
Reliability of Automated Amyloid PET Quantification: Real-World Validation of Commercial Tools Against Centiloid Project Method


Abstract
1. Introduction
2. Materials and Methods
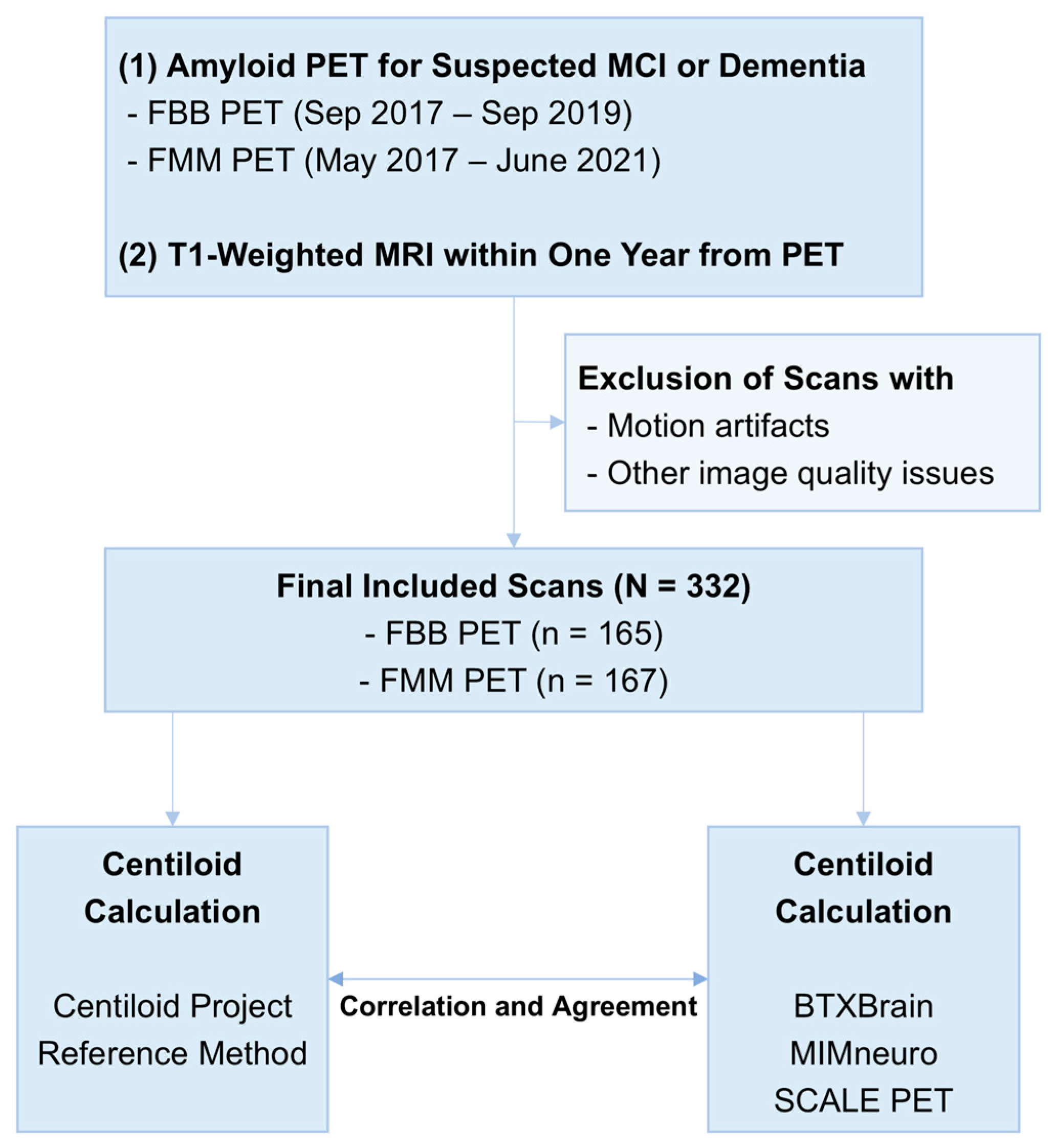
2.1. Patients
2.2. Amyloid PET Imaging and Visual Interpretation
2.3. The Centiloid Quantification Using the Original Centiloid Project Method
2.4. Automated Software-Based Centiloid Quantification
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
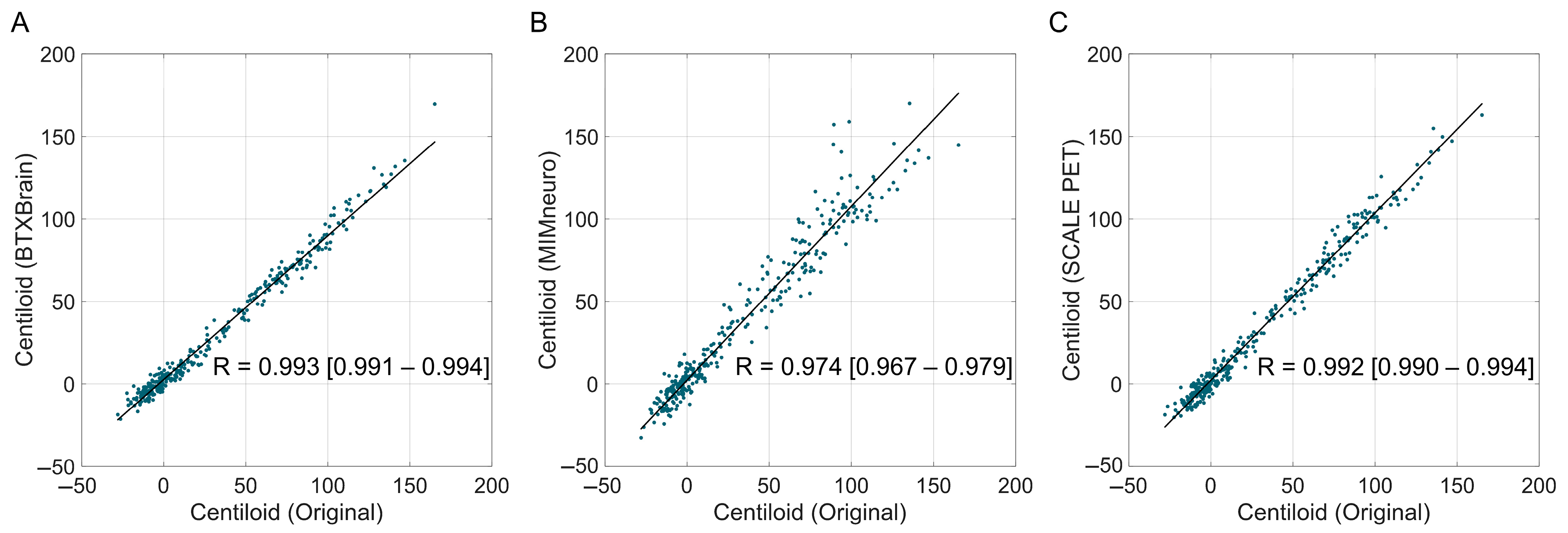
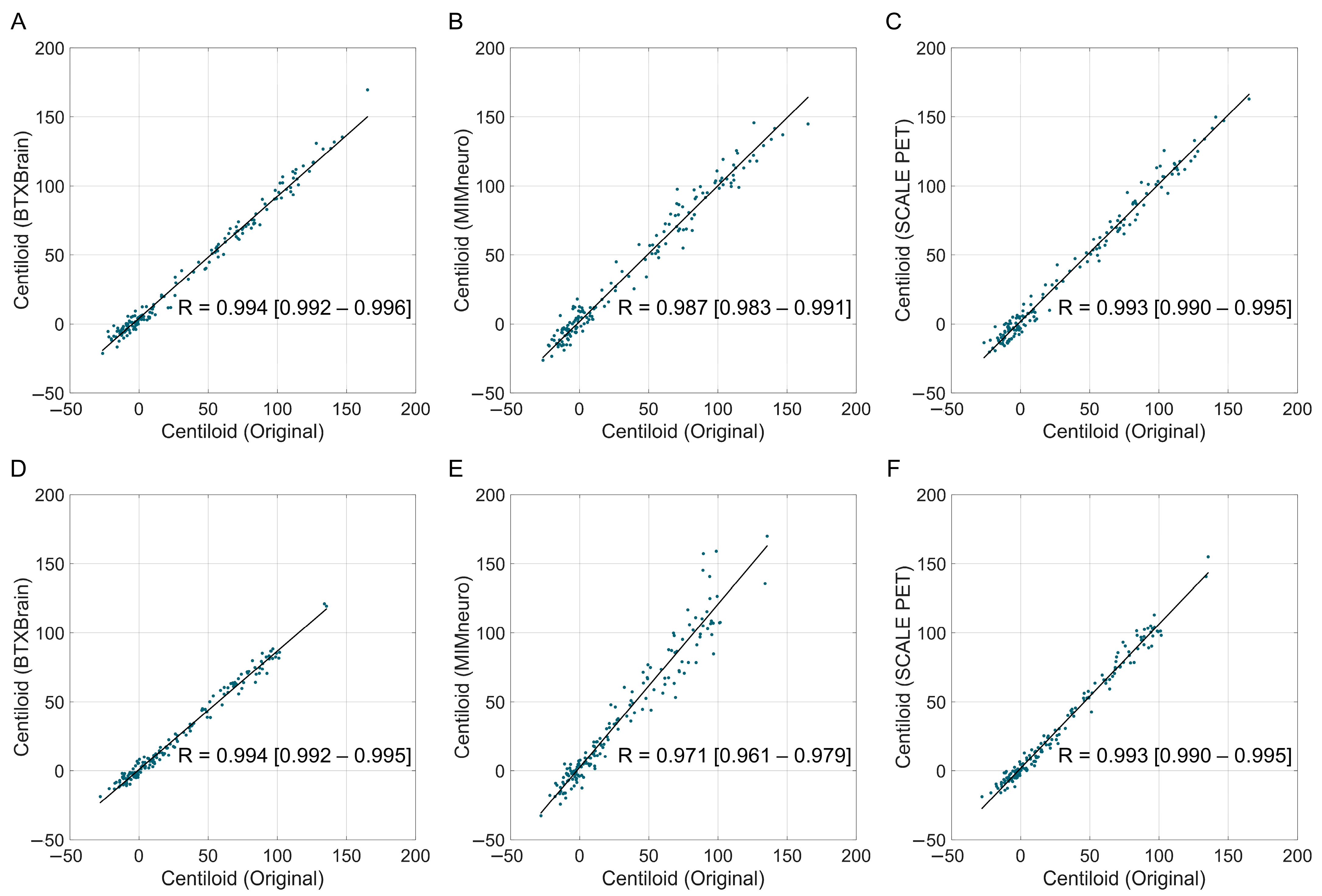
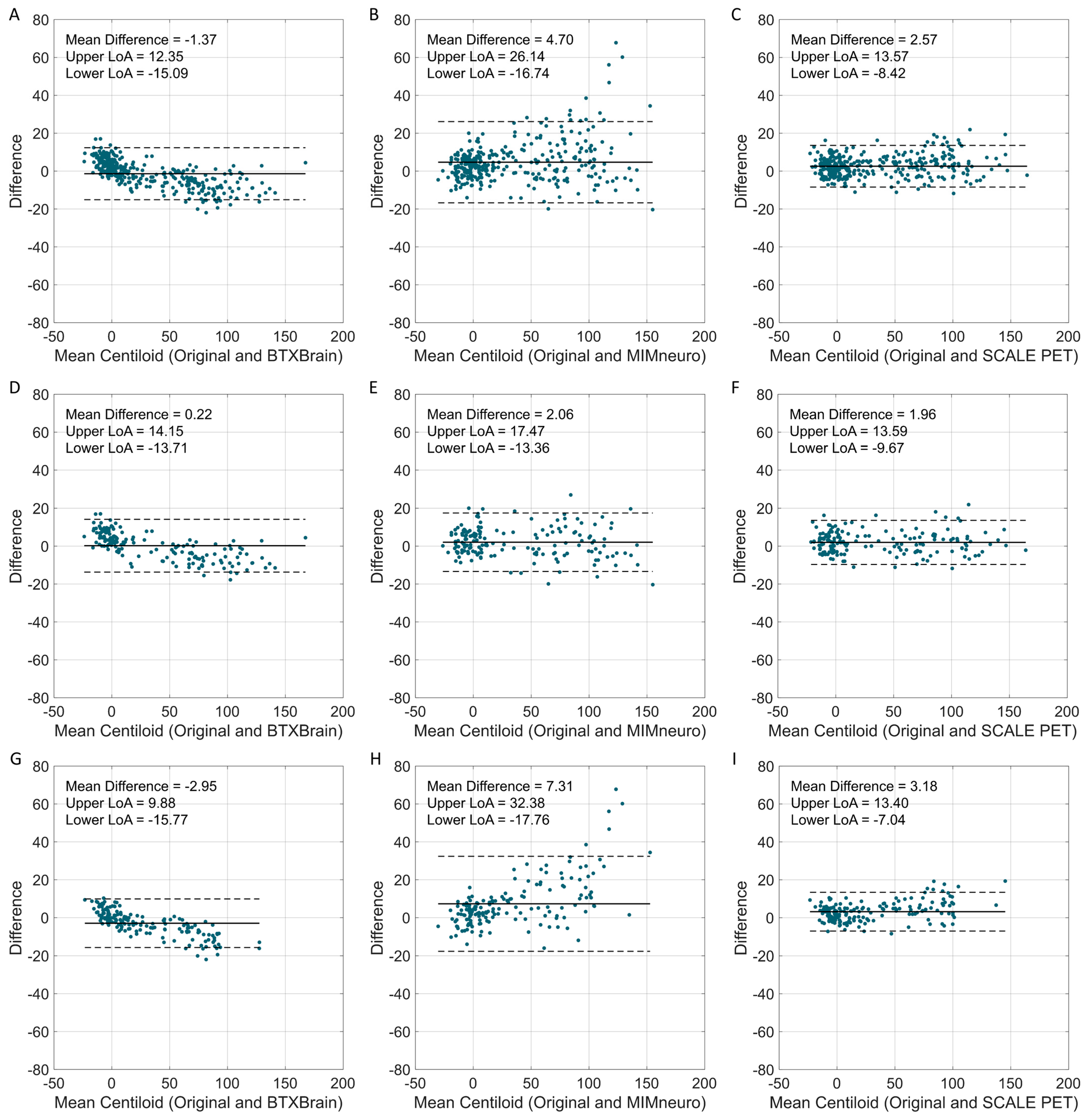
3.2. The Agreement of Software-Based Centiloid with the Reference
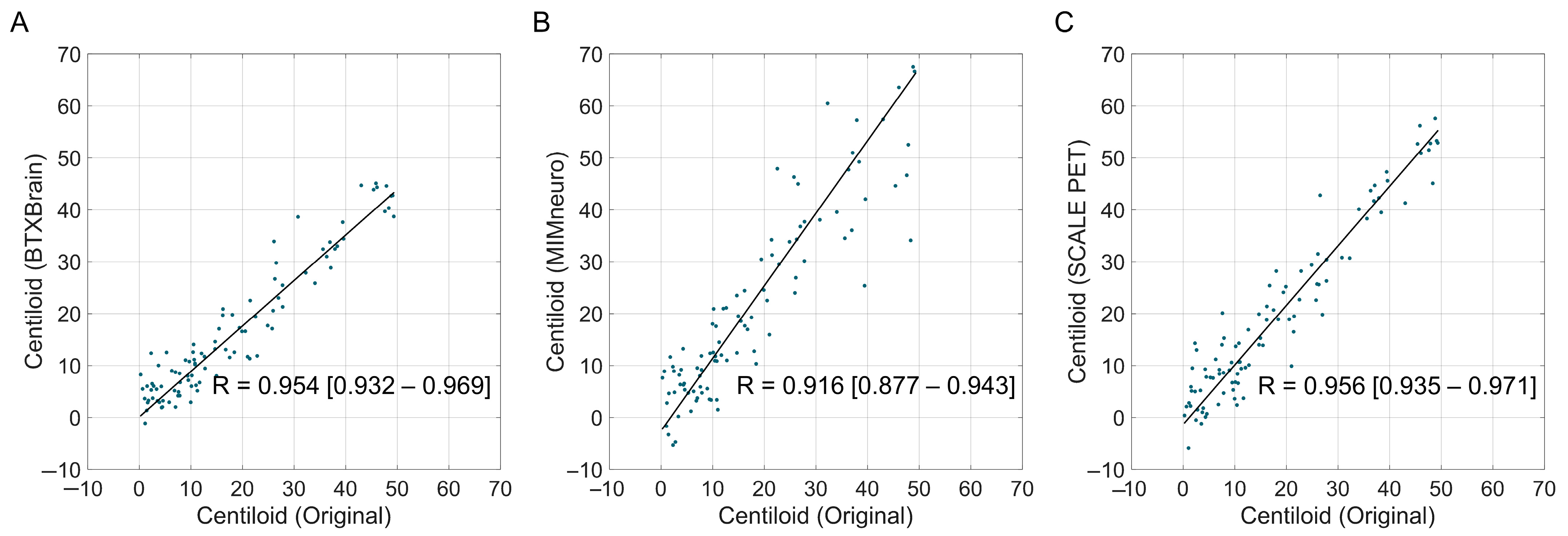
3.3. The Agreement of Software-Based Centiloid with the Original Method According to Centiloid Levels
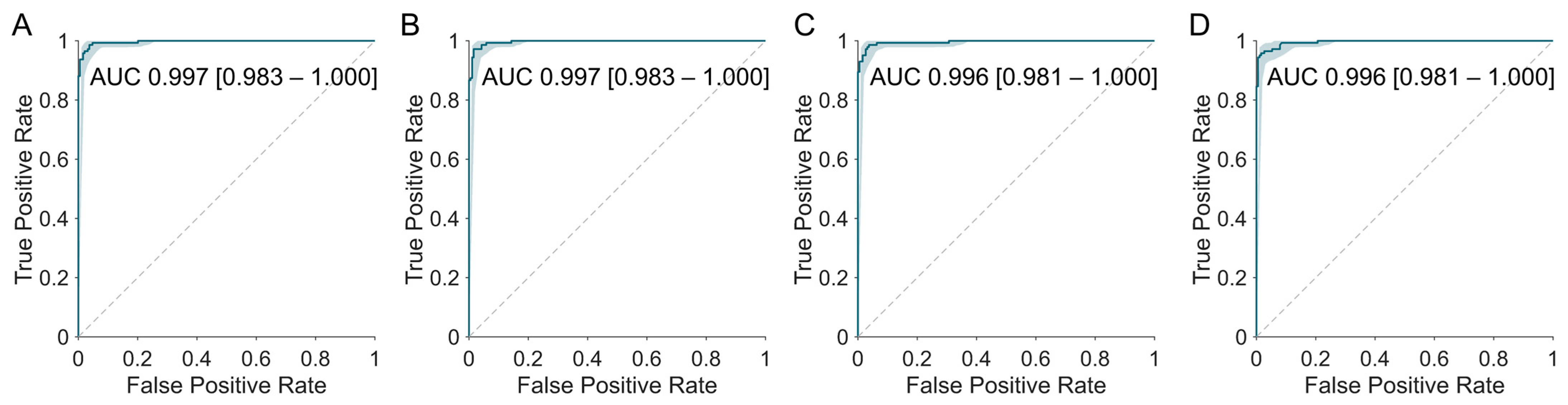
3.4. Agreement with Visual Interpretation Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AD | Alzheimer’s disease |
| FBB | [18F]Florbetaben |
| FMM | [18F]Flutemetamol |
| FDA | Food and Drug Administration |
| SUVR | Standardized uptake value ratio |
| GAAIN | Global Alzheimer’s Association Interactive Network |
| WC | Whole cerebellum |
| MNI | Montreal Neurological Institute |
| AI | Artificial intelligence |
| ICC | Intraclass correlation coefficient |
| ROC | Receiver operating characteristic |
| CDR-SB | Clinical Dementia Rating–Sum of Boxes |
| LoAs | Limits of agreement |
| AUROC | Area under the ROC curve |
References
- Therriault, J.; Schindler, S.E.; Salvadó, G.; Pascoal, T.A.; Benedet, A.L.; Ashton, N.J.; Karikari, T.K.; Apostolova, L.; Murray, M.E.; Verberk, I.; et al. Biomarker-based staging of Alzheimer disease: Rationale and clinical applications. Nat. Rev. Neurol. 2024, 20, 232–244. [Google Scholar] [CrossRef]
- Chapleau, M.; Iaccarino, L.; Soleimani-Meigooni, D.; Rabinovici, G.D. The Role of Amyloid PET in Imaging Neurodegenerative Disorders: A Review. J. Nucl. Med. 2022, 63, 13S–19S. [Google Scholar] [CrossRef]
- Minoshima, S.; Drzezga, A.E.; Barthel, H.; Bohnen, N.; Djekidel, M.; Lewis, D.H.; Mathis, C.A.; McConathy, J.; Nordberg, A.; Sabri, O.; et al. SNMMI Procedure Standard/EANM Practice Guideline for Amyloid PET Imaging of the Brain 1.0. J. Nucl. Med. 2016, 57, 1316–1322. [Google Scholar] [CrossRef]
