
Four-Dimensional Dual-Energy Computed Tomography-Derived Parameters and Their Correlation with Thyroid Gland Functional Status


Abstract
1. Introduction
2. Methods
2.1. Patient Selection
2.2. Imaging Technique
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Correlation Between Thyroid Density and Thyroid Function: Thyroid Density on Non-Contrast CT Scans (SECT + DECT (Mixed)) and TSH/FT4
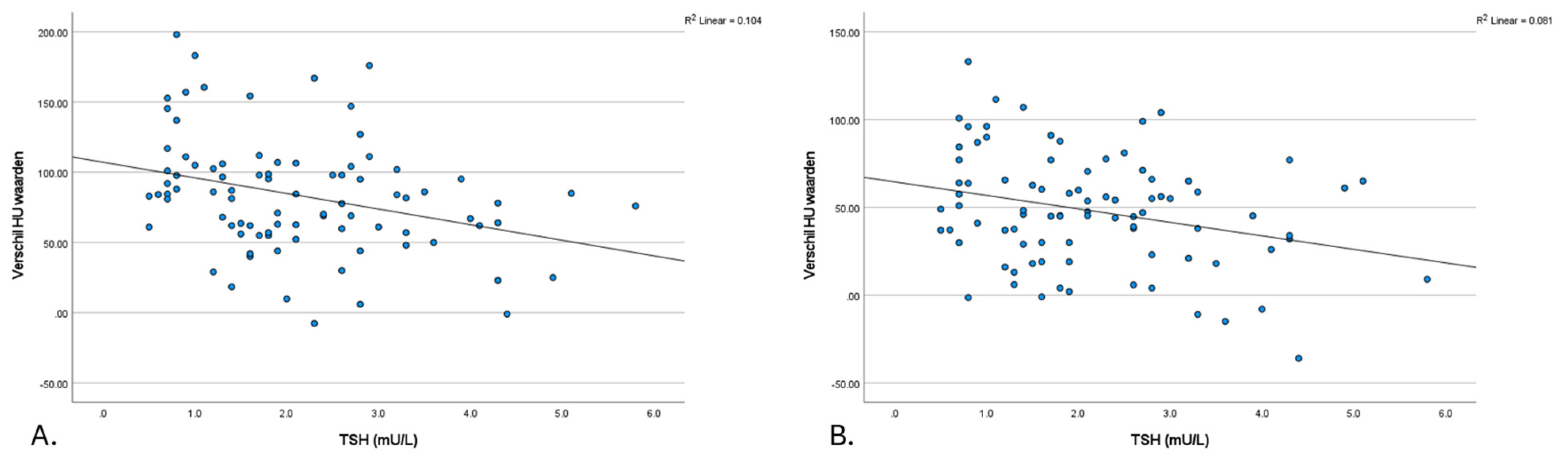
3.2. Thyroid Density Changes (ΔHU): Correlations with TSH
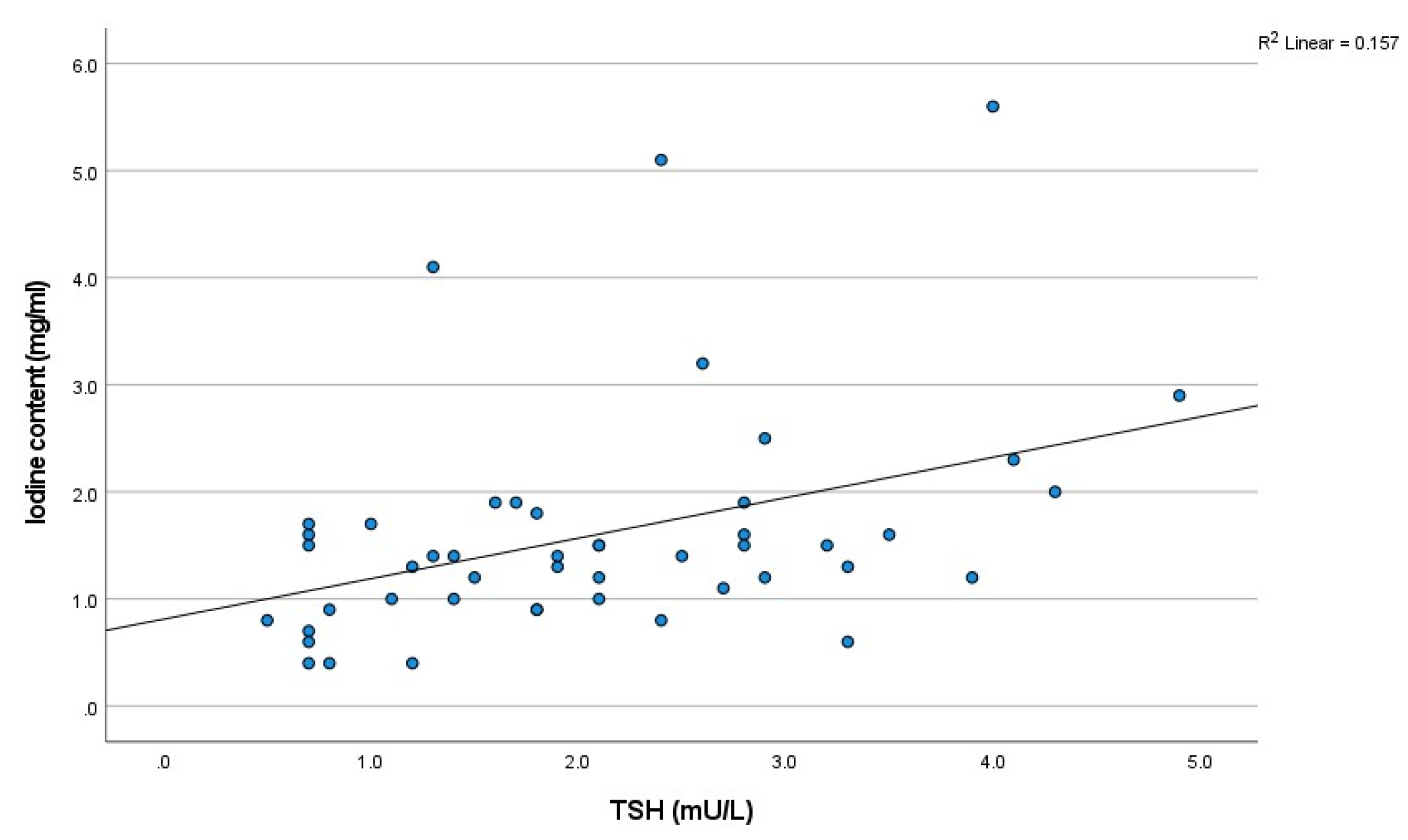
3.3. Iodine Concentration in Thyroid: Correlation with TSH
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheehan, M.T. Biochemical Testing of the Thyroid: TSH is the Best and, Oftentimes, Only Test Needed—A Review for Primary Care. Clin. Med. Res. 2016, 14, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Yazdaan, H.E.; Jaya, F.; Sanjna, F.; Junaid, M.; Rasool, S.; Baig, A.; Natt, M.Z.; Maurya, N.; Iqbal, S.; Yeldo, B.A.; et al. Advances in Thyroid Function Tests: Precision Diagnostics and Clinical Implications. Cureus 2023, 15, e48961. [Google Scholar] [CrossRef] [PubMed]
- Brent, G.A. Mechanisms of thyroid hormone action. J. Clin. Investig. 2012, 122, 3035–3043. [Google Scholar] [CrossRef] [PubMed]
- Lisco, G.; De Tullio, A.; Triggiani, D.; Zupo, R.; Giagulli, V.A.; De Pergola, G.; Guastamacchia, E.; Sabbà, C.; Triggiani, V. Iodine Deficiency and Iodine Prophylaxis: An Overview and Update. Nutrients 2023, 15, 1004. [Google Scholar] [CrossRef]
- Imanishi, Y.; Ehara, N.; Shinagawa, T.; Tsujino, D.; Endoh, I.; Baba, K.; Kanemaki, Y.; Iida, S.; Hayakawa, M.; Miyazaki, O.; et al. Correlation of CT Values, Iodine Concentration, and Histological Changes in the Thyroid. J. Comput. Assist. Tomogr. 2000, 24, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, M.H.; Scholtz, J.E.; Kraft, J.; Bauer, R.W.; Kaup, M.; Dewes, P.; Bucher, A.M.; Burck, I.; Wagenblast, J.; Lehnert, T.; et al. Assessment of an Advanced Monoenergetic Reconstruction Technique in Dual-Energy Computed Tomography of Head and Neck Cancer. Eur. Radiol. 2015, 25, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Forghani, R.; Roskies, M.; Liu, X.; Tan, X.; Mlynarek, A.; Payne, R.J.; Nair, J.R.; Hier, M.P.; Levental, M. Dual-Energy CT Characteristics of Parathyroid Adenomas on 25-and 55-Second 4D-CT Acquisitions: Preliminary Experience. J. Comput. Assist. Tomogr. 2016, 40, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.Y.; Zhang, X.Y.; Wei, W.; Li, X.T.; Li, Y.L.; Xu, M.; Sun, Y.S.; Zhang, X.P. Identification of benign and malignant thyroid nodules by in vivo iodine concentration measurement using single-source dual energy CT: A retrospective diagnostic accuracy study. Medicine 2016, 95, e4816. [Google Scholar] [CrossRef] [PubMed]
