
Qualitative Comparison of Image Stitching Algorithms for Multi-Camera Systems in Laparoscopy

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Multi-Camera Systems
1.2. Image Stitching in Current Multi-Camera Systems
1.3. Analysis
1.4. Goals and Contributions
2. State-of-the-Art in Image Stitching
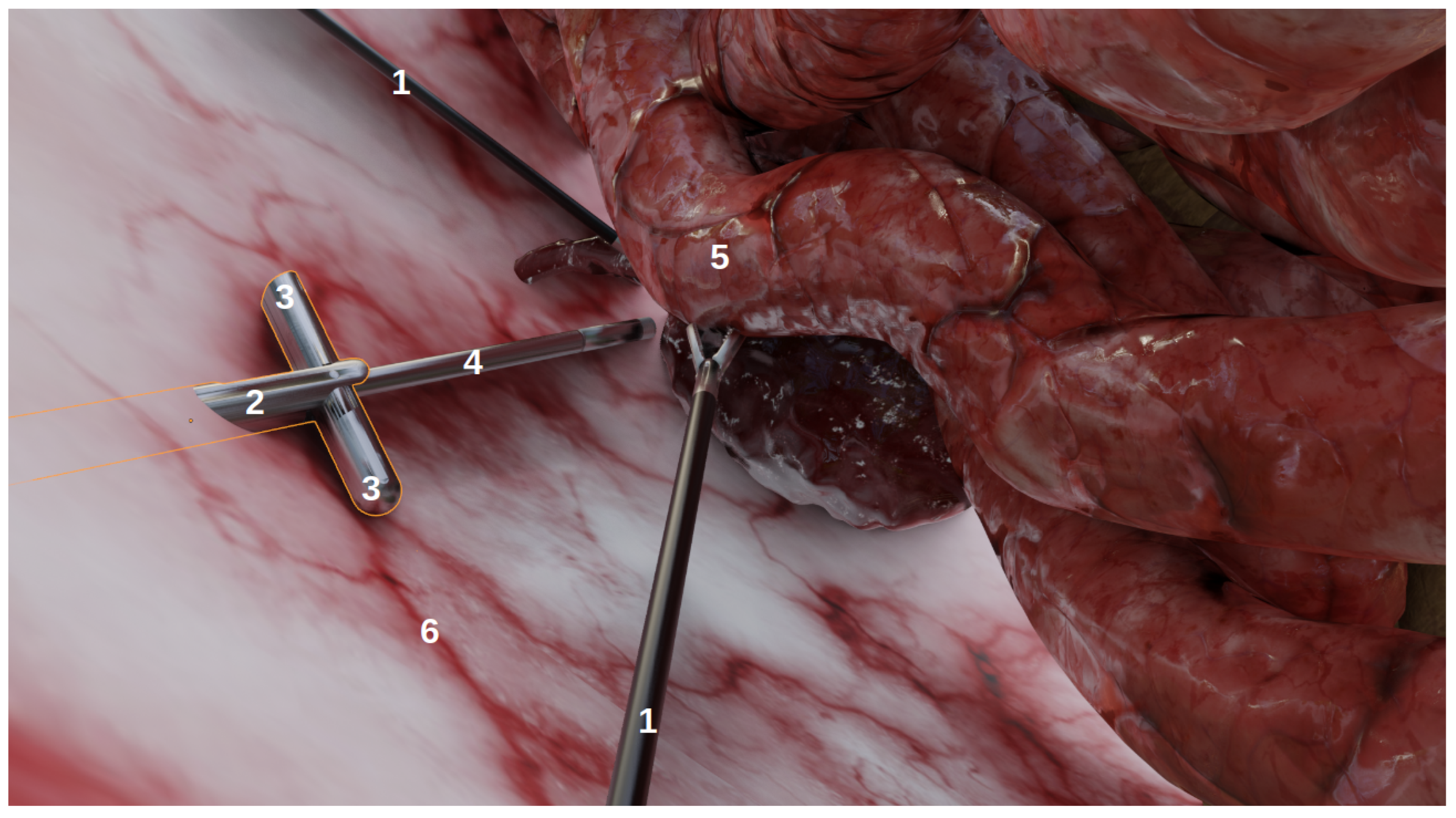
3. Material: A New Simulated Environment
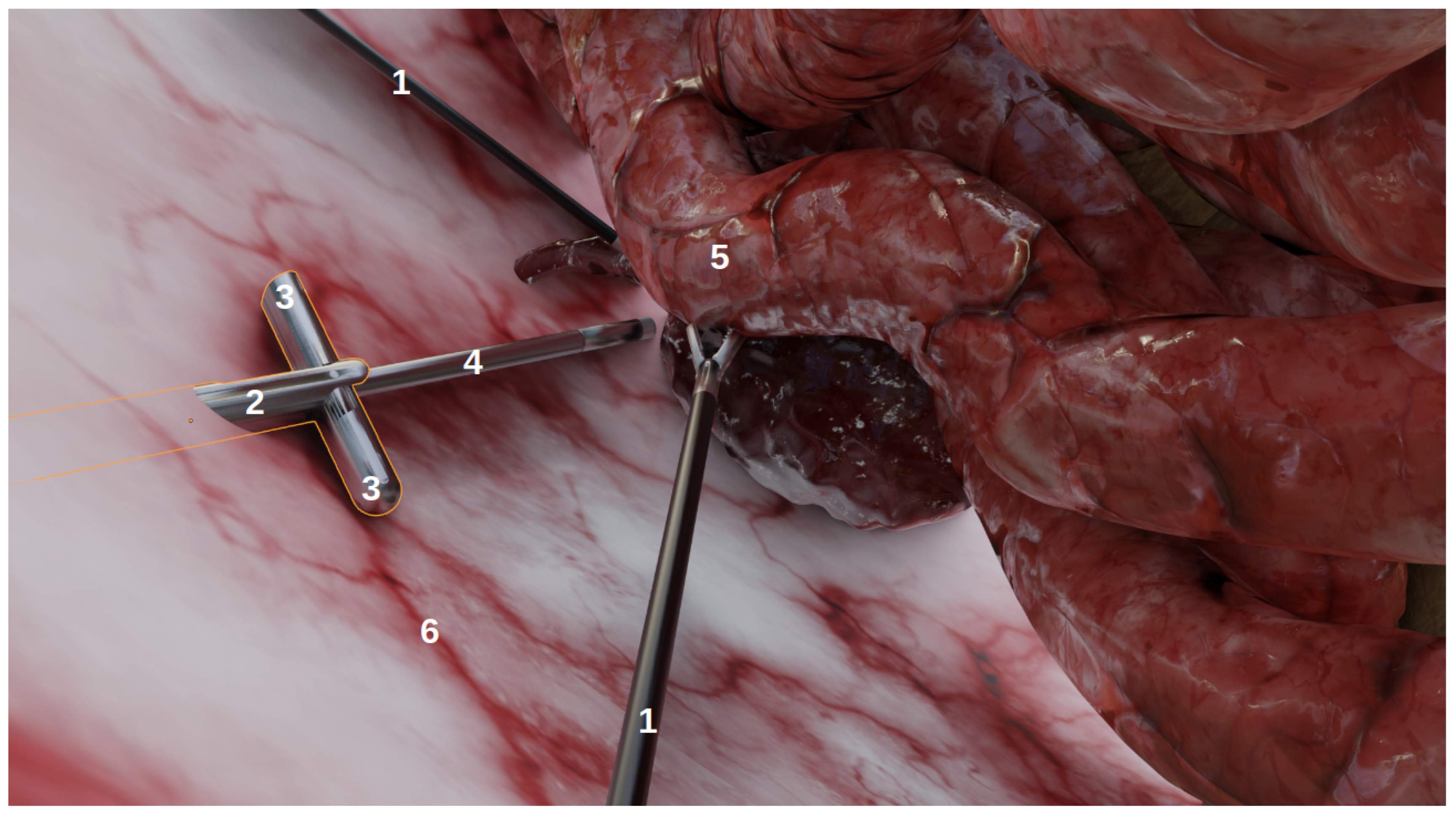
- Organs, with corresponding realistic image textures, e.g., intestines, blood vessels, abdomen;
- Tools: laparoscopic forceps and a 5 mm endoscope with LEDs;
- Multi-camera prototypes, where the number of cameras and their focals, FoVs and inter-spaces can be modified. In this study, we simulated the multi-camera prototype of [6] with two deployable Misumi TD-VBL31105L-77 cameras (1.83 mm focal, 69° × 43° FoV) and an inter-space of 4.5 cm. These specifications were established according to the results of a specifically performed experiment, provided in Supplementary Material Figures S4 and S5, which showed that this was a good compromise between overlap and the enlargement of the field of view.
- Tools: e.g., the number/position/orientation of forceps;
- Endoscope: the depth inside the abdomen cavity, camera parameters (e.g., focal, resolution), the power of the LEDs;
- Multi-camera system: the position/orientation of the device, camera parameters (e.g., focal, resolution), the power of the LEDs;
- Rendering parameters: the type of rendering engine, output image resolution and exposure.
