
Predictive Model for the Diagnosis of Uterine Prolapse Based on Transperineal Ultrasound

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Data Collection
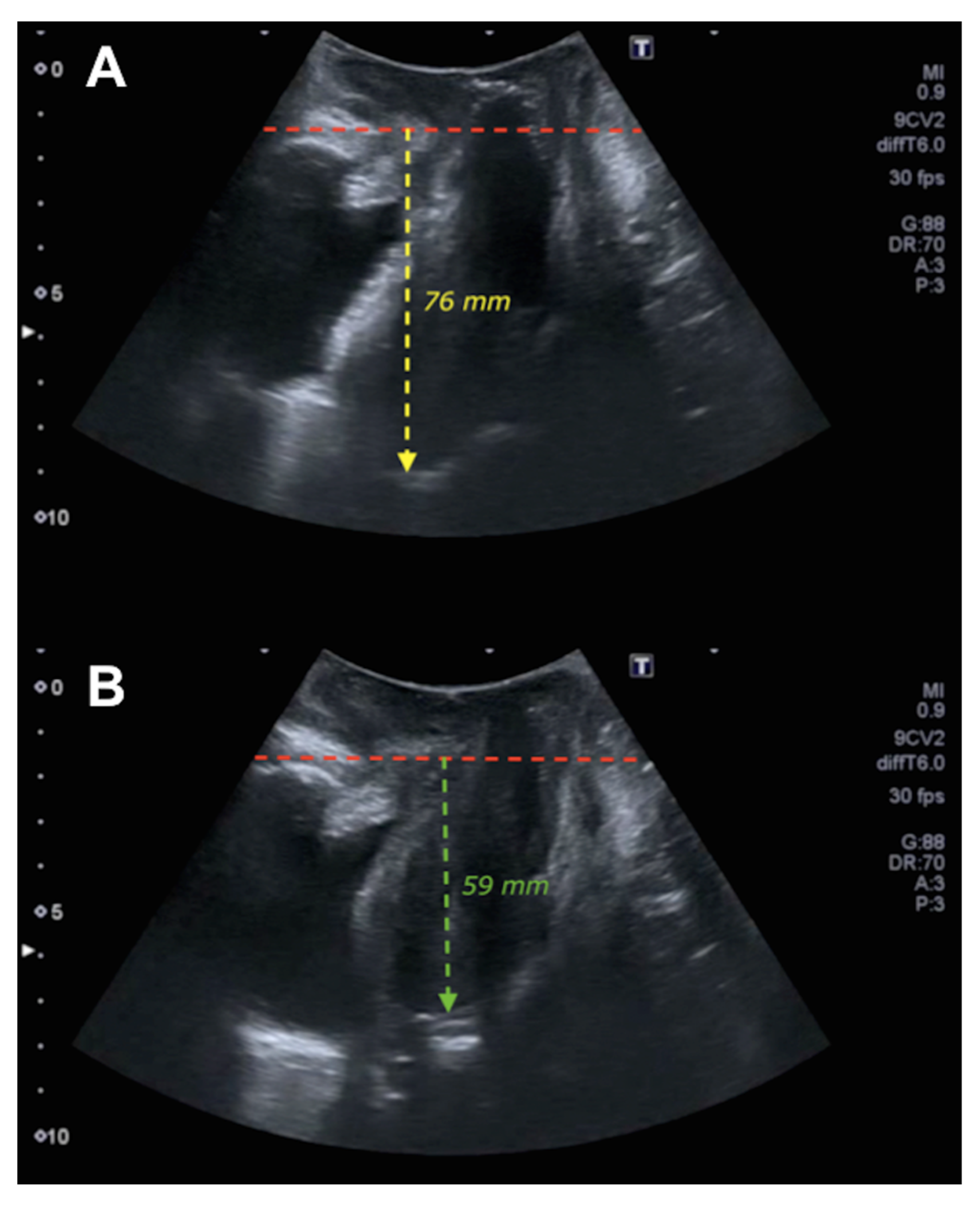
2.3. Ultrasound Assessment
2.4. Statistical Analysis
Evaluation of the Logistic Regression Models
3. Results
4. Discussion
Limitations and Strength
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| POP | Pelvic organ prolapse |
| RVA | Retrovesical angle |
| UP | Uterine prolapse |
| CE | Cervical elongation |
| ICS POP-Q | International Continence Society Pelvic Organ Prolapse Quantification system |
References
- Molina, F.S.; Nicolaides, K.H. Ultrasound in labor and delivery. Fetal Diagn. Ther. 2010, 27, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Gugliotta, G.; Schiattarella, A.; Giunta, M.; De Franciscis, P.; Potito, S.; Calagna, G. Translabial ultrasound evaluation after tension-free transobturator tape technique: Outcomes based on the tape’s position. Int. J. Gynaecol. Obstet. 2022. [Google Scholar] [CrossRef] [PubMed]
- Dietz, H.P.; Lekskulchai, O. Ultrasound assessment of prolapse: The relationship between prolapse severity and symptoms. Ultrasound Obstet. Gynecol. 2007, 29, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Shek, K.L.; Dietz, H.P. What is abnormal uterine descent on translabial ultrasound? Int. Urogynecol. J. 2015, 26, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, V.H.; Chantarasorn, V.; Shek, K.L.; Dietz, H.P. Does levator ani injury affect cystocele type? Ultrasound Obstet. Gynecol. 2010, 36, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Green, T.H., Jr. Urinary stress incontinence: Differential diagnosis, pathophysiology, and management. Am. J. Obstet. Gynecol. 1975, 122, 368–400. [Google Scholar] [CrossRef]
- Chantarasorn, V.; Dietz, H.P. Diagnosis of cystocele type by clinical examination and pelvic floor ultrasound. Ultrasound Obstet. Gynecol. 2012, 39, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Dietz, H.P.; Steensma, A.B. Posterior compartment prolapse on two-dimensional and three-dimensional pelvic floor ultrasound: The distinction between true rectocele, perineal hypermotility and enterocele. Ultrasound Obstet. Gynecol. 2005, 26, 73–77. [Google Scholar] [CrossRef] [PubMed]
- García-Mejido, J.A.; Ramos-Vega, Z.; Armijo-Sánchez, A.; Fernández-Palacín, A.; García-Jimenez, R.; Sainz, J.A. Differential diagnosis of middle compartment pelvic organ prolapse with transperineal ultrasound. Int. Urogynecol. J. 2021, 23, 2219–2225. [Google Scholar] [CrossRef]
- García-Mejido, J.A.; Ramos Vega, Z.; Armijo Sánchez, A.; Fernández-Palacín, A.; Fernández, C.B.; Sainz Bueno, J.A. Interobserver variability of ultrasound measurements for the differential diagnosis of uterine prolapse and cervical elongation without uterine prolapse. Int. Urogynecol. J. 2021, 1–7. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef]
