
Bridging the Finger-Action Gap between Hand Patients and Healthy People in Daily Life with a Biomimetic System

Abstract
:1. Introduction
2. Materials and Methods
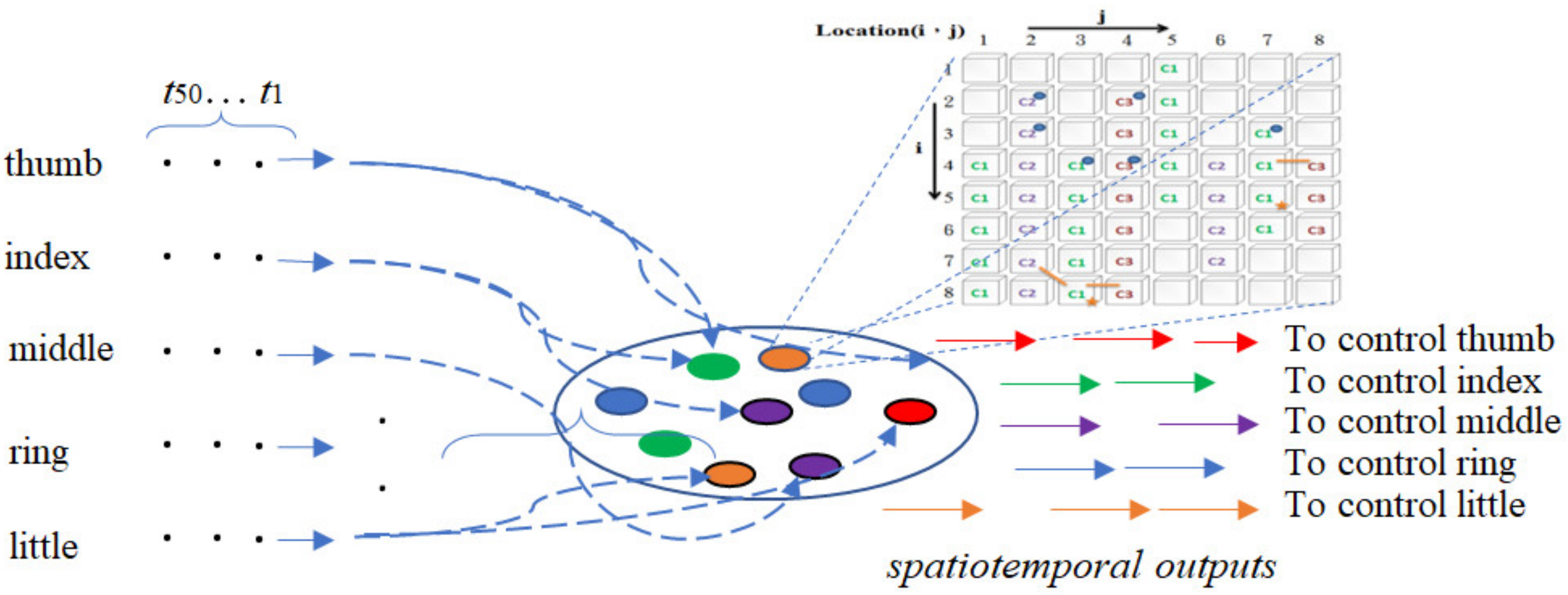
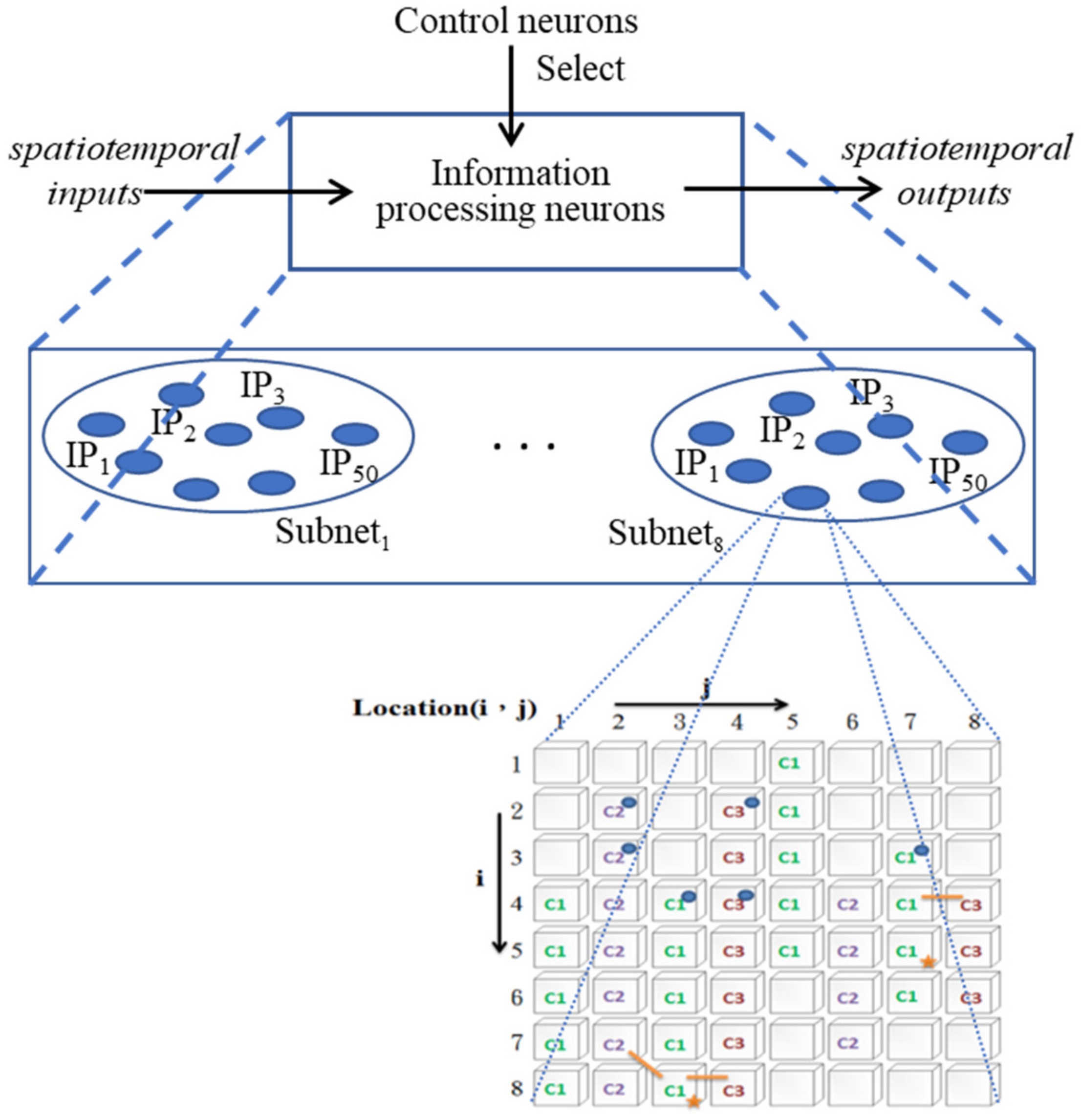
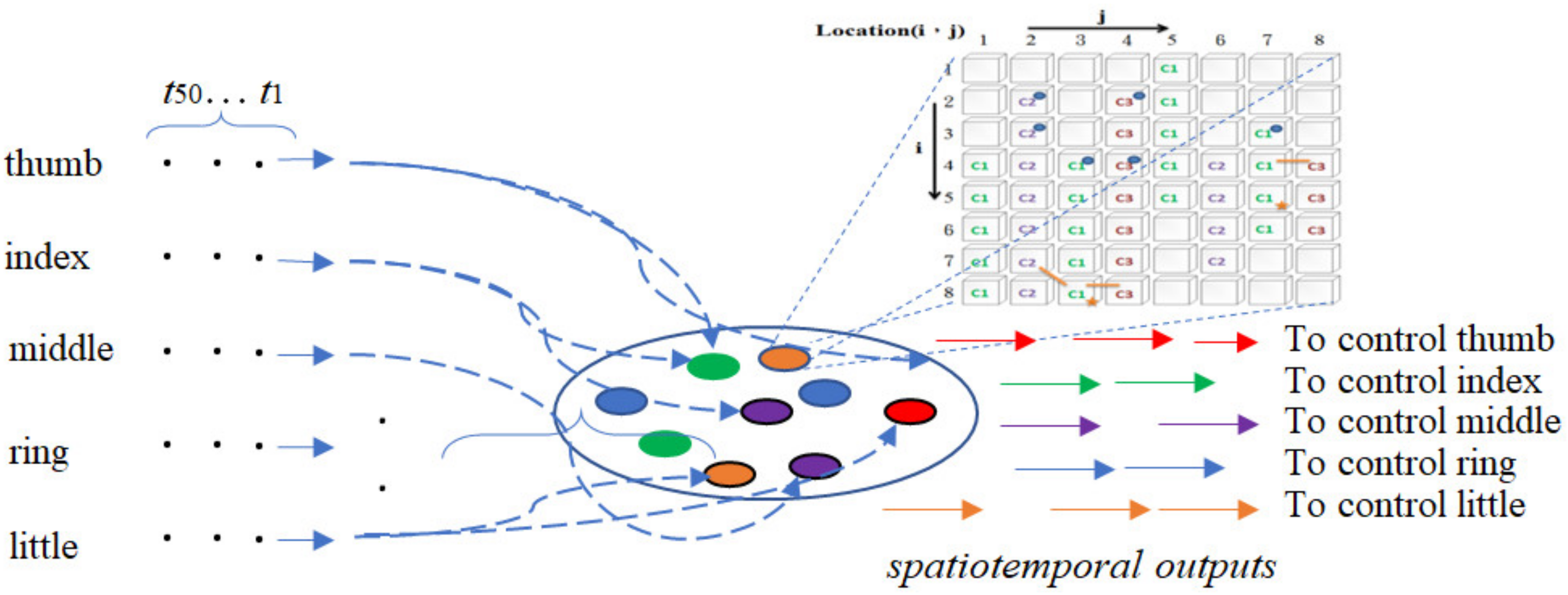
2.1. The Architecture of the ANM System
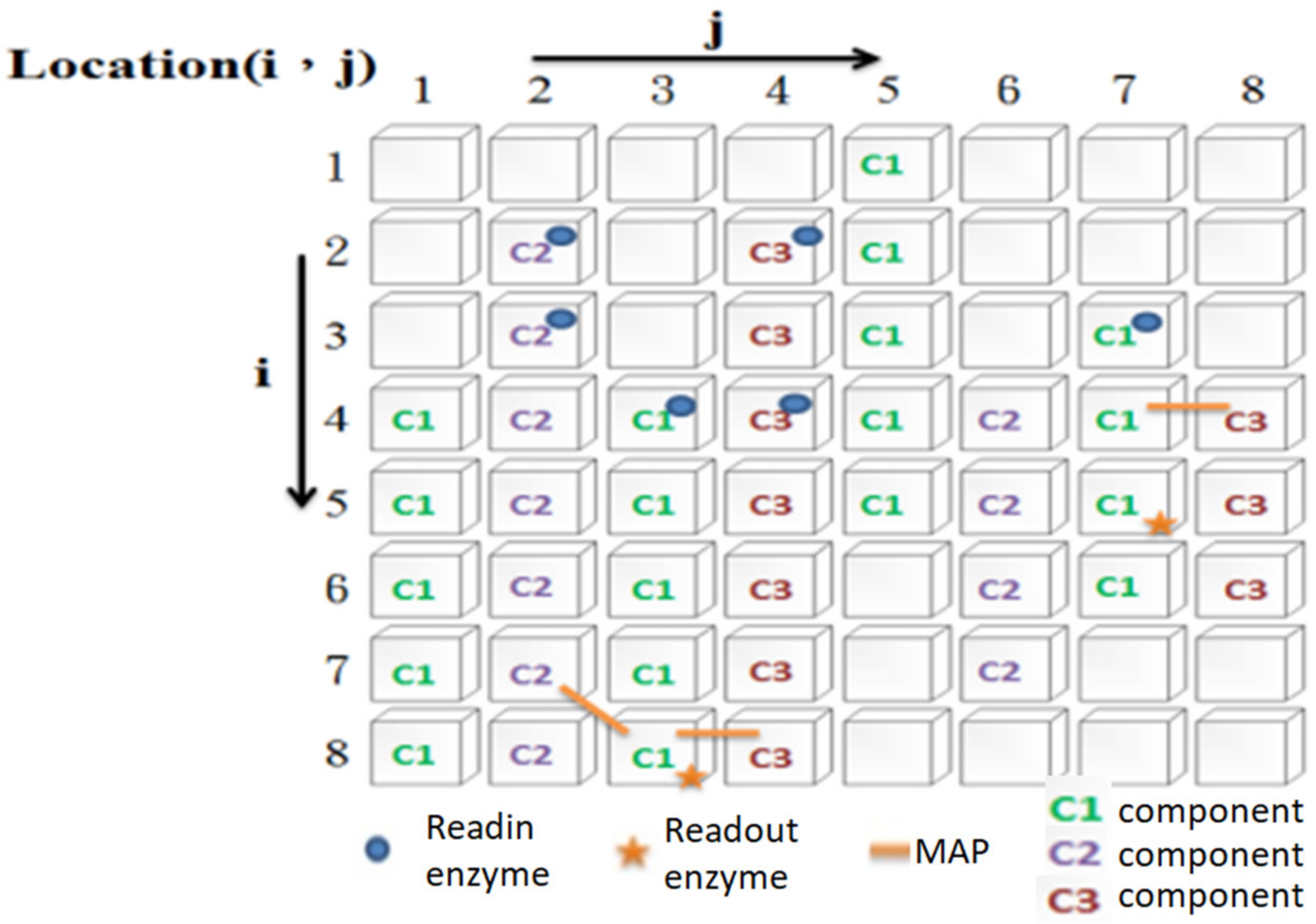
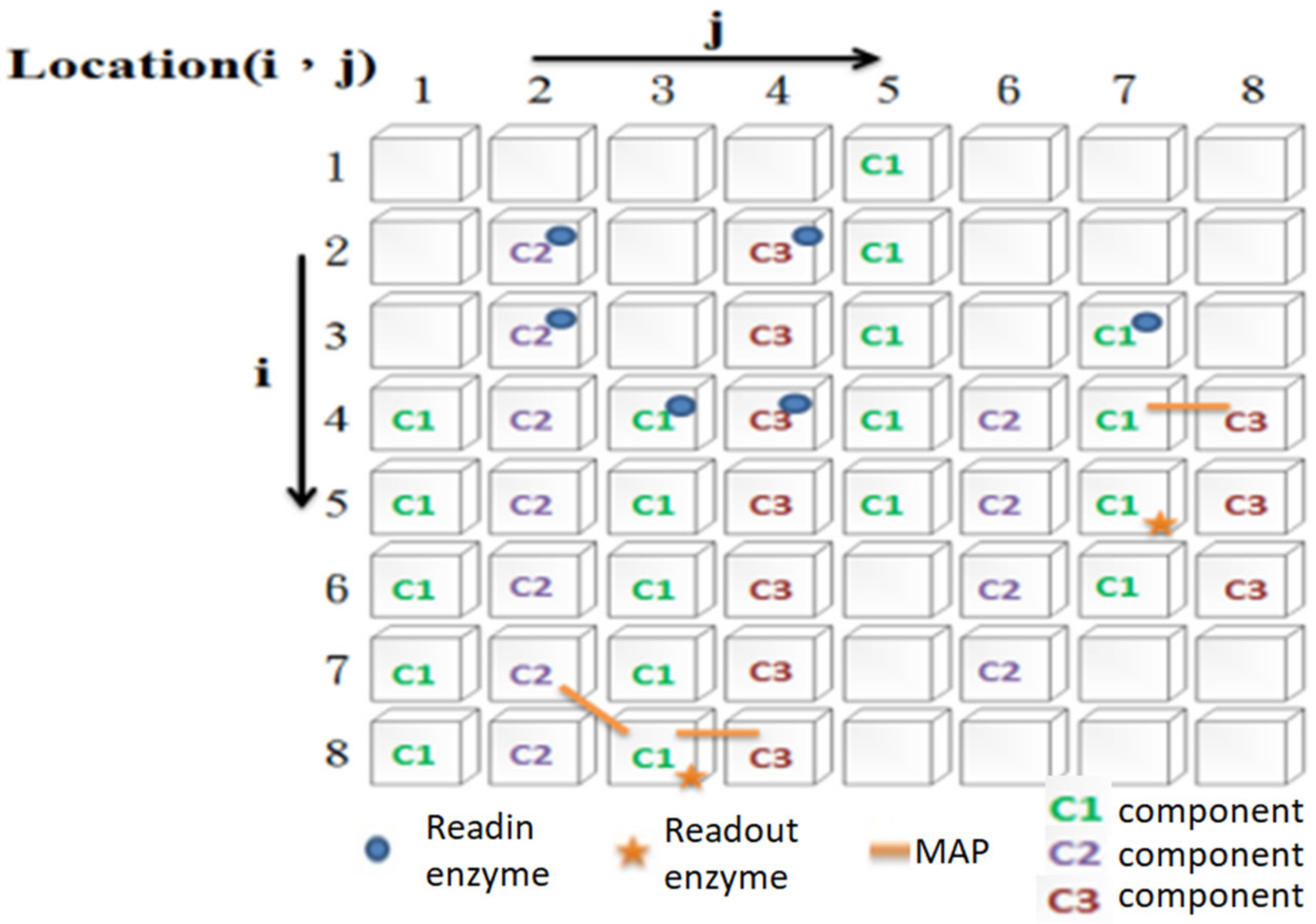
2.2. Information Processing Mechanism of an IP Neuron
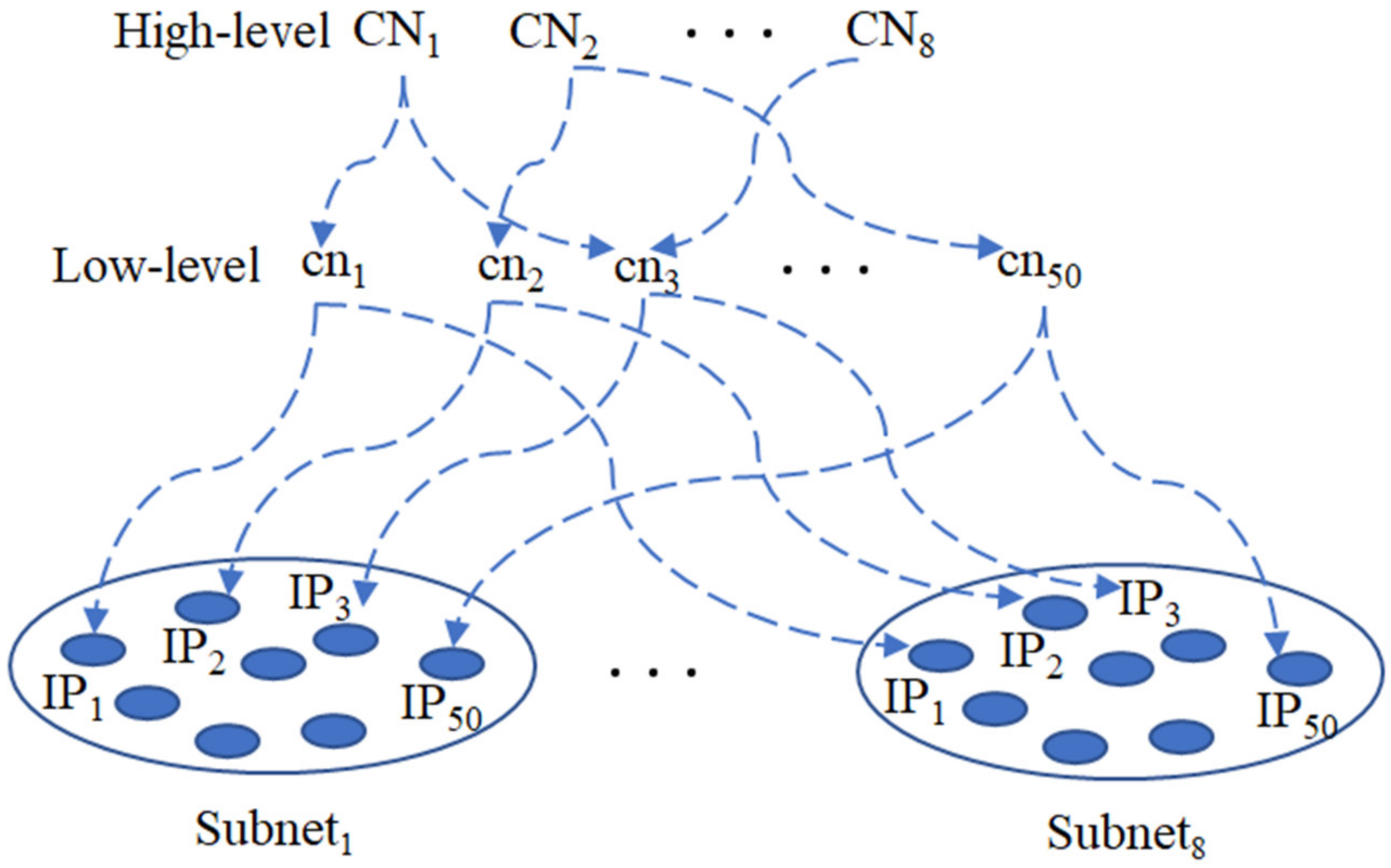
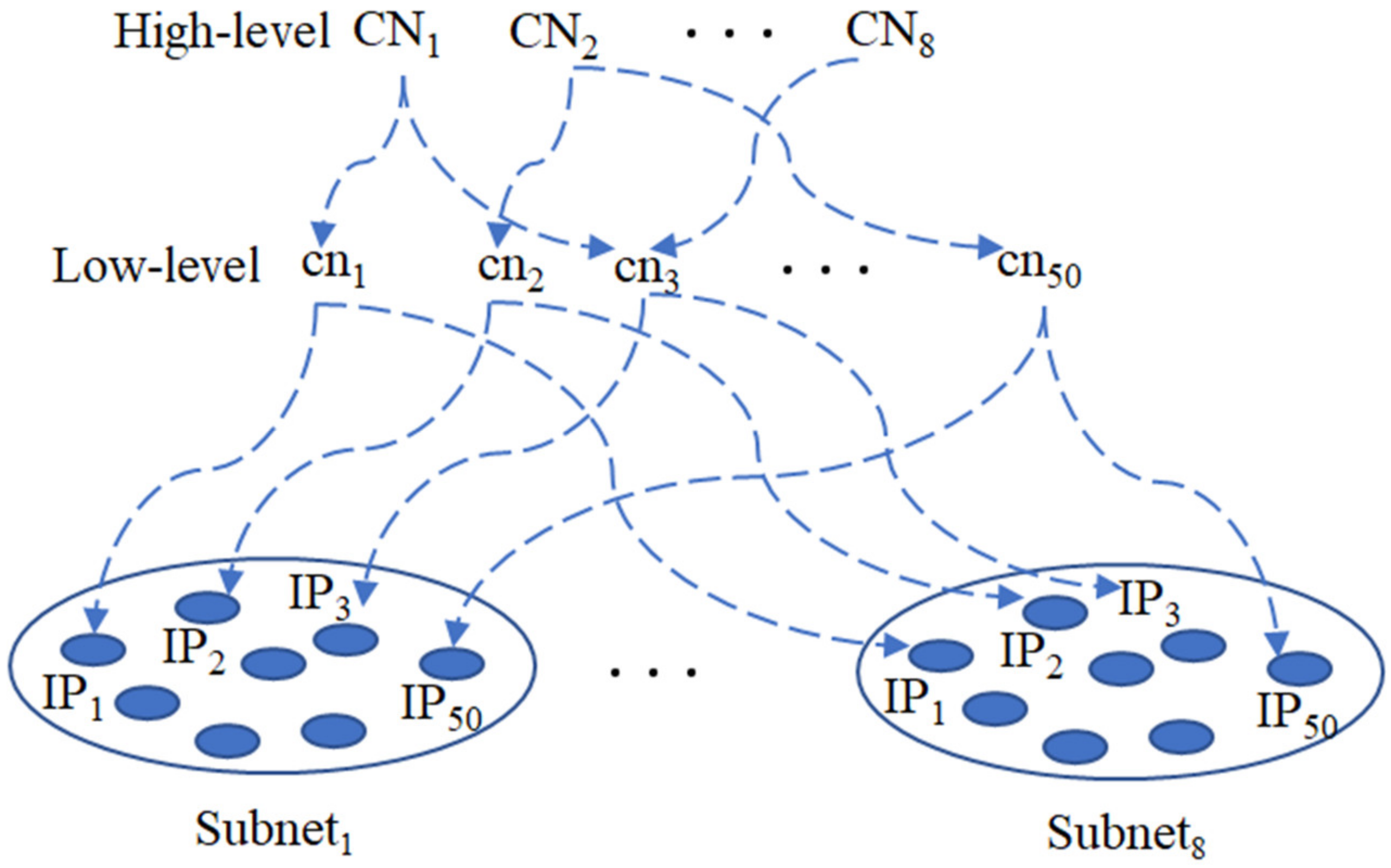
2.3. Information Processing Networks
2.4. Control Networks
2.5. Evolutionary Learning at the Level of IP Neurons
- Evaluate the suitability of each subnet;
- Select the subnet with better performance;
- Copy and mutate from a better-performing subnet to a poorer subnet. The copy and mutation step occurs between the same bundle of IP neurons (the copying and mutation of C1, C2, and C3 signal transmission components on the cytoskeleton, MAP, readin, readout, and pattern of connections with input).
2.6. Evolutionary Learning at the Level of CN Neurons
- Evaluate the fitness of IP neurons selected by high-level CN neurons (via low-level CN neurons);
- Select high-level CN neurons with better performance;
- Copy and make mutations change from high-level CN neurons with better performance to relatively poor high-level CN neurons. The copy and mutation step occurs in the combination of low-level CN neurons selected by high-level CN neurons.
