

Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom Apparatus

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Custom Thoracic Phantom Mold Construction
2.2. Synthetic Phantom Preparations
2.3. Synthetic Phantom Apparatus Setup and Ultrasound Image Collection
2.4. Euthanized Porcine Pneumothorax Model
2.5. Image Processing and Augmentation
2.6. Algorithm Training and Testing
3. Results
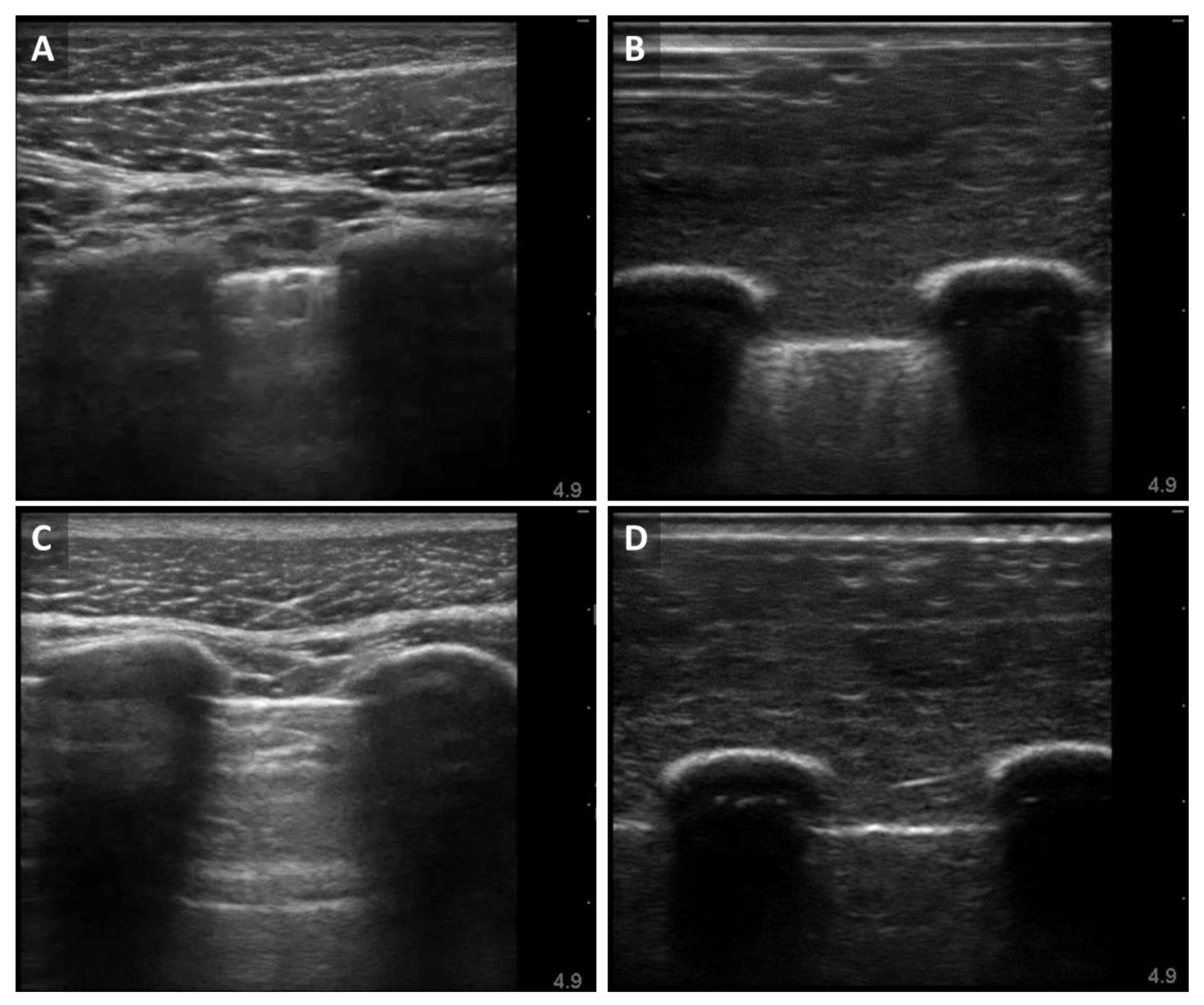
3.1. Ultrasound B-Mode Image Results for the Synthetic Phantom Apparatus
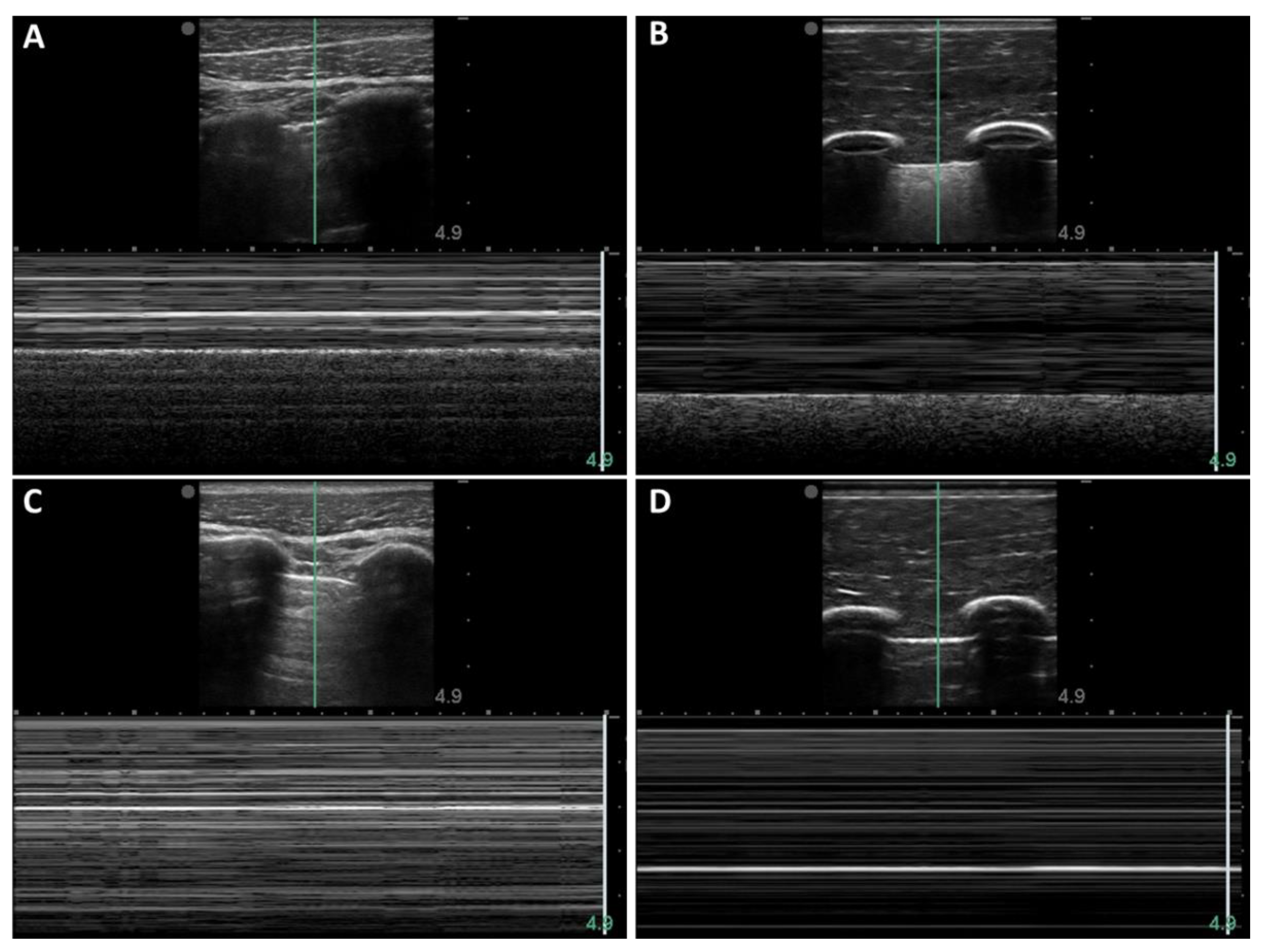
3.2. M-Mode Comparison of Porcine and Synthetic Platforms
3.3. Image Classifier Algorithm Training
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
DoD Disclaimer
References
- American College of Emergency Physicians. Council Resolution on Ultrasound. ACEP News 1990, 11. [Google Scholar]
- Society for Academic Emergency Medicine. Ultrasound Position Statement. SAEM Newsletter 1991. summer. [Google Scholar]
- Whitson, M.R.; Mayo, P.H. Ultrasonography in the Emergency Department. Crit. Care 2016, 20, 227. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians. ACEP Emergency Ultrasound Guidelines–2001. Ann. Emerg. Med. 2001, 38, 470–481. [Google Scholar] [CrossRef]
- American College of Emergency Physicians. Emergency Ultrasound Guidelines. Ann. Emerg. Med. 2009, 53, 550–570. [Google Scholar] [CrossRef] [PubMed]
- Alrajhi, K.; Woo, M.Y.; Vaillancourt, C. Test Characteristics of Ultrasonography for the Detection of Pneumothorax: A Systematic Review and Meta-Analysis. Chest 2012, 141, 703–708. [Google Scholar] [CrossRef]
- Ebrahimi, A.; Yousefifard, M.; Mohammad Kazemi, H.; Rasouli, H.R.; Asady, H.; Moghadas Jafari, A.; Hosseini, M. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Meta-Analysis. Tanaffos 2014, 13, 29–40. [Google Scholar]
- Avila, J.; Smith, B.; Mead, T.; Jurma, D.; Dawson, M.; Mallin, M.; Dugan, A. Does the Addition of M-Mode to B-Mode Ultrasound Increase the Accuracy of Identification of Lung Sliding in Traumatic Pneumothoraces? J. Ultrasound Med. 2018, 37, 2681–2687. [Google Scholar] [CrossRef]
- Zhang, M.; Liu, Z.-H.; Yang, J.-X.; Gan, J.-X.; Xu, S.-W.; You, X.-D.; Jiang, G.-Y. Rapid Detection of Pneumothorax by Ultrasonography in Patients with Multiple Trauma. Crit. Care 2006, 10, R112. [Google Scholar] [CrossRef]
