
Low kV Computed Tomography of Parenchymal Abdominal Organs—A Systematic Animal Study of Different Contrast Media Injection Protocols

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
2.2. CT Imaging
2.3. Injection Protocols
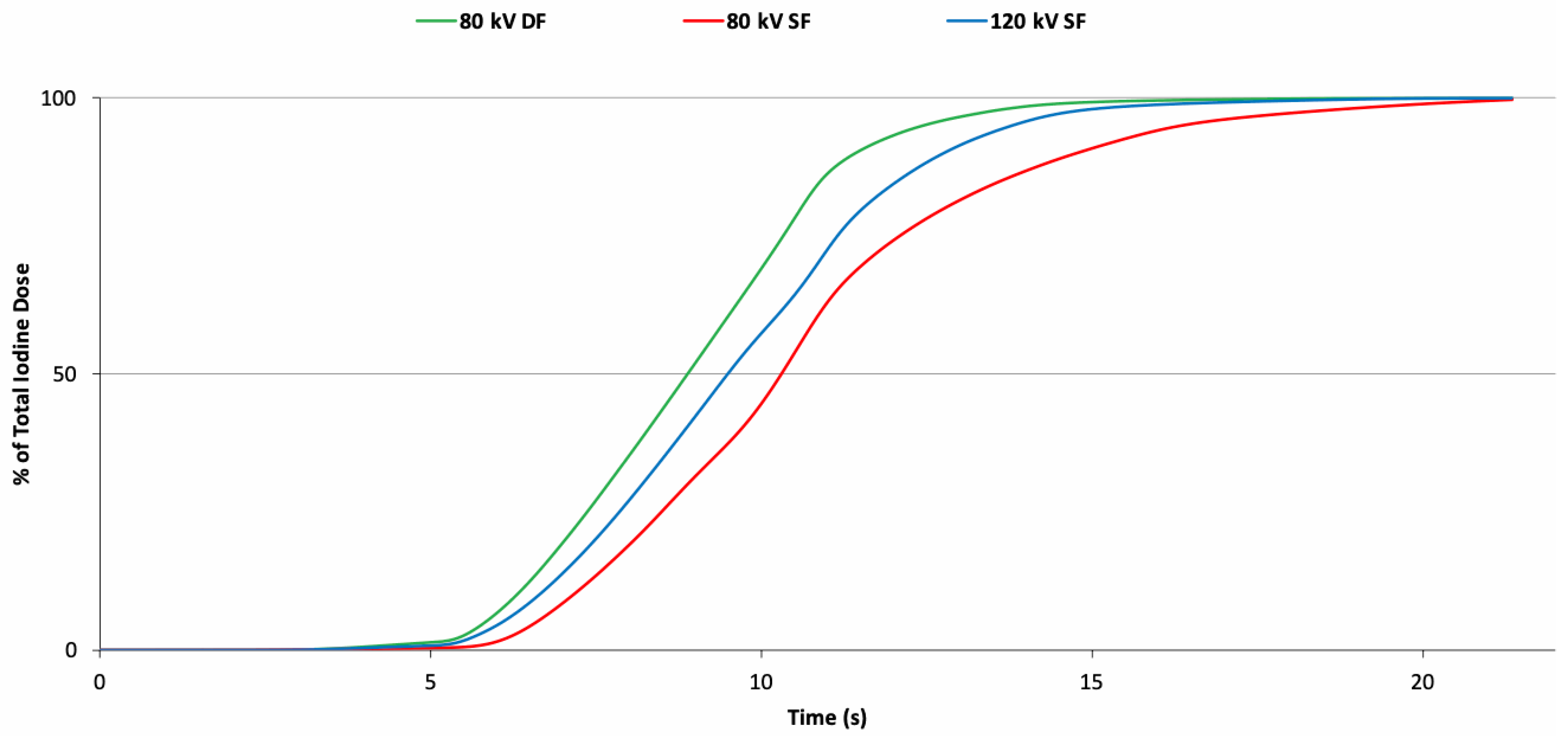
2.4. Fluid Delivery Measurements
2.5. Image Evaluation
2.6. Statistical Analysis
3. Results
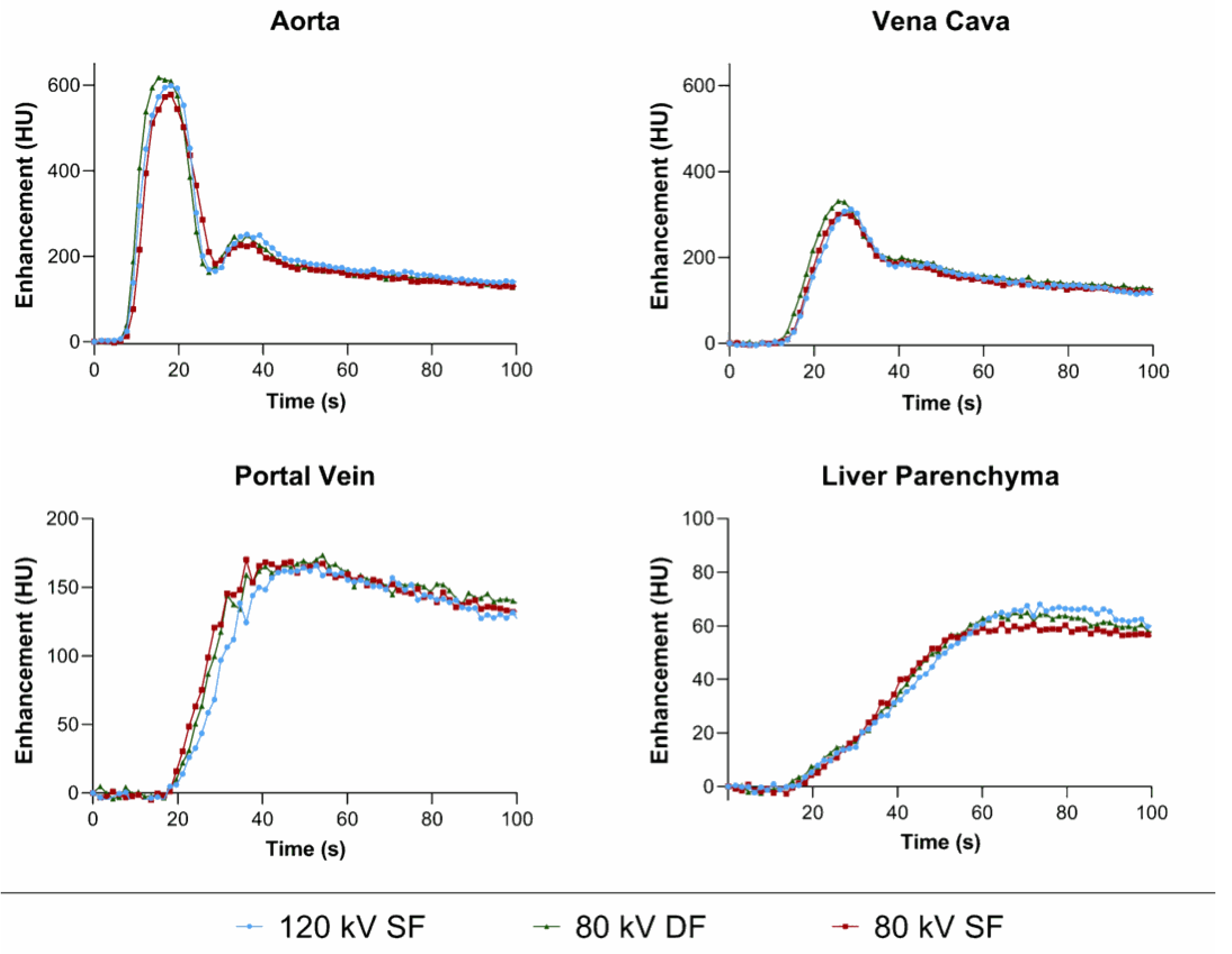
3.1. Dynamic CT
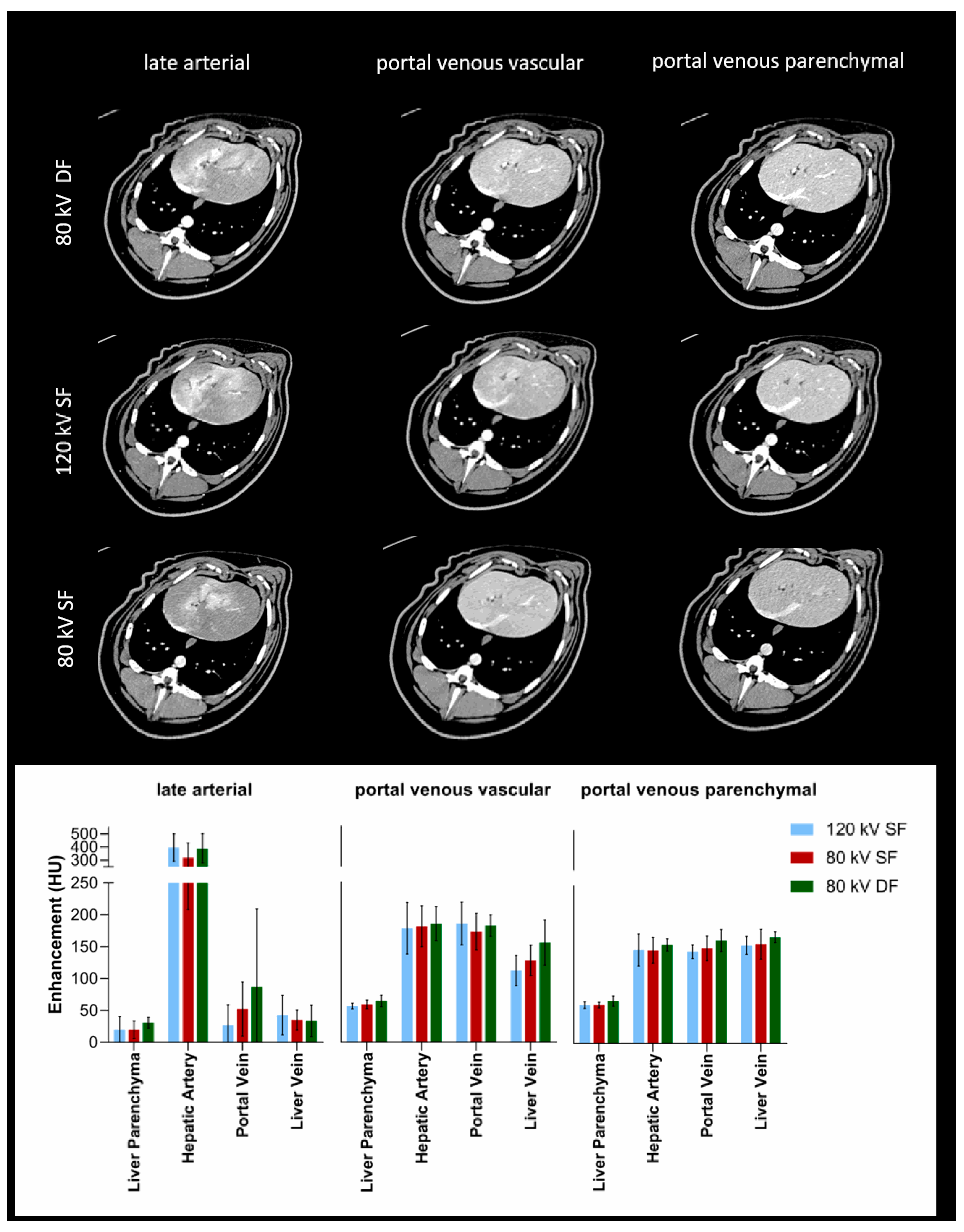
3.2. Multiphase Abdominal CT
3.3. Liver
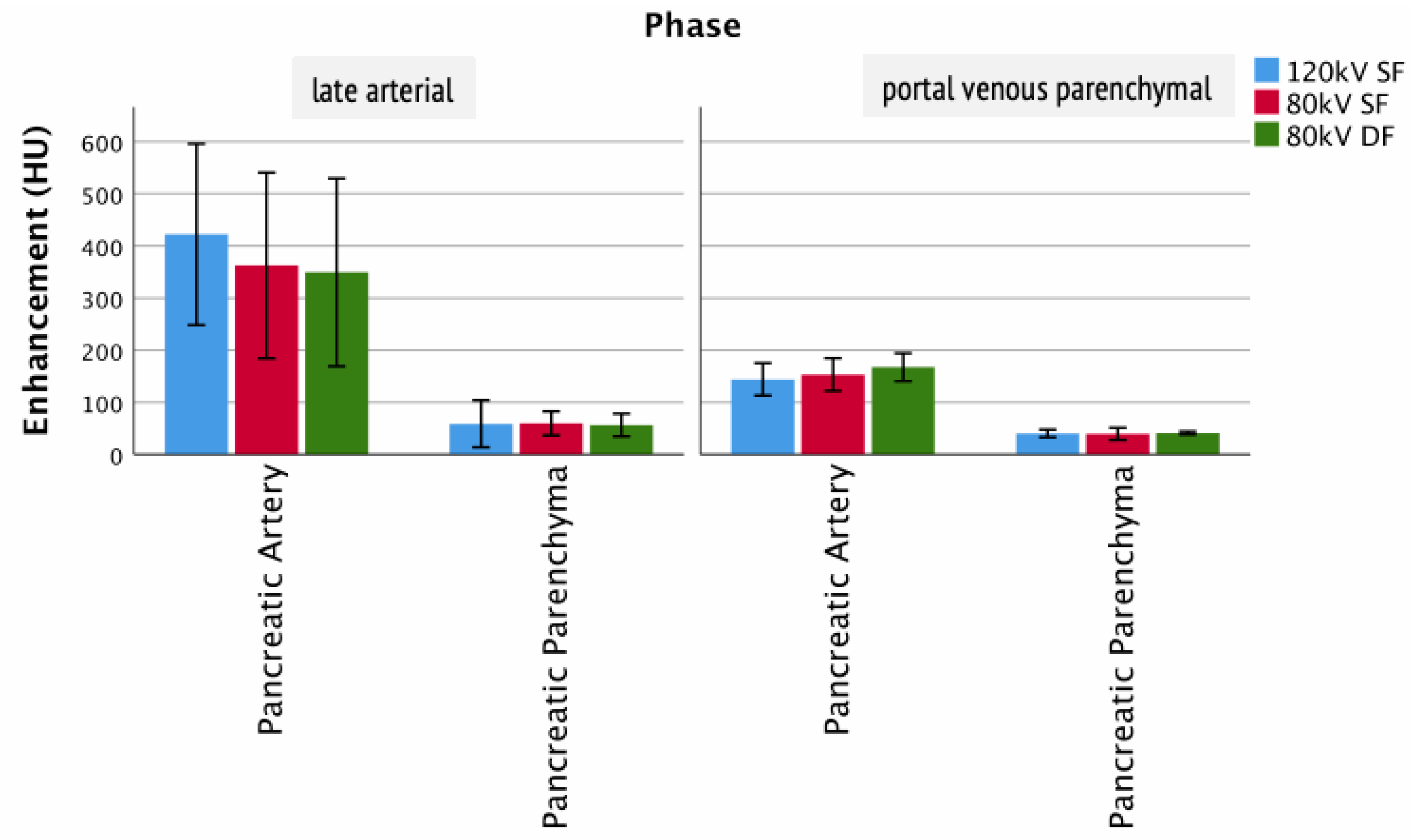
3.4. Pancreas
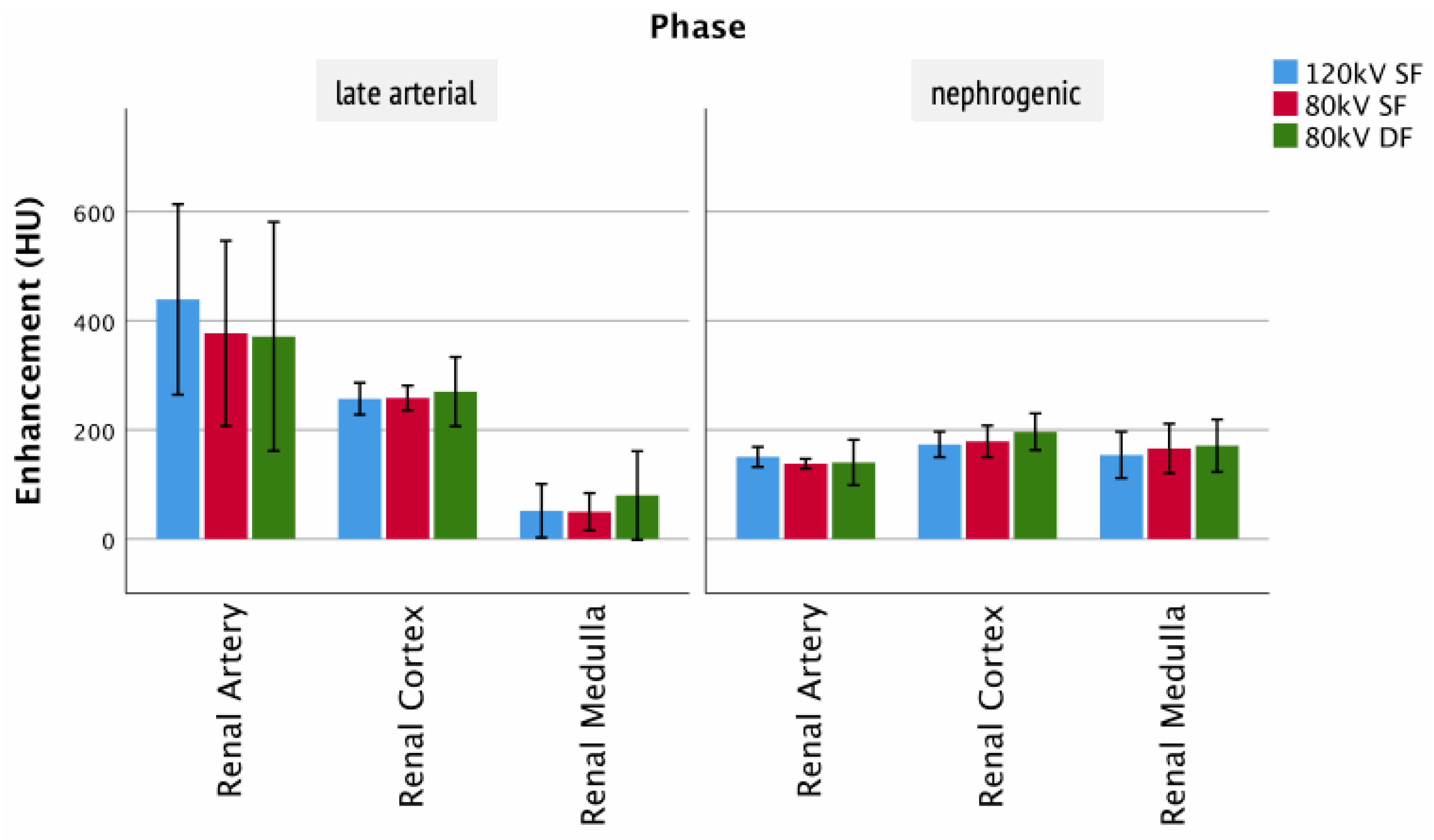
3.5. Kidney
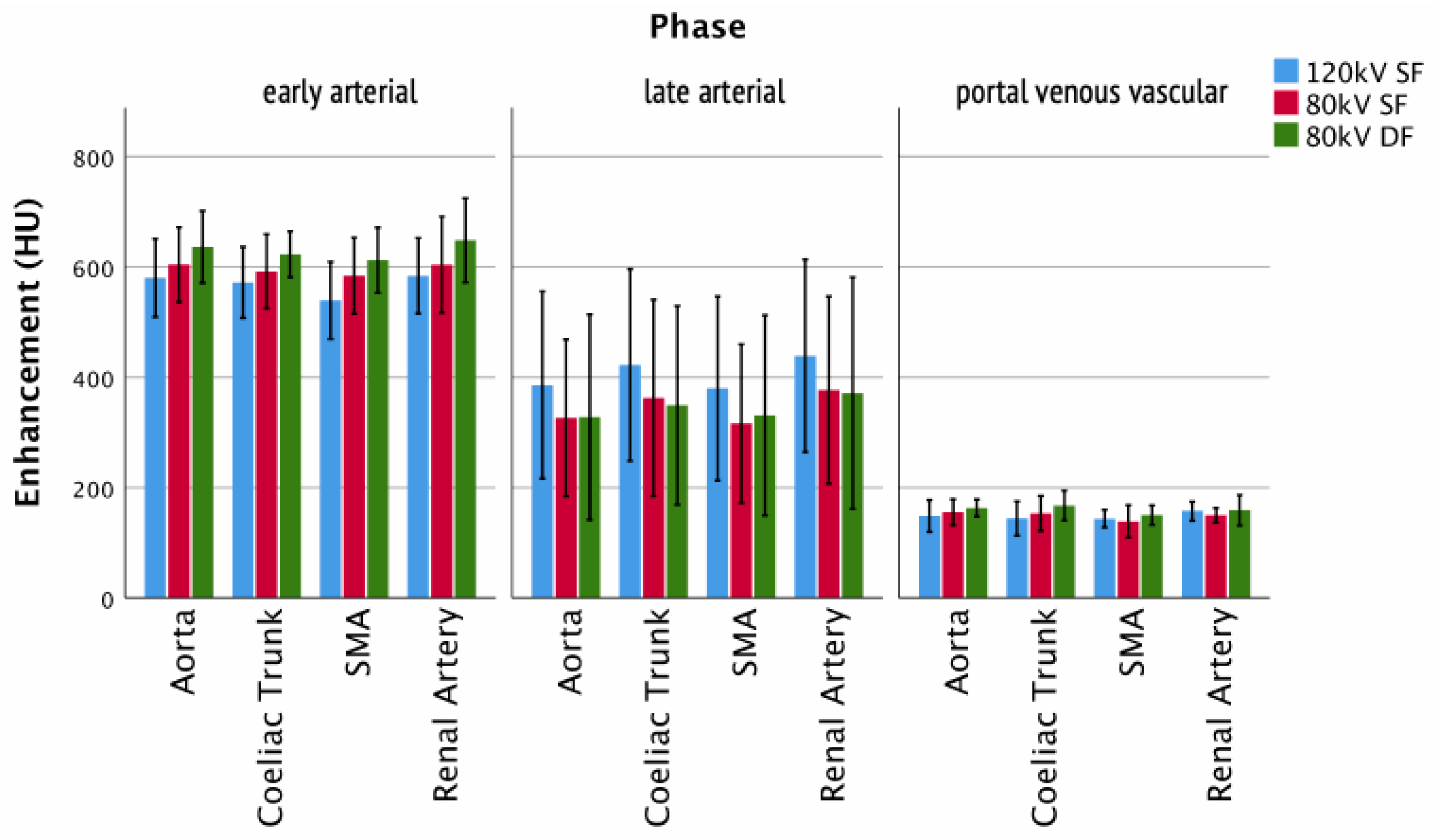
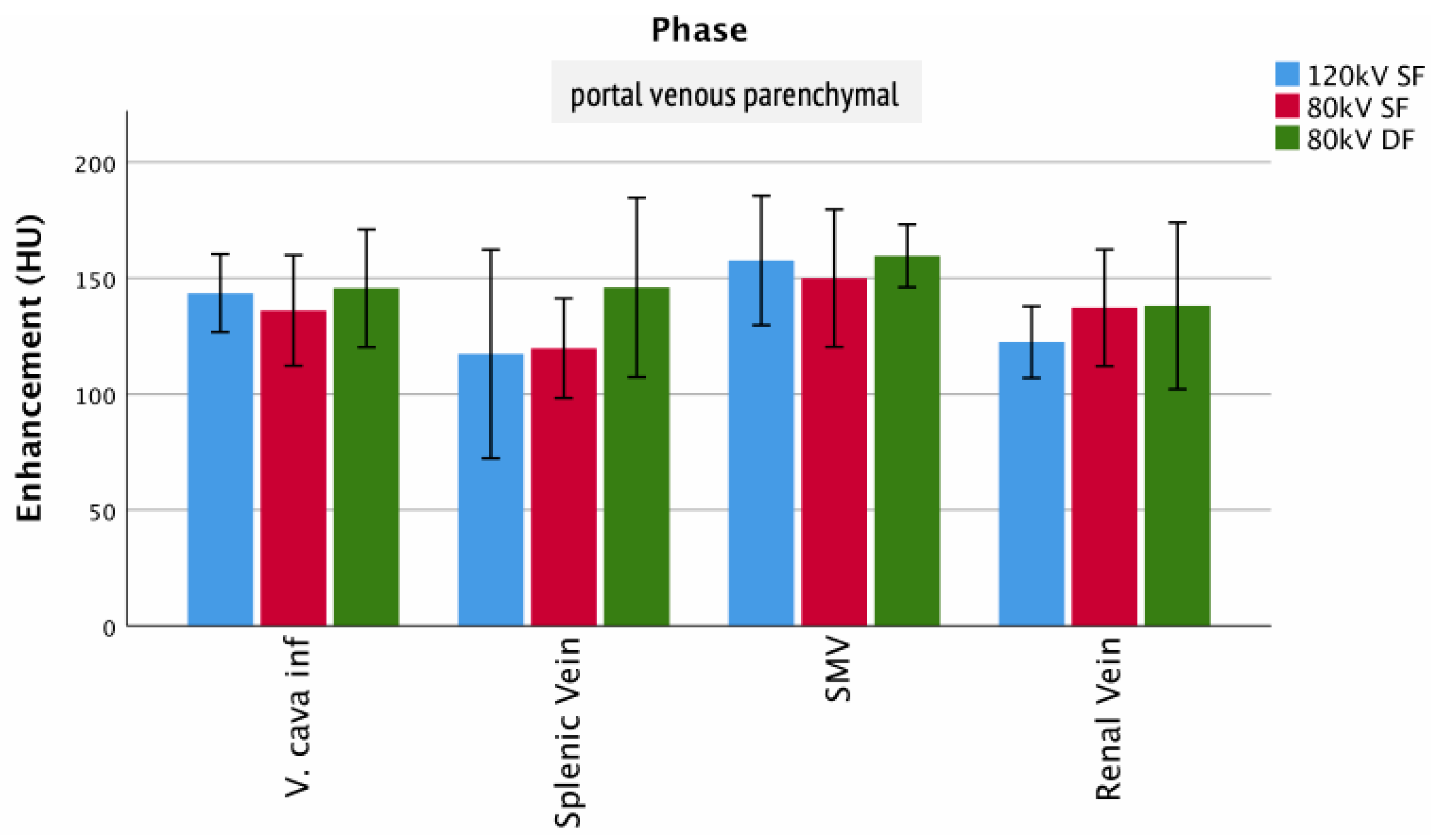
3.6. Arteries and Veins
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | area under the curve |
| CM | contrast media |
| CNR | contrast to noise ratio |
| CTA | computed tomography angiography |
| CO | cardiac output |
| DF | DualFlow |
| FW300 | full width 300 |
| FWHM | full width half max |
| IDR | iodine delivery rate |
| kV | kilovoltage |
| MaxHU | maximum Hounsfield units |
| SF | single flow |
| SNR | signal to noise ratio |
| SV | stroke volume |
| TTP | time to peak |
References
- Wintersperger, B.; Jakobs, T.; Herzog, P.; Schaller, S.; Nikolaou, K.; Suess, C.; Weber, C.; Reiser, M.; Becker, C. Aorto-iliac multidetector-row CT angiography with low kV settings: Improved vessel enhancement and simultaneous reduction of radiation dose. Eur. Radiol. 2005, 15, 334–341. [Google Scholar] [CrossRef]
