

The Development of a Biomimetic Model of Bacteria Migration on Indwelling Urinary Catheter Surfaces

 ,
,  ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. CAUTI Initiation by Extraluminal Migration
1.2. CAUTI Prevention by Chlorhexidine
1.3. In Vitro Modelling of Extraluminal Migration
2. Materials and Methods
2.1. Bacterial Strains, Media, Materials and Urinary Catheters
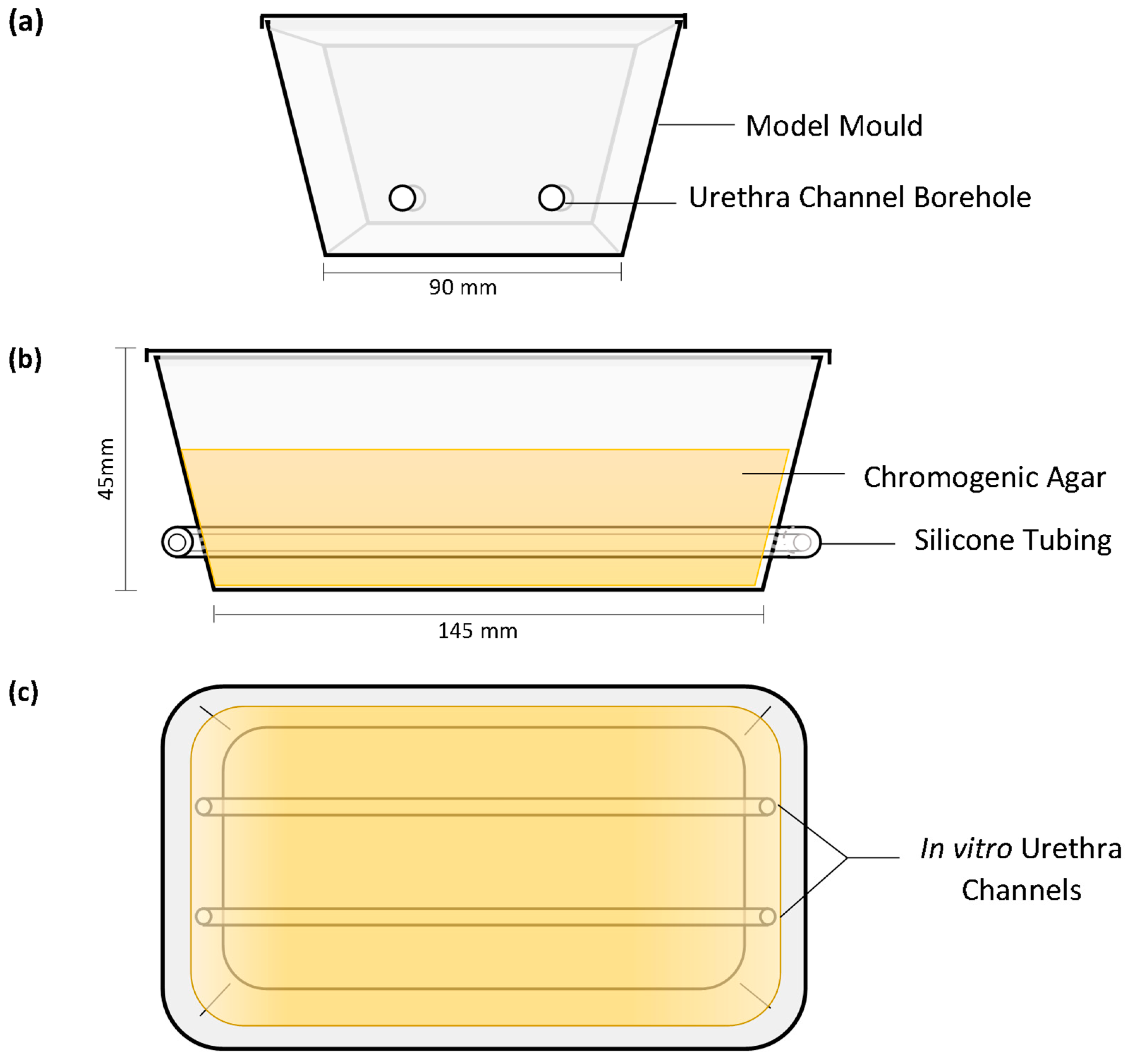
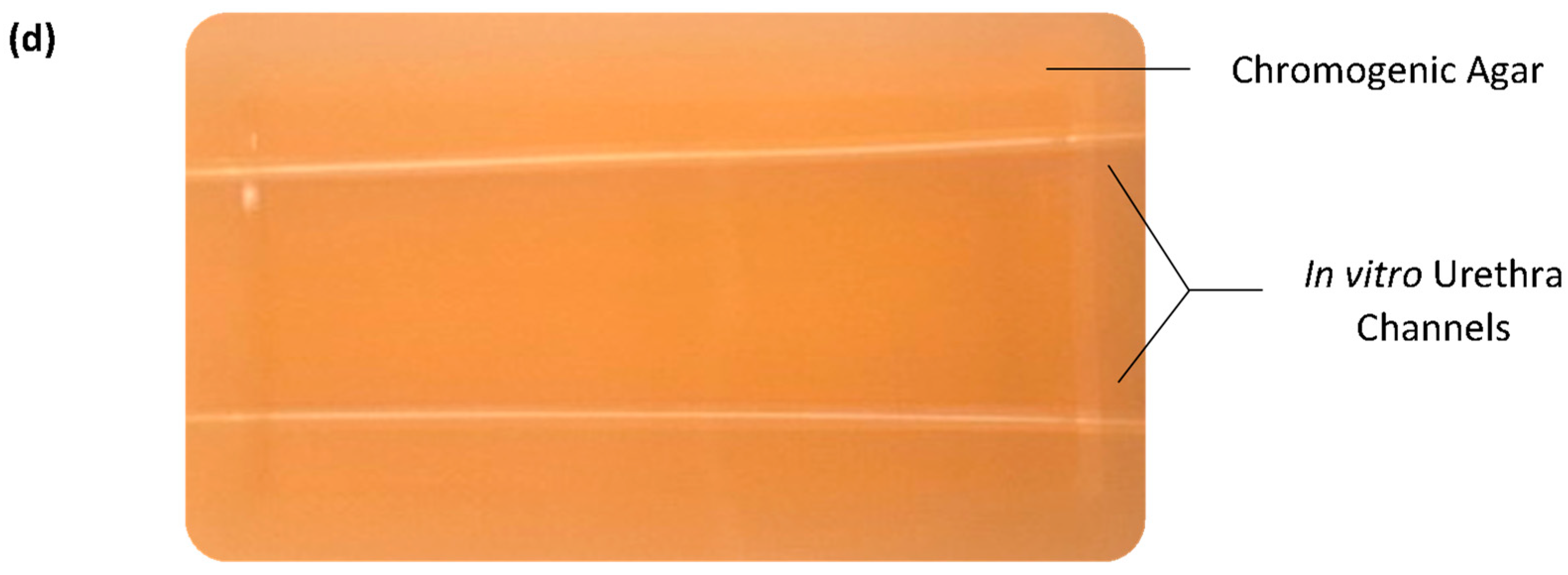
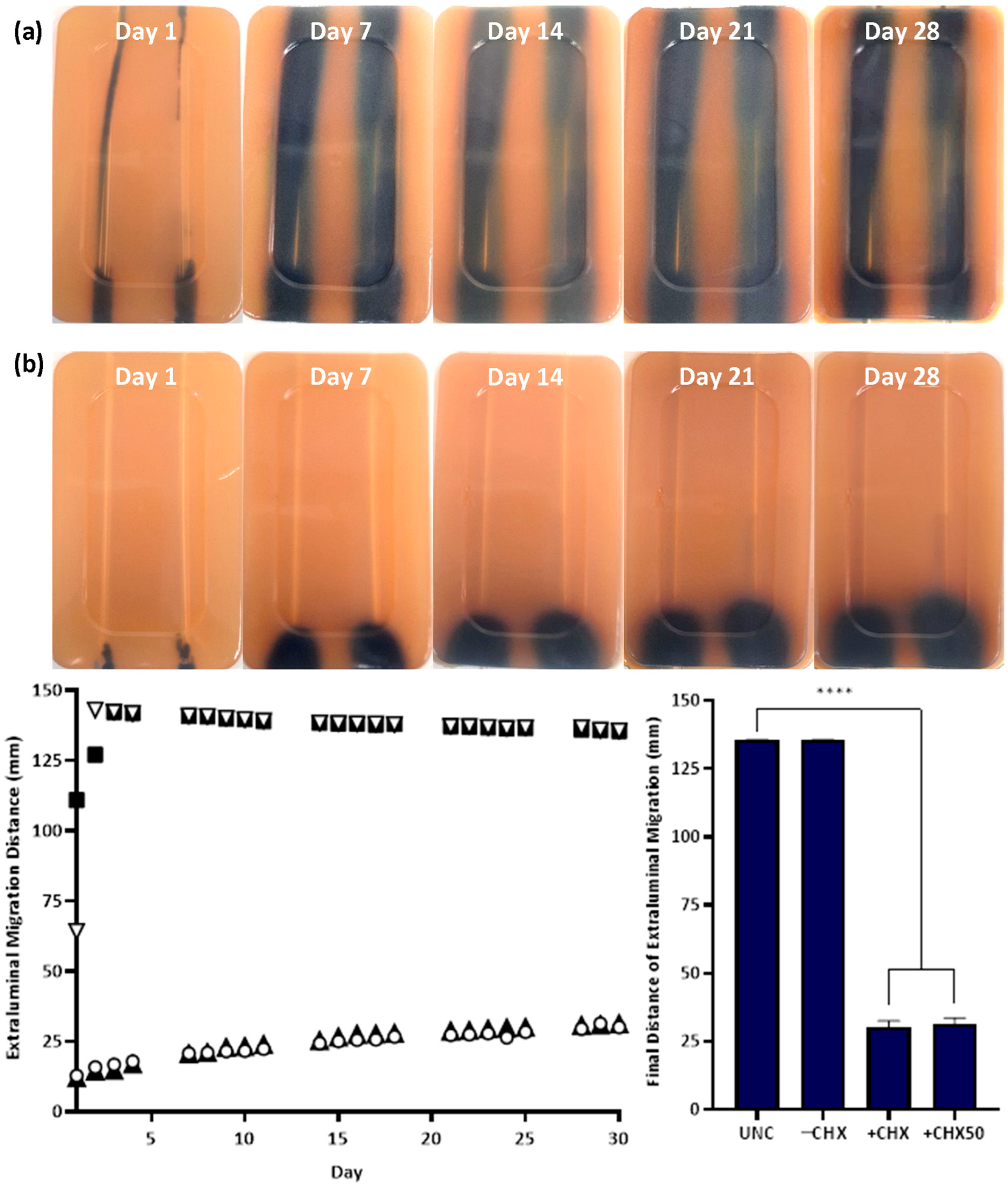
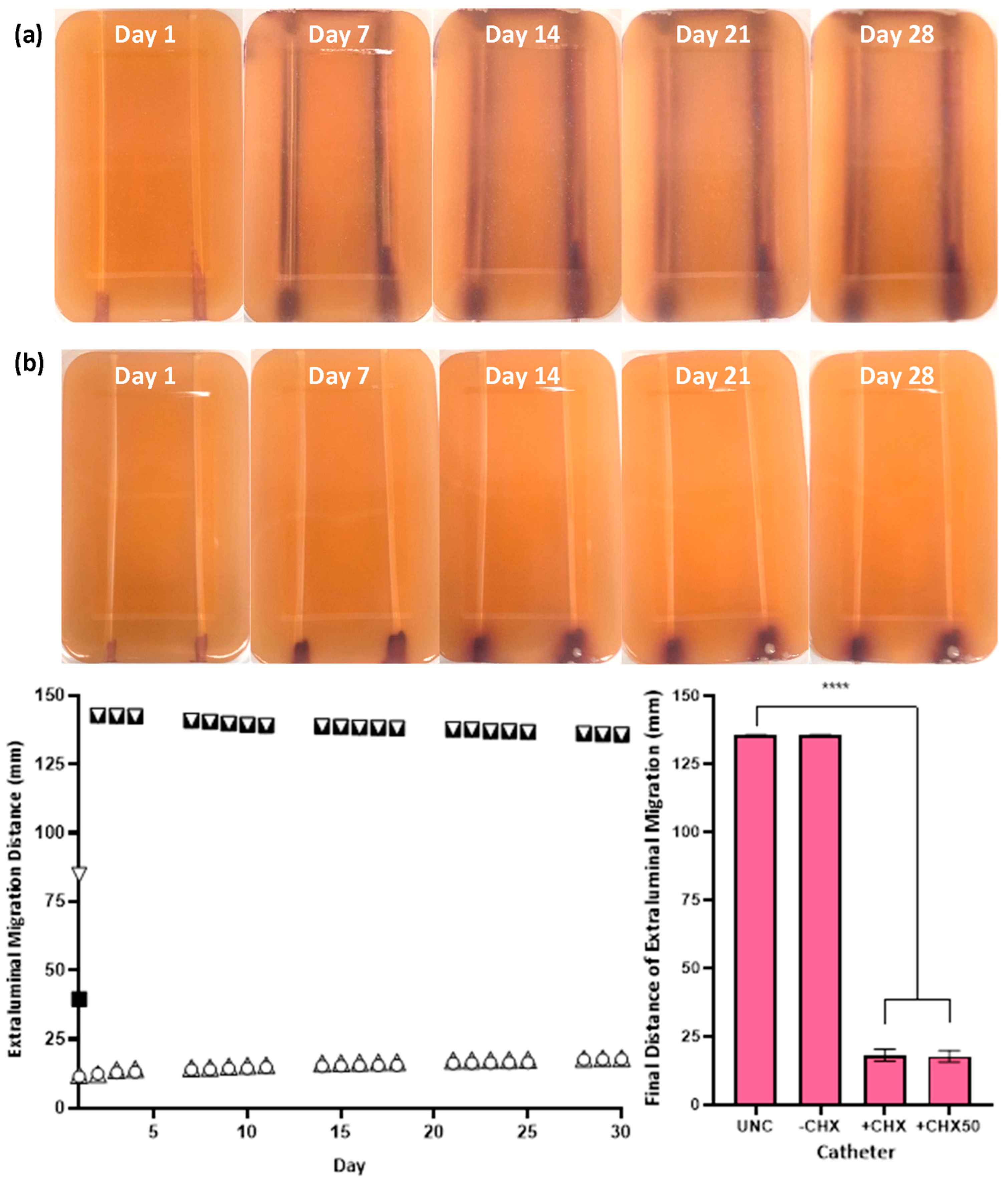
2.2. In Vitro Extraluminal Migration Model
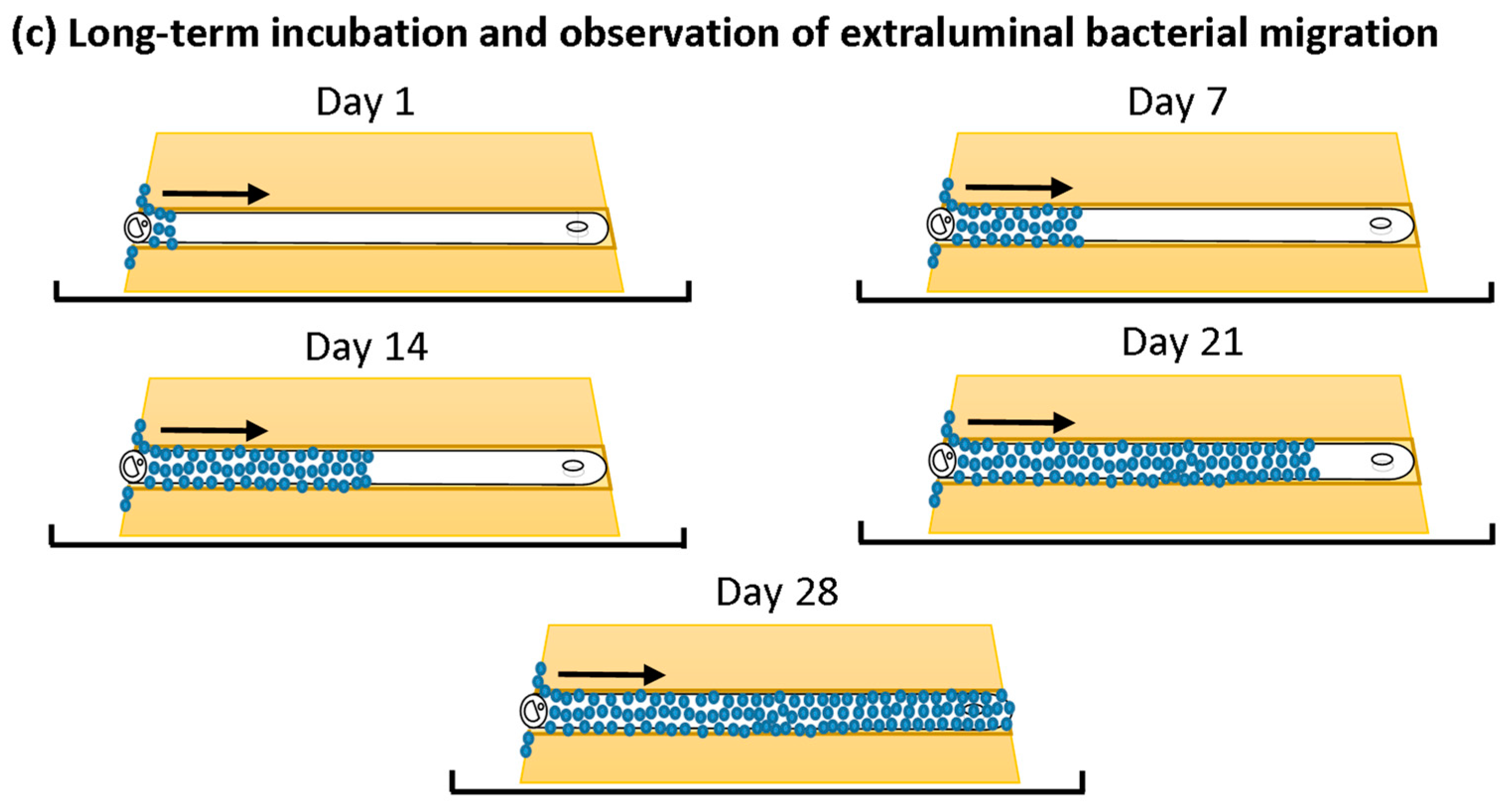
2.3. In Vitro Extraluminal Migration
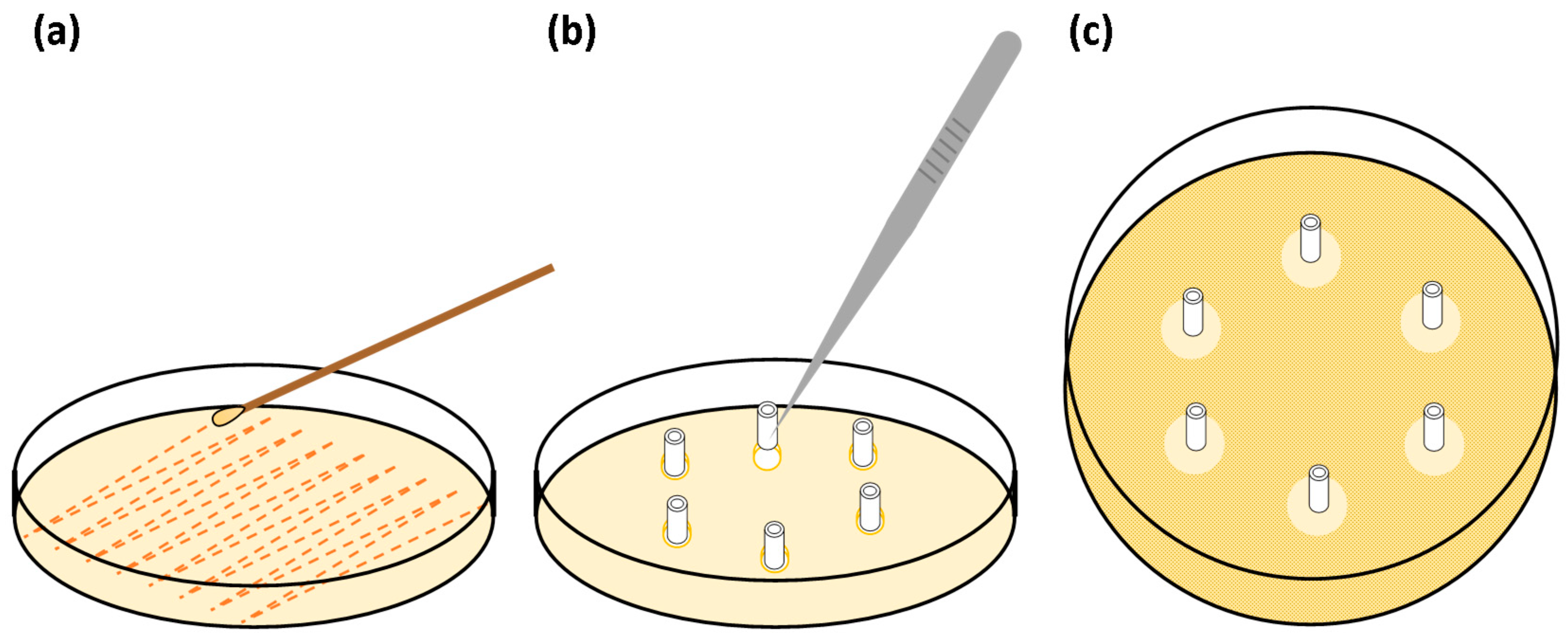
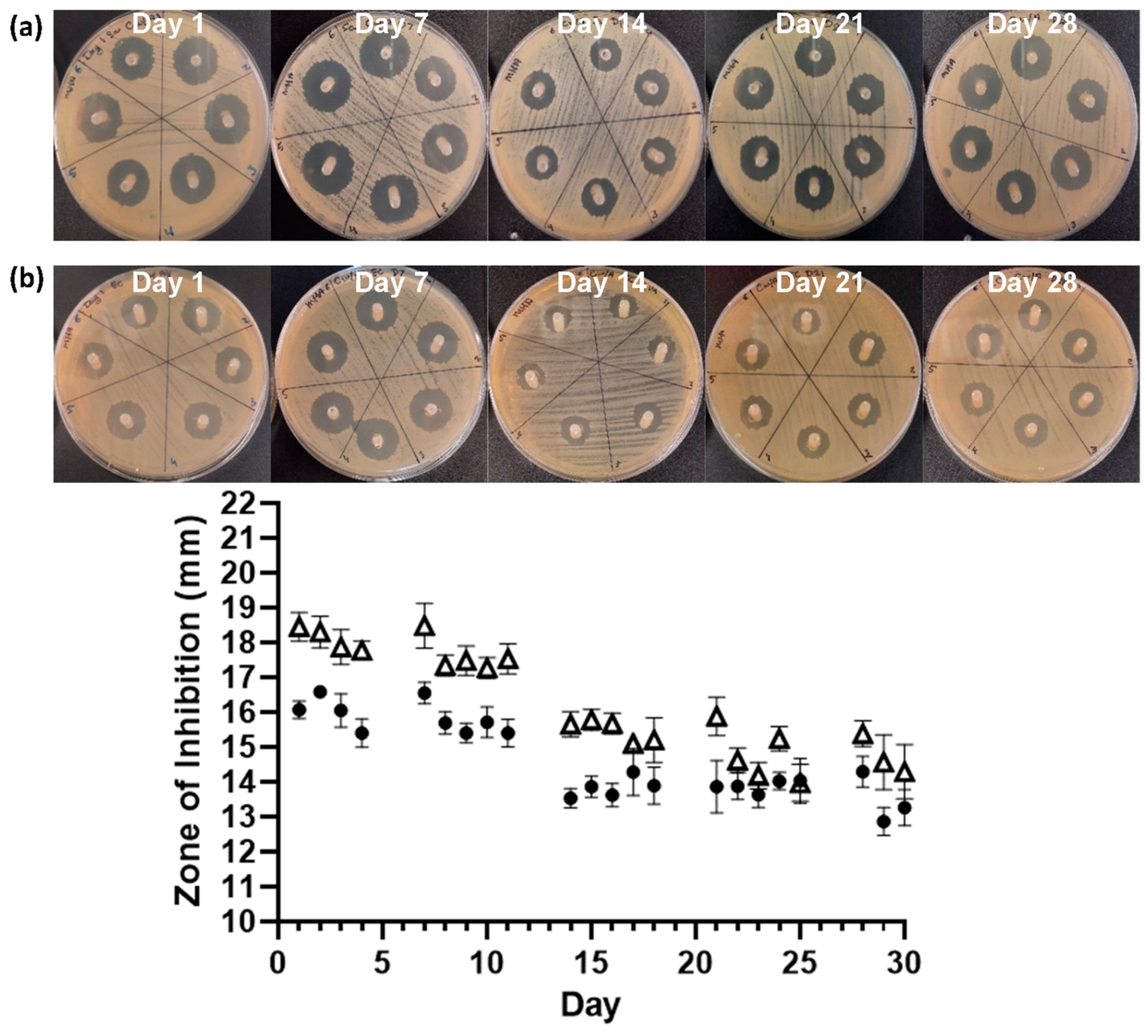
2.4. Serial Plate Transfer Test (SPTT)
2.5. Minimum Inhibitory Concentration (MIC)
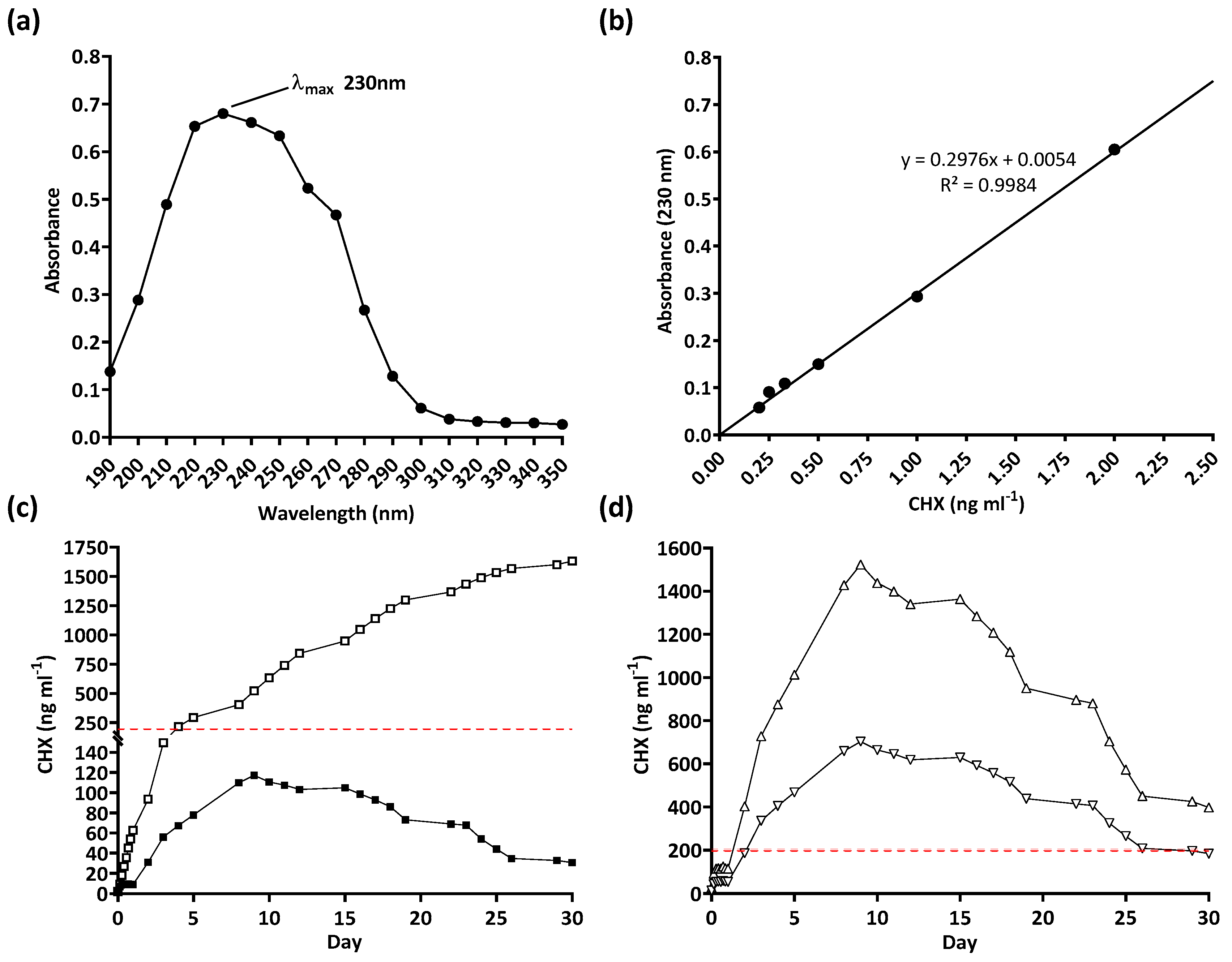
2.6. Drug Release Trial
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Cortese, Y.J.; Wagner, V.E.; Tierney, M.; Devine, D.; Fogarty, A. Review of Catheter-Associated Urinary Tract Infections and In Vitro Urinary Tract Models. J. Healthc. Eng. 2018, 2018, 2986742. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, J.; Radera, S. Biofilm-Mediated Urinary Tract Infections. In Biofilms in Human Diseases: Treatment and Control, 1st ed.; Kumar, S., Chandra, N., Singh, L., Hashmi, M.Z., Varma, A., Eds.; Springer: Cham, Switzerland, 2019; pp. 177–214. [Google Scholar]
- Melo, L.D.R.; Veiga, P.; Cerca, N.; Kropinski, A.M.; Almeida, C.; Azeredo, J.; Sillankorva, S. Development of a phage cocktail to control Proteus mirabilis catheter-associated urinary tract infections. Front. Microbiol. 2016, 7, 1024. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, S.M.; Stickler, D.J.; Mobley, H.L.T.; Shirtliff, M.E. Complicated Catheter-Associated Urinary Tract Infections Due to Escherichia coli and Proteus mirabilis. Clin. Microbiol. Rev. 2008, 21, 26–59. [Google Scholar] [CrossRef] [PubMed]
- Maki, D.G.; Tambyah, P.A. Engineering out the risk for infection with urinary catheters. Emerg. Infect. Dis. 2001, 7, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Darouiche, R.O.; Safar, H.; Raad, I.I. In Vitro Efficacy of Antimicrobial-Coated Bladder Catheters in Inhibiting Bacterial Migration along Catheter Surface. J. Infect. Dis. 1997, 176, 1109–1112. [Google Scholar] [CrossRef] [PubMed]
- Summers, J.; Goeres, D.M. Catheter-Associated Urinary Tract Infections: Development of a Test Method for Assessing the Efficacy of Antimicrobial Technologies/Products. In Targeting Biofilms in Translational Research, Device Development, and Industrial Sectors, 1st ed.; Williams, D.L., Ed.; Springer: Cham, Switzerland, 2019; pp. 29–53. [Google Scholar]
- Miller, A.; Gillespie, W.A.; Linton, K.B.; Slade, N.; Mitchell, J.P. Postoperative Infection in Urology. Lancet 1958, 272, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Maiti, P.; Dey, R.; Kundu, A.; Dey, R. Biofilms on indwelling urologic devices: Microbes and antimicrobial management prospect. Ann. Med. Health Sci. Res. 2014, 4, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Barford, J.M.T.; Anson, K.; Hu, Y.; Coates, A.R.M. A model of