- Kido, S.; Hirano, Y.; Mabu, S. Deep Learning for Pulmonary Image Analysis: Classification, Detection, and Segmentation. In Deep Learning in Medical Image Analysis; Lee, G., Fujita, H., Eds.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2020; Volume 1213, pp. 47–58. ISBN 978-3-030-33127-6. [Google Scholar]
- Park, S.; Lee, S.M.; Kim, N.; Choe, J.; Cho, Y.; Do, K.-H.; Seo, J.B. Application of Deep Learning–Based Computer-Aided Detection System: Detecting Pneumothorax on Chest Radiograph after Biopsy. Eur. Radiol. 2019, 29, 5341–5348. [Google Scholar] [CrossRef]
- Alakwaa, W.; Nassef, M.; Badr, A. Lung Cancer Detection and Classification with 3D Convolutional Neural Network (3D-CNN). Int. J. Adv. Comput. Sci. Appl. 2017, 8, 409–417. [Google Scholar] [CrossRef]
- Han, S.; Kang, H.-K.; Jeong, J.-Y.; Park, M.-H.; Kim, W.; Bang, W.-C.; Seong, Y.-K. A Deep Learning Framework for Supporting the Classification of Breast Lesions in Ultrasound Images. Phys. Med. Biol. 2017, 62, 7714–7728. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.A.; Washington, K.N.; Tran, T.D.; Reiter, A.; Lediju Bell, M.A. Deep Learning to Obtain Simultaneous Image and Segmentation Outputs From a Single Input of Raw Ultrasound Channel Data. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 2493–2509. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Escobar, J.; Ordóñez-Guillén, N.E.; Villarreal-Reyes, S.; Galaviz-Mosqueda, A.; Kober, V.; Rivera-Rodriguez, R.; Rizk, J.E.L. Deep-Learning Based Detection of COVID-19 Using Lung Ultrasound Imagery. PLoS ONE 2021, 16, e0255886. [Google Scholar] [CrossRef]
- Baumgartner, C.F.; Kamnitsas, K.; Matthew, J.; Smith, S.; Kainz, B.; Rueckert, D. Real-Time Standard Scan Plane Detection and Localisation in Fetal Ultrasound Using Fully Convolutional Neural Networks. In Medical Image Computing and Computer-Assisted Intervention–MICCAI 2016; Ourselin, S., Joskowicz, L., Sabuncu, M.R., Unal, G., Wells, W., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 203–211. [Google Scholar]
- Liu, S.; Wang, Y.; Yang, X.; Lei, B.; Liu, L.; Li, S.X.; Ni, D.; Wang, T. Deep Learning in Medical Ultrasound Analysis: A Review. Engineering 2019, 5, 261–275. [Google Scholar] [CrossRef]
- Xu, D.; Abbas, S.; Chan, V.W.S. Ultrasound Phantom for Hands-on Practice. Reg. Anesth. Pain Med. 2005, 30, 593–594. [Google Scholar] [CrossRef]