- Ippolito, D.; Talei Franzesi, C.; Fior, D.; Bonaffini, P.A.; Minutolo, O.; Sironi, S. Low kV settings CT angiography (CTA) with low dose contrast medium volume protocol in the assessment of thoracic and abdominal aorta disease: A feasibility study. Br. J. Radiol. 2015, 88, 20140140. [Google Scholar] [CrossRef] [Green Version]
- Thor, D.; Brismar, T.B.; Fischer, M.A. Low tube voltage dual source computed tomography to reduce contrast media doses in adult abdomen examinations: A phantom study. Med. Phys. 2015, 42, 5100–5109. [Google Scholar] [CrossRef]
- Lell, M.M.; Jost, G.; Korporaal, J.G.; Mahnken, A.H.; Flohr, T.G.; Uder, M.; Pietsch, H. Optimizing contrast media injection protocols in state-of-the art computed tomographic angiography. Invest. Radiol. 2015, 50, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Mangold, S.; Wichmann, J.L.; Schoepf, U.J.; Caruso, D.; Tesche, C.; Steinberg, D.H.; Varga-Szemes, A.; Stubenrauch, A.C.; Bayer, R.R., II; Biancalana, M.; et al. Diagnostic accuracy of coronary CT angiography using 3(rd)-generation dual-source CT and automated tube voltage selection: Clinical application in a non-obese and obese patient population. Eur. Radiol. 2017, 27, 2298–2308. [Google Scholar] [CrossRef]