catheter-associated urinary tract infection initiated by bacterial contamination of the catheter tip. BJU Int. 2008, 102, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Thomas-White, K.; Brady, M.; Wolfe, A.J.; Mueller, E.R. The Bladder Is Not Sterile: History and Current Discoveries on the Urinary Microbiome. Curr. Bladder Dysfunct. Rep. 2016, 11, 18–24. [Google Scholar] [CrossRef]
- Cortese, Y.J.; Wagner, V.E.; Tierney, M.; Scully, D.; Devine, D.M.; Fogarty, A. Pathogen displacement during intermittent catheter insertion: A novel in vitro urethra model. J. Appl. Microbiol. 2020, 128, 1191–1200. [Google Scholar] [CrossRef]
- Singha, P.; Locklin, J.; Handa, H. A review of the recent advances in antimicrobial coatings for urinary catheters. Acta Biomater. 2017, 50, 20–40. [Google Scholar] [CrossRef] [PubMed]
- Majeed, A.; Sagar, F.; Latif, A.; Hassan, H.; Iftikhar, A.; Darouiche, R.O.; Al Mohajer, M. Does antimicrobial coating and impregnation of urinary catheters prevent catheter-associated urinary tract infection? A review of clinical and preclinical studies. Expert Rev. Med. Devices 2019, 16, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Fasugba, O.; Cheng, A.C.; Gregory, V.; Graves, N.; Koerner, J.; Collignon, P.; Gardner, A.; Mitchell, B.G. Chlorhexidine for meatal cleaning in reducing catheter-associated urinary tract infections: A multicentre stepped-wedge randomised controlled trial. Lancet Infect. Dis. 2019, 19, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, B.G.; Fasugba, O.; Cheng, A.C.; Gregory, V.; Koerner, J.; Collignon, P.; Gardner, A.; Graves, N. Chlorhexidine versus saline in reducing the risk of catheter associated urinary tract infection: A cost-effectiveness analysis. Int. J. Nurs. Stud. 2019, 97, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Gefter, J.; Zaks, B.; Kirmayer, D.; Lavy, E.; Steinberg, D.; Friedman, M. Chlorhexidine sustained-release varnishes for catheter coating—Dissolution kinetics and antibiofilm properties. Eur. J. Pharm. Sci. 2018, 112, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Srisang, S.; Wongsuwan, N.; Boongird, A.; Ungsurungsie, M.; Wanasawas, P.; Nasongkla, N. Multilayer