- Lo, M.D.; Ackley, S.H.; Solari, P. Homemade Ultrasound Phantom for Teaching Identification of Superficial Soft Tissue Abscess. Emerg. Med. J. 2012, 29, 738–741. [Google Scholar] [CrossRef]
- Mp, M.; Me, M. Preparation of a Homemade Ultrasound Biopsy Phantom. J. Clin. Ultrasound: JCU 1989, 17, 456–458. [Google Scholar] [CrossRef]
- Selame, L.A.; Risler, Z.; Zakaria, S.J.; Hughes, L.P.; Lewiss, R.E.; Kehm, K.; Goodsell, K.; Kalwani, R.; Mirsch, D.; Kluger, S.B.; et al. A Comparison of Homemade Vascular Access Ultrasound Phantom Models for Peripheral Intravenous Catheter Insertion. J. Vasc. Access 2021, 22, 891–897. [Google Scholar] [CrossRef]
- da Silva, F.A.M.; De Matheo, L.L.; von Krüger, M.A.; de Albuquerque Pereira, W.C. Lung Ultrasonography Phantom for Lung-Pulse Sign Simulation. In XXVI Brazilian Congress on Biomedical Engineering; Costa-Felix, R., Machado, J.C., Alvarenga, A.V., Eds.; Springer Singapore: Singapore, 2019; pp. 831–836. [Google Scholar]
- Barillari, A.; Kiuru, S. Detection of Spontaneous Pneumothorax with Chest Ultrasound in the Emergency Department. Intern. Emerg. Med. 2010, 5, 253–255. [Google Scholar] [CrossRef]
- Oveland, N.P.; Sloth, E.; Andersen, G.; Lossius, H.M. A Porcine Pneumothorax Model for Teaching Ultrasound Diagnostics. Acad. Emerg. Med. 2012, 19, 586–592. [Google Scholar] [CrossRef]
- Schindelin, J.; Rueden, C.T.; Hiner, M.C.; Eliceiri, K.W. The ImageJ Ecosystem: An Open Platform for Biomedical Image Analysis. Mol. Reprod. Dev. 2015, 82, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An Open-Source Platform for Biological-Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Snider, E.J.; Hernandez-Torres, S.I.; Boice, E.N. An Image Classification Deep-Learning Algorithm for Shrapnel Detection from Ultrasound Images. Sci. Rep. 2022, 12, 8427. [Google Scholar] [CrossRef]
- Boice, E.N.; Hernandez-Torres, S.I.; Snider, E.J. Comparison of Ultrasound Image Classifier Deep Learning Algorithms for Shrapnel Detection. J. Imaging 2022, 8, 140. [Google Scholar] [CrossRef] [PubMed]
- Husain, L.F.; Hagopian, L.; Wayman, D.; Baker, W.E.; Carmody, K.A. Sonographic Diagnosis of Pneumothorax. J. Emerg. Trauma Shock 2012, 5, 76–81. [Google Scholar] [CrossRef]