- Morris, E.; Chalkidou, A.; Hammers, A.; Peacock, J.; Summers, J.; Keevil, S. Diagnostic accuracy of 18F amyloid PET tracers for the diagnosis of Alzheimer’s disease: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 374–385. [Google Scholar] [CrossRef]
- Klunk, W.E.; Koeppe, R.A.; Price, J.C.; Benzinger, T.L.; Devous, M.D.; Jagust, W.J.; Johnson, K.A.; Mathis, C.A.; Minhas, D.; Pontecorvo, M.J.; et al. The Centiloid Project: Standardizing quantitative amyloid plaque estimation by PET. Alzheimer’s Dement. 2015, 11, 1–15.e14. [Google Scholar] [CrossRef] [PubMed]
- Battle, M.R.; Pillay, L.C.; Lowe, V.J.; Knopman, D.; Kemp, B.; Rowe, C.C.; Doré, V.; Villemagne, V.L.; Buckley, C.J. Centiloid scaling for quantification of brain amyloid with [18F]flutemetamol using multiple processing methods. EJNMMI Res. 2018, 8, 107. [Google Scholar] [CrossRef]
- Rowe, C.C.; Doré, V.; Jones, G.; Baxendale, D.; Mulligan, R.S.; Bullich, S.; Stephens, A.W.; De Santi, S.; Masters, C.L.; Dinkelborg, L.; et al. 18F-Florbetaben PET beta-amyloid binding expressed in Centiloids. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 2053–2059. [Google Scholar] [CrossRef] [PubMed]
- Navitsky, M.; Joshi, A.D.; Kennedy, I.; Klunk, W.E.; Rowe, C.C.; Wong, D.F.; Pontecorvo, M.J.; Mintun, M.A.; Devous, M.D., Sr. Standardization of amyloid quantitation with florbetapir standardized uptake value ratios to the Centiloid scale. Alzheimer’s Dement. 2018, 14, 1565–1571. [Google Scholar] [CrossRef]
- Joshi, A.D.; Pontecorvo, M.J.; Lu, M.; Skovronsky, D.M.; Mintun, M.A.; Devous, M.D. A Semiautomated Method for Quantification of F 18 Florbetapir PET Images. J. Nucl. Med. 2015, 56, 1736–1741. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, H.G.; Collij, L.E.; Heeman, F.; Bollack, A.; Shekari, M.; Salvadó, G.; Alves, I.L.; Garcia, D.V.; Battle, M.; Buckley, C.; et al. Quantification of amyloid PET for future clinical use: A state-of-the-art review. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3508–3528. [Google Scholar] [CrossRef]
- Collij, L.E.; Bollack, A.; La Joie, R.; Shekari, M.; Bullich, S.; Roé-Vellvé, N.; Koglin, N.; Jovalekic, A.; Garciá, D.V.; Drzezga, A.; et al. Centiloid recommendations for clinical context-of-use from the AMYPAD consortium. Alzheimer’s Dement. 2024, 20, 9037–9048. [Google Scholar] [CrossRef]
- Jagust, W.J.; Mattay, V.S.; Krainak, D.M.; Wang, S.-J.; Weidner, L.D.; Hofling, A.A.; Koo, H.; Hsieh, P.; Kuo, P.H.; Farrar, G.; et al. Quantitative Brain Amyloid PET. J. Nucl. Med. 2024, 65, 670–678. [Google Scholar] [CrossRef]
