
Vascular Deformation Mapping of Abdominal Aortic Aneurysm

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
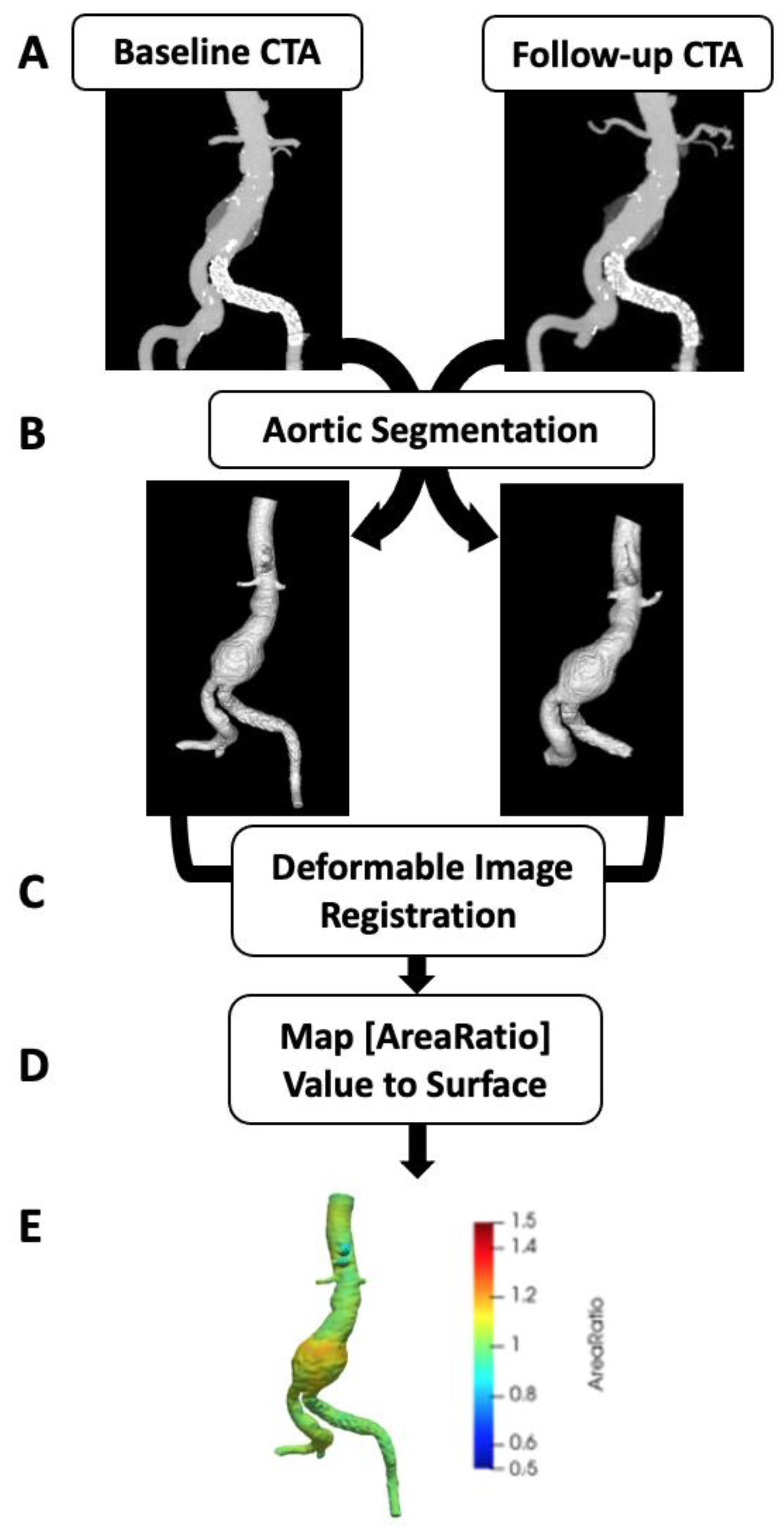
2.2. Image Segmentation
2.3. Vascular Deformation Mapping
2.4. Evaluation of Aortic Diameter and Volume
2.5. Statistics
3. Results
3.1. Patient Selection and VDM Technical Success
3.2. Patient Demographics
3.3. Evaluation of Diameter and Volume
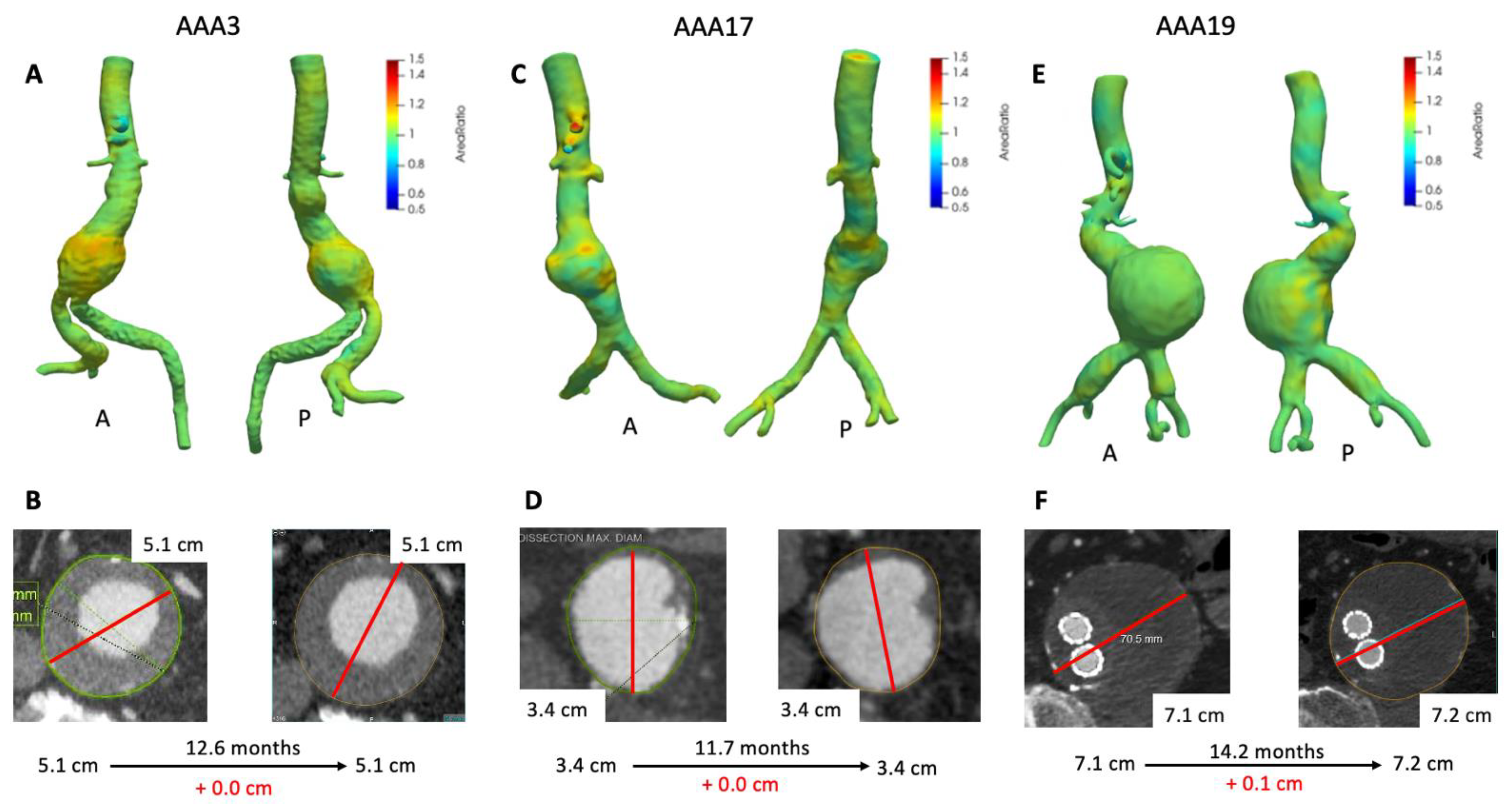
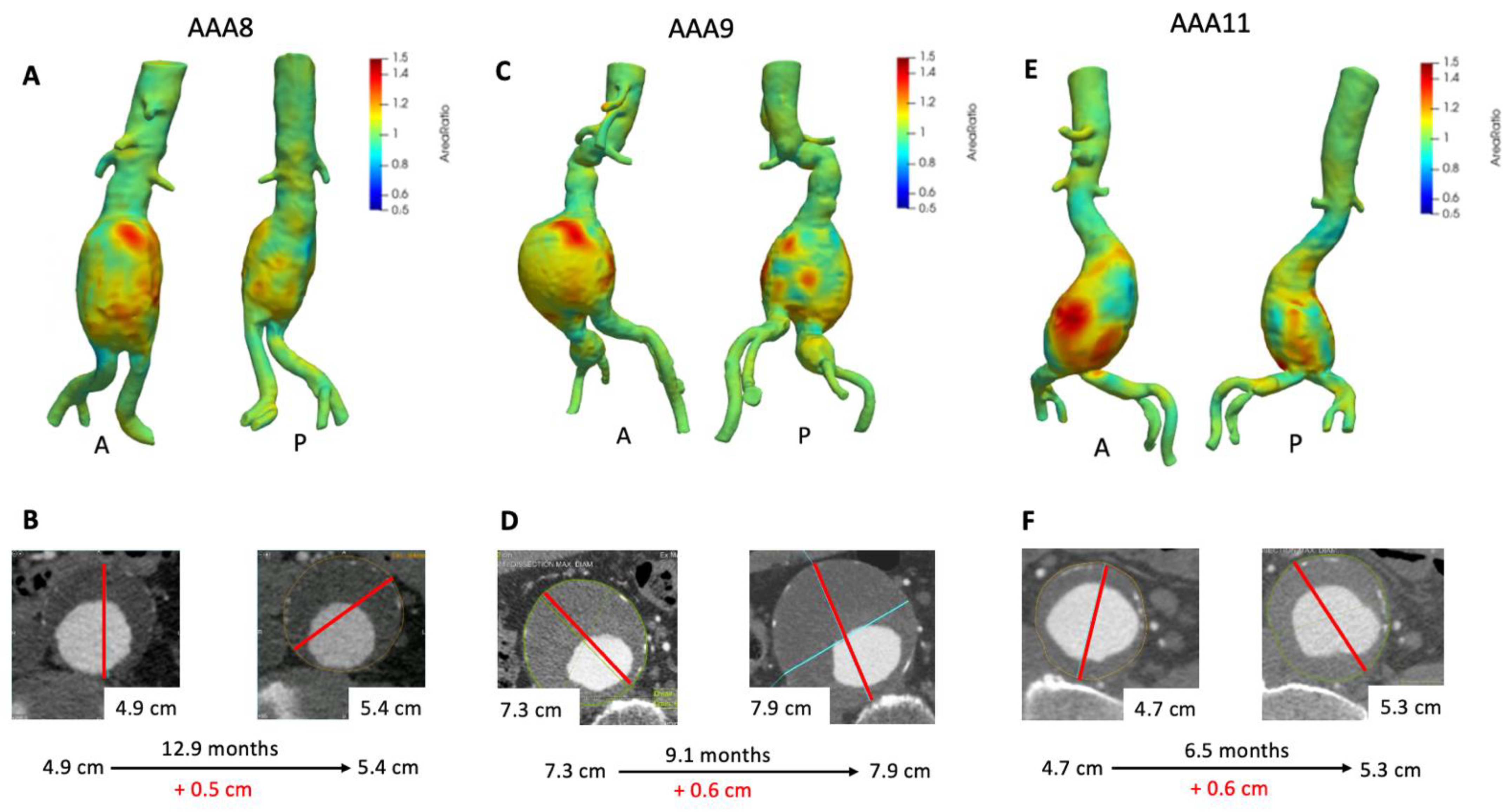
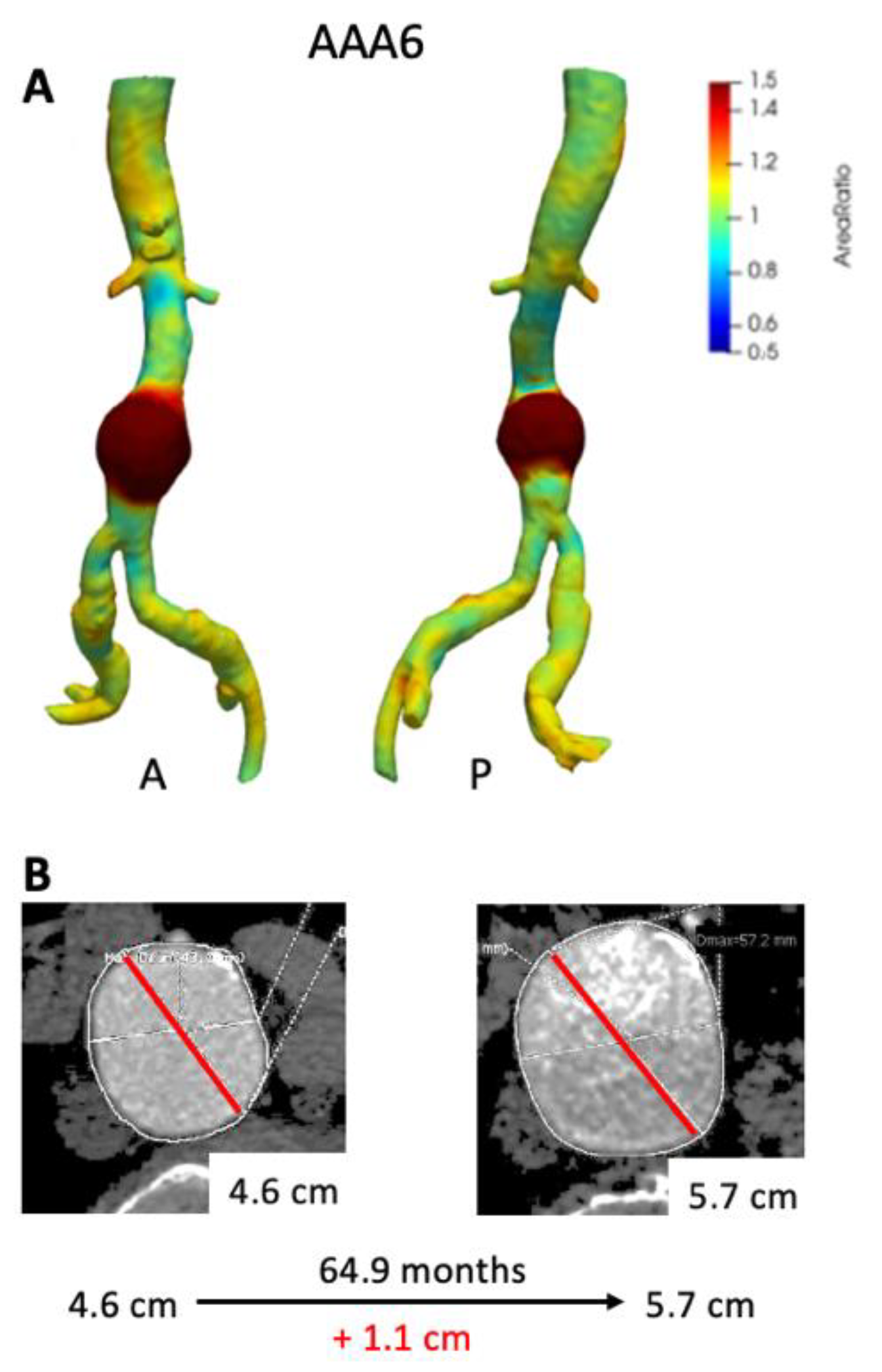
3.4. VDM Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakalihasan, N.; Limet, R.; Defawe, O. Abdominal aortic aneurysm. Lancet 2005, 365, 1577–1589. [Google Scholar] [CrossRef]
- Kniemeyer, H.W.; Kessler, T.; Reber, P.U.; Ris, H.B.; Hakki, H.; Widmer, M.K. Treatment of Ruptured Abdominal Aortic Aneurysm, a Permanent Challenge or a Waste of Resources? Prediction of Outcome Using a Multi-organ-dysfunction Score. Eur. J. Vasc. Endovasc. Surg. 2000, 19, 190–196. [Google Scholar] [CrossRef]
- Robinson, W.P. Open versus endovascular repair of rusptured abdominal aortic aneurysms: What have we learned after more than 2 decades of ruptured endovascular aneurysm repair? Surgery 2017, 162, 1207–1218. [Google Scholar] [CrossRef]
- Powell, J.T.; Brown, L.C.; Forbes, J.F.; Fowkes, F.G.R.; Greenhalgh, R.M.; Ruckley, C.V.; Thompson, S.G. Final 12-year follow-up of surgery versus surveillance in the UK Small Aneurysm Trial. Br. J. Surg. 2007, 94, 702–708. [Google Scholar] [CrossRef]
