
Pike River Mine Disaster: Systems-Engineering and Organisational Contributions


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
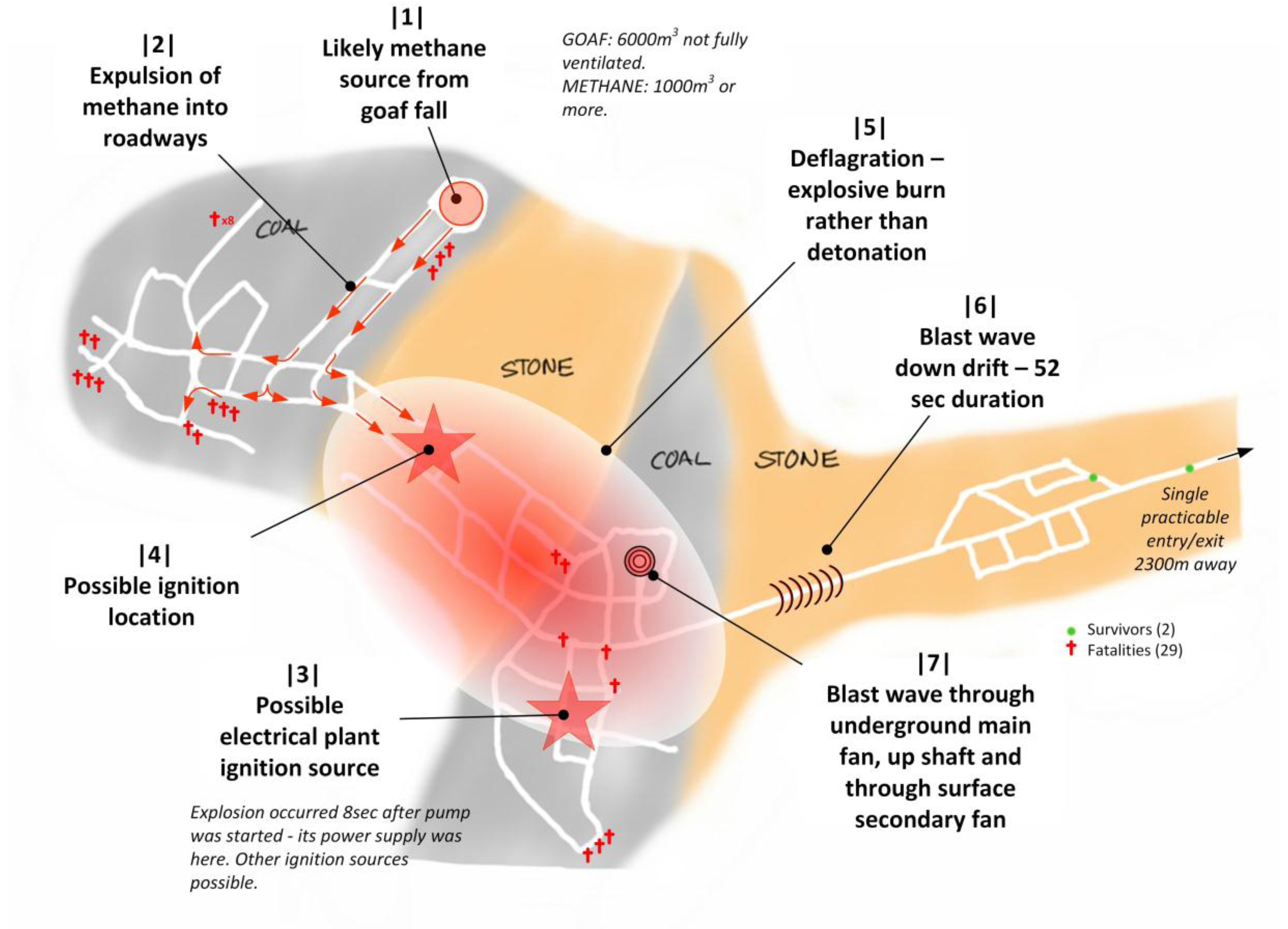
‘The Pike River underground coal mine lies high in the rugged Paparoa Range on the West Coast of the South Island. Access to the mine workings was through a single 2.3 km stone drift, or tunnel, which ran upwards through complex geological faulting to intersect the Brunner coal seam. On Friday 19 November 2010, at 3:45 p.m., the mine exploded. Twenty-nine men underground died immediately, or shortly afterwards, from the blast or from the toxic atmosphere. Two men in the stone drift, some distance from the mine workings, managed to escape. Over