3. Application Domain
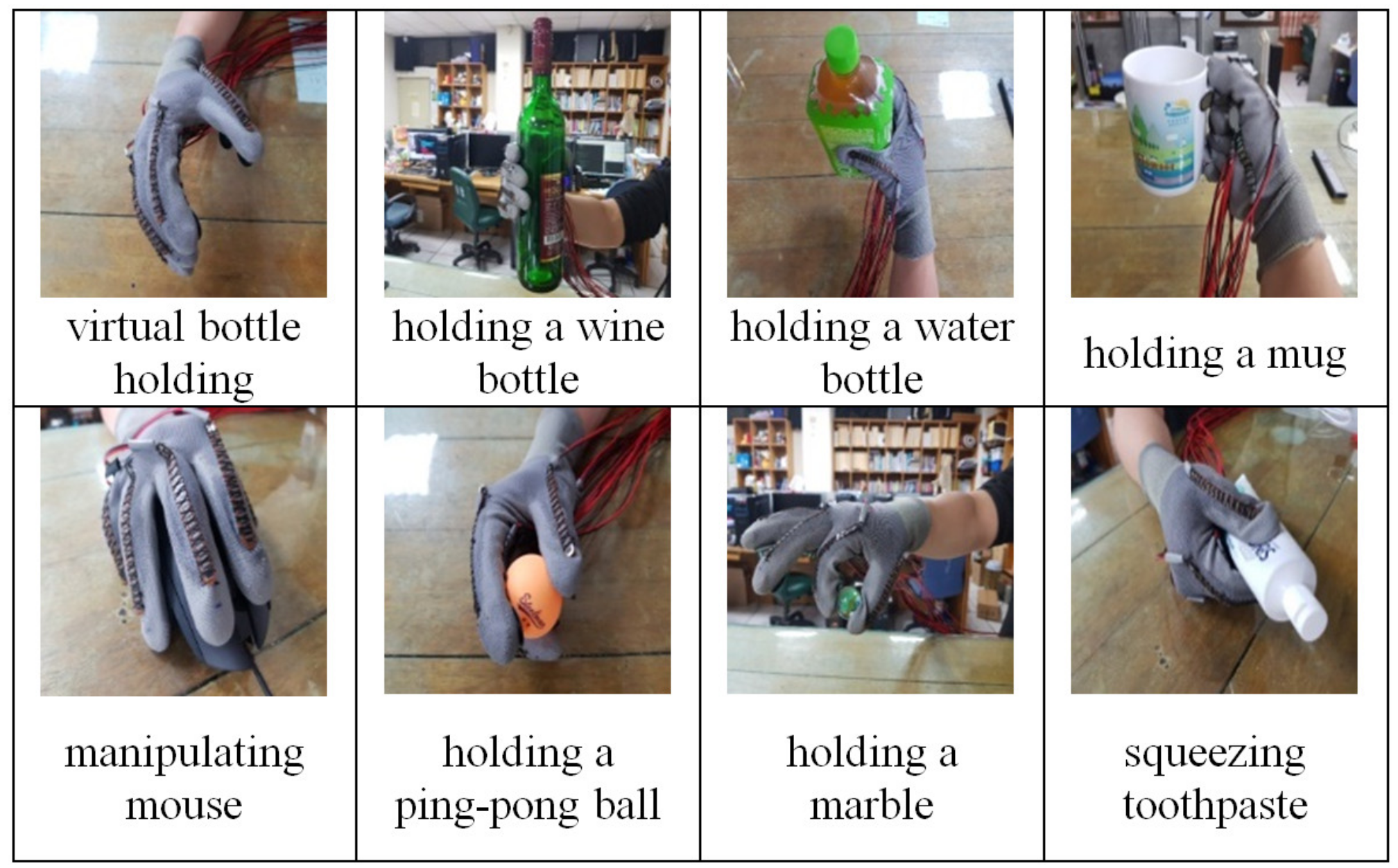
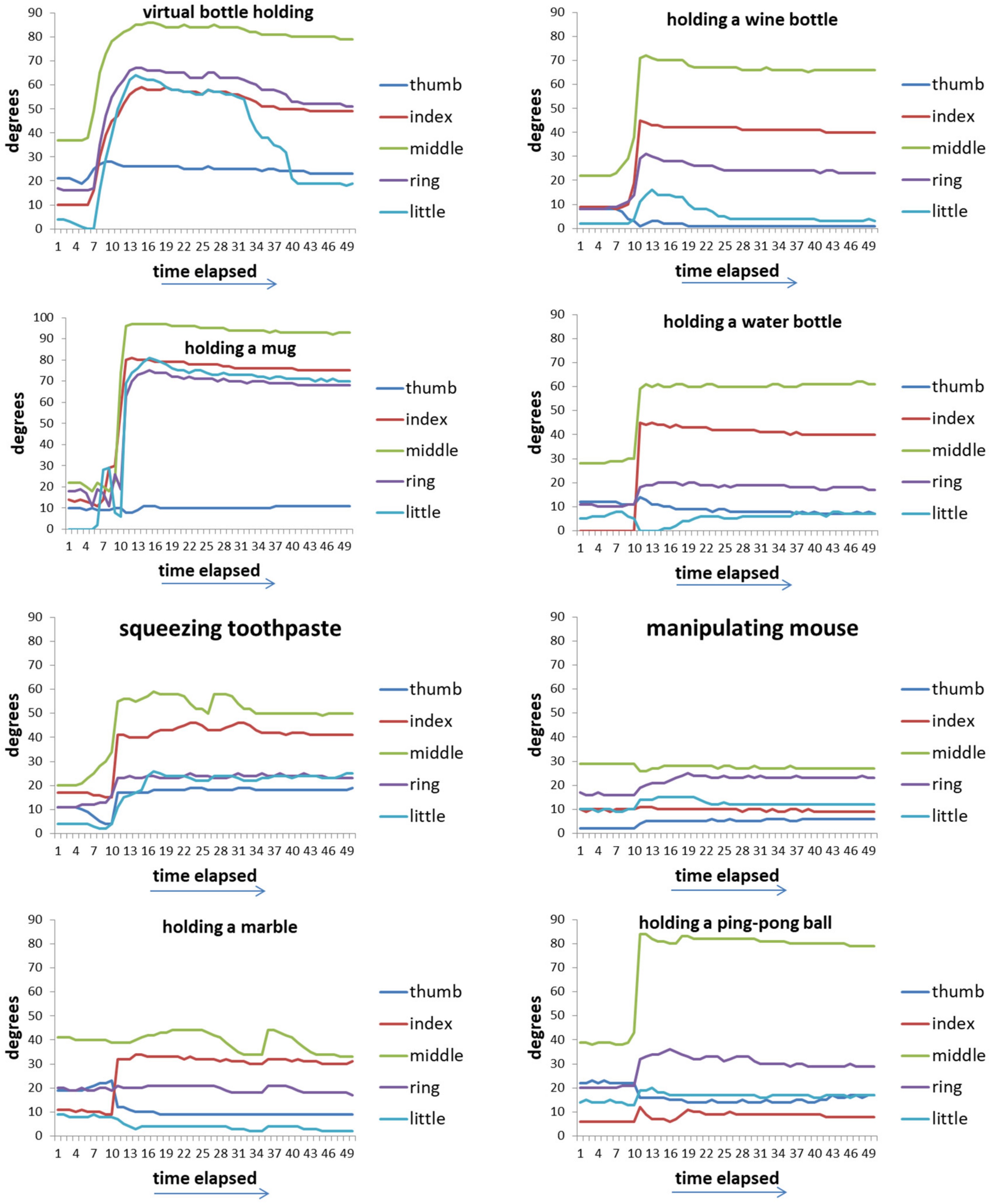
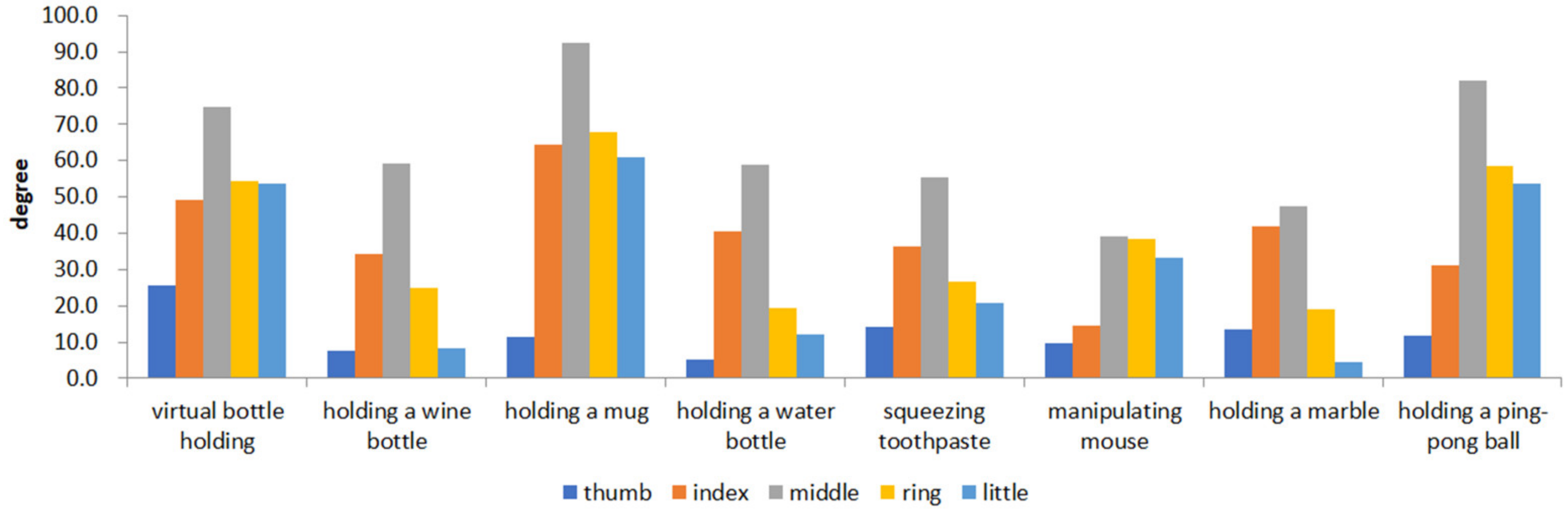
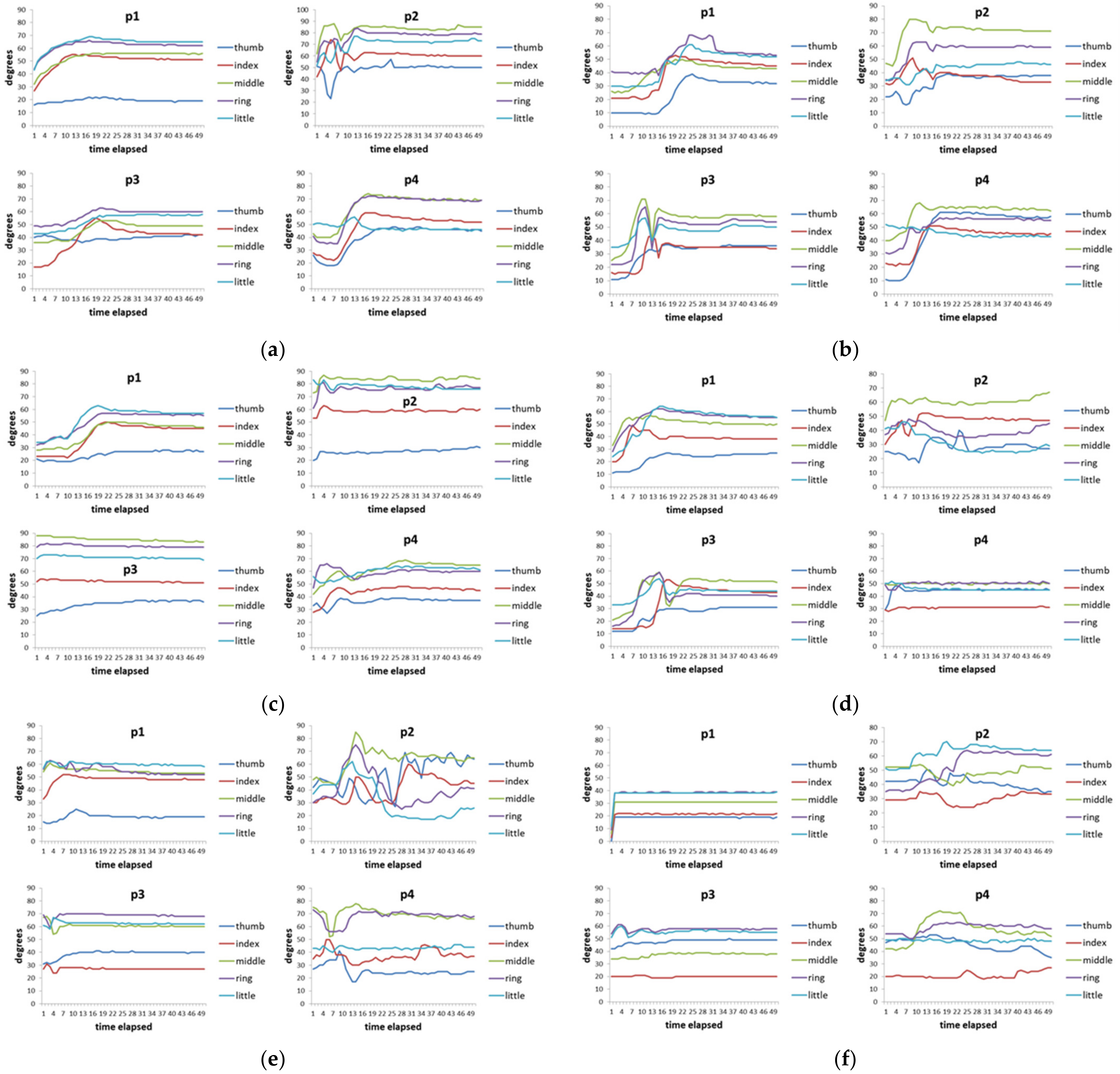
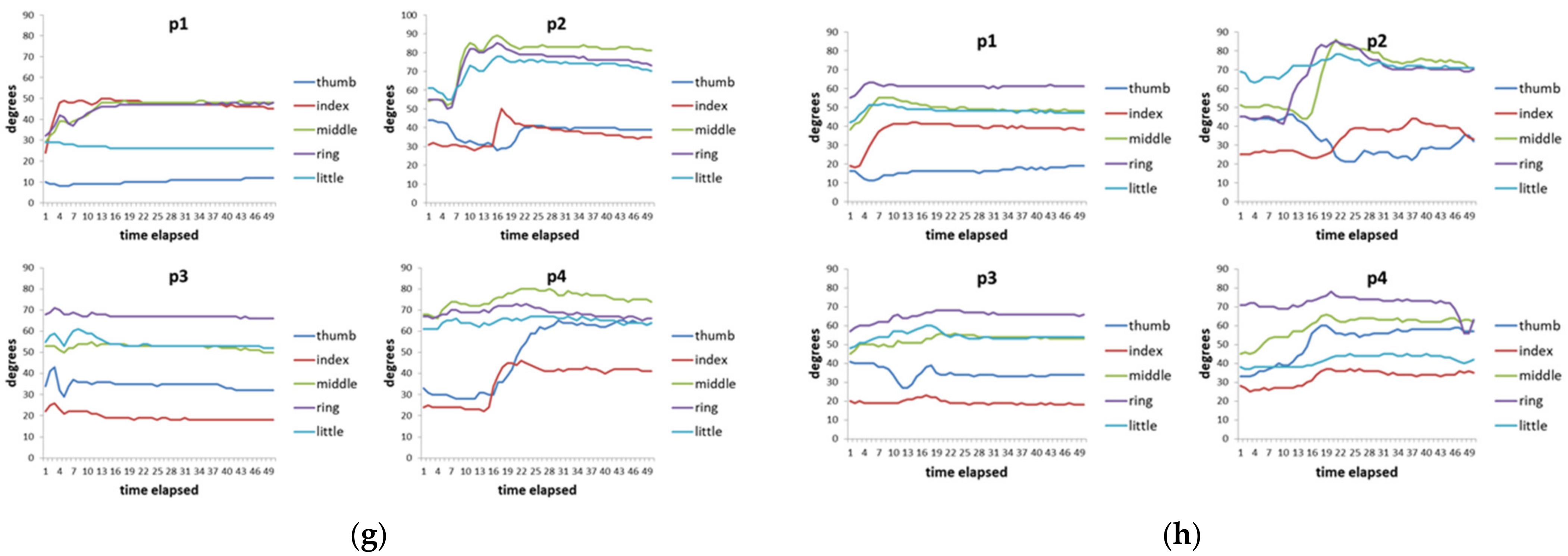
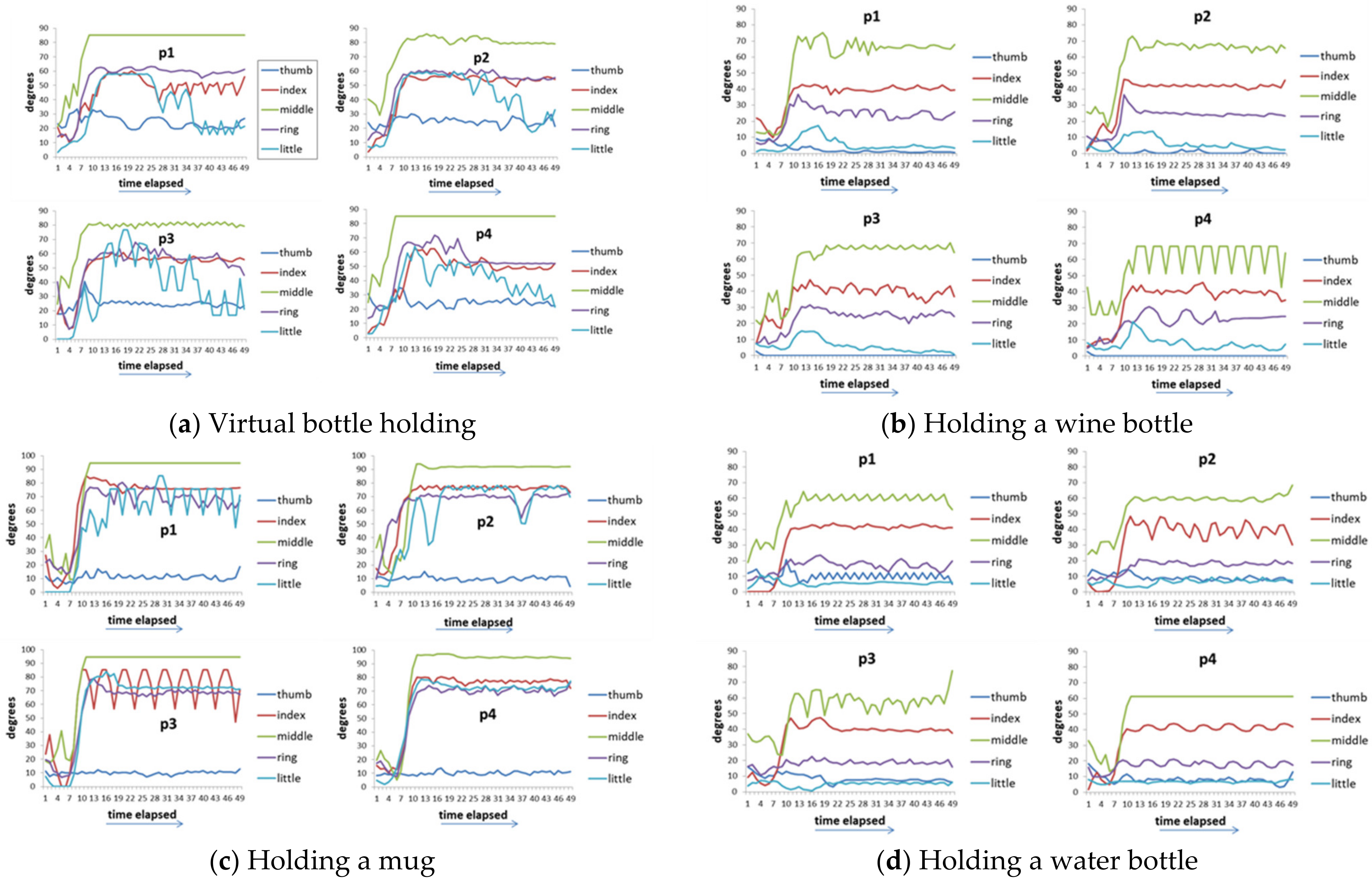
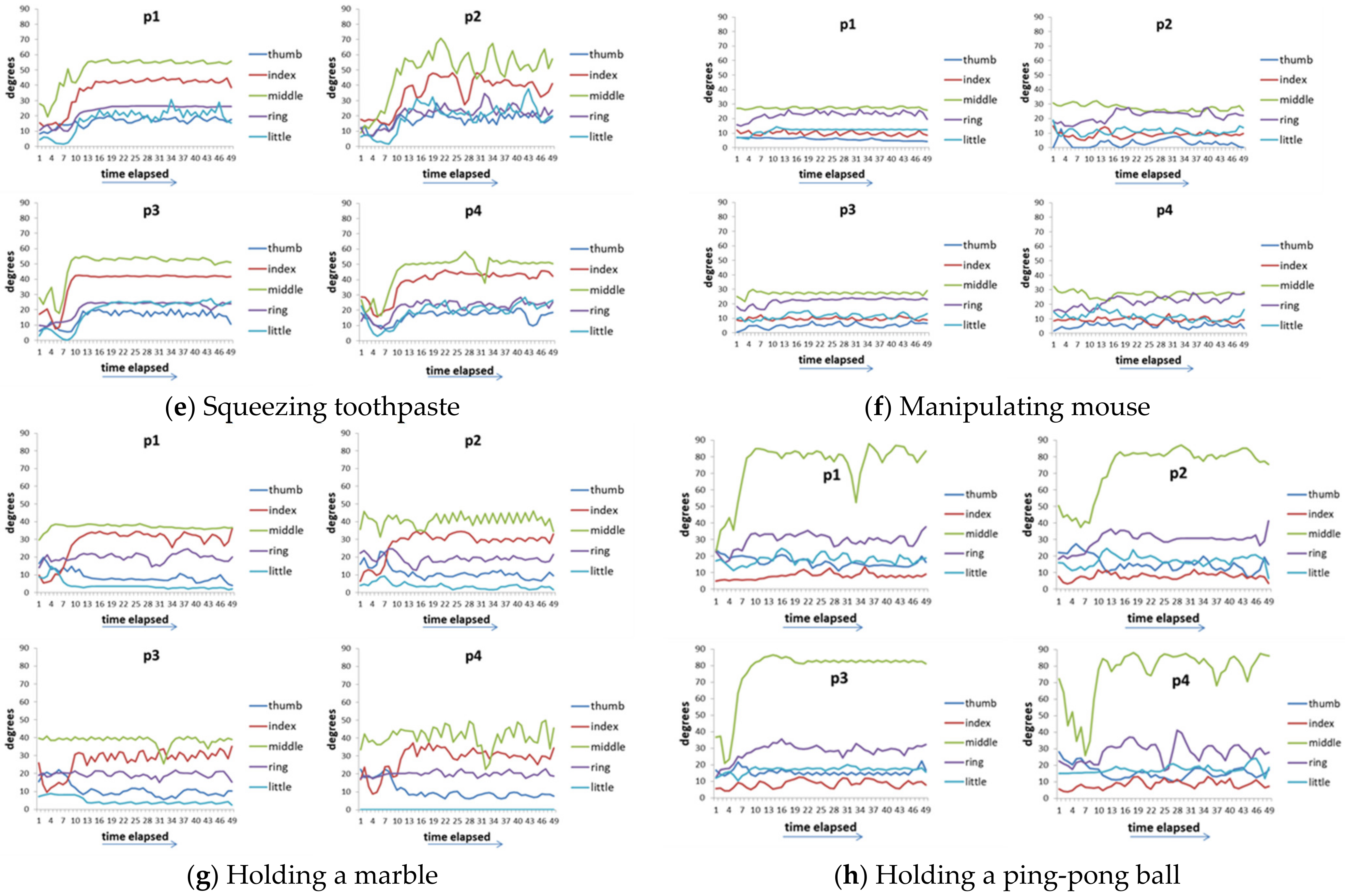
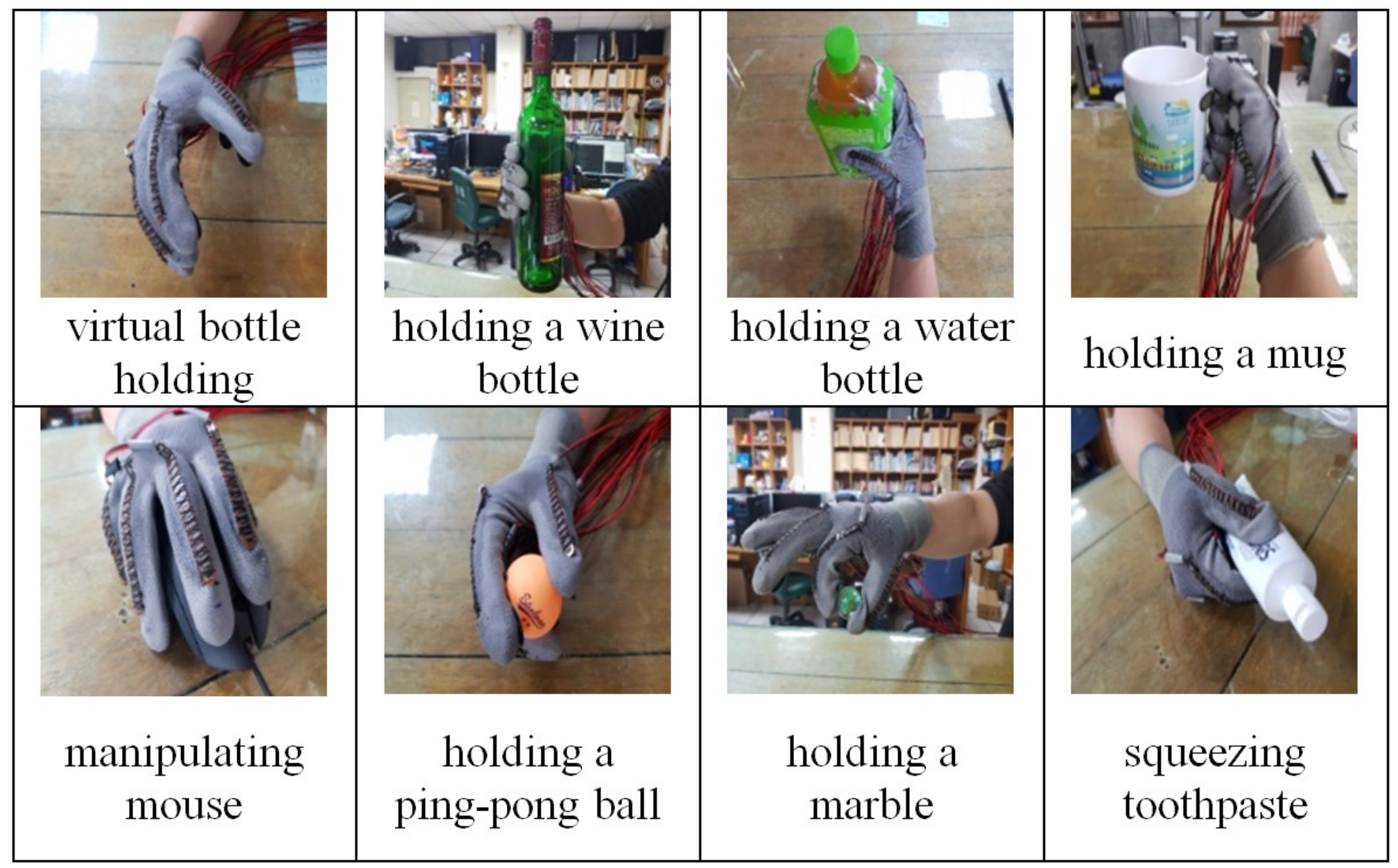
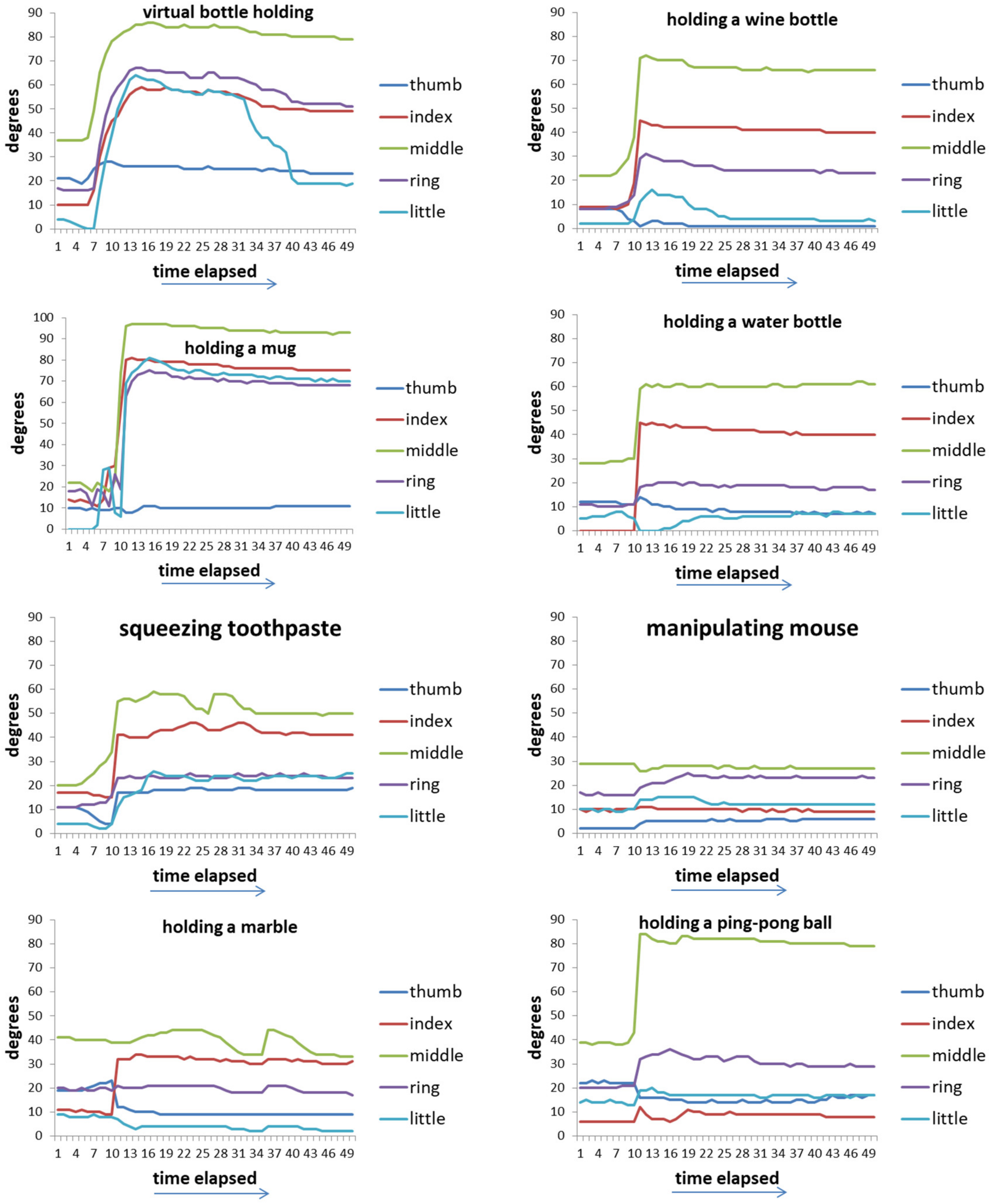
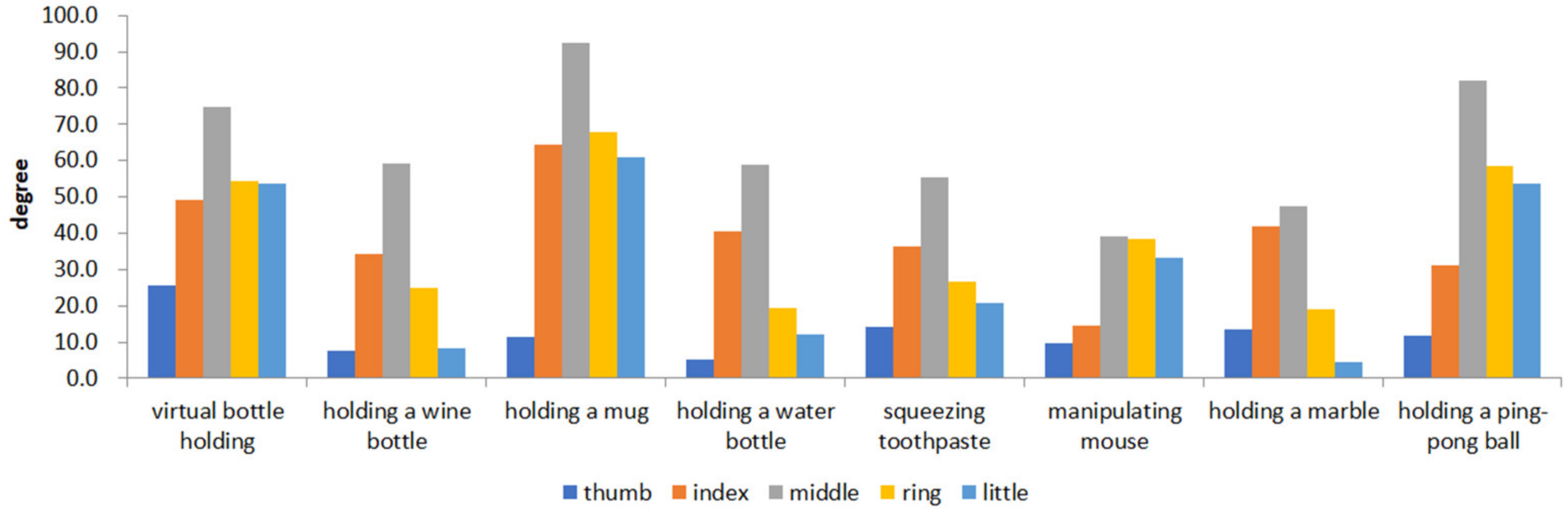
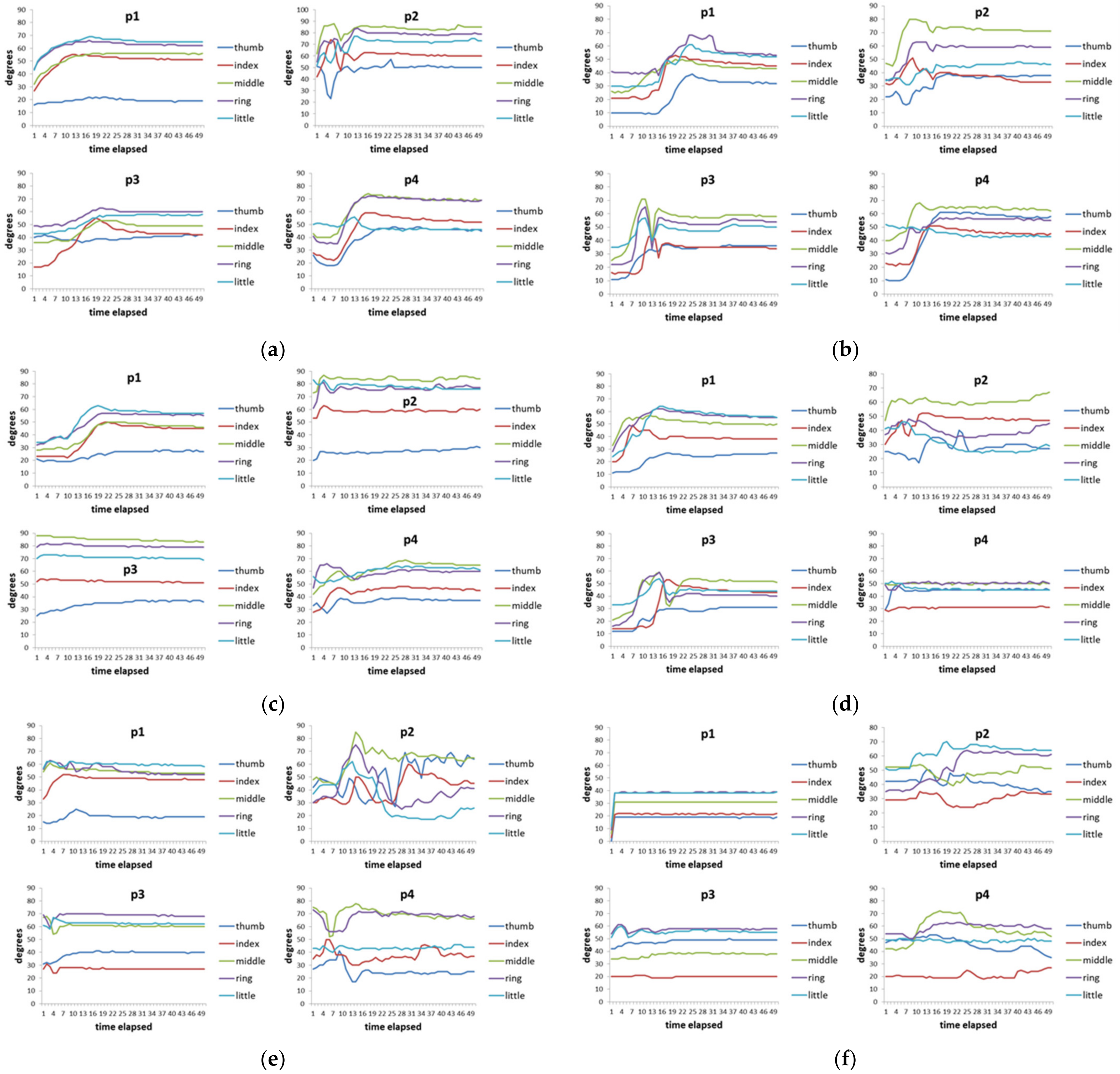
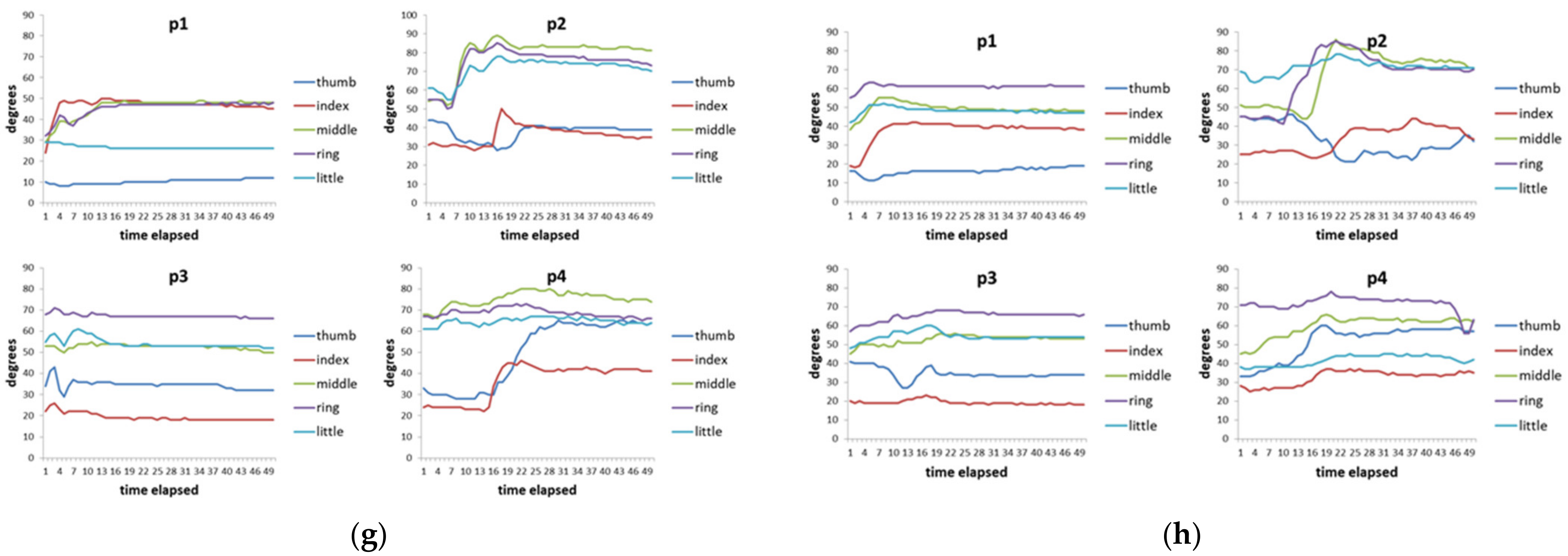
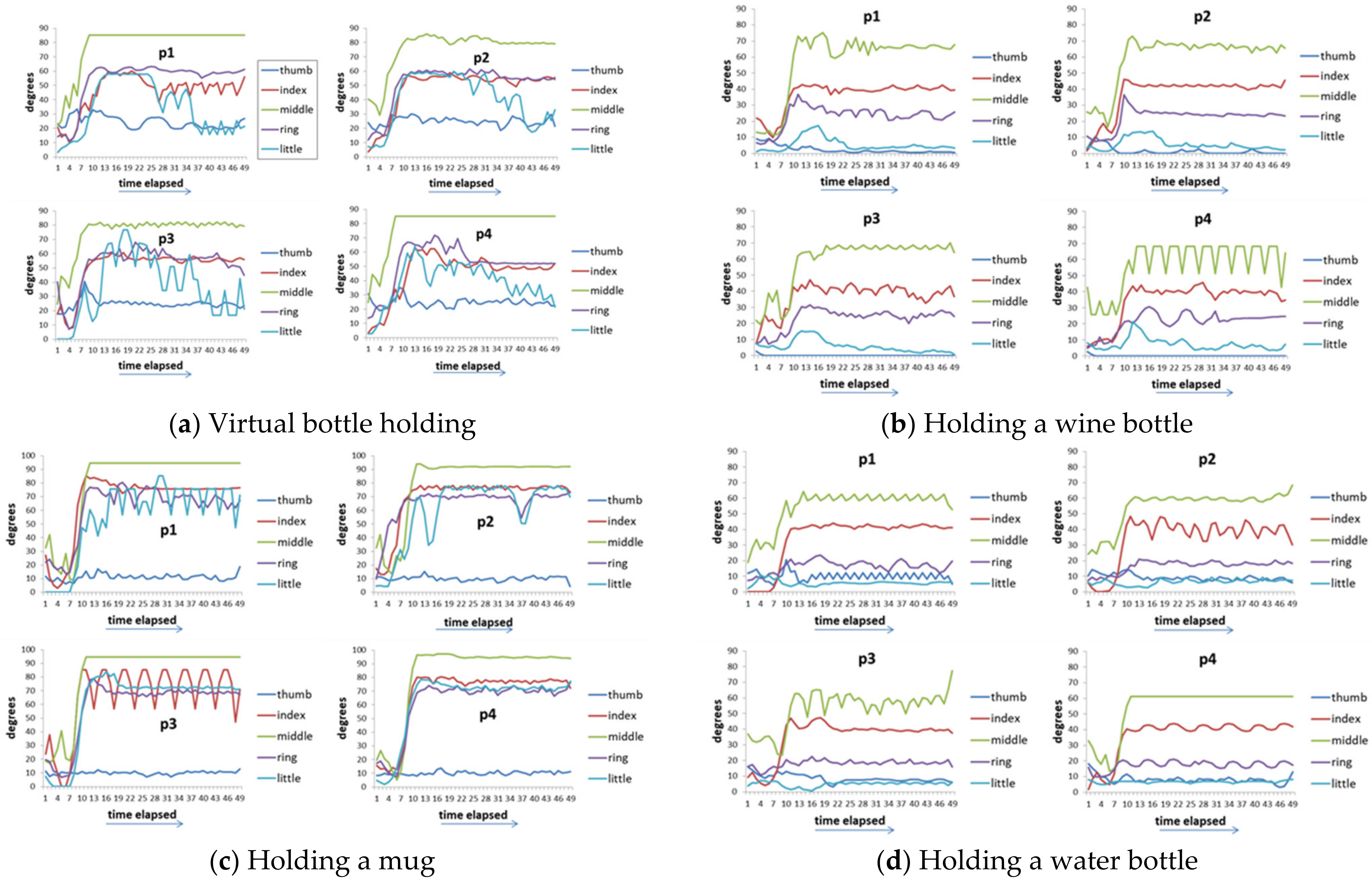
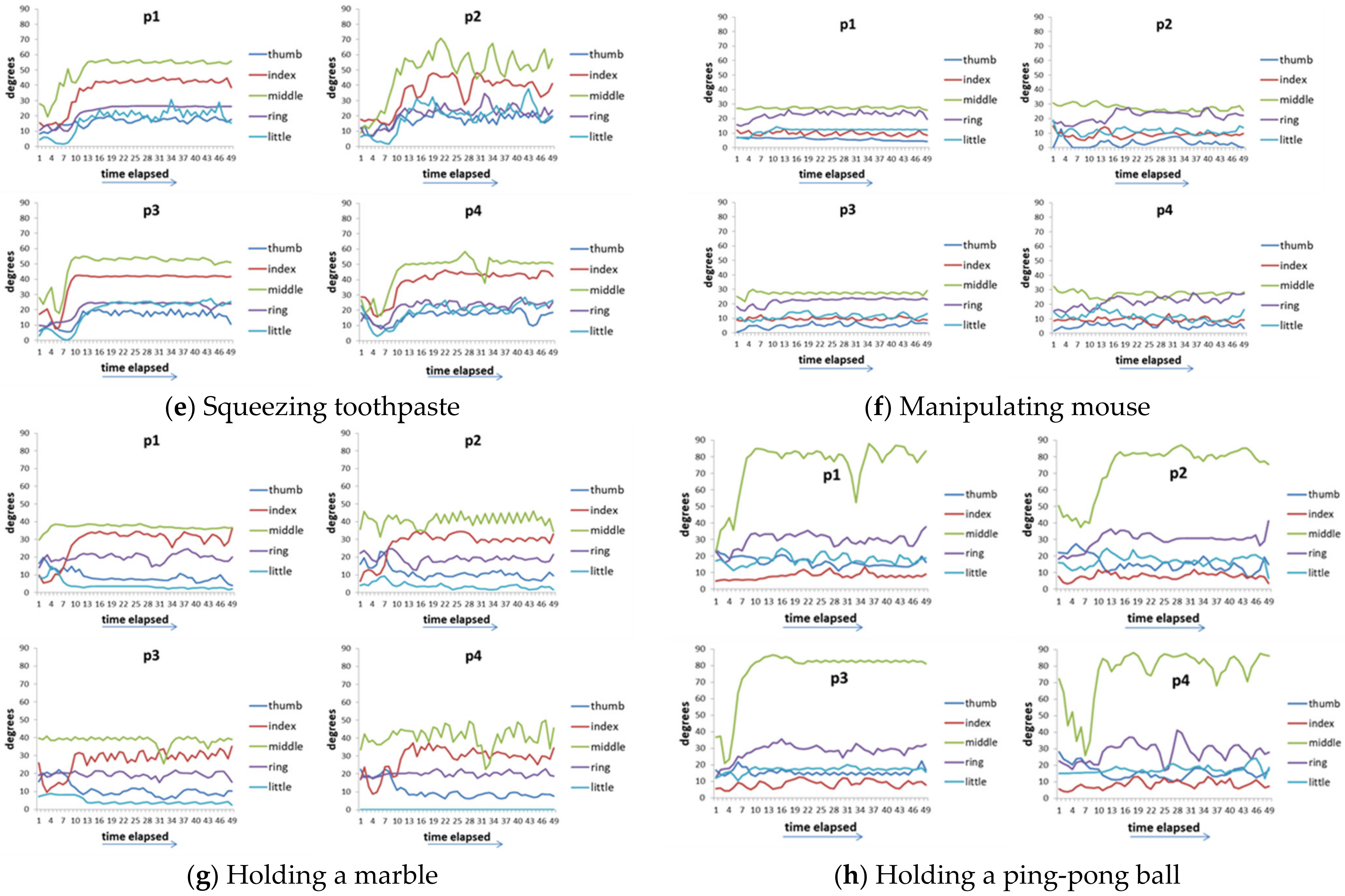
3.1. Experimental Daily Actions
3.2. Input/Output Interface
3.3. Fitness Function
4. Experiments
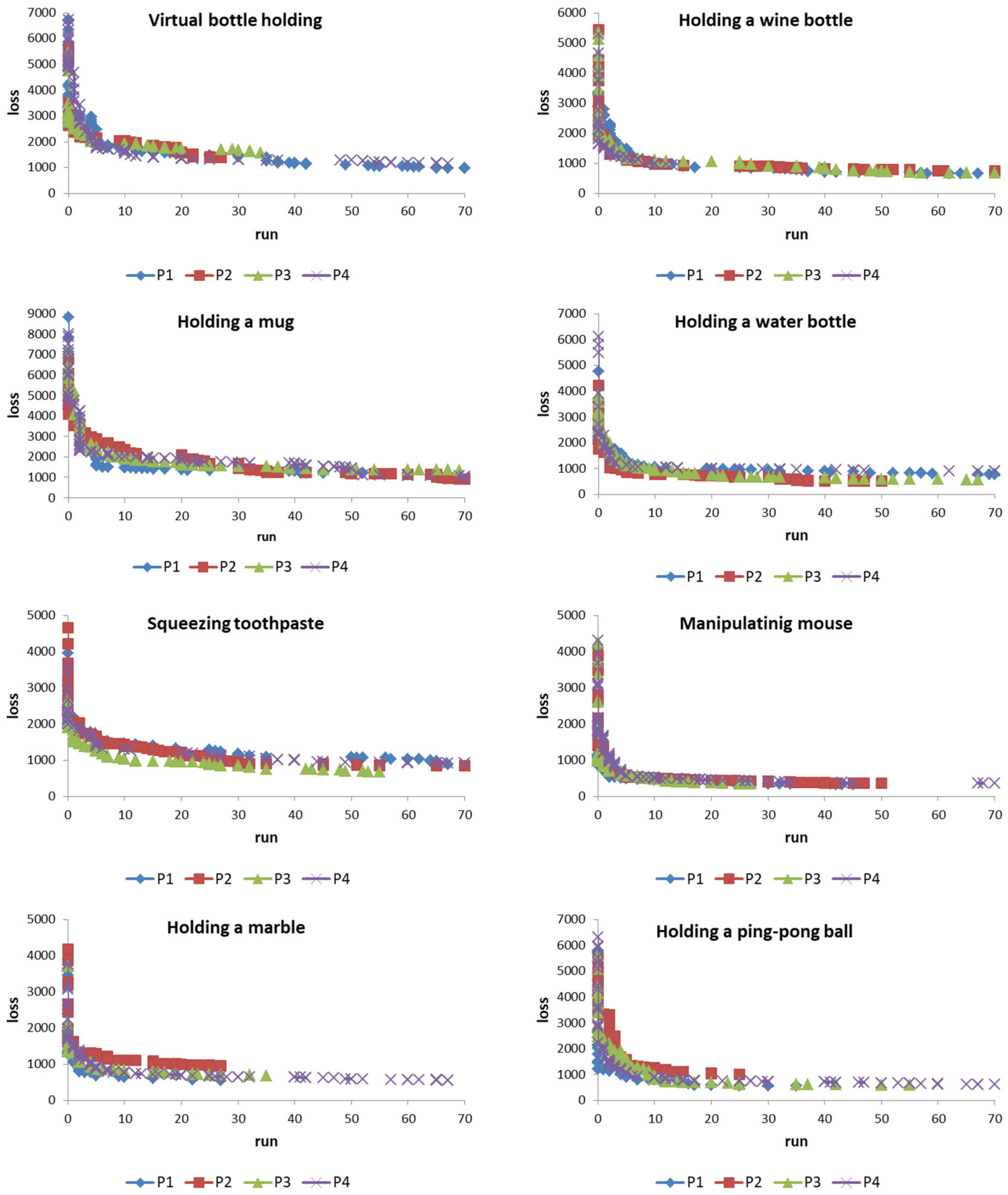
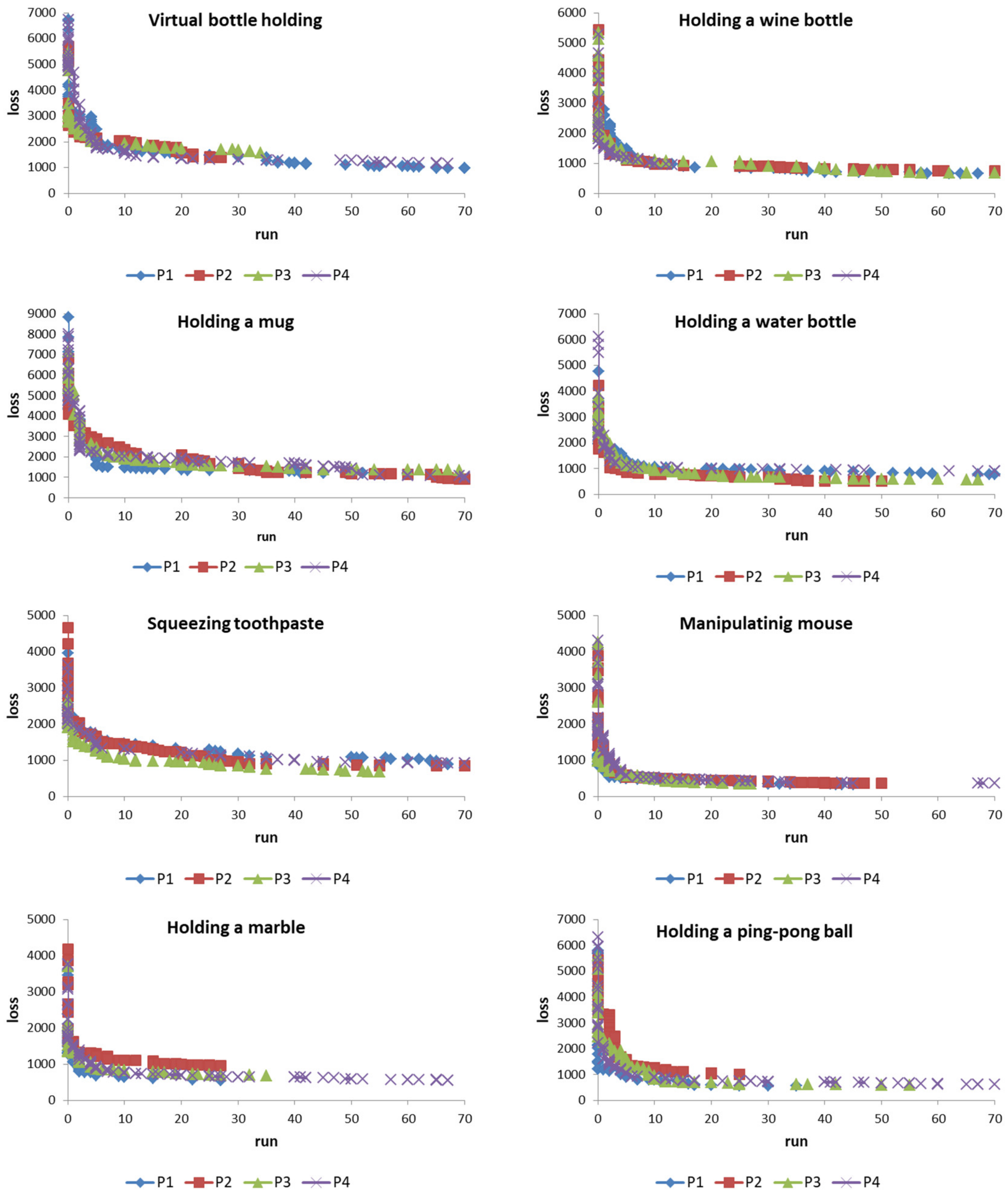
4.1. Adaptive Learning
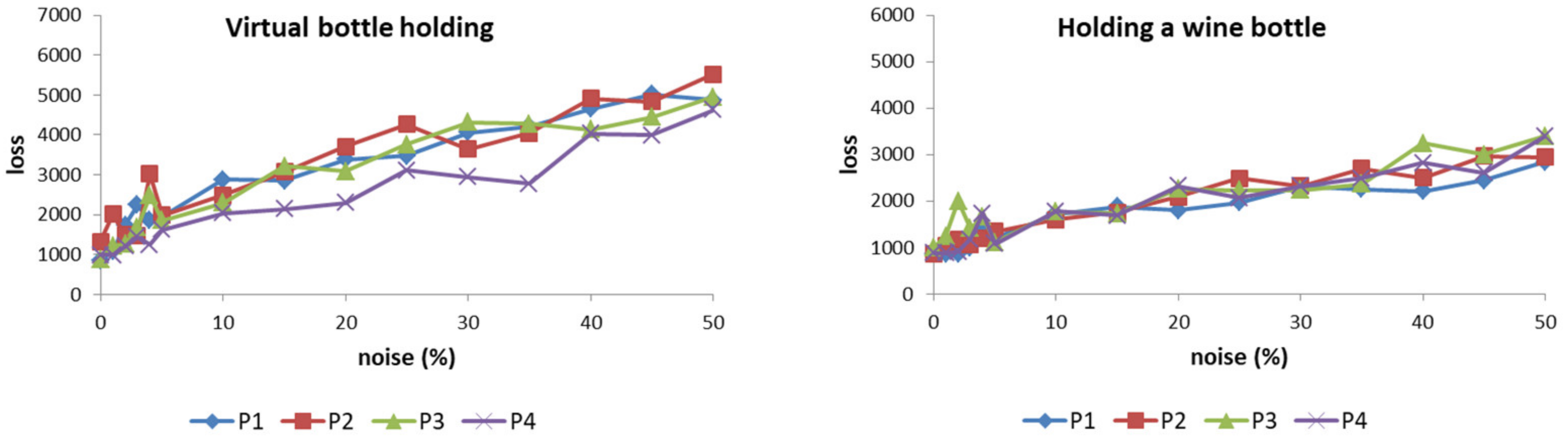
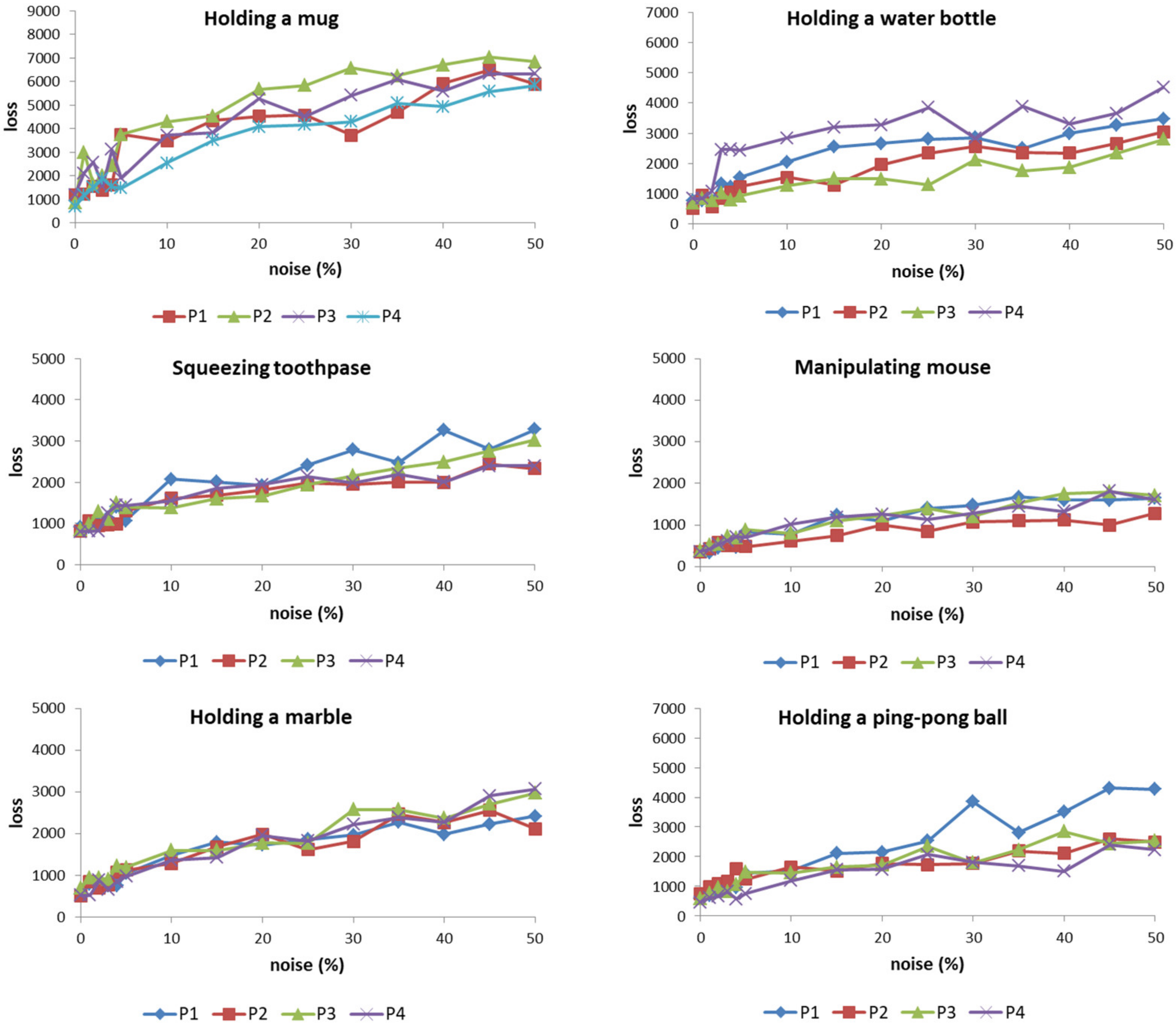
4.2. Noise Tolerance
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, V.S.; Krakauer, J.W. Robotic neurorehabilitation: A computational motor learning perspective. J. Neuroeng. Rehabil. 2009, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.A.; Jhala, M.P. A survey on perspective about the role of robotics in neurorehabilitation among physiotherapists of Ahmedabad. Int. J. Health Sci. 2022, 12, 223–228. [Google Scholar] [CrossRef]
- Rashid, A.; Hasan, O. Wearable technologies for hand joints monitoring for rehabilitation: A survey. Microelectron. J. 2019, 88, 173–183. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Toy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.S.; Lee, I.J.; Yang, S.Y.; Lo, Y.C.; Lee, J.; Chen, J.L. Design of an Inertial-Sensor-Based Data Glove for Hand Function Evaluation. Sensors 2018, 18, 1545. [Google Scholar] [CrossRef]
- Lin, B.S.; Lee, I.J.; Chiang, P.Y.; Huang, S.Y.; Peng, C.W. A Modular Data Glove System for Finger and Hand Motion Capture Based on Inertial Sensors. J. Med. Biol. Eng. 2019, 39, 532–540. [Google Scholar] [CrossRef]
- Lin, B.S.; Lee, I.J.; Chen, J.L. Novel Assembled Sensorized Glove Platform for Comprehensive Hand Function Assessment by Using Inertial Sensors and Force Sensing Resistors. IEEE Sens. J. 2020, 20, 3379–3389. [Google Scholar] [CrossRef]