- Lederle, F.A.; Wilson, S.E.; Johnson, G.R.; Reinke, D.B.; Littooy, F.N.; Acher, C.W.; Ballard, D.J.; Messina, L.M.; Gordon, I.L.; Chute, E.P.; et al. Immediate Repair Compared with Surveillance of Small Abdominal Aortic Aneurysms. N. Engl. J. Med. 2002, 346, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, F.; Ferguson, S.; Lewis, P.; Williams, I.M.; Twine, C.P. South East Wales Vascular Network. Rupture rates of untreated large abdominal aortic aneurysms in patients unfit for elective repair. J. Vasc. Surg. 2015, 61, 1606–1612. [Google Scholar] [CrossRef] [PubMed]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E.; Ballard, D.J.; Jordan, W.D.; Blebea, J.; Littooy, F.N.; Freischlag, J.A.; Bandyk, D.; Rapp, J.H.; et al. Rupture rate of large abdominal aortic aneurysms in patients refusing or unfit for elective repair. JAMA 2002, 287, 2968–2972. [Google Scholar] [CrossRef] [PubMed]
- Dryjski, M.; Driscoll, J.L.; Blair, R.C.; McGurrin, M.A.; Dagher, F.J.; Ceraolo, M.J.; O’Donnel; Blackshear, W.M. The small abdominal aortic aneurysm: The eternal dilemma. J. Cardiovasc. Surg. 1994, 35, 95–100. [Google Scholar]
- Finol, E.A.; Amon, C.H. Blood Flow in Abdominal Aortic Aneurysms: Pulsatile Flow Hemodynamics. J. Biomech. Eng. 2001, 123, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Lederle, F.A.; Wilson, S.E.; Johnson, G.R.; Reinke, D.B.; Littooy, F.N.; Acher, C.W.; Messina, K.M.; Ballard, D.J.; Ansel, H.J. Variability in measurement of abdominal aortic aneurysms. Abdominal Aortic Aneurysm Detection and Management Veterans Administration Cooperative Study Group. J. Vasc. Surg. 1995, 21, 945–952. [Google Scholar] [CrossRef]