the next nine days the mine exploded three more times before it was sealed. There is currently no access to the mine.’.[1]
2. Background
3. Method
3.1. Purpose
3.2. Approach
4. Results
4.1. Physical Accident Sequence
4.1.1. Fuel Source
4.1.2. Ignition Source
‘The commission is satisfied that the immediate cause of the first explosion was the ignition of a substantial volume of methane gas. The commission’s report identifies a number of possible explanations for the source of that accumulation of methane, and the circumstances in which it was ignited.’.[1]
4.2. Contribution from Deficient Engineering Systems
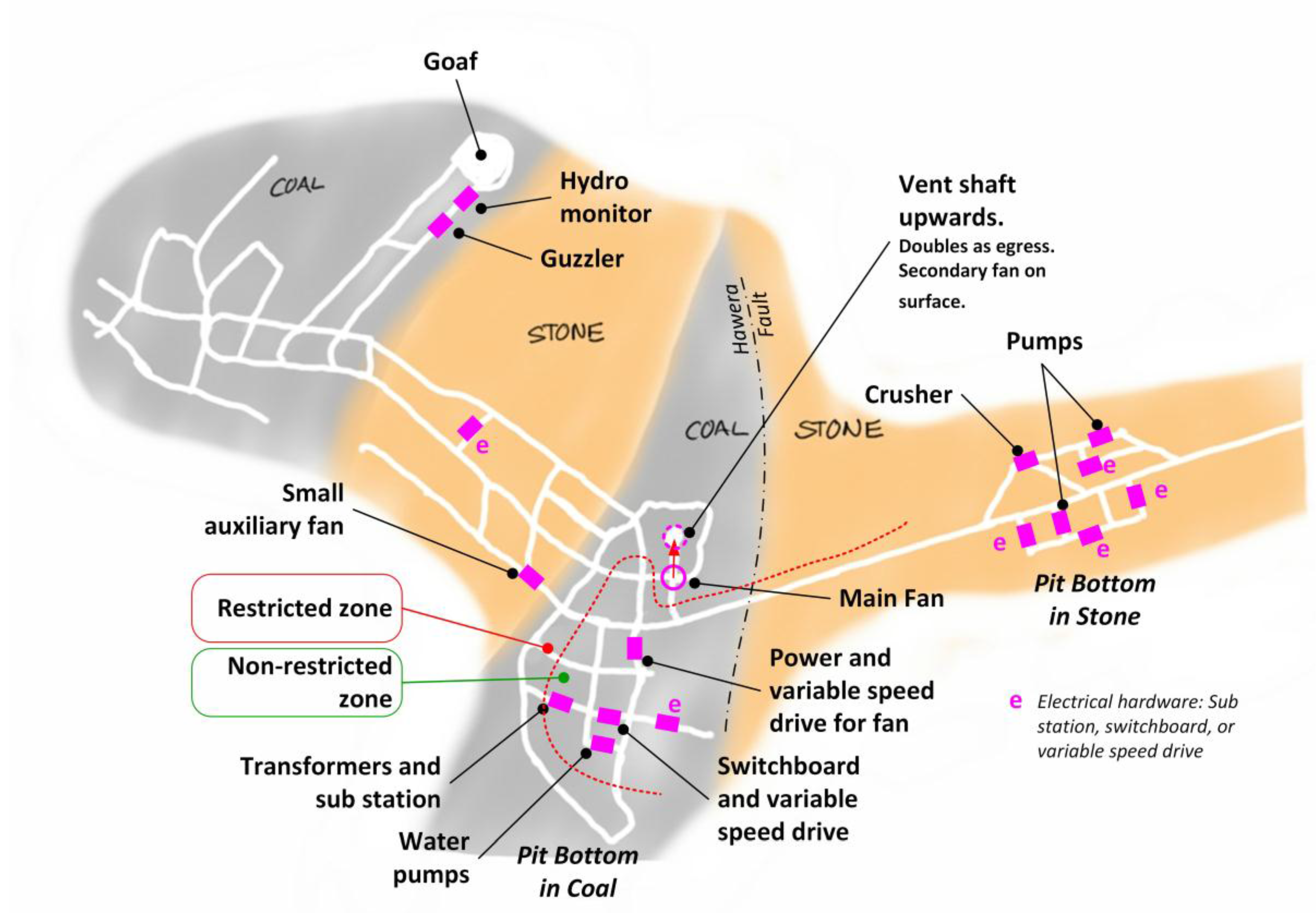
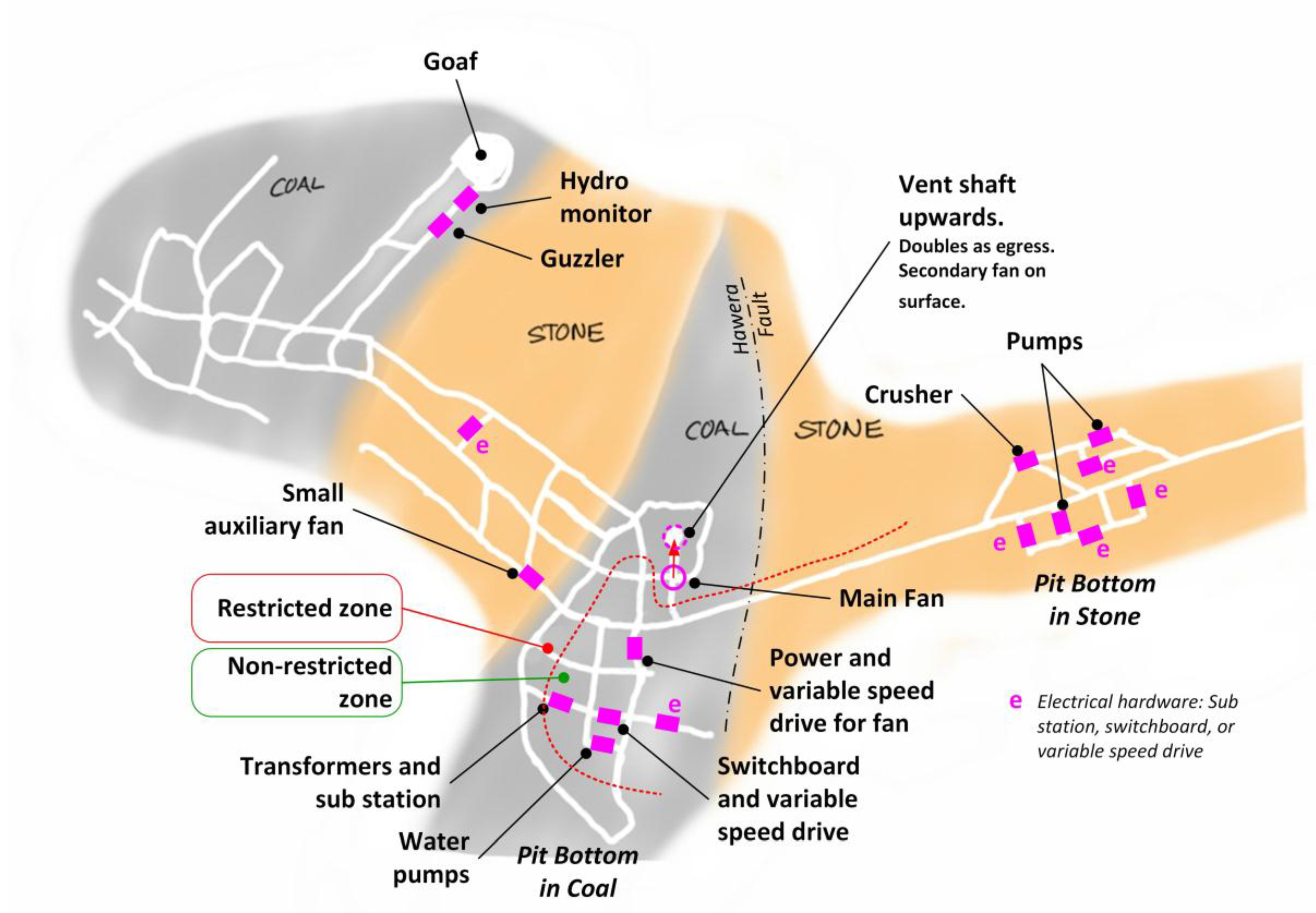
