Anatomy of Maxillary Sinus: Focus on Vascularization and Underwood Septa via 3D Imaging

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Sample and Study Design
2.3. Evaluation of AAa
- The presence of the AAa in the antral wall of the maxillary sinus;
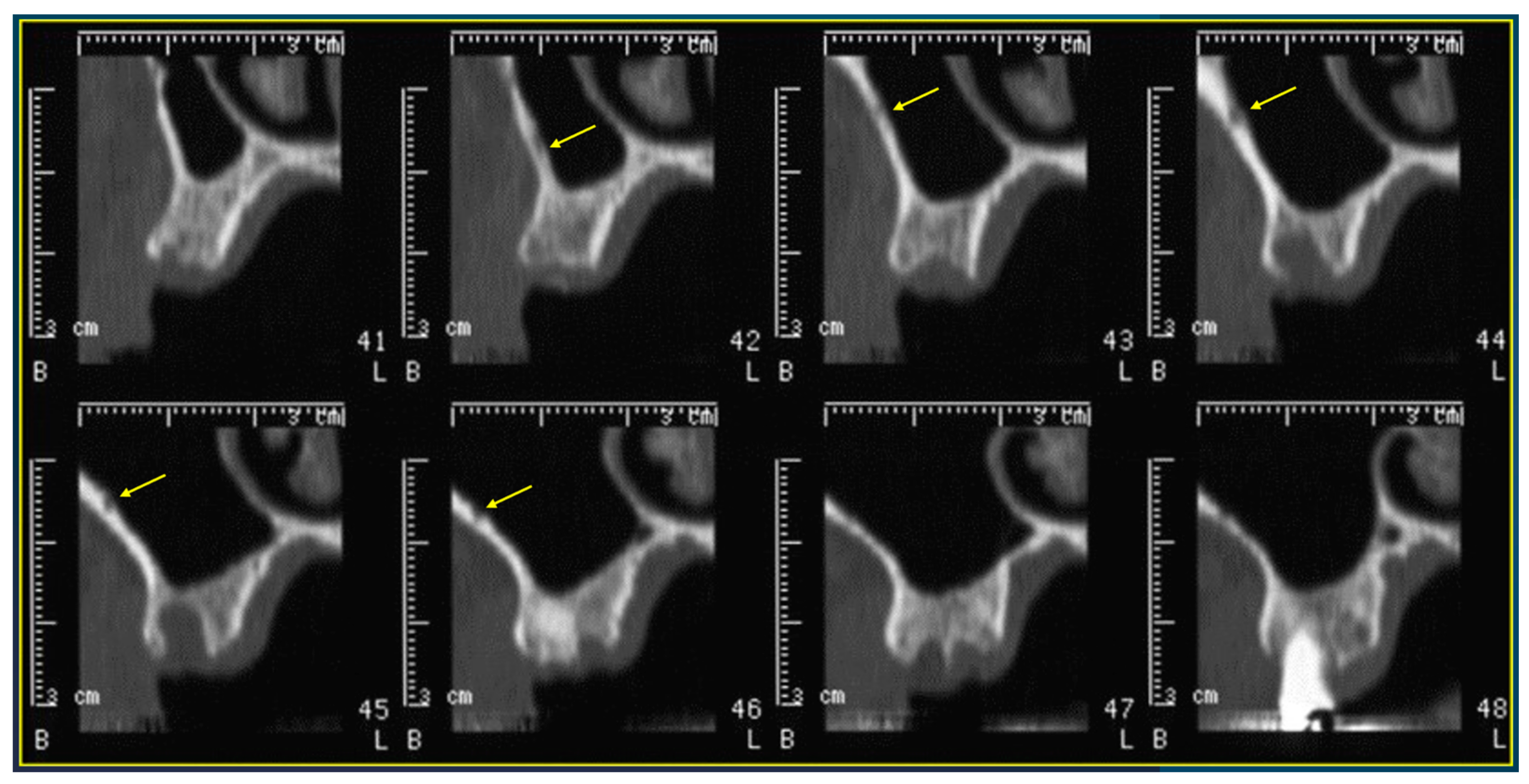
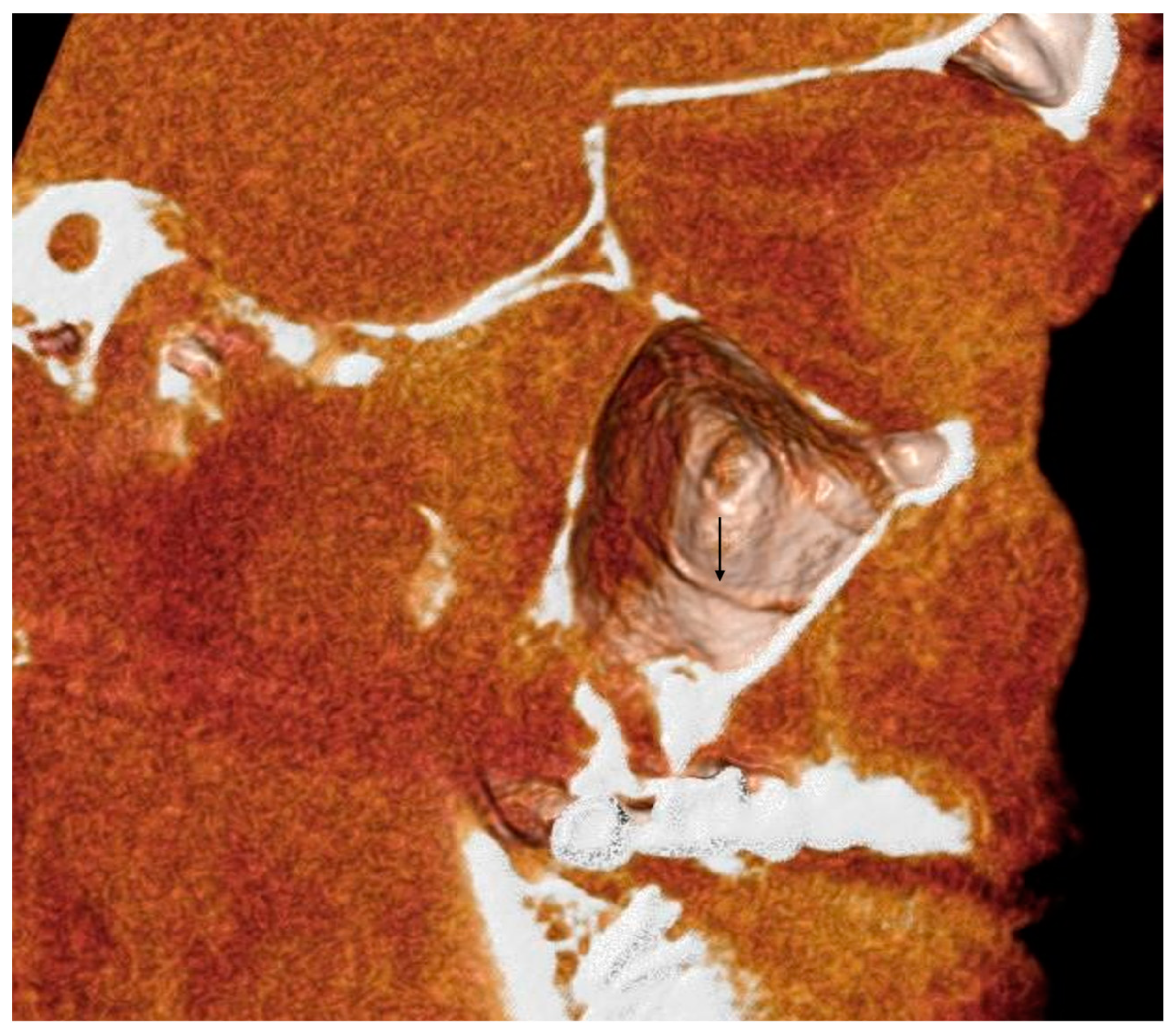
- The length of the arterial pathway in the mesiodistal dimension, on cross-section setting at 1 mm (Figure 2);
- The height of the maxillary bone crest in the cranio-caudal direction, on cross-section at the level of the first superior molar (Figure 3);
- The sized branches of the alveolar antral artery at the level of the first superior molar.