- Van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 388, 9–21. [Google Scholar] [CrossRef]
- Sims, J.R.; Zimmer, J.A.; Evans, C.D.; Lu, M.; Ardayfio, P.; Sparks, J.; Wessels, A.M.; Shcherbinin, S.; Wang, H.; Monkul Nery, E.S.; et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. JAMA 2023, 330, 512–527. [Google Scholar] [CrossRef]
- Mintun, M.A.; Lo, A.C.; Evans, C.D.; Wessels, A.M.; Ardayfio, P.A.; Andersen, S.W.; Shcherbinin, S.; Sparks, J.; Sims, J.R.; Brys, M.; et al. Donanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2021, 384, 1691–1704. [Google Scholar] [CrossRef]
- Hutton, C.; Declerck, J.; Mintun, M.A.; Pontecorvo, M.J.; Devous, M.D.; Joshi, A.D.; for the Alzheimer’s Disease Neuroimaging Initiative. Quantification of 18F-florbetapir PET: Comparison of two analysis methods. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 725–732. [Google Scholar] [CrossRef]
- Choi, W.H.; Um, Y.H.; Jung, W.S.; Kim, S.H. Automated quantification of amyloid positron emission tomography: A comparison of PMOD and MIMneuro. Ann. Nucl. Med. 2016, 30, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Landau, S.M.; Ward, T.J.; Murphy, A.; Iaccarino, L.; Harrison, T.M.; La Joie, R.; Baker, S.; Koeppe, R.A.; Jagust, W.J.; Alzheimer’s Disease Neuroimaging Initiative. Quantification of amyloid beta and tau PET without a structural MRI. Alzheimer’s Dement. 2023, 19, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Jovalekic, A.; Roé-Vellvé, N.; Koglin, N.; Quintana, M.L.; Nelson, A.; Diemling, M.; Lilja, J.; Gómez-González, J.P.; Doré, V.; Bourgeat, P.; et al. Validation of quantitative assessment of florbetaben PET scans as an adjunct to the visual assessment across 15 software methods. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3276–3289. [Google Scholar] [CrossRef] [PubMed]
- Roh, H.W.; Son, S.J.; Hong, C.H.; Moon, S.Y.; Lee, S.M.; Seo, S.W.; Choi, S.H.; Kim, E.-J.; Cho, S.H.; Kim, B.C.; et al. Comparison of automated quantification of amyloid deposition between PMOD and Heuron. Sci. Rep. 2023, 13, 9891. [Google Scholar] [CrossRef]
- Kim, S.; Wang, S.-M.; Kang, D.W.; Um, Y.H.; Han, E.J.; Park, S.Y.; Ha, S.; Choe, Y.S.; Kim, H.W.; Kim, R.E.; et al. A Comparative Analysis of Two Automated Quantification Methods for Regional Cerebral Amyloid Retention: PET-Only and PET-and-MRI-Based Methods. Int. J. Mol. Sci. 2024, 25, 7649. [Google Scholar] [CrossRef] [PubMed]