- Pham, T.; Pathirana, P.N.; Trinh, H.; Fay, P. A non-contact measurement system for the range of motion of the hand. Sensors 2015, 15, 18315–18333. [Google Scholar] [CrossRef]
- Fahn, C.-S.; Sun, H. Development of a fingertip glove equipped with magnetic tracking sensors. Sensors 2010, 10, 1119–1140. [Google Scholar] [CrossRef]
- Jarque-Bou, N.J.; Scano, A.; Atzori, M.; Müller, H. Kinematic synergies of hand grasps: A comprehensive study on a large publicly available dataset. J. Neuroeng. Rehabil. 2019, 16, 63. [Google Scholar] [CrossRef]
- O’Flynn, B.; Sachez-Torres, J.; Tedesco, S.; Downes, B.; Connolly, J.; Condell, J.; Curran, K. Novel Smart Glove Technology as a Biomechanical Monitoring Tool. Sens. Transducers 2015, 193, 23–32. [Google Scholar]
- Sundaram, S.; Kellnhofer, P.; Li, Y.; Zhu, J.-Y.; Torralba, A.; Matusik, W. Learning the signatures of the human grasp using a scalable tactile glove. Nature 2019, 569, 698–702. [Google Scholar] [CrossRef]
- Fahn, C.-S.; Sun, H. Development of a dataglove with reducing sensors based on magnetic induction. IEEE Trans. Ind. Electron. 2005, 52, 585–594. [Google Scholar] [CrossRef]
- Kim, D.H.; Lee, S.W.; Park, H.-S. Improving kinematic accuracy of soft wearable data gloves by optimizing sensor locations. Sensors 2016, 16, 766. [Google Scholar] [CrossRef]
- Connolly, J.; Condell, J.; O’Flynn, B.; Sanchez, J.T.; Gardiner, P. IMU sensor-based electronic goniometric glove for clinical finger-action analysis. IEEE Sens. J. 2018, 18, 1273–1281. [Google Scholar]
- de Pasquale, G. Glove-based systems for medical applications: Review of recent advancements. J. Text. Eng. Fash. Technol. 2018, 4, 286–295. [Google Scholar] [CrossRef]
- Henderson, J.; Condell, J.; Connolly, J.; Kelly, D.; Curran, K. Review of Wearable Sensor-Based Health Monitoring Glove Devices for Rheumatoid Arthritis. Sensors 2021, 21, 1576. [Google Scholar] [CrossRef] [PubMed]
- Raval, S.; Patel, B. A Review on grasping principle and robotic grippers. Int. J. Eng. Dev. Res. 2016, 4, 483–490. [Google Scholar]
- Shintake, J.; Cacucciolo, V.; Floreano, D.; Shea, H. Soft robotic grippers. Adv. Mater. 2016, 30, e1707035. [Google Scholar] [CrossRef]
