
Path Tracing vs. Volume Rendering Technique in Post-Surgical Assessment of Bone Flap in Oncologic Head and Neck Reconstructive Surgery: A Preliminary Study

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. CT Acquisition and Post Elaboration
2.3. Images Evaluations and Statistical Analysis
3. Results
3.1. Patients
3.2. Image Analysis—VR vs. PT
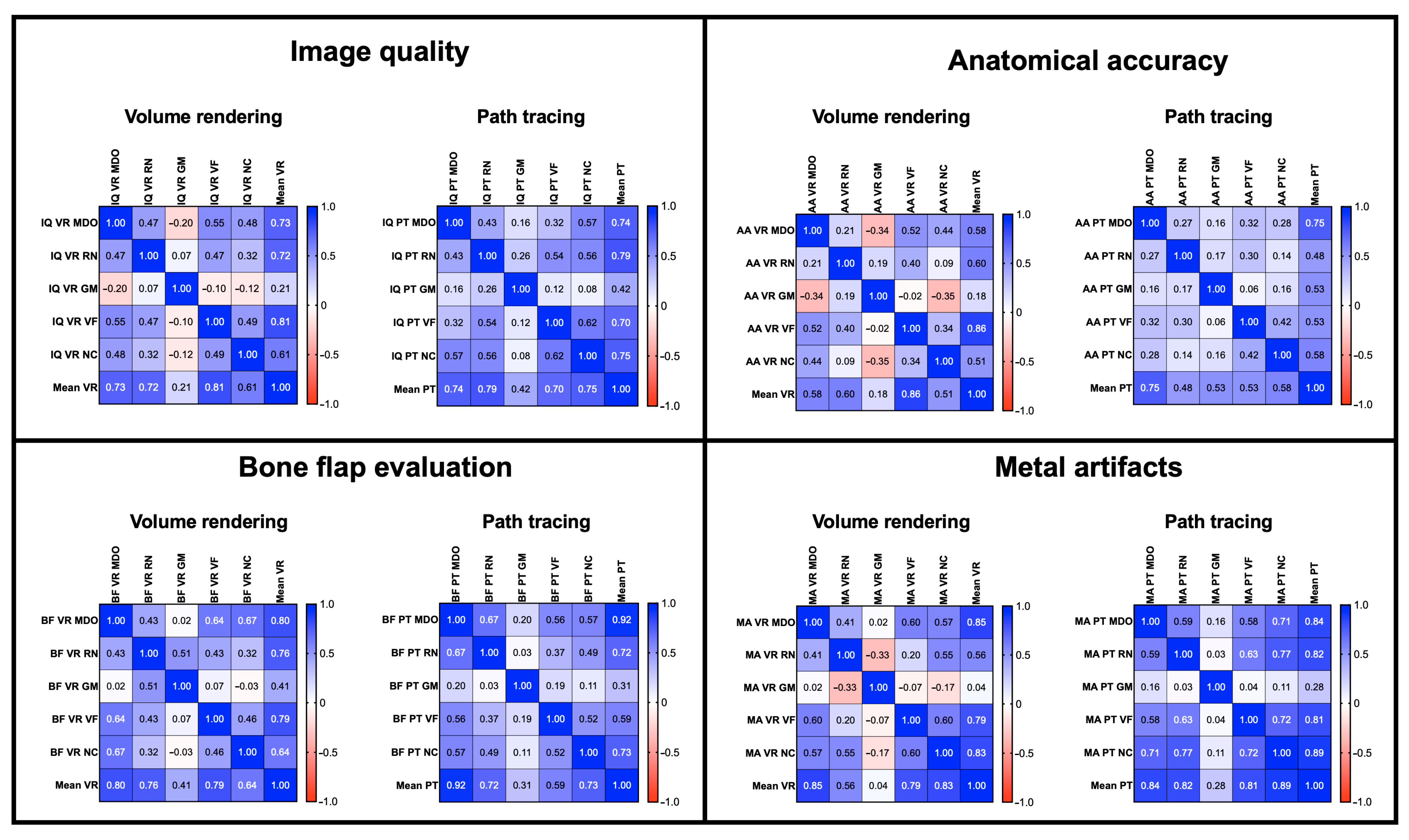
3.3. Image Analysis—Inter-Reader Agreement
4. Discussion
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flohr, T.; Schaller, S.; Stierstorfer, K.; Bruder, H.; Ohnesorge, B.; Schoepf, J. Multi-detector row CT systems and image-reconstruction techniques. Radiology 2005, 235, 756–773. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.; Kachelrieß, M.; Kalender, W.A. Technical advances in multi–slice spiral CT. Eur. J. Radiol. 2000, 36, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Prokop, M. General principles of MDCT. Eur. J. Radiol. 2003, 45, S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Luccichenti, G.; Cademartiri, F.; Pezzella, F.R.; Runza, G.; Belgrano, M.; Midiri, M.; Sabatini, U.; Bastianello, S.; Krestin, G.P. 3D reconstruction techniques made easy: Know-how and pictures. Eur. Radiol. 2005, 15, 2146–2156. [Google Scholar] [CrossRef]
- El-Seoud, S.A.; Mady, A.S.; Rashed, E. An Interactive Mixed Reality Ray Tracing Rendering Mobile Application of Medical Data in Minimally Invasive Surgeries. Int. J. Online Biomed. Eng. 2019, 15, 4–14. [Google Scholar] [CrossRef]
- Comaniciu, D.; Engel, K.; Georgescu, B.; Mansi, T. Shaping the Future through Innovations: From Medical Imaging to Precision Medicine 1. Cinematic Rendering: Photorealistic Visualisation of Medical Images. Med. Image Anal. 2016, 33, 19–26. [Google Scholar] [CrossRef]
- Debevec, P. Rendering synthetic objects into real scenes: Bridging traditional and image-based graphics with global illumination and high dynamic range photography. In Proceedings of the 25th Annual Conference on Computer Graphics and Interactive Techniques, Orlando, FL, USA, 19–24 July 1998. [Google Scholar]
- Dappa, E.; Higashigaito, K.; Fornaro, J.; Leschka, S.; Wildermuth, S.; Alkadhi, H. Cinematic rendering—An alternative to volume rendering for 3D computed tomography imaging. Insights Imaging 2016, 7, 849–856. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, Y.; Lu, Q.-H.; Zheng, K.-H.; Shi, L.-J.; Wang, Q.-J. CT two-dimensional reformation versus three-dimensional volume rendering with regard to surgical findings in the preoperative assessment of the ossicular chain in chronic suppurative otitis media. Eur. J. Radiol. 2013, 82, 1519–1524. [Google Scholar] [CrossRef]