- Shang, C.; Sakurai, K.; Nihashi, T.; Arahata, Y.; Takeda, A.; Ishii, K.; Ishii, K.; Matsuda, H.; Ito, K.; Kato, T.; et al. Comparison of consistency in centiloid scale among different analytical methods in amyloid PET: The CapAIBL, VIZCalc, and Amyquant methods. Ann. Nucl. Med. 2024, 38, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.K.; Kim, D.; Shin, S.A.; Kim, Y.K.; Choi, H.; Lee, J.S. Fast and Accurate Amyloid Brain PET Quantification Without MRI Using Deep Neural Networks. J. Nucl. Med. 2023, 64, 659–666. [Google Scholar] [CrossRef]
- Clark, C.M.; Schneider, J.A.; Bedell, B.J.; Beach, T.G.; Bilker, W.B.; Mintun, M.A.; Pontecorvo, M.J.; Hefti, F.; Carpenter, A.P.; Flitter, M.L.; et al. Use of Florbetapir-PET for Imaging β-Amyloid Pathology. JAMA 2011, 305, 275–283. [Google Scholar] [CrossRef]
- Lee, J.; Ha, S.; Kim, R.E.Y.; Lee, M.; Kim, D.; Lim, H.K. Development of Amyloid PET Analysis Pipeline Using Deep Learning-Based Brain MRI Segmentation—A Comparative Validation Study. Diagnostics 2022, 12, 623. [Google Scholar] [CrossRef]
- Rowe, C.C.; Jones, G.; Doré, V.; Pejoska, S.; Margison, L.; Mulligan, R.S.; Chan, J.G.; Young, K.; Villemagne, V.L. Standardized Expression of 18F-NAV4694 and 11C-PiB β-Amyloid PET Results with the Centiloid Scale. J. Nucl. Med. 2016, 57, 1233–1237. [Google Scholar] [CrossRef]
- Collij, L.E.; Salvadó, G.; de Wilde, A.; Altomare, D.; Shekari, M.; Gispert, J.D.; Bullich, S.; Stephens, A.; Barkhof, F.; Scheltens, P.; et al. Quantification of [18F]florbetaben amyloid-PET imaging in a mixed memory clinic population: The ABIDE project. Alzheimer’s Dement. 2023, 19, 2397–2407. [Google Scholar] [CrossRef]
- Collij, L.E.; Salvadó, G.; Shekari, M.; Lopes Alves, I.; Reimand, J.; Wink, A.M.; Zwan, M.; Niñerola-Baizán, A.; Perissinotti, A.; Scheltens, P.; et al. Visual assessment of [18F]flutemetamol PET images can detect early amyloid pathology and grade its extent. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2169–2182. [Google Scholar] [CrossRef]
- Farrell, M.E.; Jiang, S.; Schultz, A.P.; Properzi, M.J.; Price, J.C.; Becker, J.A.; Jacobs, H.I.L.; Hanseeuw, B.J.; Rentz, D.M.; Villemagne, V.L.; et al. Defining the Lowest Threshold for Amyloid-PET to Predict Future Cognitive Decline and Amyloid Accumulation. Neurology 2021, 96, e619–e631. [Google Scholar] [CrossRef]