- Vogl, T.J.; Schulz, B.; Bauer, R.W.; Stöver, T.; Sader, R.; Tawfik, A.M. Dual-energy CT applications in head and neck imaging. AJR Am. J. Roentgenol. 2012, 199, S34–S39. [Google Scholar] [CrossRef]
- Roskies, M.; Liu, X.; Hier, M.P.; Payne, R.J.; Mlynarek, A.; Forest, V.; Levental, M.; Forghani, R. 3-phase dual-energy CT scan as a feasible salvage imaging modality for the identification of non-localizing parathyroid adenomas: A prospective study. J. Otolaryngol. Head Neck Surg. 2015, 44, 44. [Google Scholar] [CrossRef]
- McCollough, C.H.; Leng, S.; Yu, L.; Fletcher, J.G. Dual- and Multi-Energy CT: Principles, Technical Approaches, and Clinical Applications. Radiology 2015, 276, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.; Bowden, D.J.; Shaida, N.; Godfrey, E.M.; Taylor, A.; Lomas, D.J.; Shaw, A.S. Virtual unenhanced second generation dual-source CT of the liver: Is it time to discard the conventional unenhanced phase? Eur. J. Radiol. 2012, 81, 1438–1445. [Google Scholar] [CrossRef] [PubMed]
- Roele, E.D.; Timmer, V.; Vaassen, L.A.A.; van Kroonenburgh, A.; Postma, A.A. Dual-Energy CT in Head and Neck Imaging. Curr. Radiol. Rep. 2017, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Pandey, V.; Reis, M.; Zhou, Y. Correlation Between Computed Tomography Density and Functional Status of the Thyroid Gland. J. Comput. Assist. Tomogr. 2016, 40, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Iida, Y.; Konishi, J.; Harioka, T.; Misaki, T.; Endo, K.; Torizuka, K. Thyroid CT number and its relationship to iodine concentration. Radiology 1983, 147, 793–795. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, B.; Nygaard, T.; Jensen, L.I.; Court-Payen, M.; Søe-Jensen, P.; Nielsen, K.G.; Fugl, M.; Hansen, J.M. Iohexol: Effects on uptake of radioactive iodine in the thyroid and on thyroid function. Acad. Radiol. 1998, 5, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Lautenschlaeger, I.E.; Hartmann, A.; Sicken, J.; Mohrs, S.; Scholz, V.B.; Neiger, R.; Kramer, M. Comparison between computed tomography and (99m)TC-pertechnetate scintigraphy characteristics of the thyroid gland in cats with hyperthyroidism. Vet. Radiol. Ultrasound 2013, 54, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Binh, D.D.; Nakajima, T.; Otake, H.; Higuchi, T.; Tsushima, Y. Iodine concentration calculated by dual-energy computed tomography (DECT) as a functional parameter to evaluate thyroid metabolism in patients with hyperthyroidism. BMC Med. Imaging 2017, 17, 43. [Google Scholar] [CrossRef]