4. Benchmarking of Image Stitching Algorithms
4.1. Methodology
4.2. Experiments
5. Results
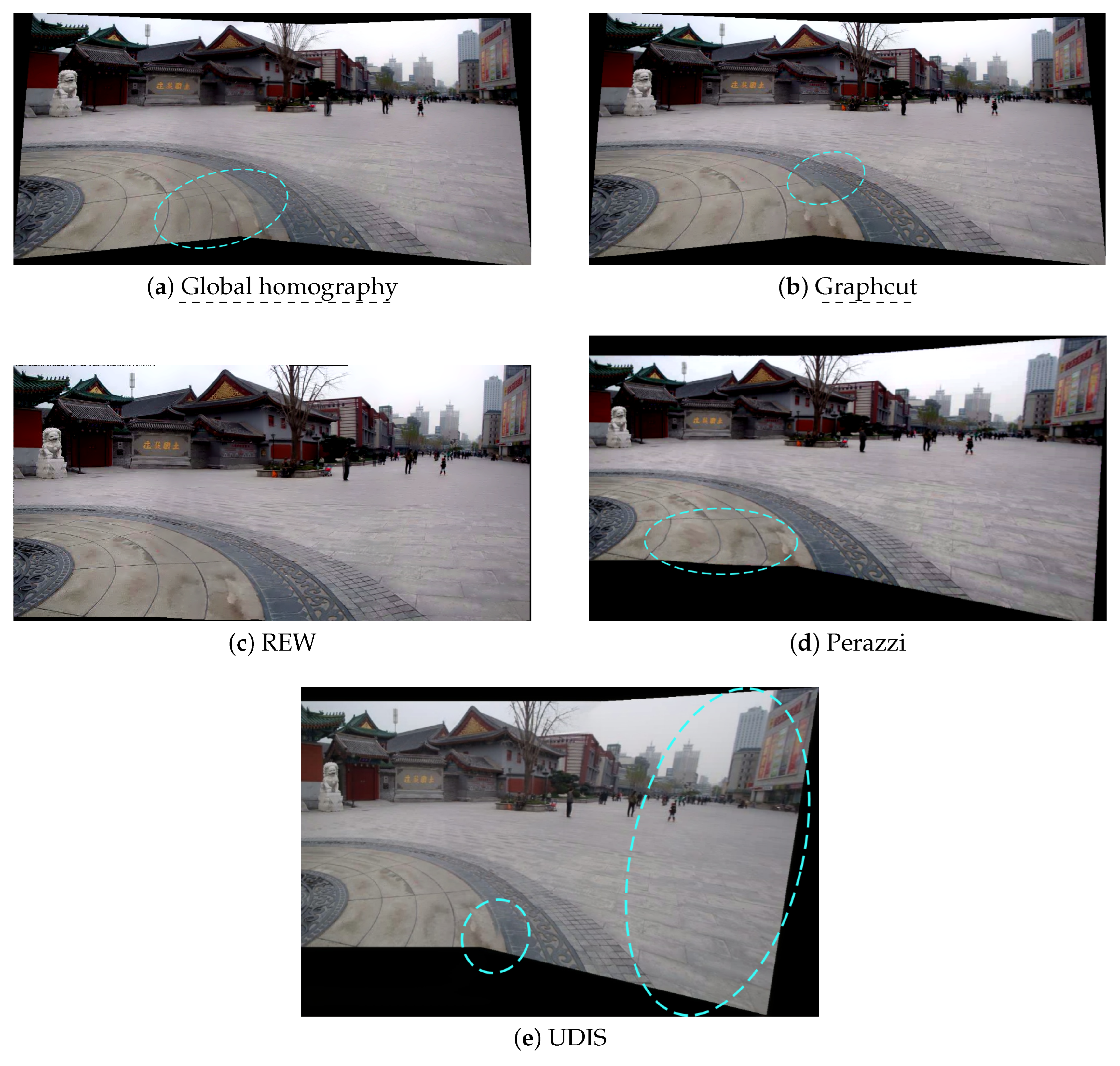
5.1. Experiment 1: On a Non-Laparoscopic Scenario
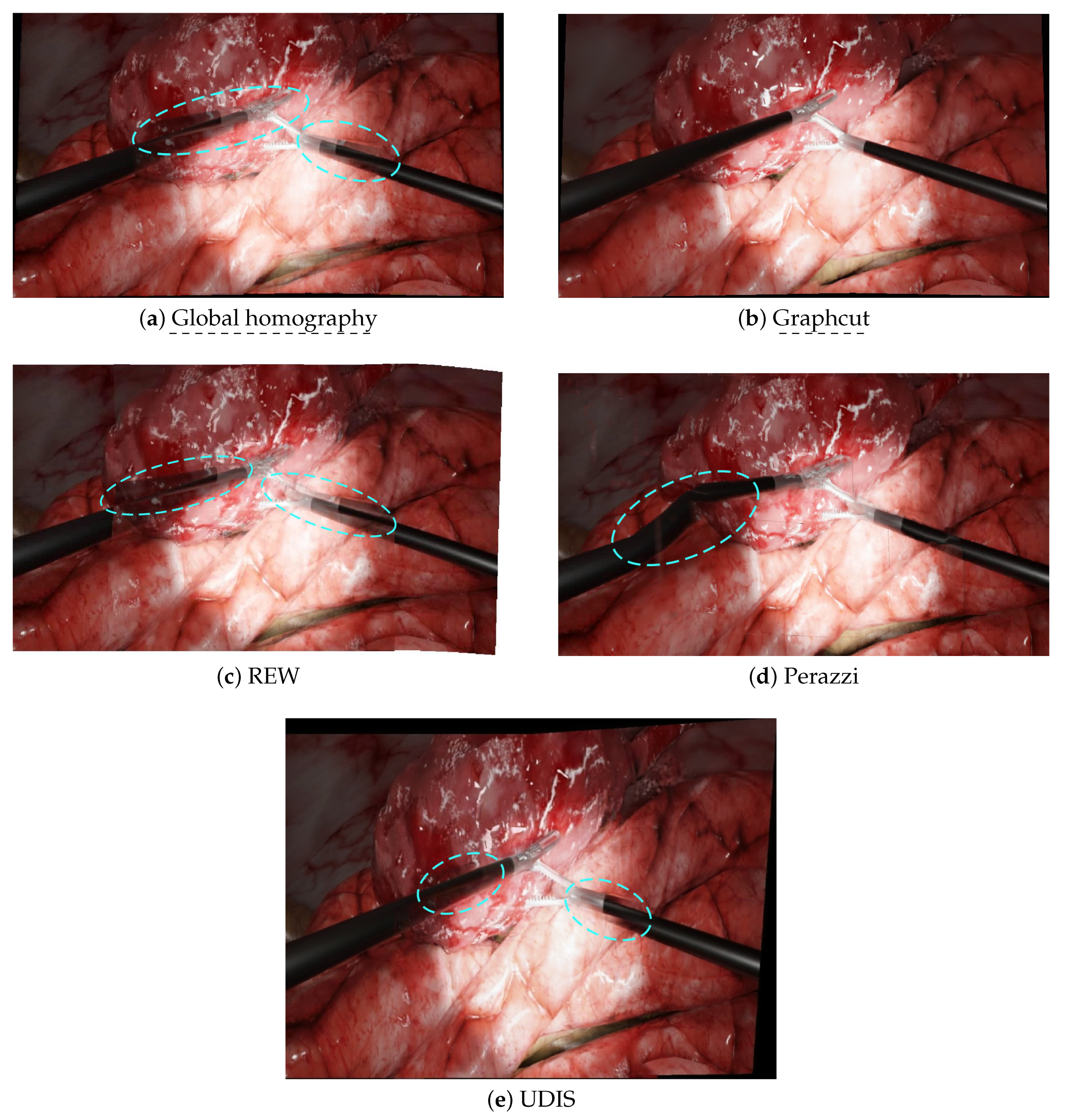
5.2. Experiment 2: Laparoscopic Scenarios
6. Analysis
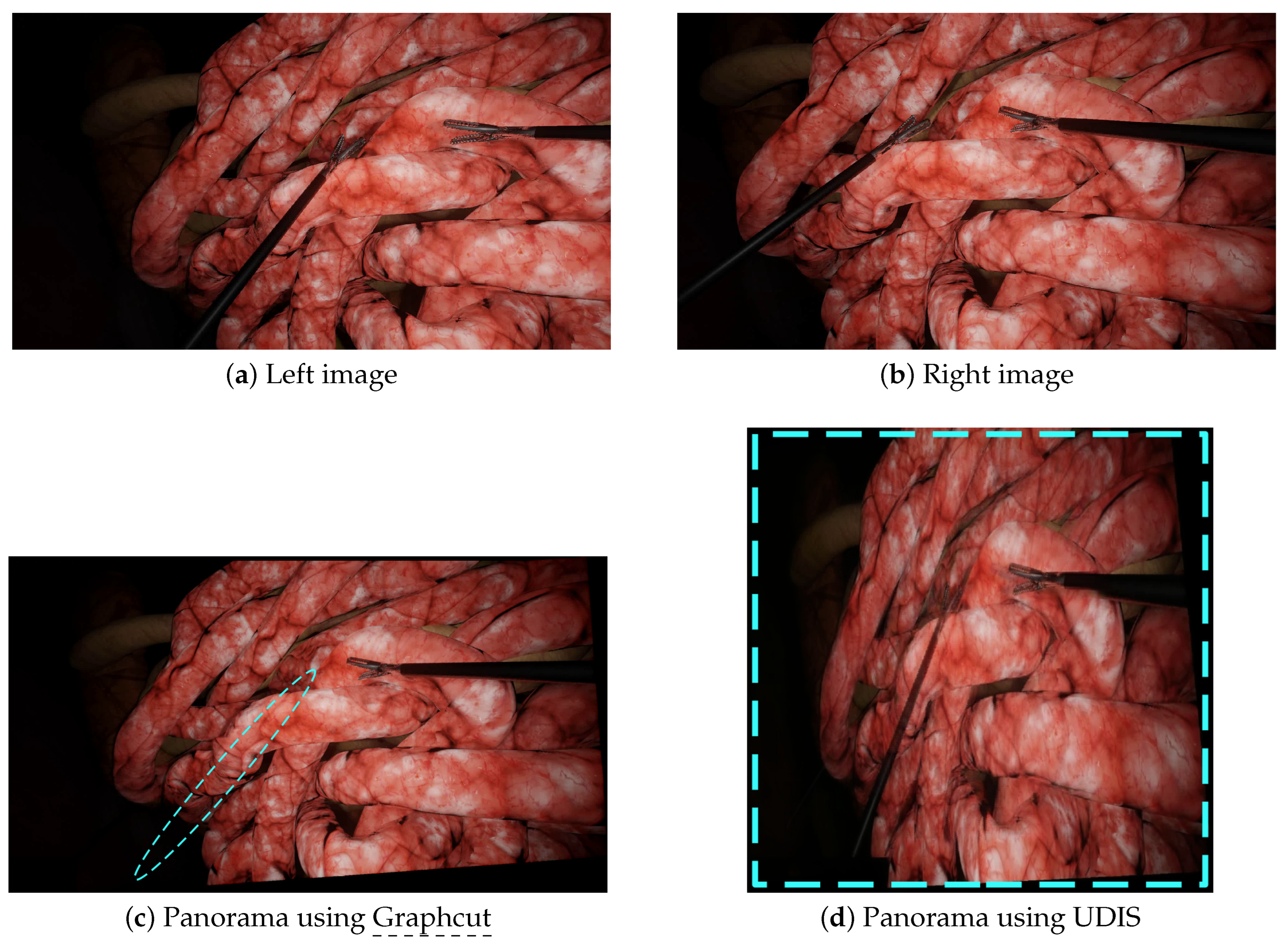
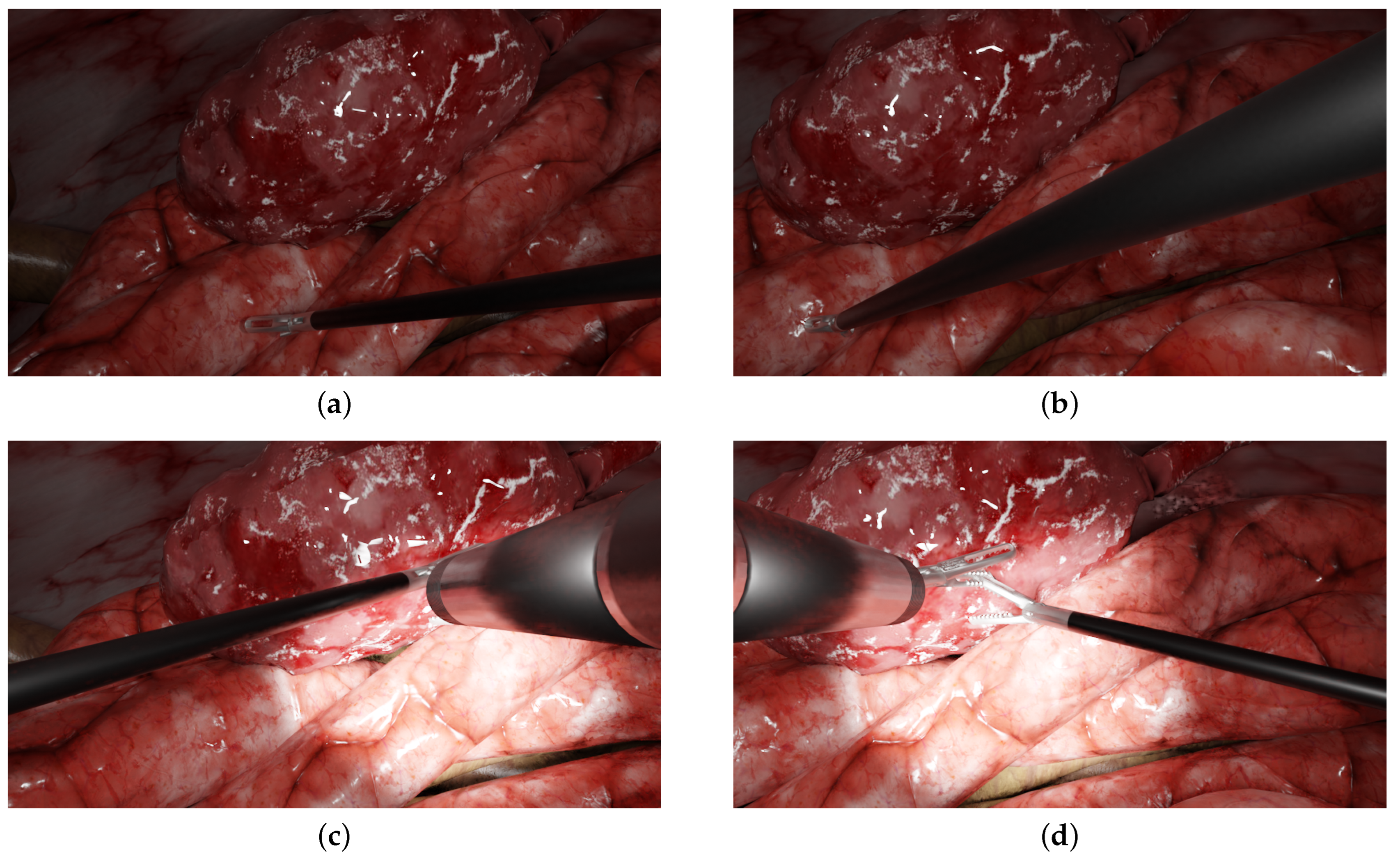
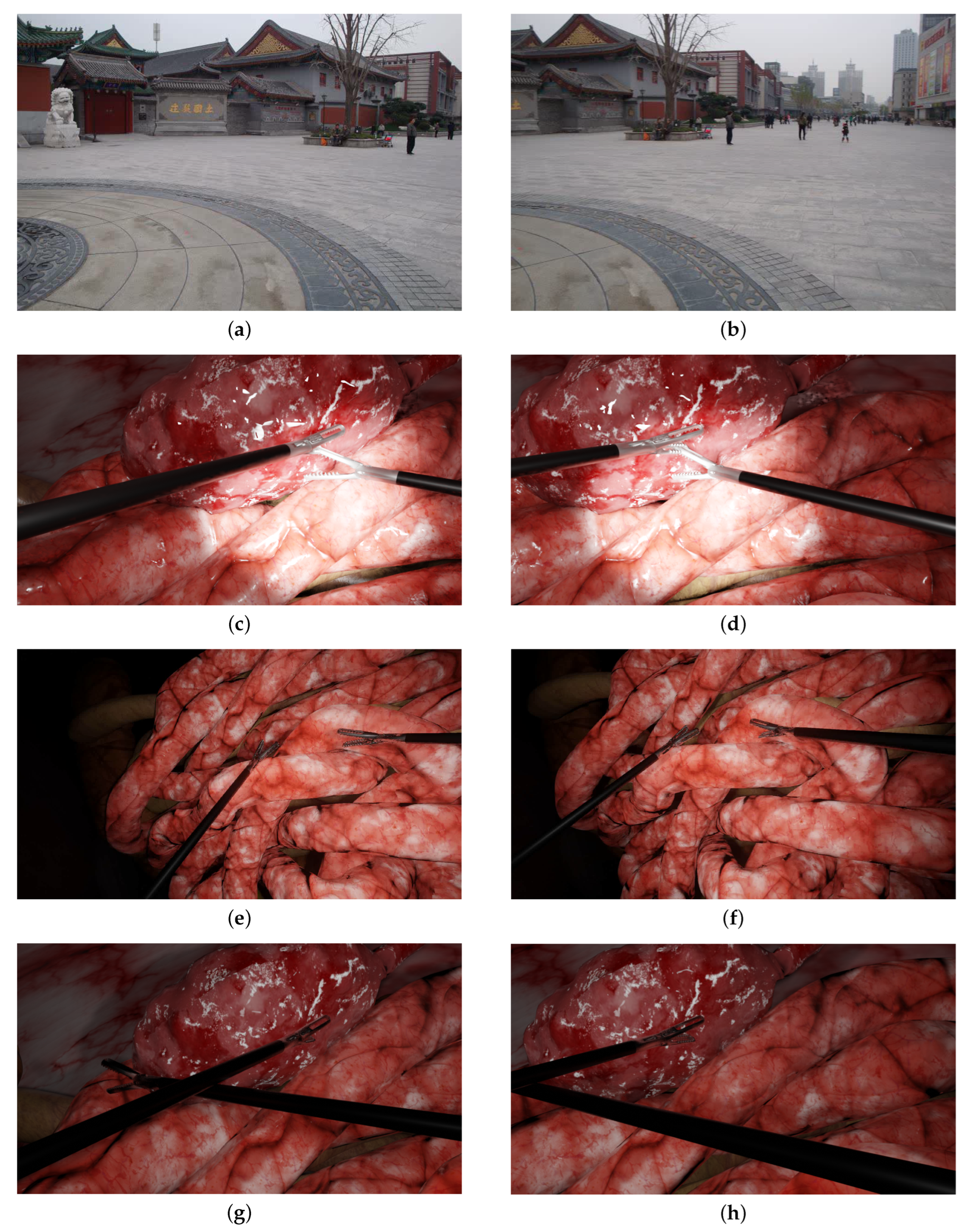
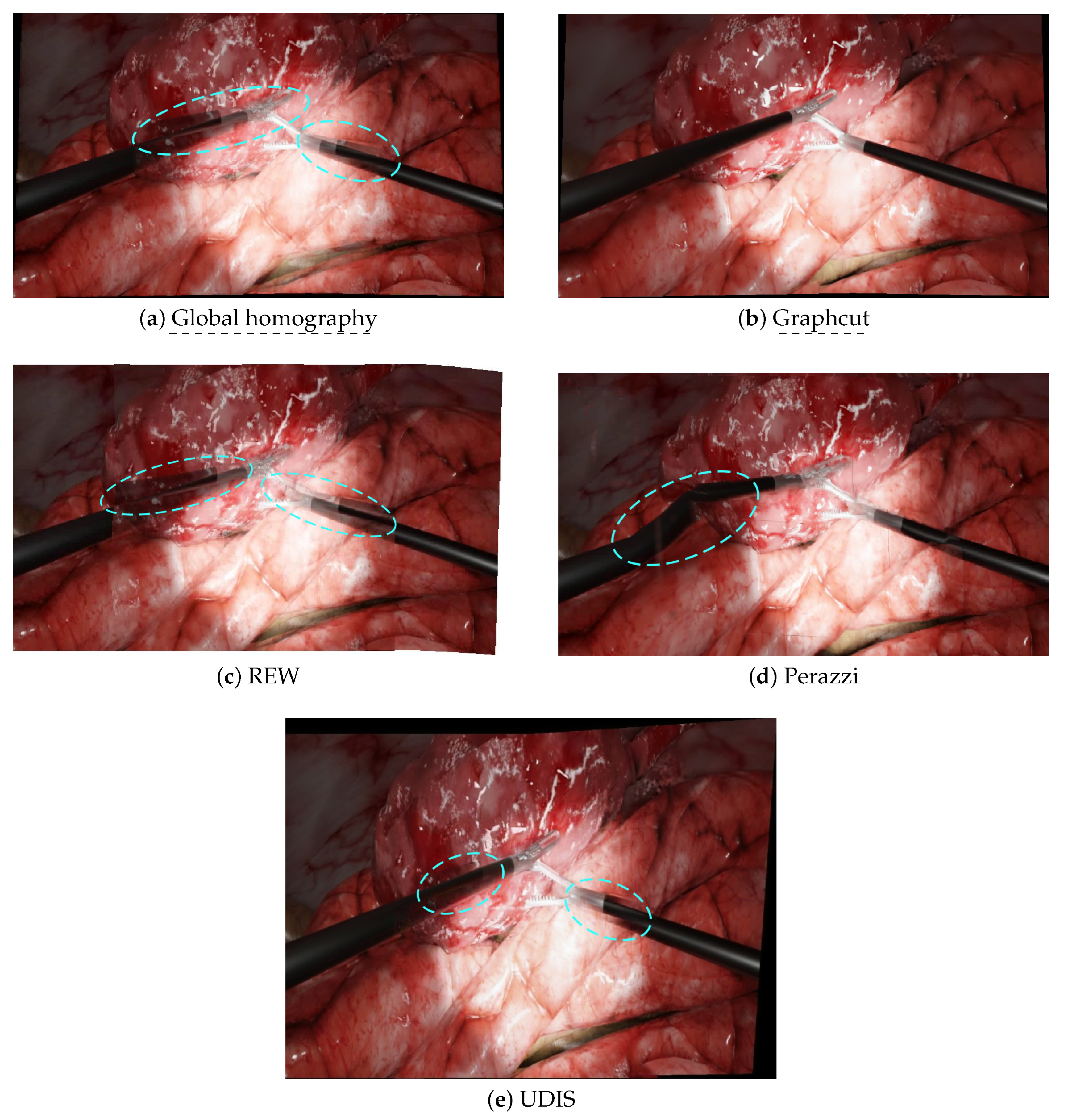
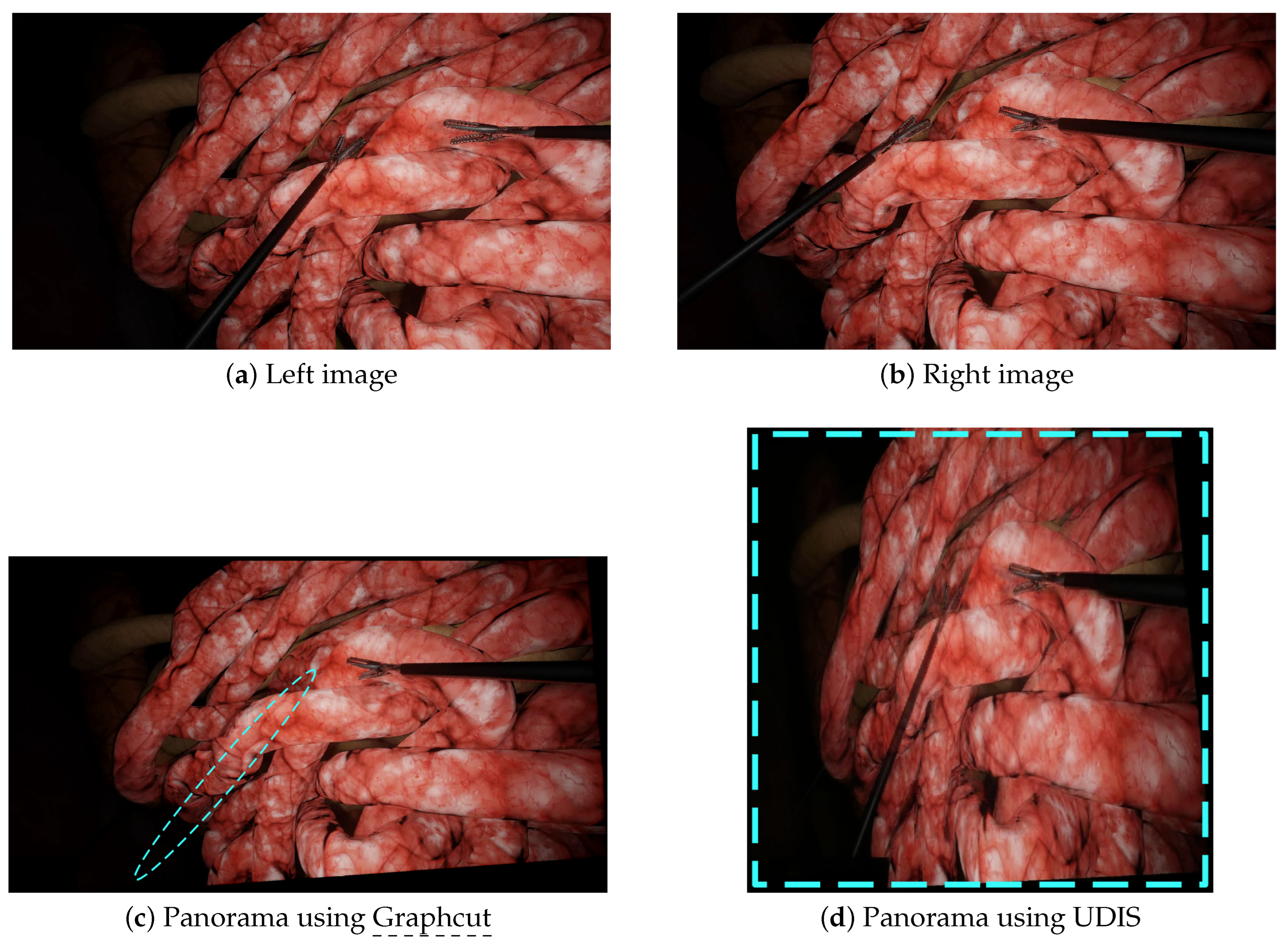
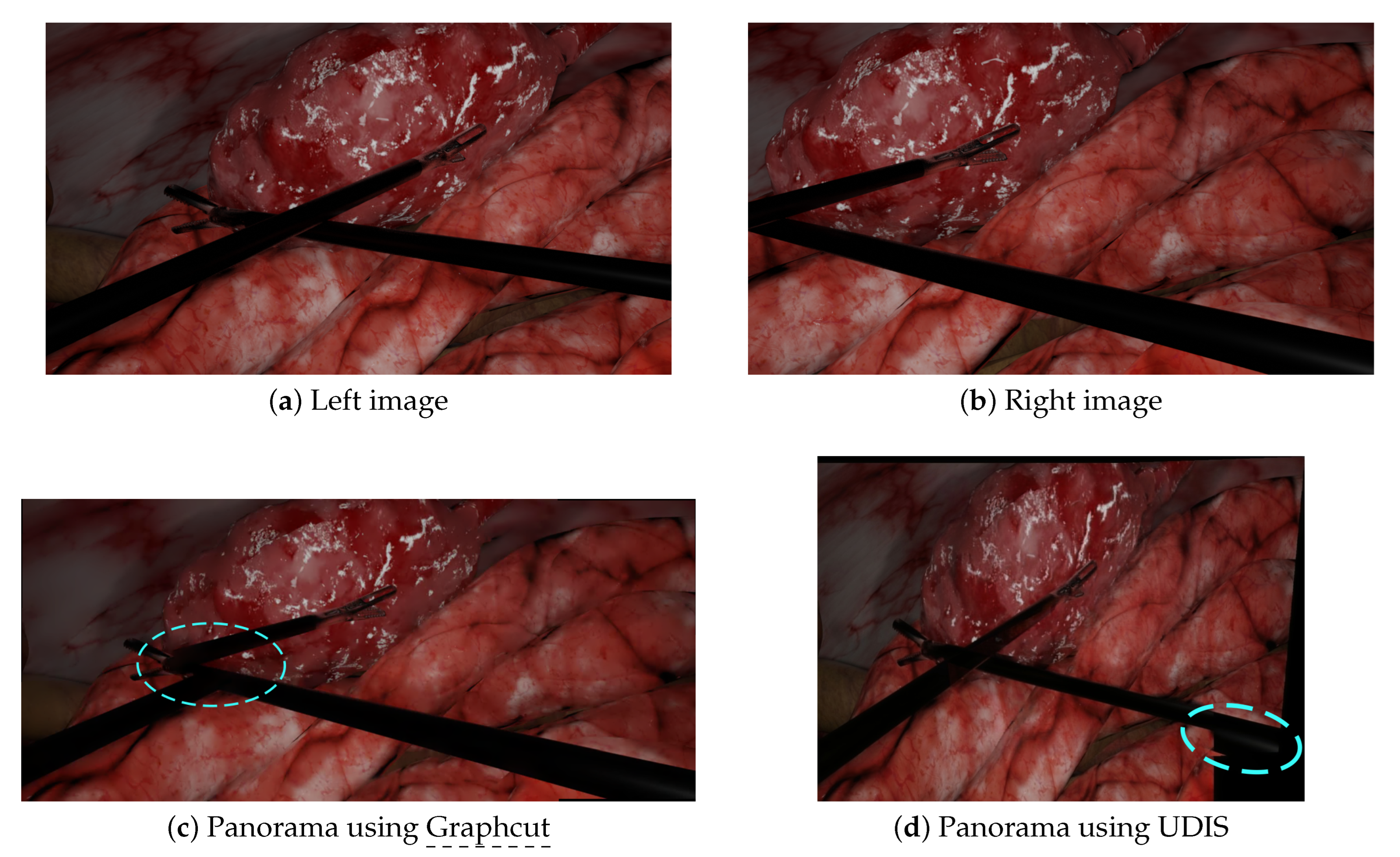
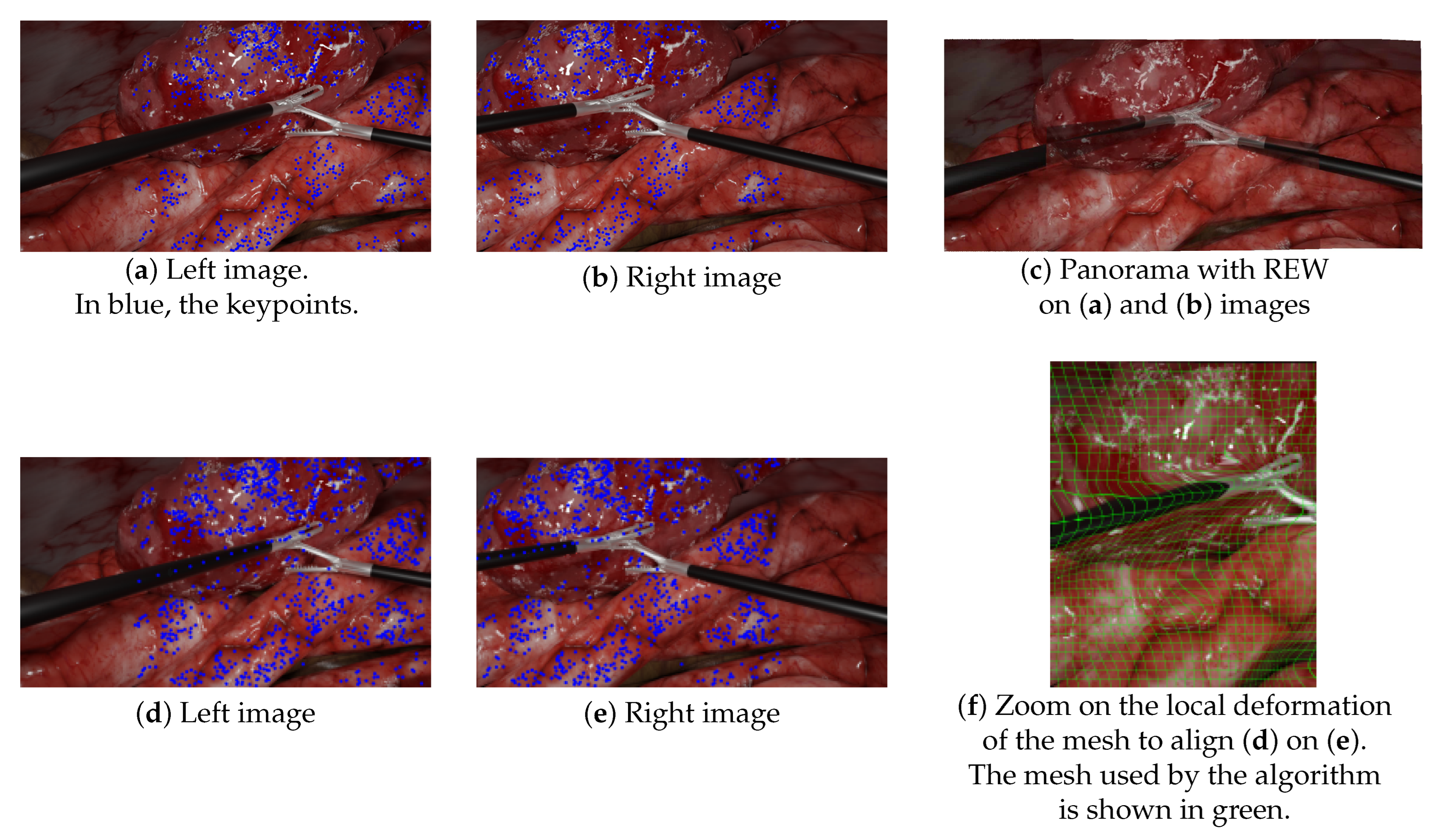