- Salvatore, S.; Athanasiou, S.; Digesu, G.A.; Soligo, M.; Sotiropoulou, M.; Serati, M.; Antsaklis, A.; Milani, R. Identification of risk factors for genital prolapse recurrence. Neurourol. Urodyn. 2009, 28, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Tsikouras, P.; Dafopoulos, A.; Vrachnis, N.; Iliodromiti, Z.; Bouchlariotou, S.; Pinidis, P.; Tsagias, N.; Liberis, V.; Galazios, G.; Von Tempelhoff, G.F. Uterine prolapse in pregnancy: Risk factors, complications and management. J. Matern. Fetal Neonatal Med. 2014, 27, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Broekhuis, S.R.; Fütterer, J.J.; Barentsz, J.O.; Vierhout, M.E.; Kluivers, K.B. A systematic review of clinical studies on dynamic magnetic resonance imaging of pelvic organ prolapse: The use of reference lines and anatomical landmarks. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2009, 20, 721–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, H.P.; Mann, K. What is clinically relevant prolapse? An attempt at defining cutoffs for the clinical assessment of pelvic organ descent. Int. Urogynecol. J. 2014, 25, 451–455. [Google Scholar] [CrossRef]
- Dietz, H.P.; Simpson, J.M. Levator trauma is associated with pelvic organ prolapse. BJOG 2008, 115, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Dietz, H.P.; Shek, K.L. Tomographic ultrasound imaging of the pelvic floor: Which levels matter most? Ultrasound Obstet. Gynecol. 2009, 33, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Orejuela, F.; Shek, K.L.; Dietz, H.P. The time factor in the assessment of prolapse and levator ballooning. Int. Urogynecol. J. 2012, 23, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Dietz, H. Ultrasound imaging of the pelvic floor. Part 1: Two-dimensional aspects. Ultrasound Obstet. Gynecol. 2004, 23, 80–92. [Google Scholar] [CrossRef] [PubMed]
- García-Mejido, J.A.; Bonomi-Barby, M.J.; Armijo-Sanchez, A.; Borrero-Fernández, C.; Castro-Portillo, L.; Vargas-Broquetas, M.; Sainz, J.A. Metodología para el estudio ecográfico transperineal del suelo pélvico. Clin. Investig. Ginecol. Obstet. 2021, 48, 190–195. [Google Scholar] [CrossRef]
- Dietz, H.P.; Bernardo, M.J.; Kirby, A.; Shek, K.L. Minimal criteria for the diagnosis of avulsion of the puborectalis muscle by tomographic ultrasound. Int. Urogynecol. J. 2011, 22, 699–704. [Google Scholar] [CrossRef]
- Dietz, H.P.; Pattillo Garnham, A.; Guzmán Rojas, R. Is it necessary to diagnose levator avulsion on pelvic floor muscle contraction? Ultrasound Obstet. Gynecol. 2017, 49, 252–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, H.P.; Garnham, A.P.; Rojas, R.G. Is the levator-urethra gap helpful for diagnosing avulsion? Int. Urogynecol. J. 2016, 27, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Lone, F.W.; Thakar, R.; Sultan, A.H.; Stankiewicz, A. Accuracy of assessing Pelvic Organ Prolapse Quantification points using dynamic 2D transperineal ultrasound in women with pelvic organ prolapse. Int. Urogynecol. J. 2012, 23, 1555–1560. [Google Scholar] [CrossRef] [PubMed]