- Zhu, G.; Xiao, X.; Li, C.; Ma, J.; Ponraj, G.; Prituja, A.V.; Ren, H. A bimanual robotic teleoperation architecture with anthropomorphic hybrid grippers for unstructured manipulation tasks. Appl. Sci. 2020, 10, 2086. [Google Scholar] [CrossRef]
- Cotugno, G.; Althoefer, K.; Nanayakkara, T. The role of the thumb: Study of finger motion in grasping and reachability space in human and robotic Hands. IEEE Trans. Syst. Man Cybern. 2017, 47, 1061–1070. [Google Scholar] [CrossRef]
- Kappassov, Z.; Corrales, J.A.; Perdereau, V. Tactile sensing in dexterous robot hands. Rob. Auton. Syst. 2015, 74, 195–220. [Google Scholar] [CrossRef]
- Owen, M.; Au, C.; Fowke, A. Development of a dexterous prosthetic hand. J. Comput. Inf. Sci. Eng. 2018, 18, 010801. [Google Scholar] [CrossRef]
- Segil, J. (Ed.) Handbook of Biomechatronics, 1st ed; Academic Press: Cambridge, MA, USA, 2018; ISBN 9780128125397. [Google Scholar]
- Chen, J.-C.; Conrad, M. A multilevel neuromolecular architecture that uses the extradimensional bypass principle to facilitate evolutionary learning. Phys. D Nonlinear Phenom. 1994, 75, 417–437. [Google Scholar] [CrossRef]
- Chen, J.-C.; Conrad, M. Learning synergy in a multilevel neuronal architecture. Biosystems 1994, 32, 111–142. [Google Scholar] [CrossRef]
- Chen, J.-C. A study of the continuous optimization problem using a wood stick robot controlled by a biologically-motivated system. J. Dyn. Syst. Meas. Control Trans. ASME 2015, 137, 071008. [Google Scholar] [CrossRef]
- Chen, J.-C. Continual learning for addressing optimization problems with a snake-like robot controlled by a self-Organizing model. Appl. Sci. 2020, 10, 4848. [Google Scholar] [CrossRef]
- Chen, J.-C. Using artificial neuro-molecular system in robotic arm motion control—Taking simulation of rehabilitation as an example. Sensors 2022, 22, 2584. [Google Scholar] [CrossRef]
- Priel, A.; Tuszynski, J.A.; Woolf, N.J. Neural cytoskeleton capabilities for learning and memory. J. Biol. Phys. 2010, 36, 3–21. [Google Scholar] [CrossRef]
- Lynch, G.; Rex, C.S.; Chen, L.Y.; Gall, C.M. The substrates of memory: Defects, treatments, and enhancement. Eur. J. Pharmacol. 2008, 585, 2–13. [Google Scholar] [CrossRef]