- The lack of keypoints in textureless areas, such as tools: Figure 9a–c illustrates this lack of keypoints on laparoscopic tools, resulting in the poor alignment of the aforementioned tools. This issue is not specific to our simulated environment, as laparoscopic tools are generally mostly uniform. As previous research that has attempted to propose more textured instruments has never been translated into clinical use, this issue remains a challenge to solve. Kim et al. [10] tried to handle this by replacing keypoint detection with a disparity-based approach that was more robust to textureless areas. However, since their evaluation was performed without any visible instruments, there is no guarantee that it would help to find keypoints on the tools;
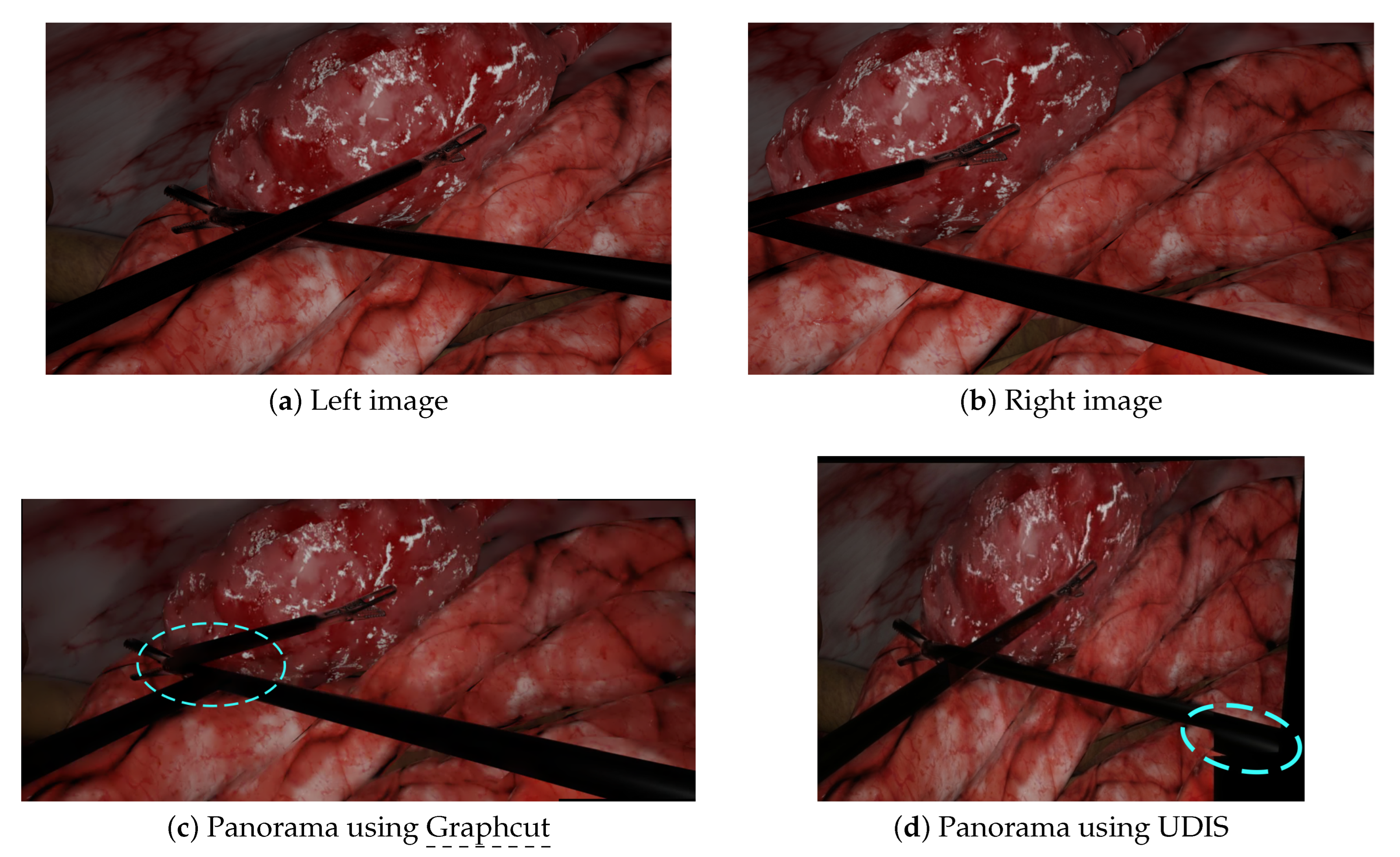
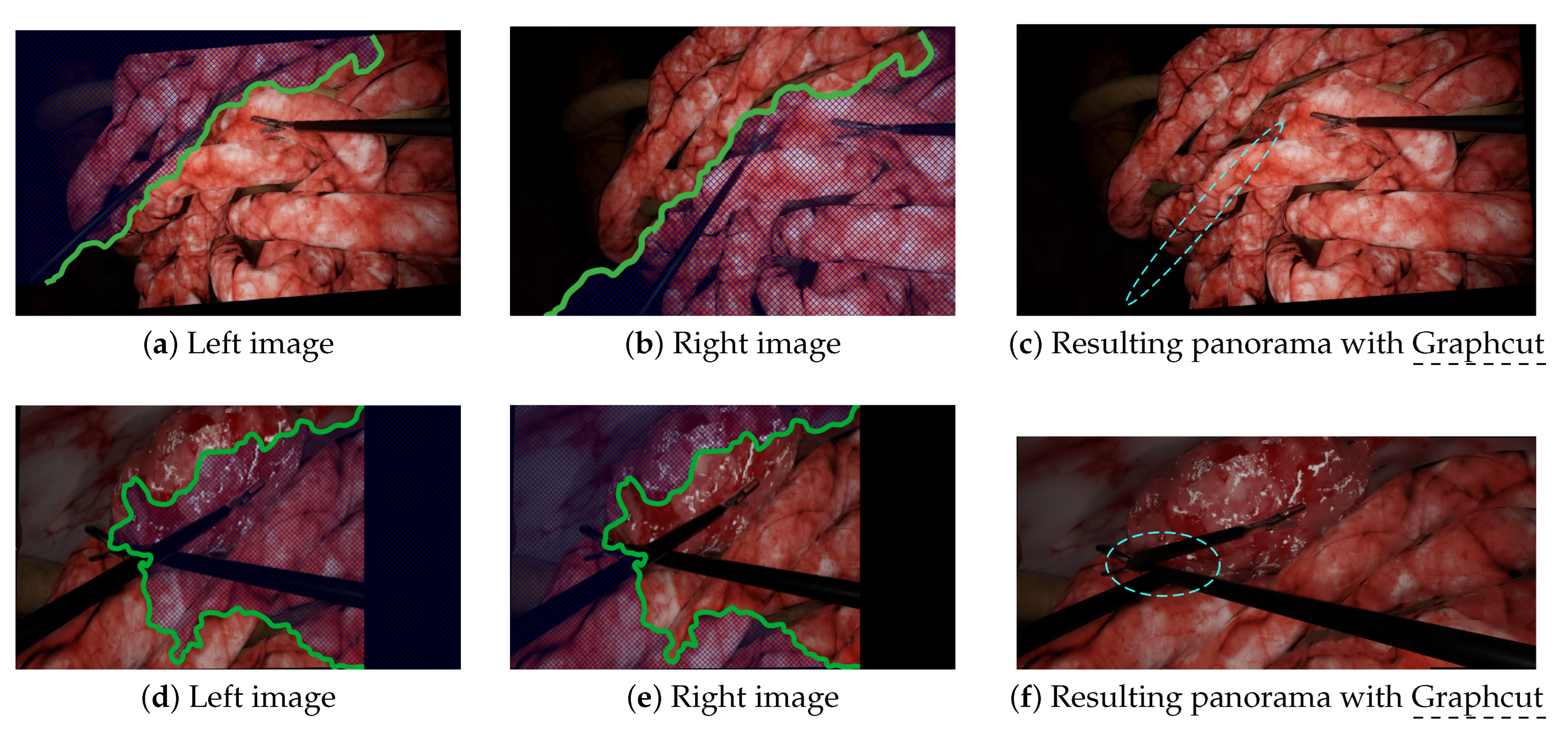
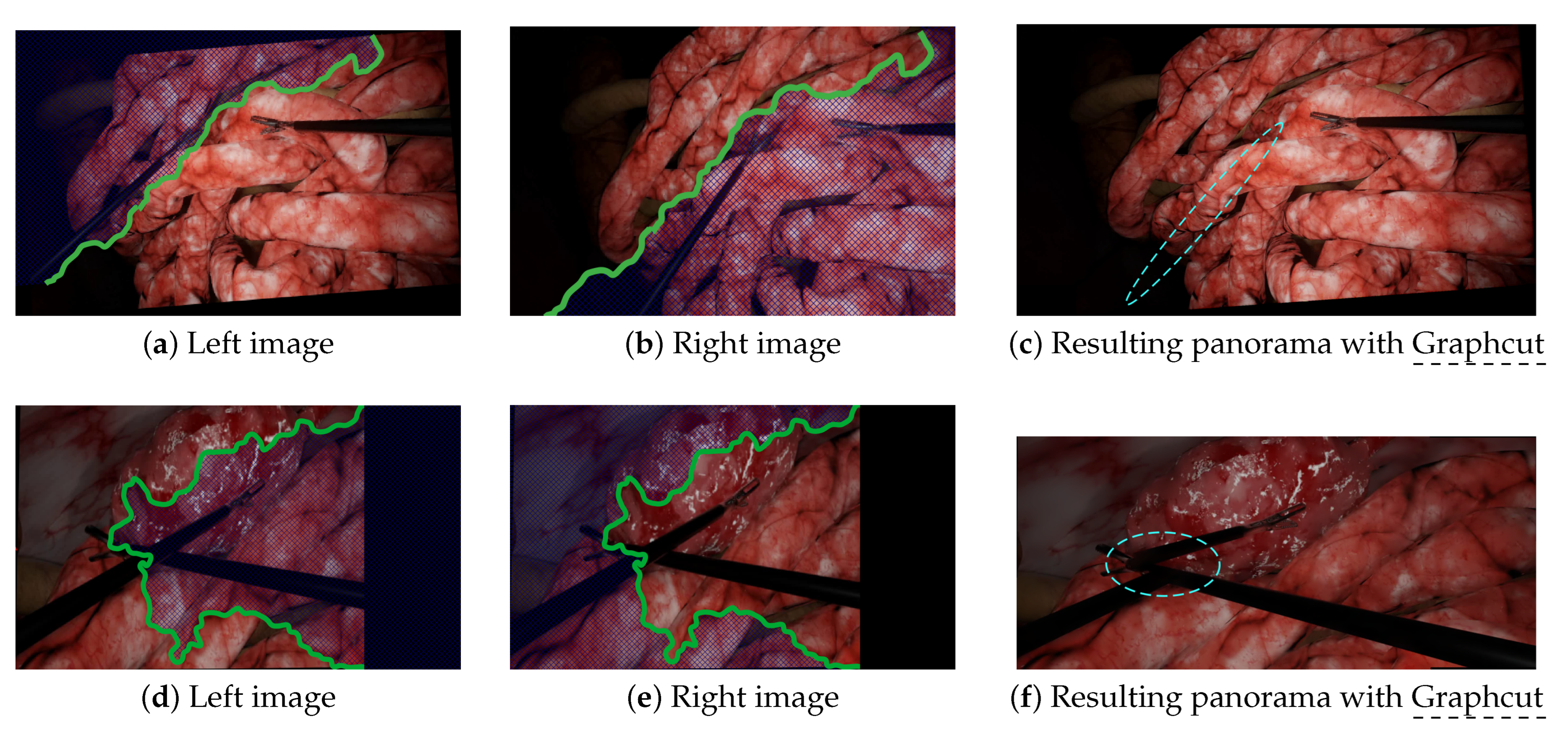
- Mesh-based methods are intrinsically inadequate in situations containing objects in very different planes. Since mesh-based models compute the continuous deformation of a grid, they expect the parallax issue to be some kind of continuous problem through space too. While being somewhat true in outdoor panoramic photography, this is incorrect in laparoscopy, which contains