- Vannier, M.W.; Marsh, J.L.; Warren, J.O. Three dimensional CT reconstruction images for craniofacial surgical planning and evaluation. Radiology 1984, 150, 179–184. [Google Scholar] [CrossRef]
- Song, S.W.; Jun, B.C.; Chae, S.R.; Kim, B.G. Clinical Utility of Three-Dimensional Facial Computed Tomography in the Treatment of Nasal Bone Fractures: A New Modality Involving an Air-Bone View with a Volume Rendering Technique. Indian J. Otolaryngol. Head Neck Surg. 2013, 65, 210–215. [Google Scholar] [CrossRef]
- Schmidle, G.; Rieger, M.; Klauser, A.; Thauerer, M.; Hoermann, R.; Gabl, M. Intraosseous rotation of the scaphoid: Assessment by using a 3D CT model—An anatomic study. Eur. Radiol. 2014, 24, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Falchi, M.; Rollandi, G.A. CT of pelvic fractures. Eur. J. Radiol. 2004, 50, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Lawler, L.P.; Fishman, E.K. Multi–Detector Row CT of Thoracic Disease with Emphasis on 3D Volume Rendering and CT Angiography. RadioGraphics 2001, 21, 1257–1273. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Chu, L.C.; Fishman, E.K. Cinematic rendering of small bowel pathology: Preliminary observations from this novel 3D CT visualisation method. Abdom. Radiol. 2018, 43, 2928–2937. [Google Scholar] [CrossRef]
- Rowe, S.P.; Chu, L.C.; Fishman, E.K. Evaluation of Stomach Neoplasms with 3-Dimensional Computed Tomography: Focus on the Potential Role of Cinematic Rendering. J. Comput. Assist. Tomogr. 2018, 42, 661–666. [Google Scholar] [CrossRef]
- Chu, L.C.; Rowe, S.P.; Fishman, E.K. Cinematic rendering of focal liver masses. Diagn. Interv. Imaging 2019, 100, 467–476. [Google Scholar] [CrossRef]
- Rowe, S.P.; Chu, L.C.; Fishman, E.K. Computed Tomography Cinematic Rendering in the Evaluation of Colonic Pathology. J. Comput. Assist. Tomogr. 2019, 43, 475–484. [Google Scholar] [CrossRef]
- Rowe, S.P.; Chu, L.C.; Fishman, E.K. Initial experience with 3D CT cinematic rendering of acute pancreatitis and associated complications. Abdom. Radiol. 2020, 45, 1290–1298. [Google Scholar] [CrossRef]
- Rowe, S.P.; Chu, L.C.; Meyer, A.R.; Gorin, M.A.; Fishman, E.K. The application of cinematic rendering to CT evaluation of upper tract urothelial tumors: Principles and practice. Abdom. Radiol. 2019, 44, 3886–3892. [Google Scholar] [CrossRef]
- Rowe, S.P.; Meyer, A.R.; Gorin, M.A.; Chu, L.C.; Fishman, E.K. Evaluation of the urinary bladder using three-dimensional CT cinematic rendering. Diagn. Interv. Imaging 2020, 101, 771–781. [Google Scholar] [CrossRef]
- Jin, Y.-R.; Yang, X.-L.; Li, Q.-Q.; Yan, Z.-L.; Yang, H.-Y.; Liao, C. CT of ovarian cancer: 3D cinematic rendering for preoperative evaluation. J. Ovarian Res. 2018, 11, 86. [Google Scholar] [CrossRef] [PubMed]