- Martens, B.; Hendriks Bmf Fau-Eijsvoogel, N.G.; Eijsvoogel Ng Fau-Wildberger, J.E.; Wildberger Je Fau-Mihl, C.; Mihl, C. Individually Body Weight-Adapted Contrast Media Application in Computed Tomography Imaging of the Liver at 90 kVp. Invest. Radiol. 2019, 54, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Goshima, S.; Kanematsu, M.; Noda, Y.; Kawai, N.; Kawada, H.; Ono, H.; Bae, K.T. Minimally Required Iodine Dose for the Detection of Hypervascular Hepatocellular Carcinoma on 80-kVp CT. Am. J. Roentgenol. 2016, 206, 518–525. [Google Scholar] [CrossRef]
- Goshima, S.; Kanematsu M Fau-Noda, Y.; Noda Y Fau-Kondo, H.; Kondo H Fau-Watanabe, H.; Watanabe H Fau-Kawada, H.; Kawada H Fau-Kawai, N.; Kawai N Fau-Tanahashi, Y.; Tanahashi Y Fau-Bae, K.T.; Bae, K.T. Determination of optimal intravenous contrast agent iodine dose for the detection of liver metastasis at 80-kVp CT. Eur. Radiol. 2014, 24, 1853–1859. [Google Scholar] [CrossRef]
- Heiken, J.P.; Brink, J.A.; McClennan, B.L.; Sagel, S.S.; Crowe, T.M.; Gaines, M.V. Dynamic incremental CT: Effect of volume and concentration of contrast material and patient weight on hepatic enhancement. Radiology 1995, 195, 353–357. [Google Scholar] [CrossRef]
- Martens, B.; Hendriks, B.M.F.; Mihl, C.; Wildberger, J.E. Tailoring Contrast Media Protocols to Varying Tube Voltages in Vascular and Parenchymal CT Imaging: The 10-to-10 Rule. Invest. Radiol. 2020, 55, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Behrendt, F.F.; Pietsch, H.; Jost, G.; Palmowski, M.; Gunther, R.W.; Mahnken, A.H. Identification of the iodine concentration that yields the highest intravascular enhancement in MDCT angiography. AJR Am. J. Roentgenol. 2013, 200, 1151–1156. [Google Scholar] [CrossRef]