nanocoating of Foley urinary catheter by chlorhexidine-loaded nanoparticles for prolonged release and anti-infection of urinary tract. Int. J. Polym. Mater. Polym. Biomater. 2020, 69, 1081–1089. [Google Scholar] [CrossRef]
- Srisang, S.; Nasongkla, N. Spray coating of foley urinary catheter by chlorhexidine-loadedpoly(ε-caprolactone) nanospheres: Effect of lyoprotectants, characteristics, and antibacterial activity evaluation. Pharm. Dev. Technol. 2018, 24, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Srisang, S.; Nasongkla, N. Layer-by-layer dip coating of Foley urinary catheters by chlorhexidine-loaded micelles. J. Drug Deliv. Sci. Technol. 2019, 49, 235–242. [Google Scholar] [CrossRef]
- Gaonkar, T.A.; Caraos, L.; Modak, S. Efficacy of a Silicone Urinary Catheter Impregnated with Chlorhexidine and Triclosan Against Colonization With Proteus mirabilis and Other Uropathogens. Infect. Control Hosp. Epidemiol. 2007, 28, 596–598. [Google Scholar] [CrossRef]
- Gaonkar, T.A.; Sampath, L.A.; Modak, S.M. Evaluation of the Antimicrobial Efficacy of Urinary Catheters Impregnated With Antiseptics in an In Vitro Urinary Tract Model. Infect. Control Hosp. Epidemiol. 2003, 24, 506–513. [Google Scholar] [CrossRef]
- Williams, G.J.; Stickler, D.J. Some Observations on the Migration of Proteus mirabilis and Other Urinary Tract Pathogens. Infect. Control Hosp. Epidemiol. 2008, 29, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Cruz, N.; Rosenblatt, J.; Reitzel, R.A.; Chaftari, A.M.; Hachem, R.; Raad, I. Pilot Ex Vivo and in Vitro Evaluation of a Novel Foley Catheter with Antimicrobial Periurethral Irrigation for Prevention of Extraluminal Biofilm Colonization Leading to Catheter-Associated Urinary Tract Infections (CAUTIs). Biomed. Res. Int. 2019, 2019, 2869039. [Google Scholar] [CrossRef] [PubMed]
- Cortese, Y.J. The Design, Development, and Testing of Novel Next Generation In Vitro Agar-based Urethral Models for Medical Device Innovation. Athlone 2022, 104–130. Available online: https://research.thea.ie/handle/20.500.12065/4345 (accessed on 11 August 2024).