4.2.1. Unconventional Power Electrical System
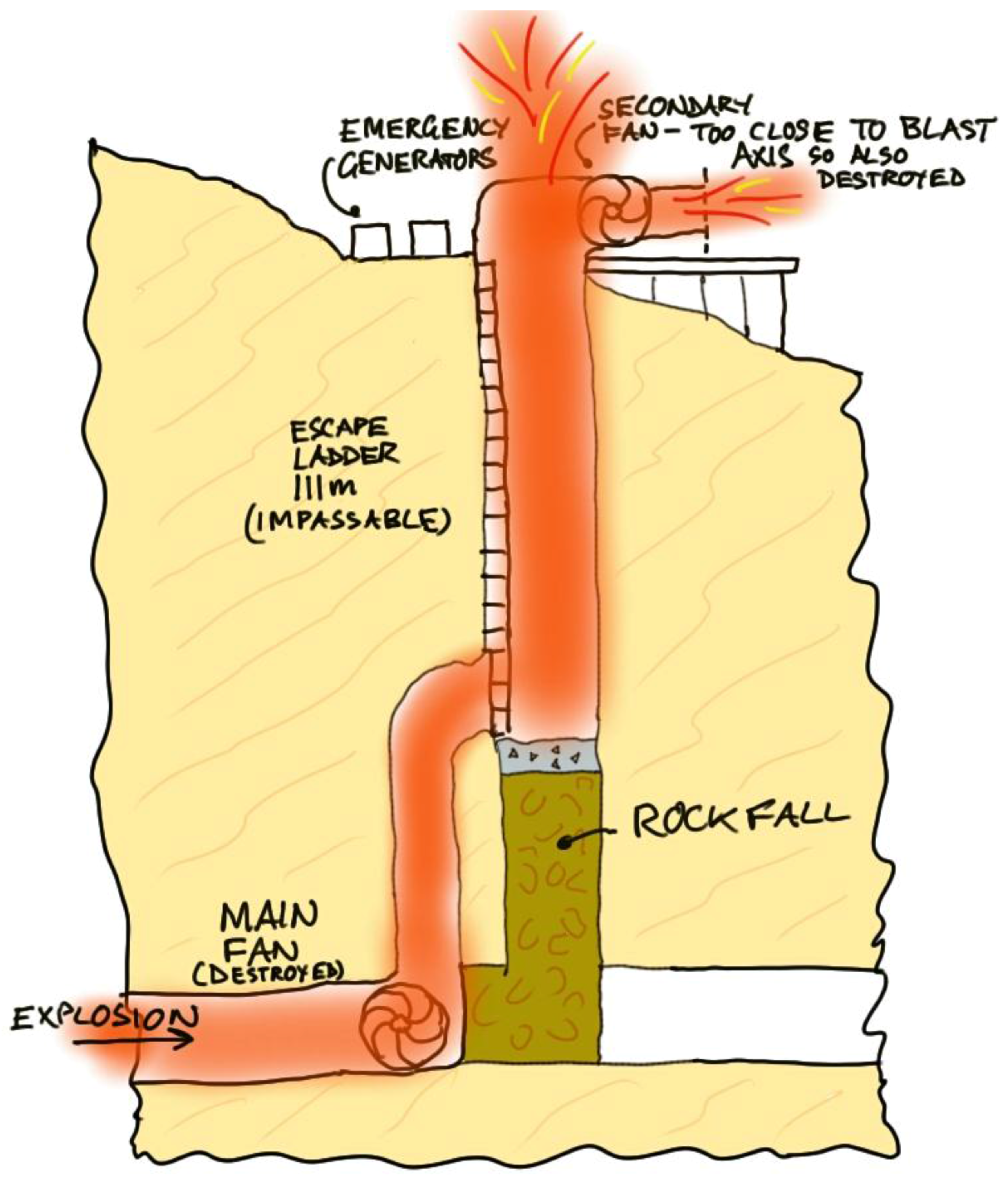
4.2.2. Unconventional Location of Main Ventilating Fan
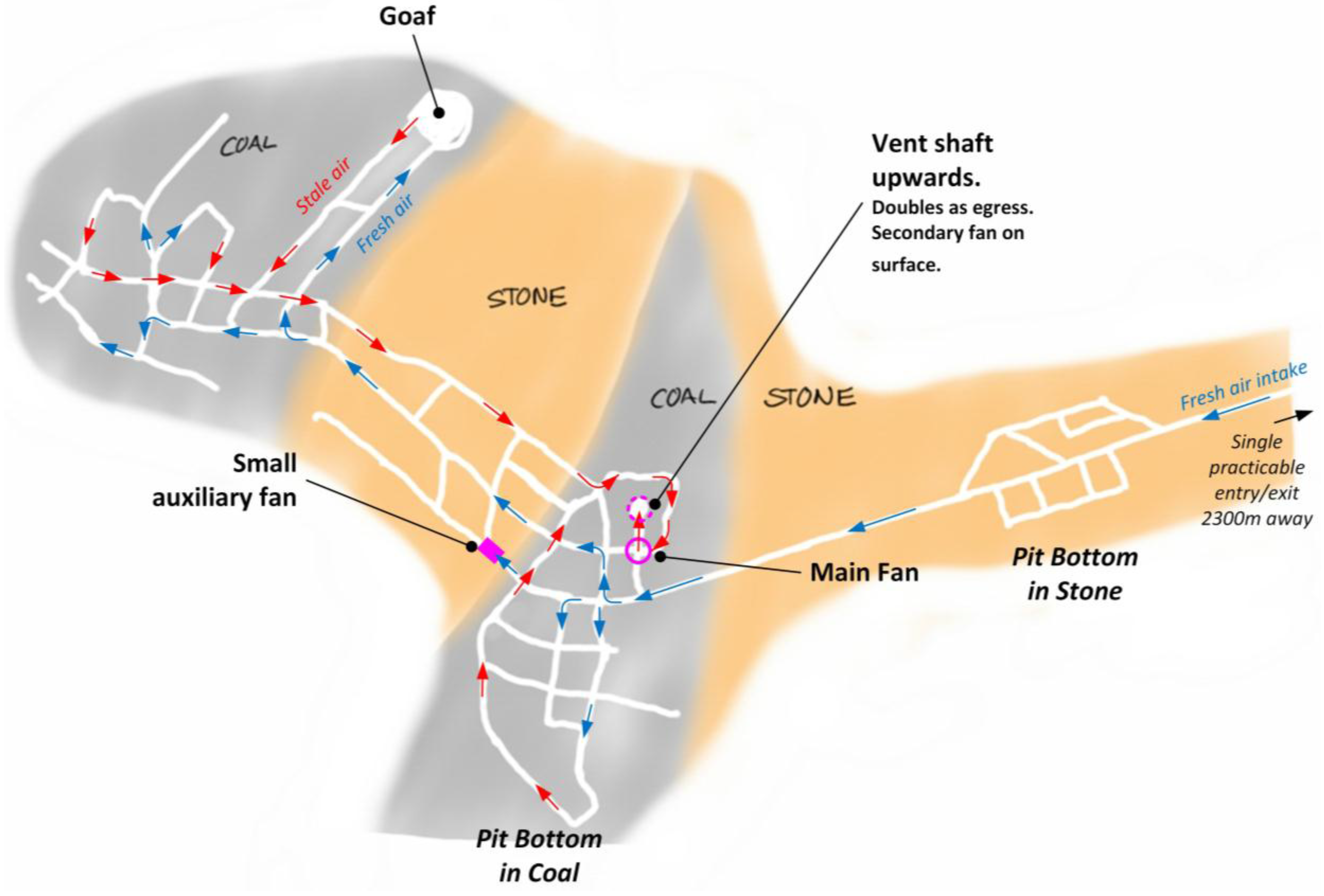
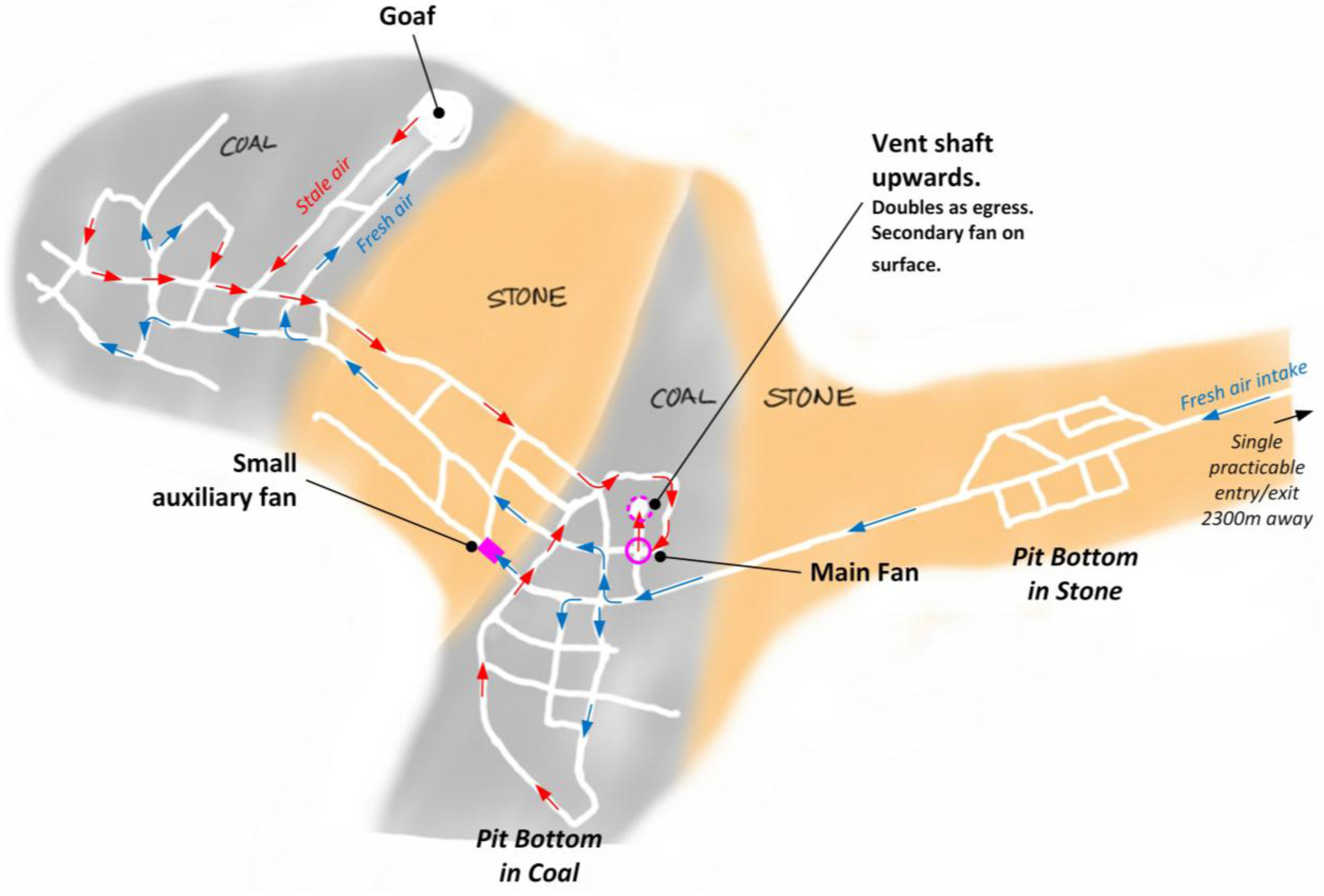
4.2.3. Ventilation System
‘Methane gas, which is found naturally in coal, is explosive when it comprises 5% to 15% in volume of air. In that range it is easily ignited. Methane control is therefore a crucial requirement in all underground coal mines. Control is maintained by effective ventilation, draining methane from the coal seam before mining if necessary, and by constant monitoring of the mine’s atmosphere.’.[1]