- Kluivers, K.B.; Jan, C.M.; Shek, H.C.; Dietz, H.P. Pelvic organ prolapse symptoms in relation to POP-Q, ordinal stages and ultrasound prolapse assessment. Int. Urogynecol. J. 2008, 19, 1299–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, H.P.; Haylen, B.T.; Broome, J. Ultrasound in the quantification of female pelvic organ prolapse. Ultrasound Obstet. Gynecol. 2001, 18, 511–514. [Google Scholar] [CrossRef]
- Broekhuis, S.R.; Kluivers, K.B.; Hendriks, J.C.M.; Futterer, J.J.; Barentsz, J.O.; Vierhout, M.E. POP-Q, dynamic MR imaging and perineal ultrasonography: Do they agree in quantification of female pelvic organ prolapse? Int. Urogynecol. J. 2009, 20, 541–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Mejido, J.A.; González-Diaz, E.; Ortega, I.; Borrero, C.; Fernández-Palacín, A.; Sainz-Bueno, J.A. 2D ultrasound diagnosis of middle compartment prolapse: A multicenter study. Quant. Imaging Med. Surg. 2021, 12, 959. [Google Scholar] [CrossRef] [PubMed]
- Swenson, C.W.; Smith, T.M.; Luo, J.; Kolenic, G.E.; Ashton-Miller, J.A.; DeLancey, J.O. Intraoperative cervix location and apical support stiffness in women with and without pelvic organ prolapse. Am. J. Obstet. Gynecol. 2017, 216, 155.e1–155.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Ashton-Miller, J.A.; DeLancey, J.O. A 3D finite element model of anterior vaginal wall support to evaluate mechanisms underlying cystocele formation. J. Biomech. 2009, 42, 1371–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Betschart, C.; Chen, L.; Ashton-Miller, J.A.; DeLancey, J.O. Using stress MRI to analyze the 3D changes in apical ligament geometry from rest to maximal Valsalva: A pilot study. Int. Urogynecol. J. 2014, 25, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Mias, N.L.; Subramaniam, N.; Friedman, T.; Shek, K.L.; Dietz, H.P. Prolapse assessment supine and standing: Do we need different cutoffs for “significant prolapse”? Int. Urogynecol. J. 2018, 29, 685–689. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| UP (ICS POP-Q) (n = 66) | CE without UP (ICS POP-Q) (n = 40) | p | 95% CI | |
|---|---|---|---|---|
| Age | 62.3 ± 11.3 | 52.1 ± 9.9 | <0.0005 | 5.9; 14.4 |
| BMI | 27.6 ± 3.3 | 28.1 ± 4.4 | 0.464 | −2.1; 1.0 |
| Deliveries | 3.1 ± 1.6 | 2.1 ± 0.9 | <0.0005 | 0.4; 1.4 |
| Cesarean sections | 0.1 ± 0.5 | 0.2 ± 0.5 | 0.384 | −0.3; 0.1 |
| Abortions | 0.5 ± 0.9 | 0.7 ± 1.0 | 0.197 | −0.6; 0.1 |
| Age at menopause | 52.6 ± 7.9 | 53.1 ± 5.6 | 0.790 | −5.0; 3.8 |
| Stress incontinence | 15 (22.7%) | 5 (12.5%) | 0.214 | −4.5; 25.0 |