- Cayne, N.S.; Veith, F.J.; Lipsitz, E.C.; Ohki, T.; Mehta, M.; Gargiulo, N.; Suggs, W.D.; Rozenblit, A.; Ricci, Z.; Timaran, C.H. Variability of maximal aortic aneurysm diameter measurements on CT scan: Significance and methods to minimize. J. Vasc. Surg. 2004, 39, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Brady, A.R.; Thompson, S.G.; Fowkes, F.G.R.; Greenhalgh, R.M.; Powell, J.T. Abdominal Aortic Aneurysm Expansion: Risk Factors and Time Intervals for Surveillance. Circulation 2004, 110, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.T.; Sweeting, M.J.; Brown, L.C.; Gotensparre, S.M.; Fowkes, F.G.; Thompson, S.G. Systematic review and meta-analysis of growth rates of small abdominal aortic aneurysms. Br. J. Surg. 2011, 98, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Hua, J.; Mower, W.R. Simple geometric characteristics fail to reliably predict abdominal aortic aneurysm wall stresses. J. Vasc. Surg. 2001, 34, 308–315. [Google Scholar] [CrossRef]
- Vorp, D.A.; Raghavan, M.L.; Webster, M.W. Mechanical wall stress in abdominal aortic aneurysm: Influence of diameter and asymmetry. J. Vasc. Surg. 1998, 27, 632–639. [Google Scholar] [CrossRef]
- Kontopodis, N.; Lioudaki, S.; Pantidis, D.; Papadopoulos, G.; Georgakarakos, E.; Ioannou, C.V. Advances in determining abdominal aortic aneurysm size and growth. World J. Radiol. 2016, 8, 148–158. [Google Scholar] [CrossRef]