- Bae, K.T.; Heiken, J.P.; Brink, J.A. Aortic and hepatic peak enhancement at CT: Effect of contrast medium injection rate--pharmacokinetic analysis and experimental porcine model. Radiology 1998, 206, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Overhoff, D.; Jost, G.; McDermott, M.; Wichtmann, B.; Schoenberg, S.O.; Pietsch, H.; Attenberger, U. Contrast Saline Mixture DualFlow Injection Protocols for Low-Kilovolt Computed Tomography Angiography: A Systematic Phantom and Animal Study. Investig. Radiol. 2020, 55, 785–791. [Google Scholar] [CrossRef]
- Miyoshi, K.; Onoda, H.; Tanabe, M.; Nakao, S.; Higashi, M.; Iida, E.; Okada, M.; Furukawa, M.; Ito, K. Image quality in dual-source multiphasic dynamic computed tomography of the abdomen: Evaluating the effects of a low tube voltage (70 kVp) in combination with contrast dose reduction. Abdom. Radiol. 2020, 45, 3755–3762. [Google Scholar] [CrossRef]
- McNulty, N.J.; Francis, I.R.; Platt, J.F.; Cohan, R.H.; Korobkin, M.; Gebremariam, A. Multi–detector row helical CT of the pancreas: Effect of contrast-enhanced multiphasic imaging on enhancement of the pancreas, peripancreatic vasculature, and pancreatic adenocarcinoma. Radiology 2001, 220, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Itoh, S.; Nagasaka, T.; Ogawa, H.; Ota, T.; Naganawa, S. CT findings in autoimmune pancreatitis: Assessment using multiphase contrast-enhanced multisection CT. Clin. Radiol. 2010, 65, 735–743. [Google Scholar] [CrossRef]