| Urge incontinence | 22 (33.3%) | 8 (20.0%) | 0.183 | −3.9; 30.6 |
| Mixed incontinence | 9 (13.6%) | 3 (7.5%) | 0.529 | −5.8; 18.0 |
| Cystocele | 51 (77.3%) | 14 (35.0%) | <0.0005 | 23.9; 60.7 |
| Rectocele | 16 (24.2%) | 3 (7.5%) | 0.037 | 3.3; 30.2 |
| Enterocele | 8 (12.1%) | 1 (2.5%) | 0.149 | −0.2; 20.6 |
| UP (ICS POP-Q) (n = 66) | CE without UP (ICS POP-Q) (n = 40) | p | 95% CI | |
|---|---|---|---|---|
| Levator hiatal area (cm2) | ||||
| Rest | 20.8 ± 5.3 | 23.1 ± 6.1 | 0.038 | −4.6; −0.1 |
| Valsalva | 31.2 ± 8.7 | 33.0 ± 8.5 | 0.297 | −5.2; 1.6 |
| LAM avulsion | 19 (28.8%) | 6 (15.0%) | 0.156 | −2.1; 29.7 |
| Ballooning | 49 (74.2%) | 35 (87.5%) | 0.139 | −28.3; 1.8 |
| Pubis–uterine fundus measurement | ||||
| Rest | −66.3 ± 12.8 | −74.8 ± 16.8 | 0.008 | 2.3; 14.6 |
| Valsalva | −41.2 ± 14.8 | −67.9 ± 17.3 | <0.0005 | 20.5; 33.0 |
| Pubis–uterine fundus measurement. Difference between rest and Valsalva | 25.1 ± 11.7 | 6.8 ± 4.4 | <0.0005 | 15.2; 21.5 |
| Models | Variables | OR | 95% CI | Calibration (Homer–Lemeshow) p | Discrimination (Harrel’s C-Index 95% CI) |
|---|---|---|---|---|---|
| 1 | Pubis–uterine fundus measurement Difference between rest and Valsalva | 1.434 | 1.219–1.688 | 0.979 | 0.967 (0.939–0.995) |
| Age | 1.121 | 1.041–1.206 | |||
| 2 | Pubis–uterine fundus measurement Difference between rest and Valsalva | 1.492 | 1.243–1.791 | 0.958 | 0.971 (0.945–0.997) |
| Age | 1.124 | 1.037–1.220 | |||
| LAM avulsion | 0.803 | 0.108–5.944 | |||
| Ballooning | 0.120 | 0.012–1.171 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Mejido, J.A.; Ramos-Vega, Z.; Fernández-Palacín, A.; Borrero, C.; Valdivia, M.; Pelayo-Delgado, I.; Sainz-Bueno, J.A. Predictive Model for the Diagnosis of Uterine Prolapse Based on Transperineal Ultrasound. Tomography 2022, 8, 1716-1725. https://doi.org/10.3390/tomography8040144
García-Mejido JA, Ramos-Vega Z, Fernández-Palacín A, Borrero C, Valdivia M, Pelayo-Delgado I, Sainz-Bueno JA. Predictive Model for the Diagnosis of Uterine Prolapse Based on Transperineal Ultrasound. Tomography. 2022; 8(4):1716-1725. https://doi.org/10.3390/tomography8040144
Chicago/Turabian StyleGarcía-Mejido, José Antonio, Zenaida Ramos-Vega, Ana Fernández-Palacín, Carlota Borrero, Maribel Valdivia, Irene Pelayo-Delgado, and José Antonio Sainz-Bueno. 2022. "Predictive Model for the Diagnosis of Uterine Prolapse Based on Transperineal Ultrasound" Tomography 8, no. 4: 1716-1725. https://doi.org/10.3390/tomography8040144
APA StyleGarcía-Mejido, J. A., Ramos-Vega, Z., Fernández-Palacín, A., Borrero, C., Valdivia, M., Pelayo-Delgado, I., & Sainz-Bueno, J. A. (2022). Predictive Model for the Diagnosis of Uterine Prolapse Based on Transperineal Ultrasound. Tomography, 8(4), 1716-1725. https://doi.org/10.3390/tomography8040144