2.4. Statistics
2.5. Evaluation of Underwood Septa
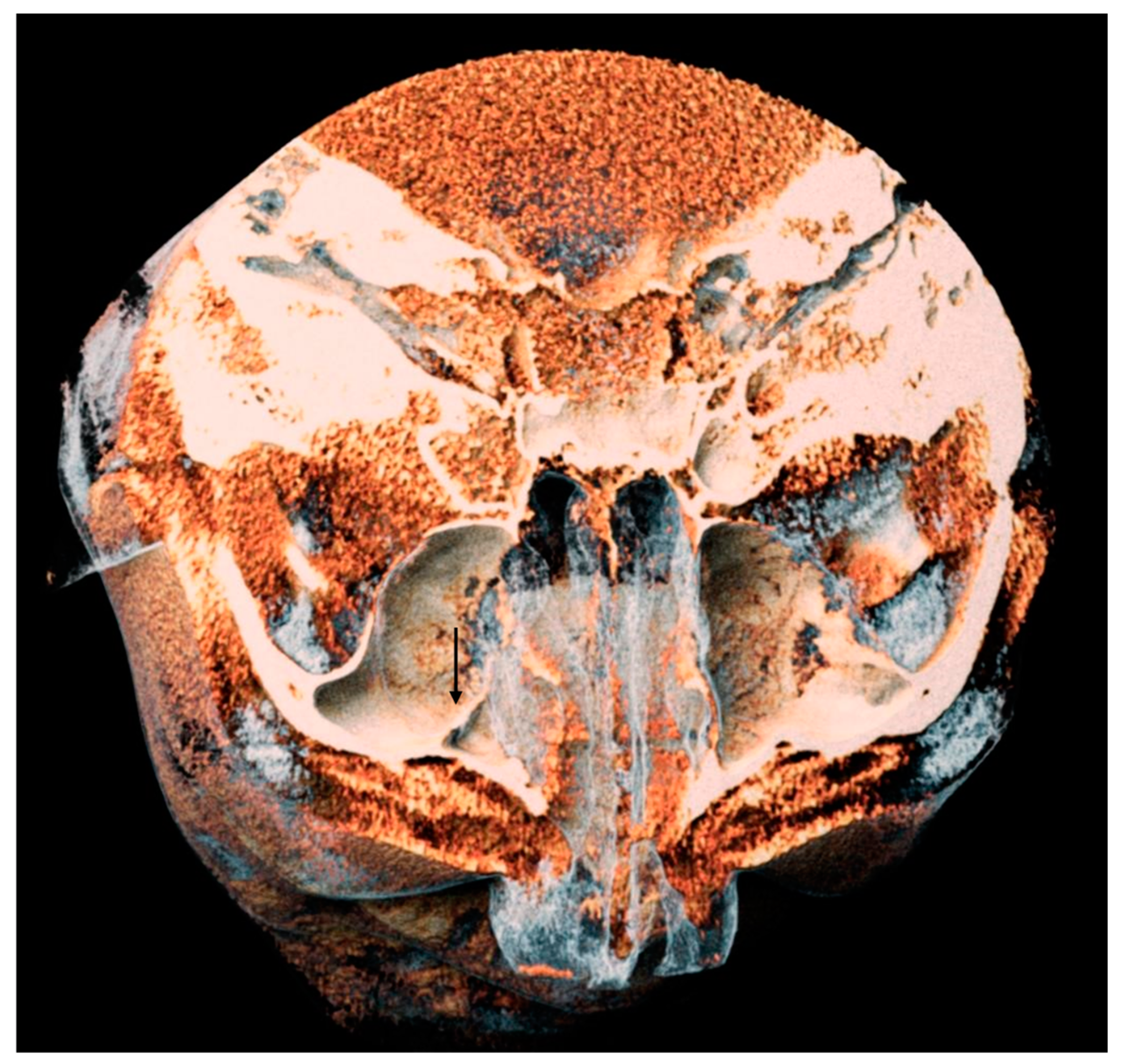
- The presence of the septa on cross-section (Figure 4);
- The height of the septa on cross-section setting from 2 mm to 0 mm, to better evaluate the maxillary sinus: this was measured from the apex of the septa to its bottom on the basal bone;
- The localization of the septa on cross-section;
- The orientation of the septa.