- Bronstein, Y.L.; Loyer, E.M.; Kaur, H.; Choi, H.; David, C.; DuBrow, R.A.; Broemeling, L.D.; Cleary, K.R.; Charnsangavej, C. Detection of small pancreatic tumors with multiphasic helical CT. Am. J. Roentgenol. 2004, 182, 619–623. [Google Scholar] [CrossRef]
- Böning, G.; Kahn, J.; Kaul, D.; Rotzinger, R.; Freyhardt, P.; Pavel, M.; Streitparth, F. CT follow-up in patients with neuroendocrine tumors (NETs): Combined radiation and contrast dose reduction. Acta Radiologica 2018, 59, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Chang, W.; Lee, E.S.; Lee, S.M.; Lee, J.M. Double low-dose dual-energy liver CT in patients at high-risk of HCC: A prospective, randomized, single-center study. Investig. Radiol. 2020, 55, 340–348. [Google Scholar] [CrossRef]
- Kanematsu, M.; Goshima, S.; Kawai, N.; Kondo, H.; Miyoshi, T.; Watanabe, H.; Noda, Y.; Tanahashi, Y.; Bae, K.T. Low-Iodine-Load and Low-Tube-Voltage CT Angiographic Imaging of the Kidney by Using Bolus Tracking with Saline Flushing. Radiology 2015, 275, 832–840. [Google Scholar] [CrossRef]
- Jost, G.; Pietsch, H.; Lengsfeld, P.; Hutter, J.; Sieber, M.A. The impact of the viscosity and osmolality of iodine contrast agents on renal elimination. Invest. Radiol. 2010, 45, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Mihl, C.; Wildberger, J.E.; Jurencak, T.; Yanniello, M.J.; Nijssen, E.C.; Kalafut, J.F.; Nalbantov, G.; Muhlenbruch, G.; Behrendt, F.F.; Das, M. Intravascular enhancement with identical iodine delivery rate using different iodine contrast media in a circulation phantom. Invest. Radiol. 