- Narayan Das, N.; Kumar, N.; Kaur, M.; Kumar, V.; Singh, D. Automated Deep Transfer Learning-Based Approach for Detection of COVID-19 Infection in Chest X-Rays. IRBM 2020, 43, 114–119. [Google Scholar] [CrossRef]
- Born, J.; Wiedemann, N.; Cossio, M.; Buhre, C.; Brändle, G.; Leidermann, K.; Aujayeb, A.; Moor, M.; Rieck, B.; Borgwardt, K. Accelerating Detection of Lung Pathologies with Explainable Ultrasound Image Analysis. Appl. Sci. 2021, 11, 672. [Google Scholar] [CrossRef]
- Baloescu, C.; Toporek, G.; Kim, S.; McNamara, K.; Liu, R.; Shaw, M.M.; McNamara, R.L.; Raju, B.I.; Moore, C.L. Automated Lung Ultrasound B-Line Assessment Using a Deep Learning Algorithm. IEEE Trans. Ultrason. Ferroelectr. Freq. Control. 2020, 67, 2312–2320. [Google Scholar] [CrossRef]
- La Salvia, M.; Secco, G.; Torti, E.; Florimbi, G.; Guido, L.; Lago, P.; Salinaro, F.; Perlini, S.; Leporati, F. Deep Learning and Lung Ultrasound for COVID-19 Pneumonia Detection and Severity Classification. Comput. Biol. Med. 2021, 136, 104742. [Google Scholar] [CrossRef]
- Lin, Z.; Li, Z.; Cao, P.; Lin, Y.; Liang, F.; He, J.; Huang, L. Deep Learning for Emergency Ascites Diagnosis Using Ultrasonography Images. J. Appl. Clin. Med. Phys. 2022, 23, e13695. [Google Scholar] [CrossRef]
- Singh, A.K.; Mayo, P.H.; Koenig, S.; Talwar, A.; Narasimhan, M. The Use of M-Mode Ultrasonography to Differentiate the Causes of B Lines. Chest 2018, 153, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Prada, G.; Vieillard-Baron, A.; Martin, A.K.; Hernandez, A.; Mookadam, F.; Ramakrishna, H.; Diaz-Gomez, J.L. Tracheal, Lung, and Diaphragmatic Applications of M-Mode Ultrasonography in Anesthesiology and Critical Care. J. Cardiothorac. Vasc. Anesth. 2021, 35, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, T.; Tang, Y.-M.; Benson, M.D.; King, S. Diaphragmatic Paralysis: The Use of M Mode Ultrasound for Diagnosis in Adults. Spinal Cord 2006, 44, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Na, S.; Choi, J.-S.; Na, S.H.; Shin, S.; Koh, S.O. An Evaluation of Diaphragmatic Movement by M-Mode Sonography as a Predictor of Pulmonary Dysfunction after Upper Abdominal Surgery. Anesth. Analg. 2010, 110, 1349–1354. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. MobileNetV2: Inverted Residuals and Linear Bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018. [Google Scholar] [CrossRef]