2.6. Statistics
3. Results
3.1. AAa Presence and Morphometry
- -
- 48% with a gauge of less than 1 mm;
- -
- 51% with a gauge between 1 and 2 mm;
- -
- 1% with a gauge greater than 2 mm.
3.2. Differences between Left and Right Hemiarches and between Genders
3.3. Underwood’s Septa Presence
3.4. Underwood’s Septa Position and Morphometry
4. Discussion
4.1. The Maxillary Sinus Arterial Vascularization
4.2. Underwood’s Septa
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mavrodi, A.; Paraskevas, G. Evolution of the paranasal sinuses’ anatomy through the ages. Anat. Cell Biol. 2013, 46, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Tubbs, R.S. Anatomical Variations in Clinical Dentistry. Anat. Var. Clin. Dent. 2019, 32, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Wilson, C.; Lachkar, S.; Tomaszewski, K.A.; Walocha, J.A.; Tubbs, R.S. Clinical anatomy of the maxillary sinus: Application to sinus floor augmentation. Anat. Cell Biol. 2019, 52, 17–24. [Google Scholar] [CrossRef]
- Bernardi, S.; Scarsella, S.; Di Fabio, D.; Oliva, A.; Di Girolamo, M.; Continenza, M.A.; Cutilli, T. Giant follicular cysts extended in pterygo-maxillary fossa, antro-naso-ethmoidal and orbital space associated to exophtalmos and diplopia in young patients. Oral Maxillofac. Surg. Cases 2018, 4, 17–22. [Google Scholar] [CrossRef]
- Raponi, I.; Giovannetti, F.; Buracchi, M.; Priore, P.; Battisti, A.; Scagnet, M.; Genitori, L.; Valentini, V. Management of orbital and brain complications of sinusitis: A practical algorithm. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2021, 49, 1124–1129. [Google Scholar] [CrossRef]
- Giovannetti, F.; Raponi, I.; Priore, P.; Macciocchi, A.; Barbera, G.; Valentini, V. Minimally-Invasive Endoscopic-Assisted Sinus Augmentation. J. Craniofac. Surg. 2019, 30, e359–e362. [Google Scholar] [CrossRef]
- Alhumaidan, G.; Eltahir, M.A.; Shaikh, S.S. Retrospective analysis of maxillary sinus septa—A cone beam computed tomography study. Saudi Dent. J. 2021, 33, 467–473. [Google Scholar] [CrossRef]
- Amine, K.; Slaoui, S.; Kanice, F.Z.; Kissa, J. Evaluation of maxillary sinus anatomical variations and lesions: A retrospective analysis using cone beam computed tomography. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 484–489. [Google Scholar] [CrossRef]
- Solar, P.; Geyerhofer, U.; Traxler, H.; Windisch, A.; Ulm, C.; Watzek, G. Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. Clin. Oral Implants Res. 1999, 10, 34–44. [Google Scholar] [CrossRef]
- Traxler, H.; Windisch, A.; Geyerhofer, U.; Surd, R.; Solar, P.; Firbas, W. Arterial blood supply of the maxillary sinus. Clin. Anat. 1999, 12, 417–421. [Google Scholar] [CrossRef]
- Mardinger, O.; Abba, M.; Hirshberg, A.; Schwartz-Arad, D. Prevalence, diameter and course of the maxillary intraosseous vascular canal with relation to sinus augmentation procedure: A radiographic study. Int. J. Oral Maxillofac. Surg. 2007, 36, 735–738. [Google Scholar] [CrossRef]
- Hur, M.S.; Kim, J.K.; Hu, K.S.; Bae, H.E.K.; Park, H.S.; Kim, H.J. Clinical implications of the topography and distribution of the posterior superior alveolar artery. J. Craniofac. Surg. 2009, 20, 551–554. [Google Scholar] [CrossRef]
- Rosano, G.; Taschieri, S.; Gaudy, J.F.; Del Fabbro, M. Maxillary sinus vascularization: A cadaveric study. J. Craniofac. Surg. 2009, 20, 940–943. [Google Scholar] [CrossRef]