very thin objects in the foreground. This issue is illustrated in Figure 9d–f. In this experiment, we manually added keypoints along the left tool to force REW to align them. As shown in Figure 9f, it induced a significant local deformation along the tool due to the brutal variation of parallax between the foreground tool and the background. There was not a smooth transition of parallax here.
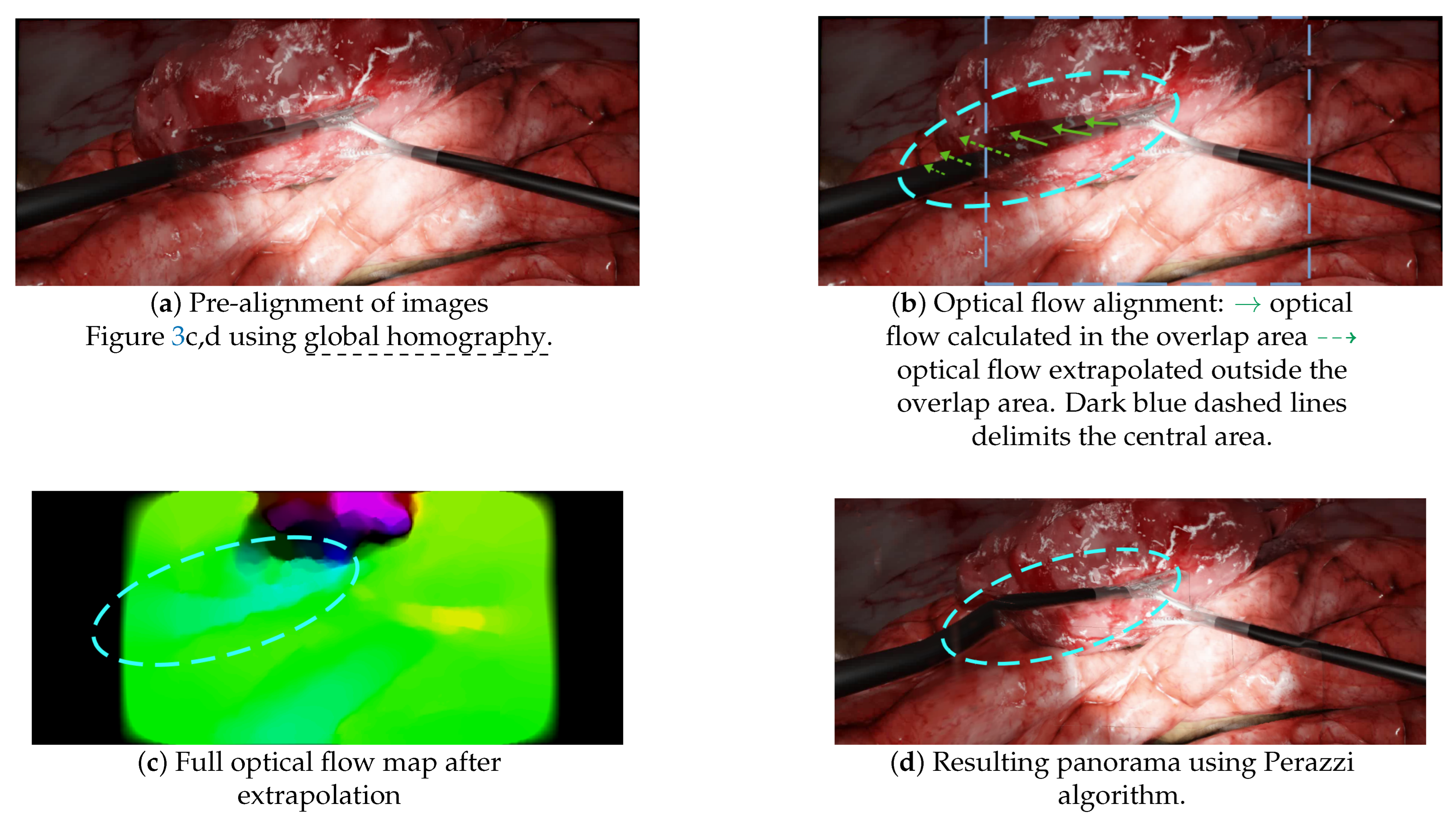
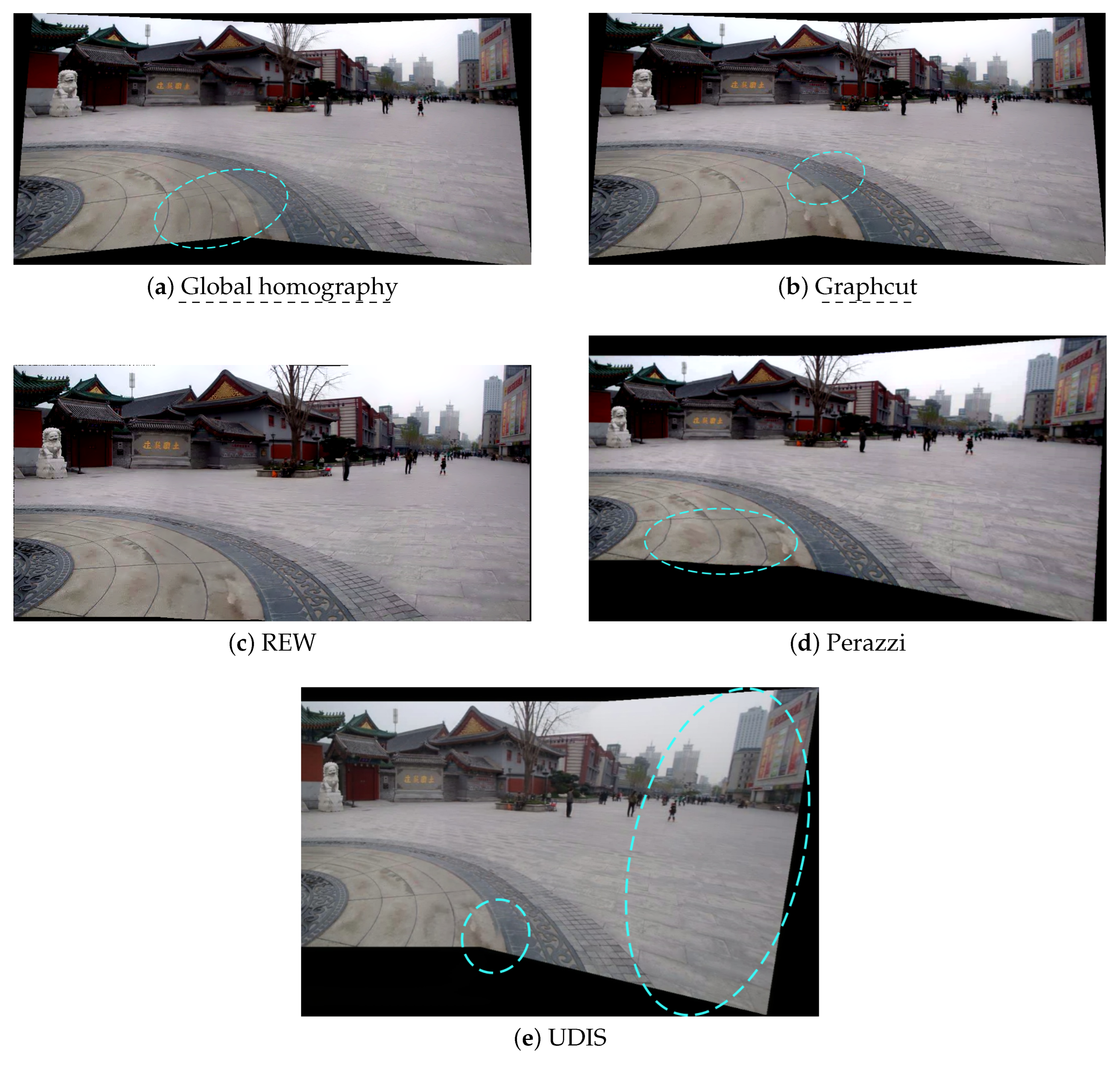
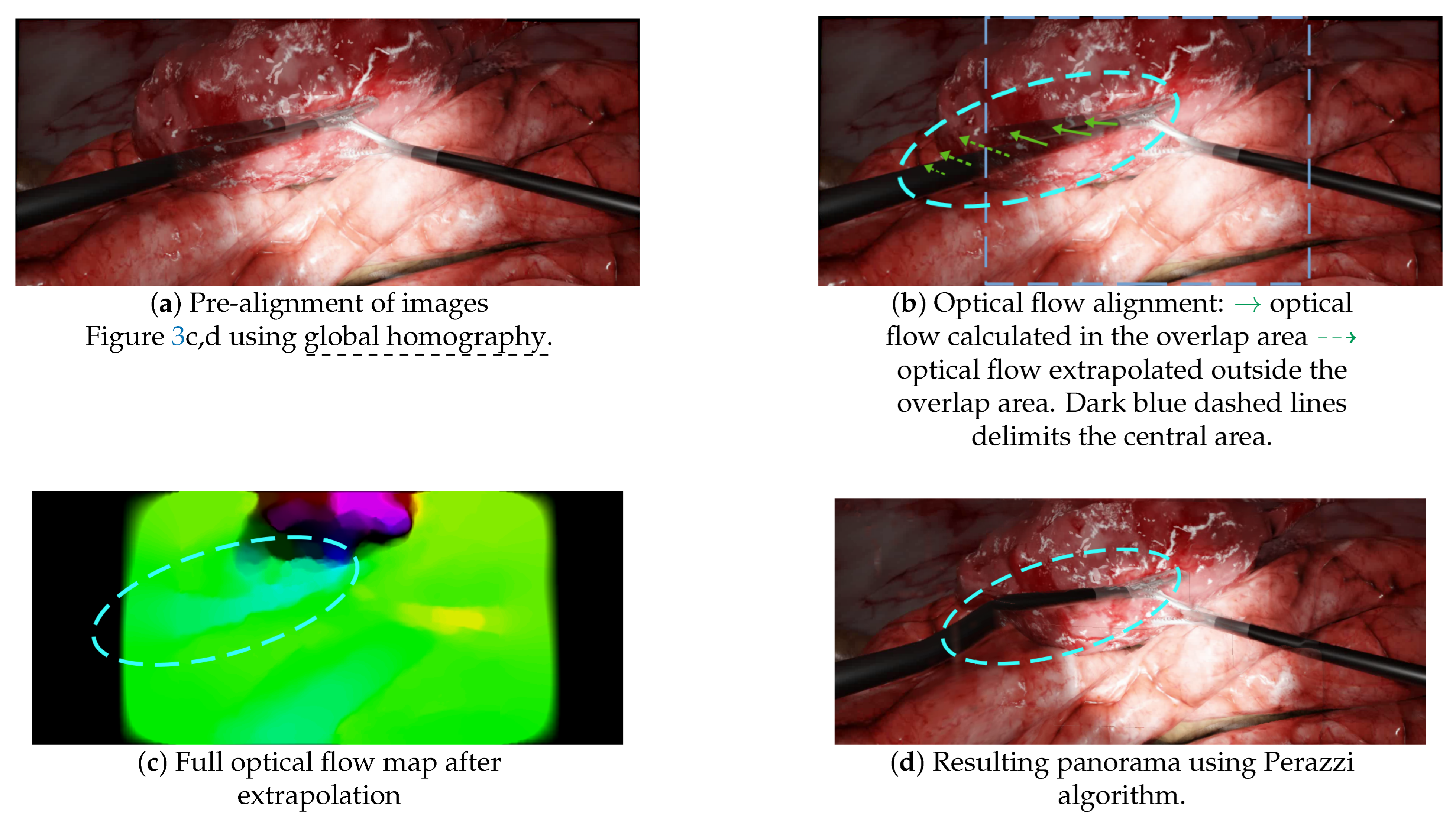
- A pre-alignment is performed using global homography, which introduces projective distortions, as illustrated in Figure 4d;
- Optical flow is then computed in the overlap area and extrapolated to outer areas, as illustrated in Figure 10b,c. This extrapolation, also called “weighted warp extrapolation”, was designed by Perazzi to smoothly join the overlap and non-overlap areas in the panorama. However, this extrapolation is performed uniformly in all directions, ignoring the structures in the image. In the laparoscopic situations, it bent the tools to join them, without considering the expected straightness of forceps, as illustrated in Figure 10d.
- The distortions: UDIS relies on a two-step pipeline, with the first step of homography estimation and the second step of refinement. This first homography estimation was not designed to minimise projective distortions and the following step of refinement cannot correct the resulting distortions;
- The duplicated elements: since deep learning approaches are data-driven approaches, it may be more appropriate to train the model with more adapted data, i.e., using thousands of laparoscopic data from our simulated environment. It would, however, require more varied scene backgrounds than those currently available in the environment.
7. Discussion
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANR | French National Research Agency |
| CPW | Content-preserving warp |
| FoV | Field of view |
| LED | Light-emitting diode |
| SIFT | Scale-invariant feature transform |
| SURF | Speeded-up robust features |
References
- Makhoul, B.; De La Taille, A.; Vordos, D.; Salomon, L.; Sebe, P.; Audet, J.; Ruiz, L.; Hoznek, A.; Antiphon, P.; Cicco, A.; et al. Laparoscopic radical nephrectomy for T1 renal cancer: The gold standard? A comparison of laparoscopic vs open nephrectomy. BJU Int. 2004, 93, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Roulet, P.; Konen, P.; Villegas, M.; Thibault, S.; Garneau, P.Y. 360 endoscopy using panomorph lens technology. In Endoscopic Microscopy V; International Society for Optics and Photonics: Bellingham, WA, USA, 2010; Volume 7558, p. 75580T. [Google Scholar]
- Kobayashi, E.; Masamune, K.; Sakuma, I.; Dohi, T. A Wide-Angle View Endoscope System Using Wedge Prisms. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Pittsburgh, PA, USA, 11–14 October 2000; Springer: Berlin/Heidelberg, Germany, 2000; pp. 661–668. [Google Scholar]
- Rivera, D.R.; Brown, C.M.; Ouzounov, D.G.; Pavlova, I.; Kobat, D.; Webb, W.W.; Xu, C. Compact and flexible raster scanning multiphoton endoscope capable of imaging unstained tissue. Proc. Natl. Acad. Sci. USA 2011, 108, 17598–17603. [Google Scholar] [CrossRef] [Green Version]
- Seibel, E.J.; Fauver, M.; Crossman-Bosworth, J.L.; Smithwick, Q.Y.; Brown, C.M. Microfabricated Optical Fiber with a Microlens That Produces Large Field-of-View Video-Rate Optical Beam Scanning for Microendoscopy Applications. In Optical Fibers and Sensors for Medical Applications III; International Society for Optics and Photonics: Bellingham, WA, USA, 2003; Volume 4957, pp. 46–55. [Google Scholar]
- Trilling, B.; Mancini, A.; Fiard, G.; Barraud, P.A.; Decrouez, M.; Vijayan, S.; Tummers, M.; Faucheron, J.L.; Silvent, S.; Schwartz, C.; et al. Improving vision for surgeons during laparoscopy: The Enhanced Laparoscopic Vision System (ELViS). Surg. Endosc. 2021, 35, 2403–2415. [Google Scholar] [CrossRef] [PubMed]
- Tamadazte, B.; Voros, S.; Boschet, C.; Cinquin, P.; Fouard, C. Augmented 3-d View for Laparoscopy Surgery. In Workshop on Augmented Environments for Computer-Assisted Interventions; Springer: Berlin/Heidelberg, Germany, 2012; pp. 117–131. [Google Scholar]
- Trilling, B.; Vijayan, S.; Goupil, C.; Kedisseh, E.; Letouzey, A.; Barraud, P.; Faucheron, J.; Fiard, G.; Voros, S. Enhanced Laparoscopic Vision Improves Detection of Intraoperative Adverse Events During Laparoscopy. IRBM, 2020, in press. [CrossRef]
- Kim, J.J.; Watras, A.; Liu, H.; Zeng, Z.; Greenberg, J.A.; Heise, C.P.; Hu, Y.H.; Jiang, H. Large-Field-of-View Visualization Utilizing Multiple Miniaturized Cameras for Laparoscopic Surgery. Micromachines 2018, 9, 431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.T.; Cheng, C.H.; Liu, D.G.; Liu, K.C.J.; Huang, W.S.W. Designing a New Endoscope for Panoramic-View with Focus-Area 3D-Vision in Minimally Invasive Surgery. J. Med. Biol. Eng. 2020, 40, 204–219. [Google Scholar] [CrossRef] [Green Version]
- Peter, L.; Tella-Amo, M.; Shakir, D.I.; Attilakos, G.; Wimalasundera, R.; Deprest, J.; Ourselin, S.; Vercauteren, T. Retrieval and registration of long-range overlapping frames for scalable mosaicking of in vivo fetoscopy. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bano, S.; Vasconcelos, F.; Amo, M.T.; Dwyer, G.; Gruijthuijsen, C.; Deprest, J.; Ourselin, S.; Vander Poorten, E.; Vercauteren, T.; Stoyanov, D. Deep Sequential Mosaicking of Fetoscopic Videos. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 311–319. [Google Scholar]
- Bano, S.; Vasconcelos, F.; Tella-Amo, M.; Dwyer, G.; Gruijthuijsen, C.; Vander Poorten, E.; Vercauteren, T.; Ourselin, S.; Deprest, J.; Stoyanov, D. Deep learning-based fetoscopic mosaicking for field-of-view expansion. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 1807–1816. [Google Scholar] [CrossRef]
- Li, L.; Bano, S.; Deprest, J.; David, A.L.; Stoyanov, D.; Vasconcelos, F. Globally Optimal Fetoscopic Mosaicking Based on Pose Graph Optimisation With Affine Constraints. IEEE Robot. Autom. Lett. 2021, 6, 7831–7838. [Google Scholar] [CrossRef]
- Aruna, K.; Anil, V.S.; Anand, A.; Jaysankar, A.; Venugopal, A.; Nisha, K.; Sreelekha, G. Image Mosaicing for Neonatal Fundus Images. In Proceedings of the 2021 8th International Conference on Smart Computing and Communications (ICSCC), Kochi, Kerala, 1–3 July 2021; pp. 100–105. [Google Scholar]
- Brown, M.; Lowe, D.G. Automatic panoramic image stitching using invariant features. Int. J. Comput. Vis. 2007, 74, 59–73. [Google Scholar] [CrossRef] [Green Version]
- Lowe, D.G. Distinctive image features from scale-invariant keypoints. Int. J. Comput. Vis. 2004, 60, 91–110. [Google Scholar] [CrossRef]
- Bay, H.; Tuytelaars, T.; Van Gool, L. Surf: Speeded up Robust Features. In Proceedings of the European Conference on Computer Vision, Graz, Austria, 7–13 May 2006; Springer: Berlin/Heidelberg, Germany, 2006; pp. 404–417. [Google Scholar]
- Kwatra, V.; Schödl, A.; Essa, I.; Turk, G.; Bobick, A. Graphcut textures: Image and video synthesis using graph cuts. ACM Trans. Graph. 2003, 22, 277–286. [Google Scholar] [CrossRef]
- Burt, P.J.; Adelson, E.H. A multiresolution spline with application to image mosaics. ACM Trans. Graph. 1983, 2, 217–236. [Google Scholar] [CrossRef]
- Zaragoza, J.; Chin, T.J.; Brown, M.S.; Suter, D. As-Projective-as-Possible Image Stitching with Moving DLT. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Portland, OR, USA, 23–28 June 2013; pp. 2339–2346. [Google Scholar]
- Zhang, F.; Liu, F. Parallax-Tolerant Image Stitching. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 3262–3269. [Google Scholar]
- Lin, C.C.; Pankanti, S.U.; Natesan Ramamurthy, K.; Aravkin, A.Y. Adaptive as-Natural-as-Possible Image Stitching. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1155–1163. [Google Scholar]
- Chen, Y.S.; Chuang, Y.Y. Natural Image Stitching with the Global Similarity Prior. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 11–14 October 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 186–201. [Google Scholar]
- Li, J.; Wang, Z.; Lai, S.; Zhai, Y.; Zhang, M. Parallax-tolerant image stitching based on robust elastic warping. IEEE Trans. Multimed. 2017, 20, 1672–1687. [Google Scholar] [CrossRef]
- Liu, F.; Gleicher, M.; Jin, H.; Agarwala, A. Content-preserving warps for 3D video stabilization. ACM Trans. Graph. 2009, 28, 1–9. [Google Scholar]
- Perazzi, F.; Sorkine-Hornung, A.; Zimmer, H.; Kaufmann, P.; Wang, O.; Watson, S.; Gross, M. Panoramic Video from Unstructured Camera Arrays. In Computer Graphics Forum; Wiley Online Library: Hoboken, HJ, USA, 2015; Volume 34, pp. 57–68. [Google Scholar]
- Zhao, Q.; Ma, Y.; Zhu, C.; Yao, C.; Feng, B.; Dai, F. Image stitching via deep homography estimation. Neurocomputing 2021, 450, 219–229. [Google Scholar] [CrossRef]
- Nguyen, T.; Chen, S.W.; Shivakumar, S.S.; Taylor, C.J.; Kumar, V. Unsupervised deep homography: A fast and robust homography estimation model. IEEE Robot. Autom. Lett. 2018, 3, 2346–2353. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, C.; Liu, S.; Jia, L.; Ye, N.; Wang, J.; Zhou, J.; Sun, J. Content-Aware Unsupervised Deep Homography Estimation. In Proceedings of the European Conference on Computer Vision, Glasgow, UK, 23–28 August 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 653–669. [Google Scholar]
- Shen, C.; Ji, X.; Miao, C. Real-Time Image Stitching with Convolutional Neural Networks. In Proceedings of the 2019 IEEE International Conference on Real-time Computing and Robotics (RCAR), Irkutsk, Russia, 4–9 August 2019; pp. 192–197. [Google Scholar]
- Lai, W.S.; Gallo, O.; Gu, J.; Sun, D.; Yang, M.H.; Kautz, J. Video Stitching for Linear Camera Arrays. arXiv 2019, arXiv:1907.13622. [Google Scholar]
- Song, D.Y.; Um, G.M.; Lee, H.K.; Cho, D. End-to-End Image Stitching Network via Multi-Homography Estimation. IEEE Signal Process. Lett. 2021, 28, 763–767. [Google Scholar] [CrossRef]
- Nie, L.; Lin, C.; Liao, K.; Liu, S.; Zhao, Y. Unsupervised deep image stitching: Reconstructing stitched features to images. IEEE Trans. Image Process. 2021, 30, 6184–6197. [Google Scholar] [CrossRef]
- Fouard, C.; Deram, A.; Keraval, Y.; Promayon, E. CamiTK: A Modular Framework Integrating Visualization, Image Processing and Biomechanical Modeling. In Soft Tissue Biomechanical Modeling for Computer Assisted Surgery; Payan, Y., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 323–354. [Google Scholar]
- Zhu, Z.; Lu, J.; Wang, M.; Zhang, S.; Martin, R.R.; Liu, H.; Hu, S.M. A comparative study of algorithms for realtime panoramic video blending. IEEE Trans. Image Process. 2018, 27, 2952–2965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Kim, S.J.; Brown, M.S. Constructing Image Panoramas Using Dual-Homography Warping. In Proceedings of the CVPR 2011, Colorado Springs, CO, USA, 20–25 June 2011; pp. 49–56. [Google Scholar]
- Cartucho, J.; Tukra, S.; Li, Y.S.; Elson, D.; Giannarou, S. VisionBlender: A tool to efficiently generate computer vision datasets for robotic surgery. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2021, 9, 331–338. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Basic | Graph Cuts-Based | Mesh-Based Models | Non-Mesh-Based Models | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Method | Global Homograpĥy [16] | Graphcut | APAP [21] | PTIS [22] | ANAP [23] | NIS [24] | REW [25] | Perazzi [27] | UDIS [34] |
| Alignment over an/along a … | Overlap region | Seam | Overlap region | Seam | Overlap region | Overlap region | Overlap region | Overlap region | Seam and overlap region |
| Features | SIFT | SIFT | SIFT | SIFT | SIFT | Grid keypoints derived from APAP [21] | SURF | Optical flow | CNN-based |
| Method | Global homography | • Global homography [16] • Graph cuts [19] | • Grid with local homo- graphies • Extrapolation outside of the over- lapping area | Iterative process: • Find a locally coherent homography • Estimate the alignment quality • Refine the alignment using CPW | • Grid with local homo- graphies • Smooth combination of homography and global similarity | Grid with local warp using CPW | • Elastic warp • Grid model to speed up computations | • Pre-alignment with global homography [16] • Optical flow alignment in the overlapping areas • Extrapolation in non-overlapping areas | • Unsupervised global homography estimation • Alignment refi- nement with reconstruction networks, perceptual losses and L1 loss along the seams |
| Similarity guidance | No | No | No | Yes | Yes | Yes | Yes | No | No |
| Content-Preserving Warp (CPW) | No | No | No | Yes | No | Yes | Yes | No | N/A |
| Advantages | • Real time | • Fast • May handle some parallax issues | • Better alignment accu- racy compared to global homography [16] • Solves medium parallax issues | • Combines advantages of seam-based methods and mesh-based methods • May handle important parallax issues | • Fewer projective distor- tions than APAP [21] | • Distortions are globally minimised • Better estimation of the global similarity trans- form compared to ANAP [23] • More natural-looking | • Fast • Minimised distortions | • Adapted to video • Does not rely on keypoints only | • Completely un- supervised • Limited GPU memory requirement • 2 fps |
| Drawbacks | • Not robust to parallax at all (blur, projective distor- tions, duplicated elements) | • Fails on some large parallax issues (discontinuity, projective distortions) | • Projective distortions in non-overlapping areas • Does not handle important parallax issues | • