.D. Left Atrial Size and Function. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Lerchbaumer, M.H.; Ebner, M.; Ritter, C.O.; Steimke, L.; Rogge, N.I.; Sentler, C.; Thielmann, A.; Hobohm, L.; Keller, K.; Lotz, J.; et al. Prognostic value of right atrial dilation in patients with pulmonary embolism. ERJ Open Res. 2021, 7, 00414–02020. [Google Scholar] [CrossRef] [PubMed]
- Alenezi, F.; Mandawat, A.; Il’giovine, Z.J.; Shaw, L.K.; Siddiqui, I.; Tapson, V.F.; Arges, K.; Rivera, D.; Romano, M.M.; Velazquez, E.J.; et al. Clinical Utility and Prognostic Value of Right Atrial Function in Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2018, 11, e006984. [Google Scholar] [CrossRef]
- Hundley, W.G.; Bluemke, D.A.; Finn, J.P.; Flamm, S.D.; Fogel, M.A.; Friedrich, M.G.; Ho, V.B.; Jerosch-Herold, M.; Kramer, C.M.; Manning, W.J.; et al. ACCF/ACR/AHA/NASCI/SCMR 2010 Expert Consensus Document on Cardiovascular Magnetic Resonance: A Report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J. Am. Coll. Cardiol. 2010, 55, 2614–2662. [Google Scholar] [CrossRef]
- Stojanovska, J.; Cronin, P.; Patel, S.; Gross, B.H.; Oral, H.; Chughtai, K.; Kazerooni, E.A. Reference Normal Absolute and Indexed Values From ECG-Gated MDCT: Left Atrial Volume, Function, and Diameter. Am. J. Roentgenol. 2011, 197, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Budoff, M.J.; Pagali, S.R.; Hamirani, Y.S.; Chen, A.; Cheu, G.; Gao, Y.; Li, D.; Mao, S. Sex-Specific Biatrial Volumetric Measurements Obtained with Use of Multidetector Computed Tomography in Subjects with and without Coronary Artery Disease. Tex. Heart Inst. J. 2014, 41, 286–292. [Google Scholar] [CrossRef]
- Lin, F.Y.; Devereux, R.B.; Roman, M.J.; Meng, J.; Jow, V.M.; Jacobs, A.; Weinsaft, J.W.; Shaw, L.J.; Berman, D.S.; Callister, T.Q.; et al. Cardiac Chamber Volumes, Function, and Mass as Determined by 64-Multidetector Row Computed Tomography: Mean Values Among Healthy Adults Free of Hypertension and Obesity. JACC Cardiovasc. Imaging 2008, 1, 782–786. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Turchetta, S.; Zonzin, P.; Zuliani, G.; Roncon, L. Left atrial size measured on CT pulmonary angiography: Another parameter of pulmonary embolism severity? A systematic review. J. Thromb. Thrombolysis 2020, 50, 181–189. [Google Scholar] [CrossRef]
- Guo, Z.-J.; Liu, H.-T.; Bai, Z.-M.; Lin, Q.; Zhao, B.-H.; Xu, Q.; Zeng, Y.-H.; Feng, W.-Q.; Zhou, H.-T.; Liang, F.; et al. A new method of CT for the cardiac measurement: Correlation of computed tomography measured cardiac parameters and pulmonary obstruction index to assess cardiac morphological changes in acute pulmonary embolism patients. J. Thromb. Thrombolysis 2018, 45, 410–416. [Google Scholar] [CrossRef]
- Aviram, G.; Soikher, E.; Bendet, A.; Ziv-Baran, T.; Berliner, S.; Shmueli, H.; Friedensohn, L.; Milwidsky, A.; Sadovnik, O.; Topilsky, Y. Automatic assessment of cardiac load due to acute pulmonary embolism: Saddle vs. central and peripheral emboli distribution. Heart Lung 2016, 45, 261–269. [Google Scholar] [CrossRef]
- Aviram, G.; Soikher, E.; Bendet, A.; Shmueli, H.; Ziv-Baran, T.; Amitai, Y.; Friedensohn, L.; Berliner, S.; Meilik, A.; Topilsky, Y. Prediction of Mortality in Pulmonary Embolism Based on Left Atrial Volume Measured on CT Pulmonary Angiography. Chest 2016, 149, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Aviram, G.; Sirota-Cohen, C.; Steinvil, A.; Keren, G.; Banai, S.; Sosna, J.; Berliner, S.; Rogowski, O. Automated volumetric analysis of four cardiac chambers in pulmonary embolism. Thromb. Haemost. 2012, 108, 384–393. [Google Scholar] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef] [PubMed]
- Russo, C.; Hahn, R.T.; Jin, Z.; Homma, S.; Sacco, R.L.; Di Tullio, M.R. Comparison of Echocardiographic Single-Plane versus Biplane Method in the Assessment of Left Atrial Volume and Validation by Real Time Three-Dimensional Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 954–960. [Google Scholar] [CrossRef]
- DePace, N.L.; Ren, J.-F.; Kotler, M.N.; Mintz, G.S.; Kimbiris, D.; Kalman, P. Two-dimensional echocardiographic determination of right atrial emptying volume: A noninvasive index in quantifying the degree of tricuspid regurgitation. Am. J. Cardiol. 1983, 52, 525–529. [Google Scholar] [CrossRef]
- Koka, A.R.; Yau, J.; Van Why, C.; Cohen, I.S.; Halpern, E.J. Underestimation of Left Atrial Size Measured with Transthoracic Echocardiography Compared With 3D MDCT. Am. J. Roentgenol. 2010, 194, W375–W381. [Google Scholar] [CrossRef] [PubMed]
- Koka, A.R.; Gould, S.D.; Owen, A.N.; Halpern, E.J. Left Atrial Volume: Comparison of 2D and 3D Transthoracic Echocardiography with ECG-gated CT Angiography. Acad. Radiol. 2012, 19, 62–68. [Google Scholar] [CrossRef]
- Kataoka, A.; Funabashi, N.; Takahashi, A.; Yajima, R.; Takahashi, M.; Uehara, M.; Takaoka, H.; Saito, M.; Yamaguchi, C.; Lee, K.; et al. Quantitative evaluation of left atrial volumes and ejection fraction by 320-slice computed-tomography in comparison with three- and two-dimensional echocardiography: A single-center retrospective-study in 22 subjects. Int. J. Cardiol. 2011, 153, 47–54. [Google Scholar] [CrossRef]
- Liu, X.-K.; Jahangir, A.; Terzic, A.; Gersh, B.J.; Hammill, S.C.; Shen, W.-K. Age- and sex-related atrial electrophysiologic and structural changes. Am. J. Cardiol. 2004, 94, 373–375. [Google Scholar] [CrossRef]
- Pan, N.-H.; Tsao, H.-M.; Chang, N.-C.; Chen, Y.-J.; Chen, S.-A. Aging Dilates Atrium and Pulmonary Veins. Chest 2008, 133, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Pritchett, A.M.; Jacobsen, S.J.; Mahoney, D.W.; Rodeheffer, R.J.; Bailey, K.R.; Redfield, M.M. Left atrial volume as an index ofleft atrial size: A population-based study. J. Am. Coll. Cardiol. 2003, 41, 1036–1043. [Google Scholar] [CrossRef]
- Damman, K.; Testani, J.M. The kidney in heart failure: An update. Eur. Heart J. 2015, 36, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Lick, A.N.; Danrad, R.; Smith, D.L.; Lammi, M.R. Left Atrium Measurements via Computed Tomography Pulmonary Angiogram as a Predictor of Diastolic Dysfunction. J. Comput. Assist. Tomogr. 2017, 41, 792–797. [Google Scholar] [CrossRef]
- Lester, S.J.; Ryan, E.W.; Schiller, N.B.; Foster, E. Best method in clinical practice and in research studies to determine left atrial size. Am. J. Cardiol. 1999, 84, 829–832. [Google Scholar] [CrossRef]
- Takemoto, Y.; Barnes, M.E.; Seward, J.B.; Lester, S.J.; Appleton, C.A.; Gersh, B.J.; Bailey, K.R.; Tsang, T.S. Usefulness of Left Atrial Volume in Predicting First Congestive Heart Failure in Patients ≥65 Years of Age with Well-Preserved Left Ventricular Systolic Function. Am. J. Cardiol. 2005, 96, 832–836. [Google Scholar] [CrossRef]
- Tsang, T.S.; Abhayaratna, W.P.; Barnes, M.E.; Miyasaka, Y.; Gersh, B.J.; Bailey, K.R.; Cha, S.S.; Seward, J.B. Prediction of Cardiovascular Outcomes with Left Atrial Size: Is Volume Superior to Area or Diameter? J. Am. Coll. Cardiol. 2006, 47, 1018–1023. [Google Scholar] [CrossRef]
- Tardivon, A.A.; Musset, D.; Maitre, S.; Brenot, F.; Dartevelle, P.; Simonneau, G.; Labrune, M. Role of CT in Chronic Pulmonary Embolism: Comparison with Pulmonary Angiography. J. Comput. Assist. Tomogr. 1993, 17, 345–351. [Google Scholar] [CrossRef]
- Rheinheimer, S.; Reh, C.; Figiel, J.; Mahnken, A.H. Assessment of right atrium volume by conventional CT or MR techniques: Which modality resembles in vivo reality? Eur. J. Radiol. 2016, 85, 1040–1044. [Google Scholar] [CrossRef]
- Takahashi, A.; Funabashi, N.; Kataoka, A.; Yajima, R.; Takahashi, M.; Uehara, M.; Takaoka, H.; Saito, M.; Yamaguchi, C.; Lee, K.; et al. Quantitative evaluation of right atrial volume and right atrial emptying fraction by 320-slice computed tomography compared with three-dimensional echocardiography. Int. J. Cardiol. 2011, 146, 96–99. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal Diastology (n = 35) | |
|---|---|
| Age (years) | 45 (34–55) |
| Gender | 18 M (51%), 17 F (49%) |
| BMI | 27.0 (23.5–32.0) |
| BSA | 1.95 ± 0.25 |
| CTPA-TTE time interval (days) | 44 (11–113) |
| Normal Diastology Cohort (n = 35) | |
|---|---|
| Simpson’s biplane LVEF (%) | 61 ± 4 |
| Transmitral E (cm/s) | 84 (63–96) |
| Transmitral A (cm/s) | 65 (53–73) |
| E/A | 1.29 ± 0.24 |
| Medial mitral e’ (cm/s) | 11 (9–12) |
| Lateral mitral e’ (cm/s) | 14 (12–15) |
| E/medial e’ | 7.9 ± 2.0 |
| E/lateral e’ | 5.9 ± 1.4 |
| TR Vmax (m/s) (n = 15) | 2.3 ± 0.2 |
| CT Atrial Measurements (Manual) | TTE Atrial Measurements | |
|---|---|---|
| 4Ch LA area (cm2) | 18.1 ± 4.1 | 18.3 ± 3.4 |
| 2Ch LA area (cm2) | 17.0 ± 4.2 | 16.7 ± 3.8 |
| LAVi (mL/m2) | 30 ± 8 | 27 ± 5 |
| 4Ch RA area (cm2) | 17.0 ± 4.1 | 15.1 ± 3.2 |
| RAVi (mL/m2) | 29 ± 9 | 20 ± 6 |
| 4Ch RA:LA area ratio | 0.91 (0.82–1.06) | 0.84 ± 0.14 |
| RA:LA volume ratio | 0.88 (0.81–1.09) | 0.76 ± 0.23 |
| Manual Measurement (n = 35) | Semiautomated Measurement (n = 35) | p-Value | |
|---|---|---|---|
| LAVi (mL/m2) | 30 ± 8 | 30 ± 7 | NS |
| RAVi (mL/m2) | 29 ± 9 | 28 ± 9 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gopalan, D.; Riley, J.; Leong, K.; Alsanjari, S.; Ariff, B.; Auger, W.; Lindholm, P. Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology. Tomography 2022, 8, 2761-2771. https://doi.org/10.3390/tomography8060230
Gopalan D, Riley J, Leong K, Alsanjari S, Ariff B, Auger W, Lindholm P. Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology. Tomography. 2022; 8(6):2761-2771. https://doi.org/10.3390/tomography8060230
Chicago/Turabian StyleGopalan, Deepa, Jan Riley, Kai’En Leong, Senan Alsanjari, Ben Ariff, Willam Auger, and Peter Lindholm. 2022. "Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology" Tomography 8, no. 6: 2761-2771. https://doi.org/10.3390/tomography8060230
APA StyleGopalan, D., Riley, J., Leong, K., Alsanjari, S., Ariff, B., Auger, W., & Lindholm, P. (2022). Biatrial Volumetric Assessment by Non-ECG-Gated CT Pulmonary Angiography Correlated with Transthoracic Echocardiography in Patients with Normal Diastology. Tomography, 8(6), 2761-2771. https://doi.org/10.3390/tomography8060230