2013, 48, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Behrendt, F.F.; Pietsch, H.; Jost, G.; Sieber, M.A.; Keil, S.; Plumhans, C.; Seidensticker, P.; Günther, R.W.; Mahnken, A.H. Intra-individual comparison of different contrast media concentrations (300 mg, 370 mg and 400 mg iodine) in MDCT. Eur. Radiol. 2010, 20, 1644–1650. [Google Scholar] [CrossRef]
- Nagayama, Y.; Oda, S.; Nakaura, T.; Tsuji, A.; Urata, J.; Furusawa, M.; Utsunomiya, D.; Funama, Y.; Kidoh, M.; Yamashita, Y. Radiation dose reduction at pediatric CT: Use of low tube voltage and iterative reconstruction. Radiographics 2018, 38, 1421–1440. [Google Scholar] [CrossRef] [Green Version]
- Bittner, D.O.; Arnold, M.; Klinghammer, L.; Schuhbaeck, A.; Hell, M.M.; Muschiol, G.; Gauss, S.; Lell, M.; Uder, M.; Hoffmann, U. Contrast volume reduction using third generation dual source computed tomography for the evaluation of patients prior to transcatheter aortic valve implantation. Eur. Radiol. 2016, 26, 4497–4504. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Part 1 | ||||||||
|---|---|---|---|---|---|---|---|---|
| Protocol | Tube Current (mAs) | Collimation (mm) | Rotation Time (s) | Pitch | CDTI (mGy∙cm/s) | Scan Duration (s) and Cycles | Reconstruction | Slice Thickness (mm) |
| 120 kV SF | 150 | 192 × 0.6 | 0.5 | - | 10 | 105/71 | Br36 | 2 |