- Taschieri, S.; Rosano, G. Management of the Alveolar Antral Artery During Sinus Floor Augmentation Procedures. J. Oral Maxillofac. Surg. 2010, 68, 230. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Tanaka, T.; Ibaragi, S.; Okui, T.; Hamaguchi, J.; Min, S.; Tubbs, R.S. Revisiting major anatomical risk factors of maxillary sinus lift and soft tissue graft harvesting for dental implant surgeons. Surg. Radiol. Anat. 2020, 42, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Lessa, A.M.G.; Oliveira, V.S.; Costa, R.B.A.; Meneses, A.T.R.; Crusoé-Rebello, I.; Costa, F.W.G.; Neves, F.S. Anatomical study of the maxillary sinus: Which characteristics can influence its volume? Surg. Radiol. Anat. 2023, 45, 81–87. [Google Scholar] [CrossRef]
- Tomaszewski, K.A.; Henry, B.M.; Kumar Ramakrishnan, P.; Roy, J.; Vikse, J.; Loukas, M.; Tubbs, R.S.; Walocha, J.A. Development of the Anatomical Quality Assurance (AQUA) checklist: Guidelines for reporting original anatomical studies. Clin. Anat. 2017, 30, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, S.; Mummolo, S.; Ciavarelli, L.M.; Li Vigni, M.; Continenza, M.A.; Marzo, G. Cone beam computed tomography investigation of the antral artery anastomosis in a population of Central Italy. Folia Morphol. 2016, 75, 149–153. [Google Scholar] [CrossRef]
- Sakhdari, S.; Panjnoush, M.; Eyvazlou, A.; Niktash, A. Determination of the Prevalence, Height, and Location of the Maxillary Sinus Septa Using Cone Beam Computed Tomography. Implant Dent. 2016, 25, 335–340. [Google Scholar] [CrossRef]
- Rosano, G.; Taschieri, S.; Gaudy, J.F.; Weinstein, T.; Del Fabbro, M. Maxillary sinus vascular anatomy and its relation to sinus lift surgery. Clin. Oral Implants Res. 2011, 22, 711–715. [Google Scholar] [CrossRef]
- Anamali, S.; Avila-Ortiz, G.; Elangovan, S.; Qian, F.; Ruprecht, A.; Finkelstein, M.; Allareddy, V. Prevalence of the posterior superior alveolar canal in cone beam computed tomography scans. Clin. Oral Implants Res. 2015, 26, e8–e12. [Google Scholar] [CrossRef]
- Apostolakis, D.; Bissoon, A.K. Radiographic evaluation of the superior alveolar canal: Measurements of its diameter and of its position in relation to the maxillary sinus floor: A cone beam computerized tomography study. Clin. Oral Implants Res. 2014, 25, 553–559. [Google Scholar] [CrossRef]
- Ilgüy, D.; Ilgüy, M.; Dolekoglu, S.; Fisekcioglu, E. Evaluation of the posterior superior alveolar artery and the maxillary sinus with CBCT. Braz. Oral Res. 2013, 27, 431–437. [Google Scholar] [CrossRef]
- Hayek, E.; Nasseh, I.; Hadchiti, W.; Bouchard, P.; Moarbes, M.; Khawam, G.; Bechara, B.; Noujeim, M. Location of Posterosuperior Alveolar Artery and Correlation with Maxillary Sinus Anatomy. Int. J. Periodontics Restorative Dent. 2015, 35, e60–e65. [Google Scholar] [CrossRef]
- Lee, S.; Fernandez, J.; Mirjalili, S.A.; Kirkpatrick, J. Pediatric paranasal sinuses—Development, growth, pathology, & functional endoscopic sinus surgery. Clin. Anat. 2022, 35, 745–761. [Google Scholar] [PubMed]
- Danesh-Sani, S.A.; Movahed, A.; ElChaar, E.S.; Chong Chan, K.; Amintavakoli, N. Radiographic Evaluation of Maxillary Sinus Lateral Wall and Posterior Superior Alveolar Artery Anatomy: A Cone-Beam Computed Tomographic Study. Clin. Implant Dent. Relat. Res. 2017, 19, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Pandharbale, A.A.; Gadgil, R.M.; Bhoosreddy, A.R.; Kunte, V.R.; Ahire, B.S.; Shinde, M.R.; Joshi, S.S. Evaluation of the Posterior Superior Alveolar Artery Using Cone Beam Computed Tomography. Polish J. Radiol. 2016, 81, 606–610. [Google Scholar] [CrossRef] [PubMed]
- Varela-Centelles, P.; Loira-Gago, M.; Seoane-Romero, J.M.; Takkouche, B.; Monteiro, L.; Seoane, J. Detection of the posterior superior alveolar artery in the lateral sinus wall using computed tomography/cone beam computed tomography: A prevalence meta-analysis study and systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghurabi, Z.H.; Abdulrazaq, S.S. Vascular Precautions Before Sinus Lift Procedure. J. Craniofac. Surg. 2018, 29, e116–e118. [Google Scholar] [CrossRef] [PubMed]
- Chitsazi, M.-T.; Shirmohammadi, A.; Faramarzi, M.; Esmaieli, F.; Chitsazi, S. Evaluation of the position of the posterior superior alveolar artery in relation to the maxillary sinus using the Cone-Beam computed tomography scans. J. Clin. Exp. Dent. 2017, 9, e394–e399. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Carrascal, N.; Salomó-Coll, O.; Gehrke, S.A.; Calvo-Guirado, J.L.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Radiological evaluation of maxillary sinus anatomy: A cross-sectional study of 300 patients. Ann. Anat. = Anat. Anzeiger Off. organ Anat. Ges. 2017, 214, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aung, M.; Panmekiat, S.; Pimkhaokham, A. The study of the alveolar antral artery canal in using cone beam computed tomography. M Dent. J. 2017, 37, 63–69. [Google Scholar]
- Tehranchi, M.; Taleghani, F.; Shahab, S.; Nouri, A. Prevalence and location of the posterior superior alveolar artery using cone-beam computed tomography. Imaging Sci. Dent. 2017, 47, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Şimşek Kaya, G.; Daltaban, Ö.; Kaya, M.; Kocabalkan, B.; Sindel, A.; Akdağ, M. The potential clinical relevance of anatomical structures and variations of the maxillary sinus for planned sinus floor elevation procedures: A retrospective cone beam computed tomography study. Clin. Implant Dent. Relat. Res. 2019, 21, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Rostetter, C.; Hungerbühler, A.; Blumer, M.; Rücker, M.; Wagner, M.; Stadlinger, B.; Lübbers, H.-T. Cone Beam Computed Tomography Evaluation of the Artery in the Lateral Wall of the Maxillary Sinus: Retrospective Analysis of 602 Sinuses. Implant Dent. 2018, 27, 434–438. [Google Scholar] [CrossRef]
- Sun, W.; Liu, A.; Gong, Y.; Shu, R.; Xie, Y. Evaluation of the Anastomosis Canal in Lateral Maxillary Sinus Wall With Cone Beam Computerized Tomography: A Clinical Study. J. Oral Implantol. 2018, 44, 5–13. [Google Scholar] [CrossRef]
- Yalcin, E.D.; Akyol, S. Relationship Between the Posterior Superior Alveolar Artery and Maxillary Sinus Pathology: A Cone-Beam Computed Tomography Study. J. Oral Maxillofac. Surg. 2019, 77, 2494–2502. [Google Scholar] [CrossRef]
- Yusof, M.Y.P.M.; Mah, M.C.; Reduwan, N.H.; Kretapirom, K.; Affendi, N.H.K. Quantitative and qualitative assessments of intraosseous neurovascular canals in dentate and posteriorly edentulous individuals in lateral maxillary sinus wall. Saudi Dent. J. 2020, 32, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, D.P.; Manhães Junior, L.R.C.; Silva, M.B.F.; Francischone, C.E.; Franco, A.; Junqueira, J.L.C. Alveolar antral artery in edentulous patients and their visualization through cone beam computed tomography. Morphologie 2021, 105, 64–68. [Google Scholar] [CrossRef]
- Alves, N.; Torres, C.; Deana, N.F.; Garay, I. Analysis of the presence, location and morphometry of the «alveolar antral artery» by cone-beam computed tomography in chilean adults. Int. J. Morphol. 2020, 38, 1760–1766. [Google Scholar] [CrossRef]
- Dias, E.; Santos, J.; Cotrim, K.; Brito, F. Tomographic evaluation of the prevalence of the intraosseous branch of the posterior superior alveolar artery. J. Oral Maxillofac. Radiol. 2019, 7, 60. [Google Scholar] [CrossRef]
- Padovani, L.S.; Oliveira, A.M.S.D.; Dutra, B.C.; Costa, F.O.; Oliveira, P.A.D. Important anatomical variations of the superior posterior alveolar artery: Studied by cone beam computed tomography. Anat. Histol. Embryol. 2020, 49, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.B.; Estrin, N.E.; Saleh, M.H.A.; Yoon, T.Y.H.; Tattan, M.; Wang, H.-L. Evaluation of length and location of the maxillary sinus intraosseous artery using computerized tomography. J. Periodontol. 2021, 92, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Fayek, M.M.; Amer, M.E.; Bakry, A.M. Evaluation of the posterior superior alveolar artery canal by cone-beam computed tomography in a sample of the Egyptian population. Imaging Sci. Dent. 2021, 51, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Godil, A.Z.; Devadiga, T.J.; Supnekar, S.C.; Kazi, A.I.; Wadwan, S.A.; Dugal, R. Position of posterior superior alveolar artery in relation to the maxillary sinus using cone beam computed tomography in Indian sub-population. J. Oral Med. Oral Surg. 2021, 27, 34. [Google Scholar] [CrossRef]
- Alves, N.; Torres-Villar, C.; Ceballos, F.; Deana, N.F. Frequency, location, and diameter of the anastomosis between the posterior superior alveolar artery and the infraorbital artery in imaging studies: Systematic review and meta-analysis. Surg. Radiol. Anat. 2023, 45, 431–443. [Google Scholar] [CrossRef]
- Henriques, I.; Caramês, J.; Francisco, H.; Caramês, G.; Hernández-Alfaro, F.; Marques, D. Prevalence of maxillary sinus septa: Systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2022, 51, 823–831. [Google Scholar] [CrossRef]
- Irinakis, T.; Dabuleanu, V.; Aldahlawi, S. Complications During Maxillary Sinus Augmentation Associated with Interfering Septa: A New Classification of Septa. Open Dent. J. 2017, 11, 140–150. [Google Scholar] [CrossRef]
- Rinaldi, F.; Piattellli, M.; Angiolani, F.; Bernardi, S.; Rastelli, E.; Varvara, G. Volumetric evaluation of maxillary sinuses using CBCTS: Radiographic study. Ital. J. Anat. Embriol. 2023, 127, 47–50. [Google Scholar] [CrossRef]
- Park, W.-B.; Kim, Y.-J.; Kang, K.L.; Lim, H.-C.; Han, J.-Y. Long-term outcomes of the implants accidentally protruding into nasal cavity extended to posterior maxilla due to inferior meatus pneumatization. Clin. Implant. Dent. Relat. Res. 2020, 22, 105–111. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AAa Intra-Osseous Variant (%) | AAa on the Left Sinus | AAa on the Right Sinus | p-Value (Chi-Square) |
|---|---|---|---|
| 100 | 96 | 97 | >0.05 |
| Parameters of AAa | Mean ± S. D. (mm) | p-Value (Student t-Test) | |