- Kauffmann, C.; Tang, A.; Therasse, E.; Giroux, M.F.; Elkouri, S.; Melanson, P.; Melanson, B.; Olivia, V.L.; Soulez, G. Measurements and detection of abdominal aortic aneurysm growth: Accuracy and reproducibility of a segmentation software. Eur. J. Radiol. 2012, 81, 1688–1694. [Google Scholar] [CrossRef]
- Parr, A.; Jayaratne, C.; Buttner, P.; Golledge, J. Comparison of volume and diameter measurement in assessing small abdominal aortic aneurysm expansion examined using computed tomographic angiography. Eur. J. Radiol. 2011, 79, 42–47. [Google Scholar] [CrossRef]
- Kontopodis, N.; Metaxa, E.; Papaharilaou, Y.; Georgakarakos, E.; Tsetis, D.; Ioannou, C.V. Value of volume measurements in evaluating abdominal aortic aneurysms growth rate and need for surgical treatment. Eur. J. Radiol. 2014, 83, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Burris, N.S.; Hoff, B.A.; Kazerooni, E.A.; Ross, B.D. Vascular Deformation Mapping (VDM) of Thoracic Aortic Enlargement in Aneurysmal Disease and Dissection. Tomography 2017, 3, 163. [Google Scholar] [CrossRef]
- Burris, N.S.; Hoff, B.A.; Patel, H.J.; Kazerooni, E.A.; Ross, B.D. Three-Dimensional Growth Analysis of Thoracic Aortic Aneurysm with Vascular Deformation Mapping. Circ. Cardiovasc. Imaging 2018, 11, e008045. [Google Scholar] [CrossRef]
- Kontopodis, N.; Metaxa, E.; Papaharilaou, Y.; Georgakarakos, E.; Tsetis, D.; Ioannou, C.V. Changes in geometric configuration and biomechanical parameters of a rapidly growing abdominal aortic aneurysm may provide insight in aneurysms natural history and rupture risk. Theor. Biol. Med. Model. 2013, 10, 67. [Google Scholar] [CrossRef]