| 80 kV SF | 430 | 192 × 0.6 | 0.5 | - | 8.3 | 105/71 | Br36 | 2 |
| 80 kV DF | 430 | 192 × 0.6 | 0.5 | - | 8.3 | 105/71 | Br36 | 2 |
| Study Part 2 | ||||||||
| 120 kV SF | 150 | 192 × 0.6 | 0.5 | 0.85 | 10 | 4 | Br40/Safire3 | 1.5 |
| 80 kV SF | 430 | 192 × 0.6 | 0.5 | 0.85 | 8.3 | 4 | Br40/Safire3 | 1.5 |
| 80 kV DF | 430 | 192 × 0.6 | 0.5 | 0.85 | 8.3 | 4 | Br40/Safire3 | 1.5 |
| Contrast Media (CM) Injection (ml/s) | Saline Injection | Dose CM (mgI/kg) | ||||
|---|---|---|---|---|---|---|
| Protocol | Tube Voltage (kV) | Flow Rate CM | DualFlow Saline | Flow Rate Saline (mL/s) | Volume (mL) | |
| SF 120 kV | 120 | 5 | - | 5 | 30 | 500 |
| SF 80 kV | 80 | 3 | - | 3 | 30 | 300 |
| DF 80 kV | 80 | 3 | 2 | 5 | 30 | 300 |
| Injection Protocol | |||||
|---|---|---|---|---|---|
| Phase | Structure | 80 kV DF (HU) | 120 kV SF (HU) | 80 kV SF (HU) | Friedmann p-Value |
| Late arterial | Liver Parenchyma | 30 ± 10 | 19 ± 21 | 20 ± 14 | 0.549 |
| Hepatic artery | 390 ± 111 | 396 ± 104 | 319. ± 111 | 0.247 | |
| Portal vein | 87 ± 123 | 27 ± 32 | 52 ± 43 | 0.819 | |
| Liver veins | 34 ± 25 | 41 ± 31 | 35 ± 16 | 0.549 | |
| Portal venous vascular | Liver Parenchyma | 65 ± 9 | 60 ± 3 | 59 ± 7 | 0.247 |
| Hepatic artery | 214 ± 44 | 178 ± 40 | 181 ± 32 | 0.247 | |
| Portal vein | 182 ± 17 | 186 ± 33 | 173 ± 28 | 0.549 | |
| Liver veins | 156 ± 35 | 112 ± 24 | 128 ± 24 | 0.247 | |
| Portal venous parenchymal | Liver Parenchyma | 67 ± 8 | 61 ± 4 | 61 ± 5 | 0.549 |