‘Pike’s ventilation and methane drainage systems could not cope with everything the company was trying to do: driving roadways through coal, drilling ahead into the coal seam and extracting coal by hydro mining, a method known to produce large quantities of methane.’.[1]
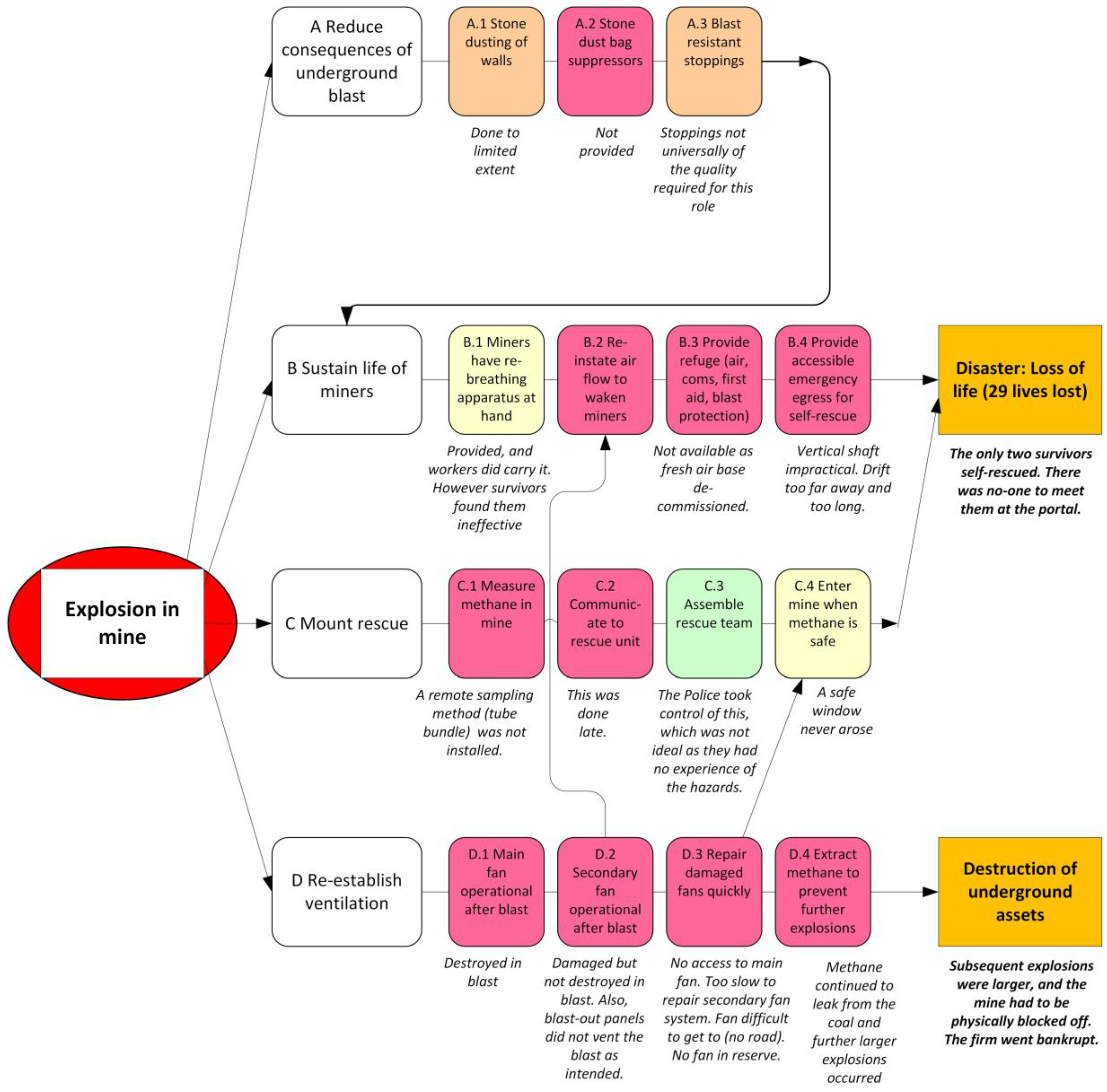
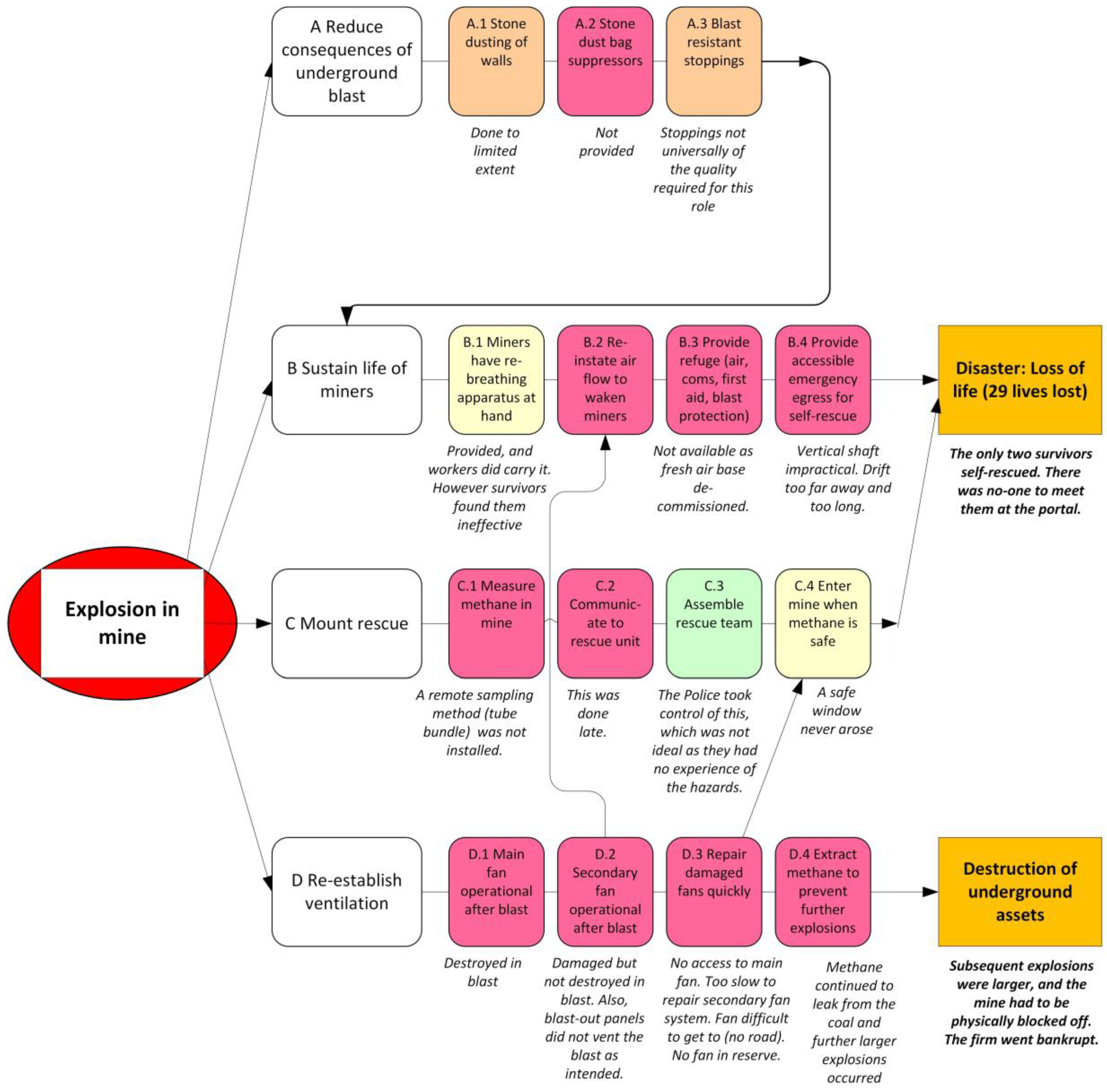
- It made the atmosphere inside the mine inhospitable to life, since there was no fresh air circulating in the mine. Consequently any miners who may have survived the first blast had no real chance of walking out themselves, not with the distances involved. Miners did have rebreathing apparatus with them, but the survivors reported that they did not work and so discarded them. However those survivors were in the drift (entrance tunnel) so closer to fresh air.