- Kaneko, T.; Matsumoto, M.; Fukui, K.; Hori, T.; Katayama, K. Clinical evaluation of thyroid CT values in various thyroid conditions. J. Comput. Tomogr. 1979, 3, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Geng, D.; Zhou, Y.; Su, G.-Y.; Si, Y.; Shen, M.-P.; Xu, X.-Q.; Wu, F.-Y. Influence of sex, age and thyroid function indices on dual-energy computed tomography-derived quantitative parameters of thyroid in patients with or without Hashimoto’s thyroiditis. BMC Med. Imaging 2023, 23, 25. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.T.; Zhai, R.; Liu, H.M.; Wang, M.; Pan, D.M. Iodine concentration and content measured by dual-source computed tomography are correlated to thyroid hormone levels in euthyroid patients: A cross-sectional study in China. BMC Med. Imaging 2020, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Rousset, B.; Dupuy, C.; Miot, F.; Dumont, J. Chapter 2 Thyroid Hormone Synthesis and Secretion. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Hoermann, R.; Midgley, J.E.; Larisch, R.; Dietrich, J.W. Relational Stability in the Expression of Normality, Variation, and Control of Thyroid Function. Front. Endocrinol. 2016, 7, 142. [Google Scholar] [CrossRef]
- Bunch, P.M.; Pavlina, A.A.; Lipford, M.E.; Sachs, J.R. Dual-Energy Parathyroid 4D-CT: Improved Discrimination of Parathyroid Lesions from Thyroid Tissue Using Noncontrast 40-keV Virtual Monoenergetic Images. AJNR Am. J. Neuroradiol. 2021, 42, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Al-Difaie, Z.; Scheepers, M.H.; Bouvy, N.D.; Engelen, S.; Havekes, B.; Postma, A.A. Can virtual non-contrast imaging replace true non-contrast imaging in multiphase scanning of the neck region? Acta Radiol. Open 2023, 12, 20584601231205159. [Google Scholar] [CrossRef] [PubMed]
- Postma, A.A.; Das, M.; Stadler, A.A.; Wildberger, J.E. Dual-Energy CT: What the Neuroradiologist Should Know. Curr. Radiol. Rep. 2015, 3, 16. [Google Scholar] [CrossRef]
- Xu, Y.; Yan, B.; Zhang, J.; Chen, J.; Zeng, L.; Wang, L. Image Decomposition Algorithm for Dual-Energy Computed Tomography via Fully Convolutional Network. Comput. Math. Methods Med. 2018, 2018, 2527516. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 87) | TNC—SECT (n = 39) | TNC—DECT (n = 48) | |