- Arias, E.A.; Sandoval, J.P.; Farjat-Pasos, J.I.; Rodríguez-Zanella, H.; de la Mora-Cervantes, R. Novel Cinematic Rendering Use for Ventricular Septal Ruptures. JACC Cardiovasc. Interv. 2021, 14, 1151–1153. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.L.; Rowe, S.P.; Fishman, E.K. Cinematic rendering of CT angiography for visualization of complex vascular anatomy after hybrid endovascular aortic aneurysm repair. Emerg. Radiol. 2021, 28, 839–843. [Google Scholar] [CrossRef] [PubMed]
- Colli, A.; Tua, L.; Punzo, B.; Baldi, D.; Cademartiri, F.; Gerosa, G. Cinematic Rendering: An Alternative to Classical Volume Rendering for Acute Aortic Dissection. Ann. Thorac. Surg. 2019, 108, e121. [Google Scholar] [CrossRef]
- Dreizin, D.; LeBedis, C.A.; Nascone, J.W. Imaging Acetabular Fractures. Radiol. Clin. North Am. 2019, 57, 823–841. [Google Scholar] [CrossRef]
- Binder, J.S.; Scholz, M.; Ellmann, S.; Uder, M.; Grützmann, R.; Weber, G.F.; Krautz, C. Cinematic Rendering in Anatomy: A Crossover Study Comparing a Novel 3D Reconstruction Technique to Conventional Computed Tomography. Anat. Sci. Educ. 2020, 14, 22–31. [Google Scholar] [CrossRef]
- Elshafei, M.; Binder, J.; Baecker, J.; Brunner, M.; Uder, M.; Weber, G.F.; Grützmann, R.; Krautz, C. Comparison of Cinematic Rendering and Computed Tomography for Speed and Comprehension of Surgical Anatomy. JAMA Surg. 2019, 154, 738–744. [Google Scholar] [CrossRef]
- Li, K.; Yan, R.; Ma, H.; Zhang, D.-F.; Ding, Y.; Li, Z. Value of the Cinematic Rendering From Volumetric Computed Tomography Data in Evaluating the Relationship Between Deep Soft Tissue Sarcomas of the Extremities and Adjacent Major Vessels. J. Comput. Assist. Tomogr. 2019, 43, 386–391. [Google Scholar] [CrossRef]
- Wollschlaeger, L.; Boos, J.; Jungbluth, P.; Grassmann, J.-P.; Schleich, C.; Latz, D.; Kroepil, P.; Antoch, G.; Windolf, J.; Schaarschmidt, B. Is CT-based cinematic rendering superior to volume rendering technique in the preoperative evaluation of multifragmentary intraarticular lower extremity fractures? Eur. J. Radiol. 2020, 126, 108911. [Google Scholar] [CrossRef]
- Steffen, T.; Winklhofer, S.; Starz, F.; Wiedemeier, D.; Ahmadli, U.; Stadlinger, B. Three-dimensional perception of cinematic rendering versus conventional volume rendering using CT and CBCT data of the facial skeleton. Ann. Anat.-Anat. Anz. 2022, 241, 151905. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Likert’s Scale Scores | |||||
|---|---|---|---|---|---|
| Parameters | 1 | 2 | 3 | 4 | 5 |
| Image Quality | Non-diagnostic | Poor quality | Good quality | Very good quality | Excellent quality |