- It made it impossible to mount a rescue from outside, because the state of the mine was unknown. It is a basic principle that rescue teams should only be sent in once the methane levels are known to be safe. Pike had no way to reduce the methane levels. It also had no way of measuring the methane levels, because it had not installed the remote sampling instruments that would have made this possible. Such instruments have long been in existence [23].‘After the explosion a major search and rescue effort was launched. There was no predictable window of opportunity within which the Mines Rescue Service (MRS) could have safely entered the mine. Pike had no system for sampling the mine atmosphere after an explosion and without that information it was impossible to assess the risks of entry. The placement of the main fan underground and the damage caused to the back-up fan on the surface meant that the mine could not be reventilated quickly.’.[1]
- The ventilation failure caused repeated explosions, more violent than the first.‘For the first few days the families were given an over optimistic view of their men’s chances of survival, but this was inadvertent. When the second explosion occurred five days later any remaining hope disappeared.’.[1]
4.3. Management and Organisational Failings
‘The drive for coal production before the mine was ready created the circumstances within which the tragedy occurred.’.[1]
4.3.1. For the Best of Economic Reasons
‘A drive for production is a normal feature of coal mining but Pike was in a particularly difficult situation. It had only one mine, which was its sole source of revenue. The company was continuing to borrow to keep operations going.’.[1]
‘Development of the mine had been difficult from the start and the company’s original prediction that it would produce more than a million tonnes of coal a year by 2008 had proved illusory. The company had shipped only 42,000 tonnes of coal in total.’.[1]
‘The mine was new and the owner, Pike River Coal Ltd (Pike), had not completed the systems and infrastructure necessary to safely produce coal. Its health and safety systems were inadequate.‘.[1]
4.3.2. Deficient Risk Management
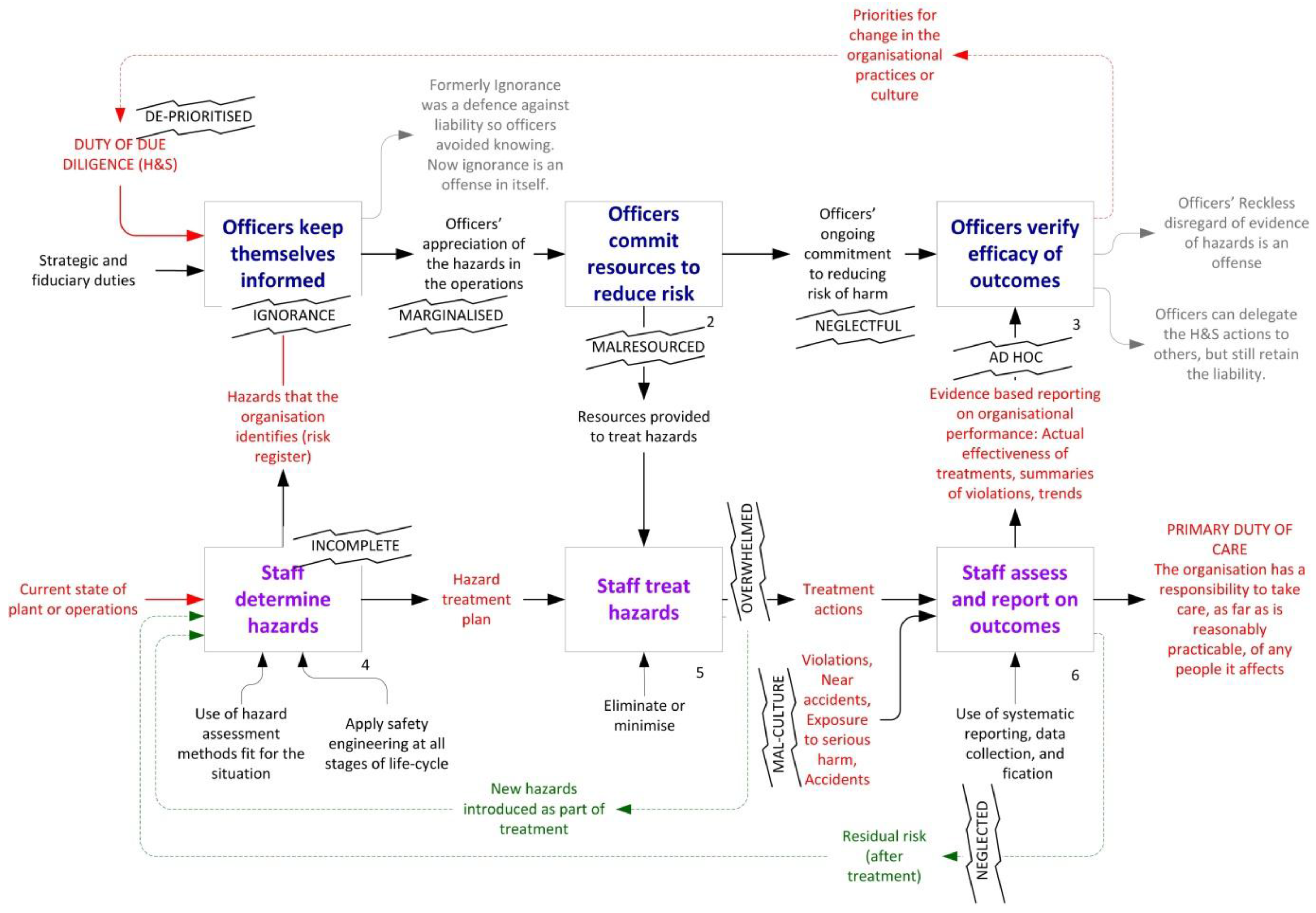
‘It is the commission’s view that even though the company was operating in a known high-hazard industry, the board of directors did not ensure that health and safety was being properly managed and the executive managers did not properly assess the health and safety risks that the workers were facing. In the drive towards coal production the directors and executive managers paid insufficient attention to health and safety and exposed the company’s workers to unacceptable risks.’.[1]
4.3.3. Organisational Culture