- Fisher, L.E.; Hook, A.L.; Ashraf, W.; Yousef, A.; Barrett, D.A.; Scurr, D.J.; Chen, X.; Smith, E.F.; Fay, M.; Parmenter, C.D.; et al. Biomaterial modification of urinary catheters with antimicrobials to give long-term broadspectrum antibiofilm activity. J. Control. Release 2015, 202, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) infections: Virulence factors, bladder responses, antibiotic, and non-antibiotic antimicrobial strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef] [PubMed]
- Pollitt, E.J.G.; Diggle, S.P. Defining motility in the Staphylococci. Cell. Mol. Life Sci. 2017, 74, 2943–2958. [Google Scholar] [CrossRef]
- Pollitt, E.J.G.; Crusz, S.A.; Diggle, S.P. Staphylococcus aureus forms spreading dendrites that have characteristics of active motility. Sci. Rep. 2015, 5, 17698. [Google Scholar] [CrossRef]
- Theriault, R.; Ward-Smith, P.; Soper, C. Leakage associated with urinary catheter usage: A design challenge. Urol. Nurs. 2012, 32, 307–312. [Google Scholar] [CrossRef]
- Al-Adham, I.; Haddadin, R.; Collier, P. Types of Microbicidal and Microbistatic Agents. In Russell, Hugo & Ayliffe’s: Principles and Practice of Disinfection, Preservation and Sterilization, 5th ed.; Fraise, A.P., Maillard, J., Sattar, S.A., Eds.; John Wiley & Sons, Ltd.: Sussex, UK, 2012; pp. 5–70. [Google Scholar]
- Willis, L. Final Report on the Safety Assessment of Chlorhexidine/Chlorhexidine Diacetate/Chlorhexidine Dihydrochloride/Chlorhexidine Digluconate. J. Am. Coll. Toxicol. 1993, 12, 201–223. [Google Scholar] [CrossRef]
- Fernandes, M.; Lourenço, T.; Lopes, A.; Santos, A.S.; Santos, M.C.P.; Barbosa, M.P. Chlorhexidine: A hidden life-threatening allergen. Asia Pac. Allergy 2019, 9, e29. [Google Scholar] [CrossRef] [PubMed]
- Werneburg, G.T. Catheter-Associated Urinary Tract Infections: Current Challenges and Future Prospects. Res. Rep. Urol. 2022, 14, 109–133. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.V.; Young, R.; Mahenthiralingam, E.; Stickler, D.J. Ultrastructure of Proteus mirabilis Swarmer Cell Rafts and Role of Swarming in Catheter-Associated Urinary Tract Infection. Infect. Immun. 2004, 72, 3941–3950. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortese, Y.J.; Fayne, J.; Colbert, D.M.; Devine, D.M.; Fogarty, A. The Development of a Biomimetic Model of Bacteria Migration on Indwelling Urinary Catheter Surfaces. Biomimetics 2024, 9, 491. https://doi.org/10.3390/biomimetics9080491
Cortese YJ, Fayne J, Colbert DM, Devine DM, Fogarty A. The Development of a Biomimetic Model of Bacteria Migration on Indwelling Urinary Catheter Surfaces. Biomimetics. 2024; 9(8):491. https://doi.org/10.3390/biomimetics9080491
Chicago/Turabian StyleCortese, Yvonne J., Joanne Fayne, Declan M. Colbert, Declan M. Devine, and Andrew Fogarty. 2024. "The Development of a Biomimetic Model of Bacteria Migration on Indwelling Urinary Catheter Surfaces" Biomimetics 9, no. 8: 491. https://doi.org/10.3390/biomimetics9080491
APA StyleCortese, Y. J., Fayne, J., Colbert, D. M., Devine, D. M., & Fogarty, A. (2024). The Development of a Biomimetic Model of Bacteria Migration on Indwelling Urinary Catheter Surfaces. Biomimetics, 9(8), 491. https://doi.org/10.3390/biomimetics9080491