- Martufi, G.; DiMartino, E.S.; Amon, C.H.; Muluk, S.C.; Finol, E.A. Three-dimensional geometrical characterization of abdominal aortic aneurysms: Image-based wall thickness distribution. J. Biomech. Eng. 2009, 131, 061015. [Google Scholar] [CrossRef]
- Farsad, M.; Zeinali-Davarani, S.; Choi, J.; Baek, S. Computational Growth and Remodeling of Abdominal Aortic Aneurysms Constrained by the Spine. J. Biomech. Eng. 2015, 137, 0910081–09100812. [Google Scholar] [CrossRef]
- Klein, S.; Staring, M.; Pluim, J.P. Evaluation of optimization methods for nonrigid medical image registration using mutual information and B-splines. IEEE Trans. Image Process. 2007, 16, 2879–2890. [Google Scholar] [CrossRef]
- Klein, S.; Staring, M.; Murphy, K.; Viergever, M.A.; Pluim, J.P. Elastix: A toolbox for intensity-based medical image registration. IEEE Trans. Med. Imaging 2010, 29, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Staring, M.; Klein, S.; Pluim, J.P. A rigidity penalty term for nonrigid registration. Med. Phys. 2007, 34, 4098–4108. [Google Scholar] [CrossRef] [PubMed]
- Elger, D.F.; Blackketter, D.M.; Budwig, R.S.; Johansen, K.H. The influence of shape on the stresses in model abdominal aortic aneurysms. J. Biomech. Eng. 1996, 118, 326–332. [Google Scholar] [CrossRef]