‘There were numerous warnings of a potential catastrophe at Pike River. One source of these was the reports made by the underground deputies and workers. For months they had reported incidents of excess methane (and many other health and safety problems). In the last 48 days before the explosion there were 21 reports of methane levels reaching explosive volumes, and 27 reports of lesser, but potentially dangerous, volumes. The reports of excess methane continued up to the very morning of the tragedy. The warnings were not heeded.’.[1]
4.3.4. Marginal Finances
‘Mining should have stopped until the risks could be properly managed.’.[1]
4.3.5. Lack of Recovery Mechanisms
‘The New Zealand Police led the emergency response and made the major decisions in Wellington. There had been no combined testing of an emergency response of this nature involving Pike, mining specialists, the MRS, the police and emergency services.’.[1]
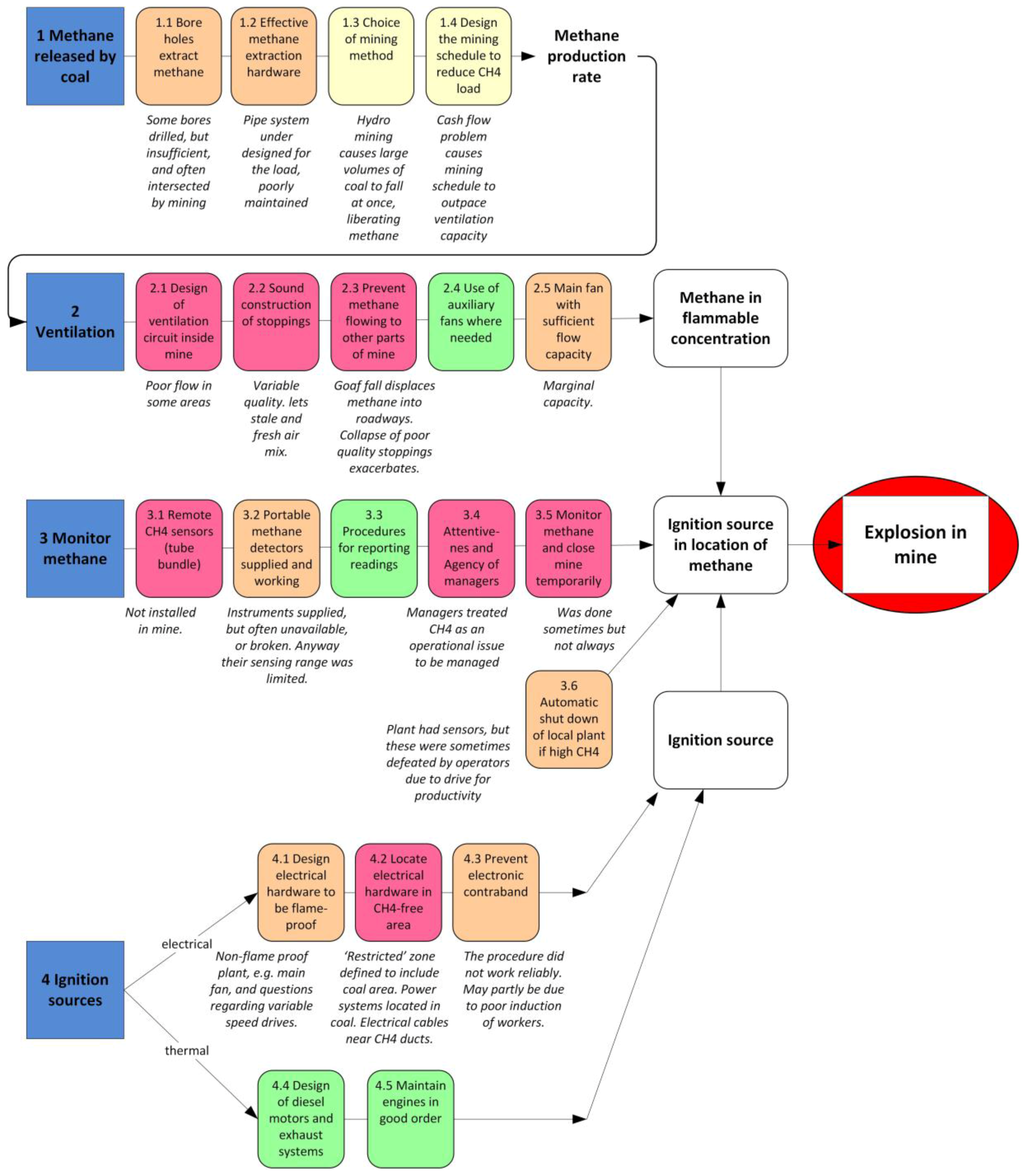
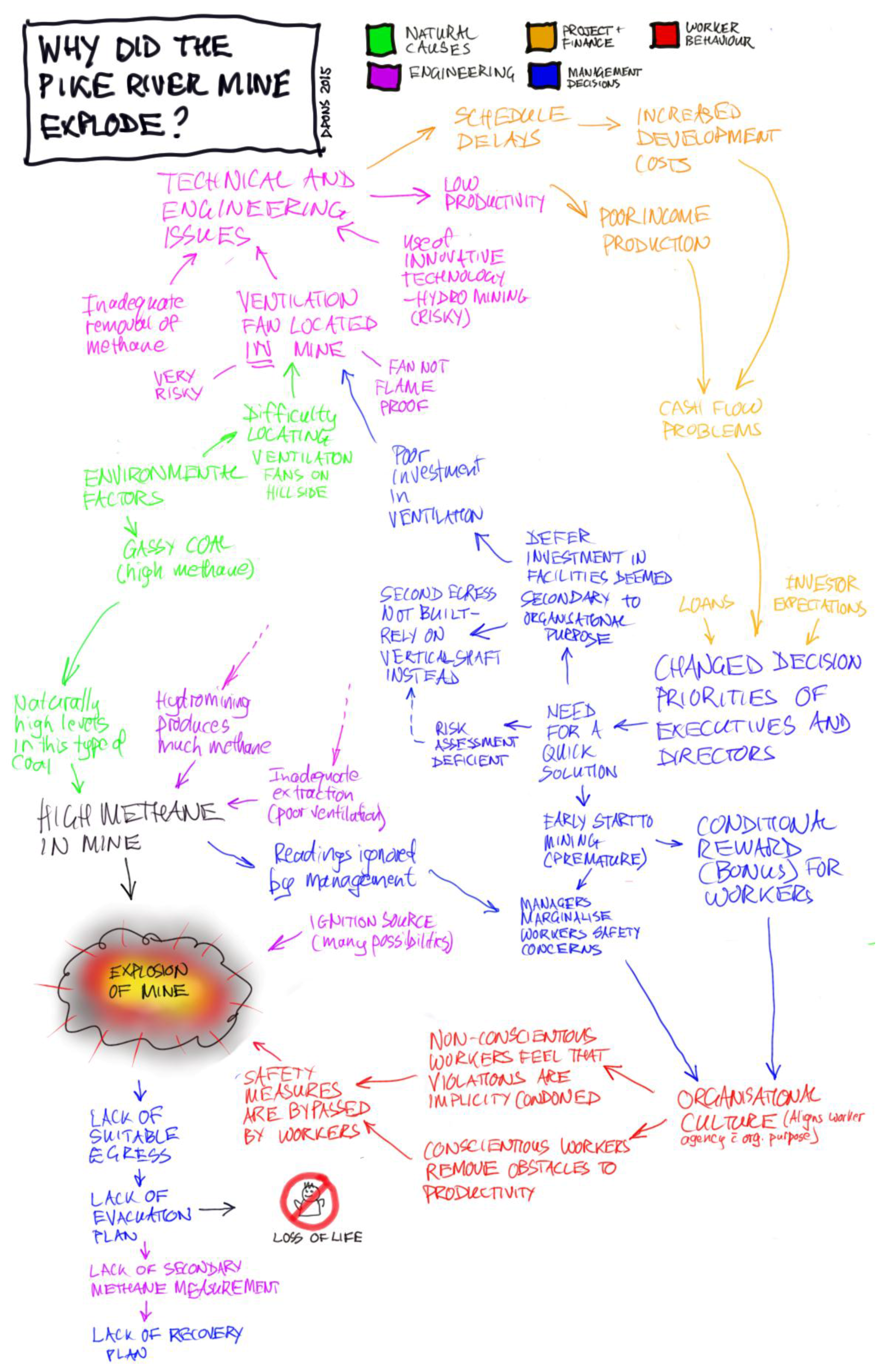
4.4. Systems Engineering Model of the Interacting Causation
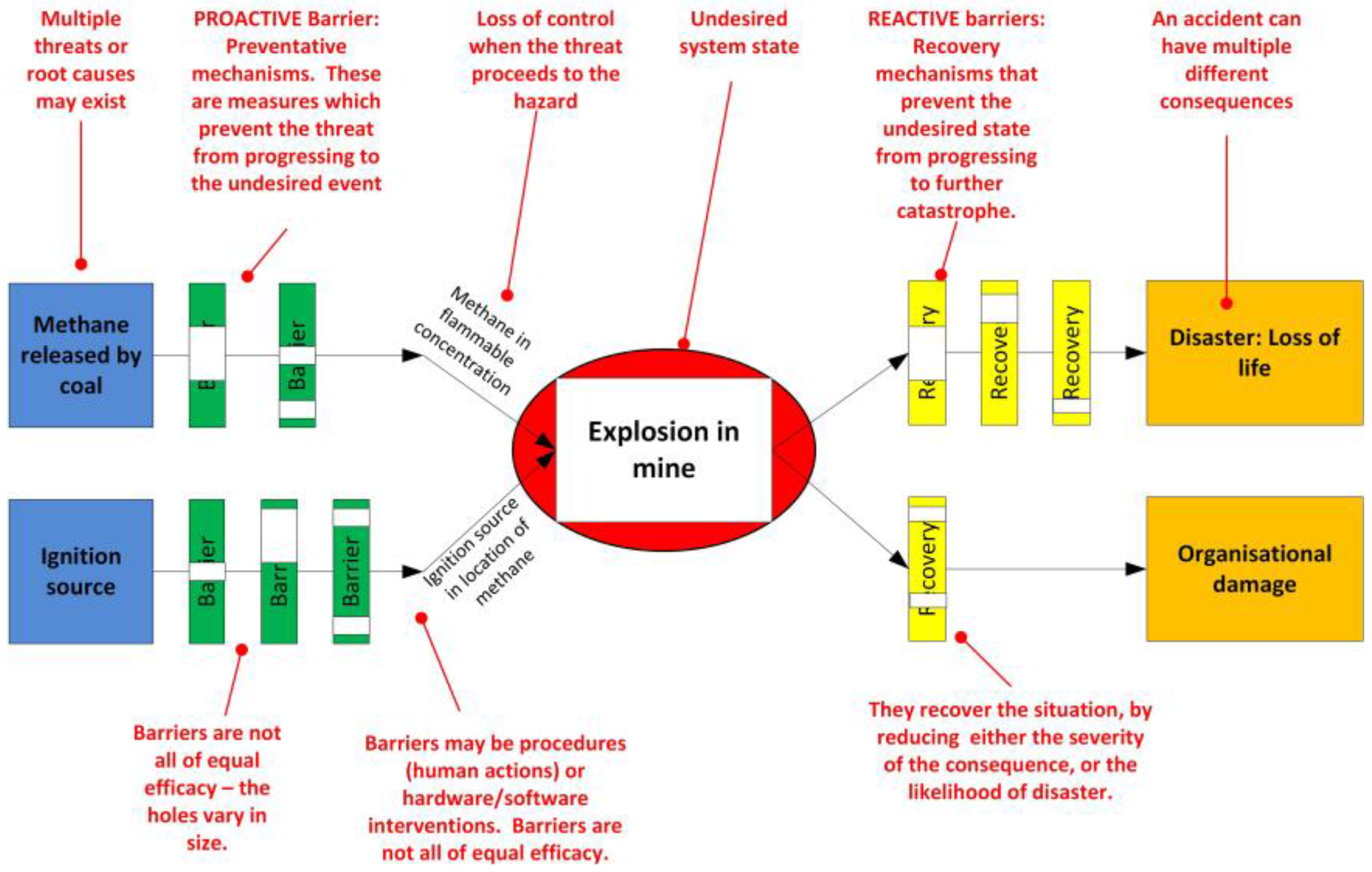
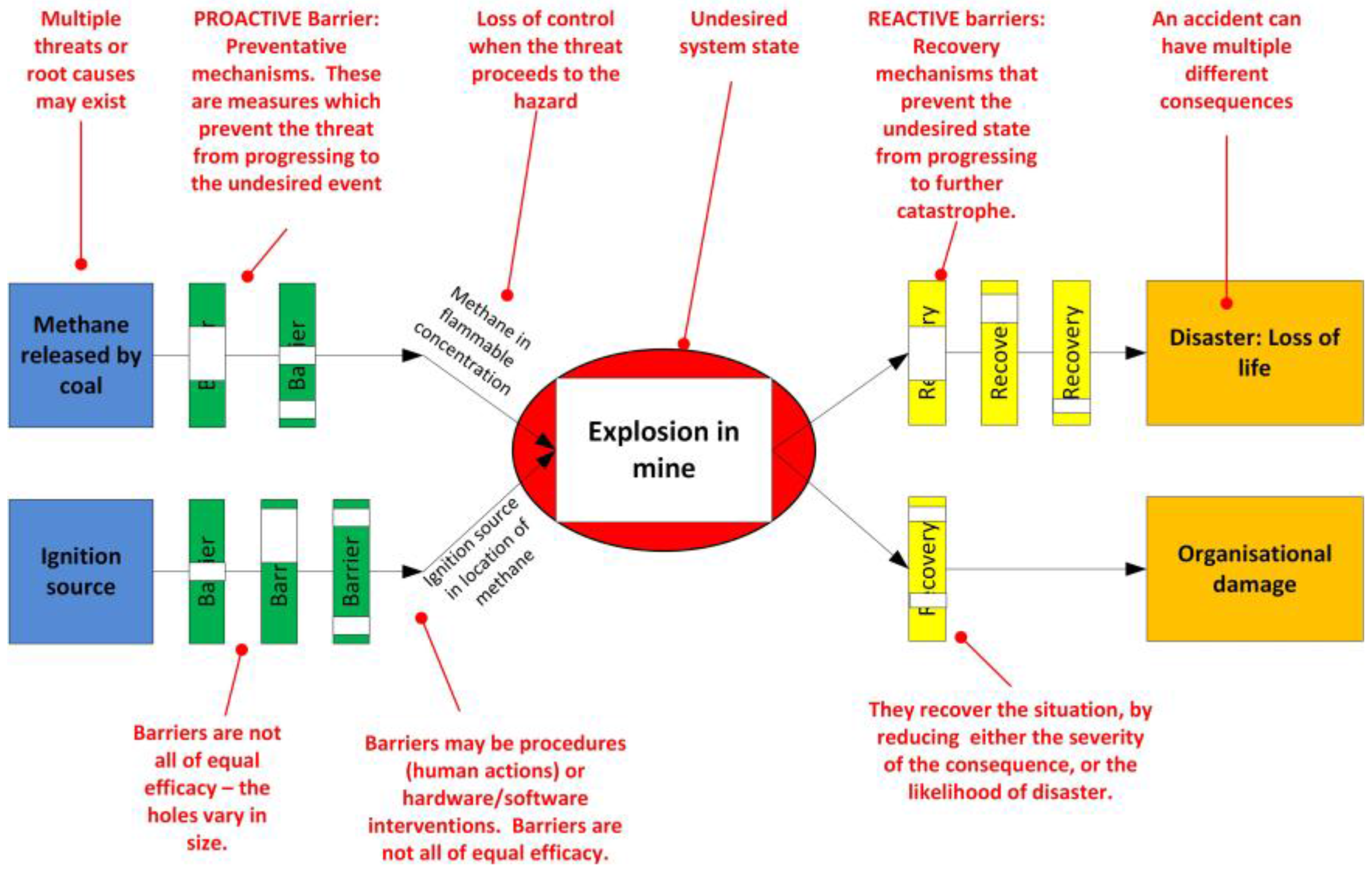
4.5. Bowtie Analysis
4.5.1. Background to the Method
4.5.2. Prevention Side
- Technology mechanisms, including:
- Good design practices that eliminate or minimise hazards in the hardware a-priori.
- Instrumentation to detect hazards and warn humans.
- Automatic control systems that suppress hazards.
- Personal protective equipment, which is the last line of defence.