- Bollack, A.; Collij, L.E.; García, D.V.; Shekari, M.; Altomare, D.; Payoux, P.; Dubois, B.; Grau-Rivera, O.; Boada, M.; Marquié, M.; et al. Investigating reliable amyloid accumulation in Centiloids: Results from the AMYPAD Prognostic and Natural History Study. Alzheimer’s Dement. 2024, 20, 3429–3441. [Google Scholar] [CrossRef] [PubMed]
- Bateman, R.J.; Smith, J.; Donohue, M.C.; Delmar, P.; Abbas, R.; Salloway, S.; Wojtowicz, J.; Blennow, K.; Bittner, T.; Black, S.E.; et al. Two Phase 3 Trials of Gantenerumab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 389, 1862–1876. [Google Scholar] [CrossRef]
- Budd Haeberlein, S.; Aisen, P.S.; Barkhof, F.; Chalkias, S.; Chen, T.; Cohen, S.; Dent, G.; Hansson, O.; Harrison, K.; von Hehn, C.; et al. Two Randomized Phase 3 Studies of Aducanumab in Early Alzheimer’s Disease. J. Prev. Alzheimer’s Dis. 2022, 9, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Andrews, J.S.; Beach, T.G.; Buracchio, T.; Dunn, B.; Graf, A.; Hansson, O.; Ho, C.; Jagust, W.; McDade, E.; et al. Revised criteria for diagnosis and staging of Alzheimer’s disease: Alzheimer’s Association Workgroup. Alzheimer’s Dement. 2024, 20, 5143–5169. [Google Scholar] [CrossRef]
- Rabinovici, G.D.; Knopman, D.S.; Arbizu, J.; Benzinger, T.L.S.; Donohoe, K.J.; Hansson, O.; Herscovitch, P.; Kuo, P.H.; Lingler, J.H.; Minoshima, S.; et al. Updated appropriate use criteria for amyloid and tau PET: A report from the Alzheimer’s Association and Society for Nuclear Medicine and Molecular Imaging Workgroup. Alzheimer’s Dement. 2025, 21, e14338. [Google Scholar] [CrossRef]
- Park, K.W. Anti-amyloid Antibody Therapies for Alzheimer’s Disease. Nucl. Med. Mol. Imaging 2024, 58, 227–236. [Google Scholar] [CrossRef]
- Kang, S.K.; Heo, M.; Chung, J.Y.; Kim, D.; Shin, S.A.; Choi, H.; Chung, A.; Ha, J.-M.; Kim, H.; Lee, J.S. Clinical Performance Evaluation of an Artificial Intelligence-Powered Amyloid Brain PET Quantification Method. Nucl. Med. Mol. Imaging 2024, 58, 246–254. [Google Scholar] [CrossRef]