- Sacks, M.S.; Vorp, D.A.; Raghavan, M.L.; Federle, M.P.; Webster, M.W. In vivo three-dimensional surface geometry of abdominal aortic aneurysms. Ann. Biomed. Eng. 1999, 27, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Speelman, L.; Schurink, G.W.H.; Bosboom, E.M.H.; Buth, J.; Breeuwer, M.; van de Voose, F.N.; Jacobs, M.H. The mechanical role of thrombus on the growth rate of an abdominal aortic aneurysm. J. Vasc. Surg. 2010, 51, 19–26. [Google Scholar] [CrossRef]
- Di Martino, E.; Mantero, S.; Inzoli, F.; Melissano, G.; Astore, D.; Chiesa, R.; Fumero, R. Biomechanics of abdominal aortic aneurysm in the presence of endoluminal thrombus: Experimental characterisation and structural static computational analysis. Eur. J. Vasc. Endovasc. Surg. 1998, 15, 290–299. [Google Scholar] [CrossRef]
- Vorp, D.A.; Lee, P.C.; Wang, D.H.; Makaroun, M.S.; Nemoto, E.M.; Ogawa, S.; Webster, M.W. Association of intraluminal thrombus in abdominal aortic aneurysm with local hypoxia and wall weakening. J. Vasc. Surg. 2001, 34, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Parr, A.; McCann, M.; Bradshaw, B.; Shahzad, A.; Buttner, P.; Golledge, J. Thrombus volume is associated with cardiovascular events and aneurysm growth in patients who have abdominal aortic aneurysms. J. Vasc. Surg. 2011, 53, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Choksy, S.A.; Wilmink, A.B.; Quick, C.R. Ruptured abdominal aortic aneurysm in the Huntingdon district: A 10-year experience. Ann. R. Coll. Surg. Engl. 1999, 81, 27–31. [Google Scholar] [PubMed]