- Human behavioural actions. These are the things that people do, most commonly represented as procedures. It is important to have a system: to be specific about these procedures and to monitor their efficacy. In the case of Pike it was reported:‘Its health and safety systems were inadequate.’.[1]
‘It is the commission’s view that even though the company was operating in a known high-hazard industry, the board of directors did not ensure that health and safety was being properly managed and the executive managers did not properly assess the health and safety risks that the workers were facing. In the drive towards coal production the directors and executive managers paid insufficient attention to health and safety and exposed the company’s workers to unacceptable risks. Mining should have stopped until the risks could be properly managed.‘.[1]
4.5.3. Recovery Side
- assess the reliability of each barrier and its limitations (size of the holes),
- identify secondary ‘escalation’ factors that cause a barrier to fail,
- implement deeper level barriers to prevent the ‘escalation’ factors from occurring, these are ‘escalation factor barriers’,
- identify what is required to maintain the barrier, and allocate responsibilities to people,
- test and evaluate the efficacy of the barriers.
5. Discussion
Implications: Legislative Consequences
‘The Department [of Labour] assumed that Pike was complying with the law, even though there was ample evidence to the contrary. The department should have prohibited Pike from operating the mine until its health and safety systems were adequate.’.[1]
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Royal Commission on the Pike River Coal Mine Tragedy. Department of Internal Affairs, New Zealand Government. Available online: http://pikeriver.royalcommission.govt.nz/Final-Report (accessed on 13 May 2016).
- International Organization for Standardization (ISO). ISO 31000:2009—Risk Management—Principles and Guidelines; ISO: Geneva, Switzerland, 2009. [Google Scholar]
- International Organization for Standardization (ISO). ISO 9001 Quality Management Systems—Requirements; ISO: Geneva, Switzerland, 2015. [Google Scholar]
- International Organization for Standardization (ISO). ISO 14001 Environmental Management Systems—Requirements with Guidance for Use; ISO: Geneva, Switzerland, 2015. [Google Scholar]
- BSI. BS OHSAS 18001 Occupational Health and Safety Management. Available online: http://www.bsigroup.com/en-GB/ohsas-18001-occupational-health-and-safety/ (accessed on 13 May 2016).
- Worksafe. Fire or Explosion in Underground Mines and Tunnels—Approved Code of Practice. Available online: http://www.business.govt.nz/worksafe/information-guidance/all-guidance-items/fire-or-explosion-in-underground-mines-and-tunnels (accessed on 13 May 2016).
- Reason, J. Human Error; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Moraru, R.I.; Babut, G.B.; Cioca, L.I. Study of methane flow in caved goafs ajacent to longwall faces in Valea Jiului coal basin. In Proceedings of the 13th International Multidisciplinary Scientific GeoConference of Modern Management of Mine Producing, Geology and Environmental Protection, Albena, Bulgaria, 16–22 June 2013.
- Man, C.-K.; Harris, M.L.; Weiss, E.S. Analysis of post-explosion residues for estimating flame travel during coal dust deflagrations. Sci. Technol. Energ. Mater. 2011, 72, 136–140. [Google Scholar]
- Du Plessis, J.J.L. Development and Evaluation of the Bagged Stone Dust Barrier. Ph.D. Thesis, Faculty of Engineering, University of the Witwatersrand, Johannesburg, South Africa, 2000. [Google Scholar]
- Amyotte, P.R.; Pegg, M.J. Explosion hazards in underground coal mines. Toxicol. Environ. Chem. 1993, 40, 189–199. [Google Scholar] [CrossRef]
- Davis, S.G.; Engel, D.; van Wingerden, K. Complex explosion development in mines: Case study—2010 Upper Big Branch mine explosion. Process Safety Progress 2015, 34, 286–303. [Google Scholar] [CrossRef]
- Du Plessis, J.J.L. Active explosion barrier performance against methane and coal dust explosions. Int. J. Coal Sci. Technol. 2015, 2, 261–268. [Google Scholar] [CrossRef]
- Mills, R.A.; Stevenson, J.W. Improved mine safety and productivity through a methane drainage system. In Proceedings of the 4th US Mine Ventilation Symposium, Berkeley, CA, USA, 5–7 June 1989.
- Trueman, R. Literature Review of the Ignition of Methane-Air Mixtures by Coal-Cutting Picks. J. S. Afr. Inst. Min. Metall. 1985, 85, 209–215. [Google Scholar]
- McMahon, W.; Britt, B.; Walker, B. Methane explosion modeling in the sago mine. In Proceedings of the 2009 SME Annual Meeting and CMA’s 111th National Western Mining Conference, Denver, CO, USA, 22–25 February 2009.
- Pang, L.; Wang, T.; Zhang, Q.; Ma, Q.; Cheng, L. Nonlinear distribution characteristics of flame regions from methane-air explosions in coal tunnels. Process Saf. Environ. Prot. 2014, 92, 193–198. [Google Scholar] [CrossRef]
- Zhang, Q.; Pang, L. Flame and temperature wave propagation characteristic of methane-air mixture in mine tunnels. Int. J. Numer. Methods Heat Fluid Flow 2013, 23, 885–898. [Google Scholar] [CrossRef]
- Cook, A.P. Methane safety research for continuous miners in South Africa. In Proceedings of the 1995 7th US Mine Ventilation Symposium, Lexington, KY, USA, 5–7 June 1995.
- Van Zyl, F.J. Proposed new method to determine the effectiveness of in-heading methane control. J. Mine Vent. Soc. S. Afr. 2000, 53, 32–39. [Google Scholar]
- Wang, A.; Mutmansky, J.M. Economic decision making for methane drainage systems for underground coal mines. Min. Eng. 1998, 50, 69–74. [Google Scholar]
- Wang, K.; Jiang, S.; Ma, X.; Wu, Z.; Zhang, W.; Shao, H. Study of the destruction of ventilation systems in coal mines due to gas explosions. Powder Technol. 2015, 286, 401–411. [Google Scholar] [CrossRef]
- Mironowicz, W.; Wasilewski, S. Hazard monitoring and control system of ventilation in a hard coal mine. In Proceedings of the 1998 International Symposium on Safety Science and Technology, Beijing, China, 1 September 1998.
- Pejic, L.M.; Torrent, J.G.; Querol, E.; Lebecki, K. A new simple methodology for evaluation of explosion risk in underground coal mines. J. Loss Prev. Process Ind. 2013, 26, 1524–1529. [Google Scholar] [CrossRef]
- Li, H.; Di, H.; Tian, S.; Li, J. The research on the impact of management levels charismatic leadership style on miners’ unsafe behavior. Open Biomed. Eng. J. 2015, 9, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Gupta, S.; Agarwal, M.; Singh, U. Categorization and standardization of accidental risk-criticality levels of human error to develop risk and safety management policy. Saf. Sci. 2016, 85, 88–98. [Google Scholar] [CrossRef]
- Laurence, D. Safety rules and regulations on mine sites—The problem and a solution. J. Saf. Res. 2005, 36, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, A. Rationale of risk taking. J. Mines Met. Fuels 2002, 50, 360–368. [Google Scholar]
- Cheng, J.; Luo, Y.; Zhou, F. Explosibility Safety Factor: An Approach to Assess Mine Gas Explosion Risk. Fire Technol. 2015, 51, 309–323. [Google Scholar] [CrossRef]
- Cheng, J.; Zhou, F. A systematic approach to assess mine atmospheric status. Fire Saf. J. 2013, 58, 142–150. [Google Scholar] [CrossRef]
- New Zealand Legislation. Health and Safety at Work Act 2015. New Zealand Government. Available online: http://www.legislation.govt.nz/act/public/2015/0070/latest/whole.html#DLM5976660 (accessed on 13 May 2016).


© 2016 by the author; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pons, D.J. Pike River Mine Disaster: Systems-Engineering and Organisational Contributions. Safety 2016, 2, 21. https://doi.org/10.3390/safety2040021
Pons DJ. Pike River Mine Disaster: Systems-Engineering and Organisational Contributions. Safety. 2016; 2(4):21. https://doi.org/10.3390/safety2040021
Chicago/Turabian StylePons, Dirk J. 2016. "Pike River Mine Disaster: Systems-Engineering and Organisational Contributions" Safety 2, no. 4: 21. https://doi.org/10.3390/safety2040021
APA StylePons, D. J. (2016). Pike River Mine Disaster: Systems-Engineering and Organisational Contributions. Safety, 2(4), 21. https://doi.org/10.3390/safety2040021