| Hepatic artery | 156 ± 10 | 148 ± 26 | 148 ± 20 | 0.692 | |
| Portal vein | 163 ± 17 | 146 ± 11 | 151 ± 19 | 0.247 | |
| Liver veins | 169 ± 9 | 156 ± 14 | 158 ± 24 | 0.247 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Overhoff, D.; Jost, G.; McDermott, M.; Weber, O.; Pietsch, H.; Schoenberg, S.O.; Attenberger, U. Low kV Computed Tomography of Parenchymal Abdominal Organs—A Systematic Animal Study of Different Contrast Media Injection Protocols. Tomography 2021, 7, 815-828. https://doi.org/10.3390/tomography7040069
Overhoff D, Jost G, McDermott M, Weber O, Pietsch H, Schoenberg SO, Attenberger U. Low kV Computed Tomography of Parenchymal Abdominal Organs—A Systematic Animal Study of Different Contrast Media Injection Protocols. Tomography. 2021; 7(4):815-828. https://doi.org/10.3390/tomography7040069
Chicago/Turabian StyleOverhoff, Daniel, Gregor Jost, Michael McDermott, Olaf Weber, Hubertus Pietsch, Stefan O. Schoenberg, and Ulrike Attenberger. 2021. "Low kV Computed Tomography of Parenchymal Abdominal Organs—A Systematic Animal Study of Different Contrast Media Injection Protocols" Tomography 7, no. 4: 815-828. https://doi.org/10.3390/tomography7040069
APA StyleOverhoff, D., Jost, G., McDermott, M., Weber, O., Pietsch, H., Schoenberg, S. O., & Attenberger, U. (2021). Low kV Computed Tomography of Parenchymal Abdominal Organs—A Systematic Animal Study of Different Contrast Media Injection Protocols. Tomography, 7(4), 815-828. https://doi.org/10.3390/tomography7040069