| Anatomical Accuracy | Non-diagnostic | Poorly demarcated bone margins | Good demarcation of bone margins | Very good demarcation of bone margins | Excellent demarcation of bone margins |
| Bone Flap Evaluation | Non-diagnostic | Poor quality | Good quality | Very good quality | Excellent quality |
| Metal Artifact | Severe | Strong | Moderate | Mild | No artefacts |
| Image Quality | Anatomical Accuracy | Bone Flap Evaluation | Metal Artifacts | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VR | PT | p | VR | PT | p | VR | PT | p | VR | PT | p | ||
| Reader | MDO | 3 | 4 | <0.05 | 3 | 4 | <0.05 | 2 | 4 | <0.05 | 3 | 4 | <0.05 |
| RN | 3 | 4 | <0.05 | 3 | 4 | <0.05 | 3 | 4 | <0.05 | 3 | 3 | 0.65 | |
| VF | 4 | 4 | <0.05 | 4 | 5 | <0.05 | 4 | 5 | <0.05 | 3 | 4 | <0.05 | |
| GM | 3 | 4 | <0.05 | 3 | 4 | <0.05 | 3 | 4 | <0.05 | 3 | 4 | <0.05 | |
| NC | 3 | 4 | < 0.05 | 4 | 4 | <0.05 | 3 | 4 | < 0.05 | 3 | 4 | <0.05 | |
| Image Quality | Anatomical Accuracy | Bone Flap Evaluation | Metal Artefacts | |||||
|---|---|---|---|---|---|---|---|---|
| VR | PT | VR | PT | VR | PT | VR | PT | |
| Median | 3 | 4 | 3 | 4 | 3 | 4 | 3 | 4 |
| Mean±SD | 3.19 ± 0.47 | 4.01 ± 0.56 | 3.24 ± 0.37 | 4.14 ± 0.45 | 3.19 ± 0.55 | 4.16 ± 0.56 | 3.15 ± 0.58 | 3.79 ± 0.64 |
| p | <0.05 | <0.05 | <0.05 | <0.05 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardobi, N.; Nocini, R.; Molteni, G.; Favero, V.; Fior, A.; Marchioni, D.; Montemezzi, S.; D’Onofrio, M. Path Tracing vs. Volume Rendering Technique in Post-Surgical Assessment of Bone Flap in Oncologic Head and Neck Reconstructive Surgery: A Preliminary Study. J. Imaging 2023, 9, 24. https://doi.org/10.3390/jimaging9020024
Cardobi N, Nocini R, Molteni G, Favero V, Fior A, Marchioni D, Montemezzi S, D’Onofrio M. Path Tracing vs. Volume Rendering Technique in Post-Surgical Assessment of Bone Flap in Oncologic Head and Neck Reconstructive Surgery: A Preliminary Study. Journal of Imaging. 2023; 9(2):24. https://doi.org/10.3390/jimaging9020024
Chicago/Turabian StyleCardobi, Nicolò, Riccardo Nocini, Gabriele Molteni, Vittorio Favero, Andrea Fior, Daniele Marchioni, Stefania Montemezzi, and Mirko D’Onofrio. 2023. "Path Tracing vs. Volume Rendering Technique in Post-Surgical Assessment of Bone Flap in Oncologic Head and Neck Reconstructive Surgery: A Preliminary Study" Journal of Imaging 9, no. 2: 24. https://doi.org/10.3390/jimaging9020024
APA StyleCardobi, N., Nocini, R., Molteni, G., Favero, V., Fior, A., Marchioni, D., Montemezzi, S., & D’Onofrio, M. (2023). Path Tracing vs. Volume Rendering Technique in Post-Surgical Assessment of Bone Flap in Oncologic Head and Neck Reconstructive Surgery: A Preliminary Study. Journal of Imaging, 9(2), 24. https://doi.org/10.3390/jimaging9020024