|---|---|---|---|
| Age years (SD) | 63.7 (10.9) | 62.0 (11.9) | 65.1 (9.9) |
| Female % (N) | 81.6 (71) | 84.6 (33) | 79.2 (38) |
| TSH mU/L (SD) | 2.1 (1.2) | 2.2 (1.3) | 2.1 (1.1) |
| FT4 mU/L (SD) | 15.7 (3.0) | 15.6 (3.5) | 15.7 (2.7) |
| Euthyroid % (N) | 86.2 (75) | 76.9 (30) | 93.8 (45) |
| Hyperthyroidism % (N) | 1.1 (1) | 0 (0) | 2.1 (1) |
| Hypothyroidism % (N) | 12.6 (11) | 23.1 (9) | 4.2 (2) |
| TNC (n = 87) | TNC—SECT (n = 39) | TNC—DECT (n = 48) | |
|---|---|---|---|
| TSH mU/L | 2.1 (1.2) | 2.2 (1.3) | 2.1 (1.1) |
| Spearman’s Rho | 0.436 | 0.435 | 0.422 |
| p-value | <0.001 * | 0.006 * | 0.003 * |
| FT4 mU/L | 15.7 (3.0) | 15.6 (3.5) | 15.7 (2.7) |
| Spearman’s Rho | −0.302 | −0.389 | −0.191 |
| p-value | 0.078 | 0.169 | 0.406 |
| Iodine concentration mmol/L | 1.6 ± 1.1 | ||
| Spearman’s Rho | - | - | 0.745 |
| p-value | - | - | <0.001 * |
| VNC 30 | VNC 50 | |
|---|---|---|
| Thyroid density HU (SD) | 48.4 (15.4) | 50.1 (15.2) |
| TSH mU/L | 2.1 (1.2) | 2.1 (1.2) |
| Spearman’s Rho | −0.034 | 0.015 |
| p-value | 0.755 | 0.894 |
| FT4 mU/L | 15.7 (3.0) | 15.7 (3.0) |
| Spearman’s Rho | 0.288 | 0.138 |
| p-value | 0.093 | 0.429 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheepers, M.H.M.C.; Al-Difaie, Z.J.J.; Bouvy, N.D.; Havekes, B.; Postma, A.A. Four-Dimensional Dual-Energy Computed Tomography-Derived Parameters and Their Correlation with Thyroid Gland Functional Status. Tomography 2025, 11, 22. https://doi.org/10.3390/tomography11030022
Scheepers MHMC, Al-Difaie ZJJ, Bouvy ND, Havekes B, Postma AA. Four-Dimensional Dual-Energy Computed Tomography-Derived Parameters and Their Correlation with Thyroid Gland Functional Status. Tomography. 2025; 11(3):22. https://doi.org/10.3390/tomography11030022
Chicago/Turabian StyleScheepers, Max H. M. C., Zaid J. J. Al-Difaie, Nicole D. Bouvy, Bas Havekes, and Alida A. Postma. 2025. "Four-Dimensional Dual-Energy Computed Tomography-Derived Parameters and Their Correlation with Thyroid Gland Functional Status" Tomography 11, no. 3: 22. https://doi.org/10.3390/tomography11030022
APA StyleScheepers, M. H. M. C., Al-Difaie, Z. J. J., Bouvy, N. D., Havekes, B., & Postma, A. A. (2025). Four-Dimensional Dual-Energy Computed Tomography-Derived Parameters and Their Correlation with Thyroid Gland Functional Status. Tomography, 11(3), 22. https://doi.org/10.3390/tomography11030022