- Hanseeuw, B.J.; Malotaux, V.; Dricot, L.; Quenon, L.; Sznajer, Y.; Cerman, J.; Woodard, J.L.; Buckley, C.; Farrar, G.; Ivanoiu, A.; et al. Defining a Centiloid scale threshold predicting long-term progression to dementia in patients attending the memory clinic: An [18F] flutemetamol amyloid PET study. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Royse, S.K.; Minhas, D.S.; Lopresti, B.J.; Murphy, A.; Ward, T.; Koeppe, R.A.; Bullich, S.; DeSanti, S.; Jagust, W.J.; Landau, S.M.; et al. Validation of amyloid PET positivity thresholds in centiloids: A multisite PET study approach. Alzheimers Res. Ther. 2021, 13, 99. [Google Scholar] [CrossRef] [PubMed]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Platforms | Metrics | Key Findings | Limitations | Ref. |
|---|---|---|---|---|---|
| C Hutton et al. (2015) | SPM; Syngo.via | SUVR | Good overall agreement | No Centiloid calculation; single new platform | [16] |
| WH Choi et al. (2016) | PMOD; MIMneuro | SUVR | Good overall agreement; regional difference | No Centiloid calculation; Single new platform | [17] |
| MR Battle et al. (2018) | SPM; PMOD; FSL | SUVR; Centiloid | Centiloid conversion equation according to each platform | Confined to conventional research platforms | [6] |
| SM Landau et al. (2022) | FreeSurfer; SPM | SUVR | Good overall agreement between MRI-dependent and MRI-free processing | Confined to conventional research platforms; no Centiloid calculation | [18] |
| A Jovalekic et al. (2023) | 15 platforms (6 for Centiloid) | SUVR; Centiloid | Descriptive analysis of values from each platform | No evaluation of correlation or inter-platform agreement | [19] |
| HW Roh et al. (2023) | PMOD; Heuron | SUVR | Good overall agreement | No Centiloid calculation; single new platform | [20] |
| S Kim et al. (2024) | Syngo.via; SCALE PET | SUVR | High predictive value for visual interpretation results in both platforms | No Centiloid calculation; no comparison with reference | [21] |
| C Shang et al. (2024) | CapAIBL; VIZCalc; Amyquant | Centiloid | Strong correlations among values using the three methods | No comparison with reference | [22] |
| Factor | Florbetaben (n = 165) | Flutemetamol (n = 167) | Total (n = 332) | t/χ2 | p |
|---|---|---|---|---|---|
| Age (year) | 74.0 ± 7.8 | 73.8 ± 7.2 | 73.9 ± 7.5 | −0.247 | 0.805 |
| Sex (male/female) | 59:106 | 48:119 | 107:225 | 1.563 | 0.211 |
| CDR-SB | 3.86 ± 3.72 | 3.87 ± 3.13 | 3.87 ± 3.44 | 0.021 | 0.983 |
| Positive amyloid scan * | 73 (44.2%) | 70 (41.9%) | 143 (47.0%) | 0.101 | 0.751 |
| Centiloid values | 35.9 ± 49.2 | 28.8 ± 38.4 | 32.3 ± 44.2 | −1.456 | 0.146 |
| Method | Slope | Intercept | R | ICC | p * |