- Prager-Khoutorsky, M.; Spira, M.E. Neurite retraction and regrowth regulated by membrane retrieval, membrane supply, and actin dynamics. Brain Res. 2009, 1251, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Fujii-Taira, I.; Murakami, A.; Hirose, N.; Aoki, N.; Izawa, E.; Fujimoto, Y.; Takano, T.; Matsushima, T.; Homma, K.J. Up-regulation of microtubule-associated protein 2 accompanying the filial imprinting of domestic chicks (Gallus gallus domesticus). Brain Res. Bull. 2008, 76, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Randolph, W.P.; Debra, L.L.; Daniel, S.L.; David, J.C.; Edith, G.M.; Patrick, L.M.; Irene, E.D.; Ronald, F.Z.; Robert, E.B.; Kerry, L.C.; et al. Parallel distributed processing and neural networks: Origins, methodology and cognitive functions. Int. J. Neurosci. 1991, 60, 195–214. [Google Scholar] [CrossRef]
- Feix, T.; Romero, J.; Schmiedmayer, H.-B.; Dollar, A.M.; Kragic, D. The grasp taxonomy of human grasp types. IEEE Trans. Human-Mach. Syst. 2015, 46, 66–77. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P1 | P2 | P3 | P4 | |||||
|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Before | After | Before | After | |
| Virtual bottle holding | 27.0 | 3.9 | 22.8 | 5.3 | 22.0 | 3.5 | 27.0 | 4.0 |
| Holding a wine bottle | 18.2 | 3.4 | 21.8 | 3.4 | 21.4 | 3.9 | 21.1 | 3.5 |
| Holding a water bottle | 19.0 | 3.0 | 16.8 | 2.1 | 15.3 | 2.8 | 24.4 | 3.4 |
| Holding a mug | 35.3 | 4.7 | 27.2 | 3.5 | 28.7 | 4.8 | 32.1 | 2.7 |
| Squeezing toothpaste | 15.8 | 3.6 | 18.6 | 3.3 | 10.6 | 3.4 | 14.5 | 3.2 |
| Manipulating mouse | 23.2 | 2.3 | 21.7 | 3.0 | 22.4 | 2.4 | 25.3 | 1.9 |
| Holding a marble | 14.3 | 2.2 | 16.7 | 2.1 | 14.8 | 2.8 | 15.1 | 2.1 |
| Holding a ping-pong | 10.4 | 1.4 | 15.5 | 1.4 | 17.0 | 1.6 | 17.2 | 1.4 |
| Virtual Bottle Holding | Holding a Wine Bottle | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| p1 | p2 | p3 | p4 | Healthy | p1 | p2 | p3 | p4 | Healthy | ||
| p1 | 0 | 9171 | 5014 | 6712 | 6742 | p1 | 0 | 6666 | 5746 | 6753 | 4550 |
| p2 | 0 | 6600 | 7870 | 7686 | p2 | 0 | 5282 | 5988 | 5441 | ||
| p3 | 0 | 5840 | 6327 | p3 | 0 | 5675 | 5359 | ||||