- Hall, A.J.; Busse, E.F.; McCarville, D.J.; Burgess, J.J. Aortic wall tension as a predictive factor for abdominal aortic aneurysm rupture: Improving the selection of patients for abdominal aortic aneurysm repair. Ann. Vasc. Surg. 2000, 14, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.L.; Wijesinha, M.A.; Panthofer, A.M.; Blackwelder, W.C.; Upchurch, G.R.; Terrin, M.L.; Curci, J.A.; Baxter, B.T.; Matsumura, J.S. Evaluating Growth Patterns of Abdominal Aortic Aneurysm Diameter with Serial Computed Tomography Surveillance. JAMA Surg. 2021. [Google Scholar] [CrossRef]
- Bian, Z.; Zhong, J.; Hatt, C.R.; Burris, N.S. A deformable image registration based method to assess directionality of thoracic aortic aneurysm growth. Med. Imaging 2021. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Age * | Sex | Smoker * | PAD | CAD | Previous Intervention | Subsequent Intervention | Rupture |
|---|---|---|---|---|---|---|---|---|
| AAA3 | 73 | Male | Current | Yes | Yes | No | Yes (EVAR) | No |
| AAA6 | 82 | Male | Never | No | Yes | No | No | No |
| AAA8 | 80 | Male | Former | No | No | No | Yes (EVAR) | No |
| AAA9 | 69 | Male | Former | No | Yes | No | Yes (EVAR) | No |
| AAA11 | 56 | Male | Current | No | No | No | Yes (EVAR) | No |
| AAA17 | 76 | Female | Former | No | No | No | Yes (EVAR) | No |
| AAA19 | 78 | Male | Former | No | Yes | Yes (EVAR) | No | No |
| Average | 72.57 | |||||||
| SD | 8.60 |
| Patient ID | Dmax CT1 (cm) | Volume CT1 (cm3) | Dmax CT2 (cm) | Volume CT2 (cm3) | ∆ Time (Months) | ∆ Dmax (cm) | ∆ Volume (cm3) |
|---|---|---|---|---|---|---|---|
| AAA3 | 5.1 | 124.15 | 5.1 | 136.02 | 12.6 | 0.0 | 11.87 |