|---|---|---|---|---|---|
| Total (n = 332) | |||||
| BTXBrain | 0.872 [0.860–0.885] | 2.702 [2.308–2.967] | 0.993 [0.991–0.994] | 0.986 [0.982–0.989] | <0.001 |
| MIMneuro | 1.053 [1.026–1.081] | 2.297 [1.904–2.778] | 0.974 [0.967–0.979] | 0.966 [0.944–0.978] | <0.001 |
| SCALE PET | 1.014 [0.999–1.029] | 2.288 [1.659–2.571] | 0.992 [0.990–0.994] | 0.991 [0.983–0.994] | <0.001 |
| Florbetaben (n = 165) | |||||
| BTXBrain | 0.883 [0.867–0.899] | 4.195 [3.563–4.859] | 0.994 [0.992–0.996] | 0.989 [0.984–0.992] | <0.001 |
| MIMneuro | 0.984 [0.959–1.009] | 1.731 [0.920–2.243] | 0.987 [0.983–0.991] | 0.986 [0.980–0.990] | <0.001 |
| SCALE PET | 0.996 [0.976–1.015] | 1.870 [1.457–2.501] | 0.993 [0.990–0.995] | 0.992 [0.988–0.995] | <0.001 |
| Flutemetamol (n = 167) | |||||
| BTXBrain | 0.859 [0.842–0.877] | 0.932 [0.667–1.345] | 0.994 [0.992–0.995] | 0.980 [0.964–0.988] | <0.001 |
| MIMneuro | 1.182 [1.130–1.231] | 2.531 [1.770–2.550] | 0.971 [0.961–0.979] | 0.941 [0.868–0.968] | <0.001 |
| SCALE PET | 1.044 [1.022–1.067] | 1.893 [1.012–2.595] | 0.993 [0.990–0.995] | 0.988 [0.969–0.944] | <0.001 |
| Method | Slope | Intercept | R | ICC | Mean Difference | p * |
|---|---|---|---|---|---|---|
| Total (n = 98) | ||||||
| BTXBrain | 0.876 [0.817–0.930] | 0.111 [−0.630–1.508] | 0.954 [0.932–0.969] | 0.942 [0.906–0.964] | −1.6 [−2.5–−0.7] | <0.001 |
| MIMneuro | 1.397 [1.261–1.507] | −2.562 [−4.803–−0.328] | 0.916 [0.877–0.943] | 0.853 [0.740–0.912] | 4.0 [2.3–5.7] | <0.001 |
| SCALE PET | 1.147 [1.078–1.210] | −1.339 [−2.482–0.397] | 0.956 [0.935–0.971] | 0.944 [0.911–0.964] | 1.6 [0.6–2.6] | <0.001 |
| Florbetaben (n = 35) | ||||||
| BTXBrain | 0.922 [0.776–1.093] | 2.375 [0.199–3.498] | 0.935 [0.874–0.967] | 0.933 [0.871–0.965] | 0.5 [−1.3–2.2] | <0.001 |
| MIMneuro | 1.104 [0.877–1.390] | −1.105 [−4.450–1.808] | 0.886 [0.785–0.942] | 0.887 [0.788–0.941] | 0.6 [−1.8–3.0] | <0.001 |
| SCALE PET | 1.155 [0.978–1.355] | −0.219 [−3.112–1.930] | 0.921 [0.849–0.960] | 0.912 [0.833–0.955] | 1.6 [−0.5–3.7] | <0.001 |
| Flutemetamol (n = 63) | ||||||
| BTXBrain | 0.890 [0.826–0.941] | −0.843 [−1.765–1.016] | 0.971 [0.953–0.983] | 0.948 [0.812–0.978] | −2.7 [−3.6–−1.8] | <0.001 |
| MIMneuro | 1.436 [1.318–1.584] | −2.078 [−5.554–−0.128] | 0.941 [0.904–0.964] | 0.838 [0.597–0.922] | 5.9 [3.6–8.1] | <0.001 |