| p4 | 0 | 6370 | p4 | 0 | 5270 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Holding a mug | Holding a water bottle | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 7327 | 8448 | 5811 | 8821 | p1 | 0 | 4316 | 4379 | 3922 | 4756 |
| p2 | 0 | 6533 | 4810 | 6794 | p2 | 0 | 3854 | 4849 | 4310 | ||
| p3 | 0 | 5367 | 7266 | p3 | 0 | 4511 | 3835 | ||||
| p4 | 0 | 7533 | p4 | 0 | 6112 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Squeezing toothpaste | Manipulating mouse | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 5765 | 6669 | 5759 | 3948 | p1 | 0 | 5138 | 4763 | 5131 | 2601 |
| p2 | 0 | 5551 | 6181 | 4661 | p2 | 0 | 3768 | 4337 | 3879 | ||
| p3 | 0 | 5129 | 2661 | p3 | 0 | 4228 | 4259 | ||||
| p4 | 0 | 3625 | p4 | 0 | 4307 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Holding a marble | Holding a ping-pong ball | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 7243 | 5313 | 6941 | 3587 | p1 | 0 | 6324 | 5365 | 6372 | 5809 |
| p2 | 0 | 5150 | 7094 | 4174 | p2 | 0 | 4846 | 6227 | 5425 | ||
| p3 | 0 | 7022 | 3698 | p3 | 0 | 6562 | 5600 | ||||
| p4 | 0 | 3775 | p4 | 0 | 6326 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Virtual Bottle Holding | Holding a Wine Bottle | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| p1 | p2 | p3 | p4 | Healthy | p1 | p2 | p3 | p4 | Healthy | ||
| p1 | 0 | 5044 | 3328 | 2992 | 862 | p1 | 0 | 5802 | 5065 | 5923 | 549 |
| p2 | 0 | 3958 | 3195 | 1325 | p2 | 0 | 5225 | 4906 | 1135 | ||
| p3 | 0 | 3152 | 884 | p3 | 0 | 4568 | 1180 | ||||
| p4 | 0 | 989 | p4 | 0 | 884 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Holding a mug | Holding a water bottle | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 4936 | 5364 | 5765 | 1178 | p1 | 0 | 3490 | 4033 | 5454 | 719 |
| p2 | 0 | 4630 | 5626 | 869 | p2 | 0 | 3403 | 4513 | 643 | ||
| p3 | 0 | 4598 | 1196 | p3 | 0 | 4310 | 934 | ||||
| p4 | 0 | 684 | p4 | 0 | 1140 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Squeezing toothpaste | Manipulating mouse | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 4677 | 6126 | 5405 | 905 | p1 | 0 | 6999 | 6194 | 6834 | 338 |