- Shahriari, B.; Swersky, K.; Wang, Z.; Adams, R.P.; de Freitas, N. Taking the Human Out of the Loop: A Review of Bayesian Optimization. Proc. IEEE 2016, 104, 148–175. [Google Scholar] [CrossRef]
- Snoek, J.; Larochelle, H.; Adams, R.P. Practical Bayesian Optimization of Machine Learning Algorithms. In Advances in Neural Information Processing Systems; Pereira, F., Burges, C.J., Bottou, L., Weinberger, K.Q., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2012; Volume 25. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Augmentation | Testing Type | Accuracy | Precision | Recall | Specificity | F1 |
|---|---|---|---|---|---|---|
| None | Split | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Swine | 0.500 | - | - | 1.000 | - | |
| Only X-Y Flip and Zoom | Split | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Swine | 0.500 | - | - | 1.000 | - | |
| + Histogram Normalization | Split | 0.999 | 0.999 | 1.000 | 0.999 | 0.999 |
| Swine | 0.825 | 0.792 | 0.969 | 0.68 | 0.862 | |
| + Contrast/Brightness | Split | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 |
| Swine | 0.936 | 0.898 | 0.998 | 0.873 | 0.942 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boice, E.N.; Hernandez Torres, S.I.; Knowlton, Z.J.; Berard, D.; Gonzalez, J.M.; Avital, G.; Snider, E.J. Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom Apparatus. J. Imaging 2022, 8, 249. https://doi.org/10.3390/jimaging8090249
Boice EN, Hernandez Torres SI, Knowlton ZJ, Berard D, Gonzalez JM, Avital G, Snider EJ. Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom Apparatus. Journal of Imaging. 2022; 8(9):249. https://doi.org/10.3390/jimaging8090249
Chicago/Turabian StyleBoice, Emily N., Sofia I. Hernandez Torres, Zechariah J. Knowlton, David Berard, Jose M. Gonzalez, Guy Avital, and Eric J. Snider. 2022. "Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom Apparatus" Journal of Imaging 8, no. 9: 249. https://doi.org/10.3390/jimaging8090249
APA StyleBoice, E. N., Hernandez Torres, S. I., Knowlton, Z. J., Berard, D., Gonzalez, J. M., Avital, G., & Snider, E. J. (2022). Training Ultrasound Image Classification Deep-Learning Algorithms for Pneumothorax Detection Using a Synthetic Tissue Phantom Apparatus. Journal of Imaging, 8(9), 249. https://doi.org/10.3390/jimaging8090249