| AAA6 | 4.6 | 58.13 | 5.7 | 99.81 | 64.9 | 1.1 | 41.68 |
| AAA8 | 4.9 | 113.41 | 5.4 | 151.26 | 12.9 | 0.6 | 37.85 |
| AAA9 | 7.3 | 263.42 | 7.9 | 335.43 | 9.1 | 0.6 | 72.01 |
| AAA11 | 4.8 | 103.18 | 5.2 | 139.95 | 6.5 | 0.4 | 36.77 |
| AAA17 | 3.4 | 43.70 | 3.4 | 45.49 | 11.7 | 0.0 | 1.79 |
| AAA19 | 7.1 | 243.48 | 7.2 | 238.39 | 14.2 | 0.1 | −5.09 |
| Average | 5.06 | 11.96 | 5.51 | 14.69 | |||
| SD | 1.17 | 7.15 | 1.33 | 9.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braet, D.J.; Eliason, J.; Ahmed, Y.; van Bakel, P.A.J.; Zhong, J.; Bian, Z.; Figueroa, C.A.; Burris, N.S. Vascular Deformation Mapping of Abdominal Aortic Aneurysm. Tomography 2021, 7, 189-201. https://doi.org/10.3390/tomography7020017
Braet DJ, Eliason J, Ahmed Y, van Bakel PAJ, Zhong J, Bian Z, Figueroa CA, Burris NS. Vascular Deformation Mapping of Abdominal Aortic Aneurysm. Tomography. 2021; 7(2):189-201. https://doi.org/10.3390/tomography7020017
Chicago/Turabian StyleBraet, Drew J., Jonathan Eliason, Yunus Ahmed, Pieter A. J. van Bakel, Jiayang Zhong, Zhangxing Bian, Carlos Alberto Figueroa, and Nicholas S. Burris. 2021. "Vascular Deformation Mapping of Abdominal Aortic Aneurysm" Tomography 7, no. 2: 189-201. https://doi.org/10.3390/tomography7020017
APA StyleBraet, D. J., Eliason, J., Ahmed, Y., van Bakel, P. A. J., Zhong, J., Bian, Z., Figueroa, C. A., & Burris, N. S. (2021). Vascular Deformation Mapping of Abdominal Aortic Aneurysm. Tomography, 7(2), 189-201. https://doi.org/10.3390/tomography7020017