| SCALE PET | 1.146 [1.074–1.215] | −1.684 [−2.917–0.567] | 0.973 [0.956–0.984] | 0.959 [0.926–0.977] | 1.6 [0.6–2.7] | <0.001 |
| Method | AUROC | Optimal Cutoff | Sensitivity | Specificity | Cutoff for 99% Sensitivity | Cutoff for 99% Specificity |
|---|---|---|---|---|---|---|
| Original | 0.997 [0.983–1.000] | 21.4 | 0.986 [0.950–0.998] | 0.963 [0.925–0.985] | 19.9 | 30.8 |
| BTXBrain | 0.997 [0.983–1.000] | 21.3 | 0.972 [0.930–0.992] | 0.984 [0.954–0.997] | 16.6 | 37.6 |
| MIMneuro | 0.996 [0.981–1.000] | 28.2 | 0.986 [0.950–0.998] | 0.963 [0.925–0.985] | 21.1 | 38.1 |
| SCALE PET | 0.996 [0.981–1.000] | 25.4 | 0.958 [0.911–0.984] | 0.984 [0.954–0.997] | 18.8 | 30.8 |
| Method | Agreement with Reference | Proportional Bias | Concordance with Visual Reading |
|---|---|---|---|
| BTXBrain | R = 0.993, ICC = 0.986 for all; R= 0.994, ICC = 0.989 for FBB; R = 0.994, ICC = 0.980 for FMM | Slope = 0.872 for all; Slope = 0.883 for FBB; Slope = 0.859 for FMM. | AUROC 0.997 |
| MIMneuro | R = 0.974, ICC = 0.966 for all; R = 0.987, ICC = 0.986 for FBB; R = 0.971, ICC = 0.941 for FBB | Slope = 1.053 for all; Slope = 0.984 for FBB; Slope = 1.182 for FMM | AUROC 0.996 |
| SCALE PET | R = 0.992, ICC = 0.991 for all; R = 0.993, ICC = 0.992 for FBB; R = 0.993, ICC = 0.988 for FMM | Slope = 1.014 for all; Slope = 0.996 for FBB; Slope = 1.044 for FMM | AUROC 0.996 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, Y.-k.; Min, J.W.; Kwon, S.J.; Ha, S. Reliability of Automated Amyloid PET Quantification: Real-World Validation of Commercial Tools Against Centiloid Project Method. Tomography 2025, 11, 86. https://doi.org/10.3390/tomography11080086
Kang Y-k, Min JW, Kwon SJ, Ha S. Reliability of Automated Amyloid PET Quantification: Real-World Validation of Commercial Tools Against Centiloid Project Method. Tomography. 2025; 11(8):86. https://doi.org/10.3390/tomography11080086
Chicago/Turabian StyleKang, Yeon-koo, Jae Won Min, Soo Jin Kwon, and Seunggyun Ha. 2025. "Reliability of Automated Amyloid PET Quantification: Real-World Validation of Commercial Tools Against Centiloid Project Method" Tomography 11, no. 8: 86. https://doi.org/10.3390/tomography11080086
APA StyleKang, Y.-k., Min, J. W., Kwon, S. J., & Ha, S. (2025). Reliability of Automated Amyloid PET Quantification: Real-World Validation of Commercial Tools Against Centiloid Project Method. Tomography, 11(8), 86. https://doi.org/10.3390/tomography11080086