| AAa Length-right side | 24.06 ± 5.66 | 0.06 (1.85) | |
| AAa Length-left side | 23.21 ± 5.43 | ||
| Cranio-caudal distance AAa-right side | 12.25 ± 3.84 | 0.007 (−2.72) | |
| Cranio-caudal distance AAa-left side | 13.44 ± 3.91 | ||
| AAa Medium-size branches-right side | 1.07 ± 0.38 | 0.72 (0.36) | |
| AAa Medium-size branches-left side | 1.07 ± 0.33 | ||
| Medium-Size Branch | Number of Cases on Right Side | Number of Cases on Left Side | Frequency (%) |
|---|---|---|---|
| ≤1 mm | 52 | 44 | 48% |
| range 1–2 mm | 47 | 56 | 51% |
| >2 mm | 1 | 0 | 1% |
| Gender | Cranio-Caudal Distance of the Right AAa (Mean ± S.D.) | Cranio-Caudal Distance of the Left AAa (Mean ± S.D.) | p Value (Student’s t-Test) |
|---|---|---|---|
| M | 11.66 ± 33.83 | 13.42 ± 43.31 | >0.05 |
| F | 12.671 ± 41.23 | 13.46 ± 35.99 | |
| Gender | Length of the Right AAa (Mean ± S.D.) | Length of the Left AAa (Mean ± S.D.) | p Value (Student’s t-Test) |
| M | 24.225 ± 48.54 | 24.141 ± 51.82 | >0.05 |
| F | 23.947 ± 62.09 | 22.494 ± 55.61 |
| Gender | Caliber of the Right AAa (Mean ± S.D.) (mm) | Caliber of the Left AAa (Mean ± S.D.) (mm) | p Value (Student’s t-Test) |
|---|---|---|---|
| M | 1.18 ± 0.44 | 1.13 ± 0.33 | >0.05 |
| F | 1.07 ± 0.31 | 1.02 ± 0.32 | |
| p value (Student’s t-test) | <0.05 |
| Patients with Septa (n) | Single Septa (n) | Double Septa (n) | p-Value (Chi-Square between Males and Females) | |
|---|---|---|---|---|
| Total of patients | 15 | 11 | 4 | >0.05 |
| Female patients | 9 | 6 | 3 | |
| Male patients | 6 | 5 | 1 |
| Single Septa (n) | Double Septa (n) | |
|---|---|---|
| Right side | 7 | 4 |
| Male patients | 5 | 1 |
| Female patients | 2 | 3 |
| Left side | 4 | 0 |
| Male patients | 0 | 0 |
| Female patients | 4 | 0 |
| Anterior (n) | Central (n) | Posterior (n) | |
|---|---|---|---|
| Right side | 4 | 2 | 1 |
| Male patients | 4 | 0 | 1 |
| Female patients | 0 | 2 | 0 |
| Left side | 3 | 1 | 0 |
| Male patients | 0 | 0 | 0 |
| Female patients | 3 | 1 | 0 |
| Anterior | Central | Posterior | |
|---|---|---|---|
| Right side | 0 | 3 | 1 |
| Male patients | 0 | 1 | 0 |
| Female patients | 0 | 2 | 0 |
| Left side | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardi, S.; Bianchi, S.; Gerardi, D.; Petrelli, P.; Rinaldi, F.; Piattelli, M.; Macchiarelli, G.; Varvara, G. Anatomy of Maxillary Sinus: Focus on Vascularization and Underwood Septa via 3D Imaging. Tomography 2024, 10, 444-458. https://doi.org/10.3390/tomography10040034
Bernardi S, Bianchi S, Gerardi D, Petrelli P, Rinaldi F, Piattelli M, Macchiarelli G, Varvara G. Anatomy of Maxillary Sinus: Focus on Vascularization and Underwood Septa via 3D Imaging. Tomography. 2024; 10(4):444-458. https://doi.org/10.3390/tomography10040034
Chicago/Turabian StyleBernardi, Sara, Serena Bianchi, Davide Gerardi, Pierpaolo Petrelli, Fabiola Rinaldi, Maurizio Piattelli, Guido Macchiarelli, and Giuseppe Varvara. 2024. "Anatomy of Maxillary Sinus: Focus on Vascularization and Underwood Septa via 3D Imaging" Tomography 10, no. 4: 444-458. https://doi.org/10.3390/tomography10040034
APA StyleBernardi, S., Bianchi, S., Gerardi, D., Petrelli, P., Rinaldi, F., Piattelli, M., Macchiarelli, G., & Varvara, G. (2024). Anatomy of Maxillary Sinus: Focus on Vascularization and Underwood Septa via 3D Imaging. Tomography, 10(4), 444-458. https://doi.org/10.3390/tomography10040034