| p2 | 0 | 6429 | 5462 | 819 | p2 | 0 | 6163 | 6936 | 358 | ||
| p3 | 0 | 4916 | 854 | p3 | 0 | 5297 | 389 | ||||
| p4 | 0 | 804 | p4 | 0 | 356 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Holding a marble | Holding a ping-pong ball | ||||||||||
| p1 | p2 | p3 | p4 | healthy | p1 | p2 | p3 | p4 | healthy | ||
| p1 | 0 | 6712 | 5149 | 7606 | 563 | p1 | 0 | 5801 | 4826 | 5124 | 578 |
| p2 | 0 | 5892 | 6409 | 519 | p2 | 0 | 5097 | 6047 | 755 | ||
| p3 | 0 | 7738 | 697 | p3 | 0 | 6817 | 602 | ||||
| p4 | 0 | 528 | p4 | 0 | 470 | ||||||
| healthy | 0 | healthy | 0 | ||||||||
| Virtual Bottle Holding | Holding a Wine Bottle | Holding a Mug | Holding a Water Bottle | Squeezing Toothpaste | Manipulating Mouse | Holding a Marble | Holding a Ping-Pong Ball | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ANM | MLP | ANM | MLP | ANM | MLP | ANM | MLP | ANM | MLP | ANM | MLP | ANM | MLP | ANM | MLP | |
| p1 | 861 | 1278 | 548 | 823 | 1177 | 947 | 760 | 919 | 905 | 639 | 338 | 1361 | 562 | 1510 | 578 | 519 |
| p2 | 1325 | 1504 | 854 | 674 | 869 | 2061 | 643 | 934 | 818 | 401 | 358 | 984 | 518 | 1051 | 754 | 455 |
| p3 | 884 | 1324 | 986 | 639 | 1195 | 1276 | 706 | 1053 | 853 | 757 | 388 | 1088 | 696 | 1121 | 601 | 493 |
| p4 | 988 | 1295 | 883 | 680 | 684 | 712 | 841 | 1137 | 803 | 512 | 355 | 601 | 527 | 1623 | 469 | 592 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-C. Bridging the Finger-Action Gap between Hand Patients and Healthy People in Daily Life with a Biomimetic System. Biomimetics 2023, 8, 76. https://doi.org/10.3390/biomimetics8010076
Chen J-C. Bridging the Finger-Action Gap between Hand Patients and Healthy People in Daily Life with a Biomimetic System. Biomimetics. 2023; 8(1):76. https://doi.org/10.3390/biomimetics8010076
Chicago/Turabian StyleChen, Jong-Chen. 2023. "Bridging the Finger-Action Gap between Hand Patients and Healthy People in Daily Life with a Biomimetic System" Biomimetics 8, no. 1: 76. https://doi.org/10.3390/biomimetics8010076
APA StyleChen, J.-C. (2023). Bridging the Finger-Action Gap between Hand Patients and Healthy People in Daily Life with a Biomimetic System. Biomimetics, 8(1), 76. https://doi.org/10.3390/biomimetics8010076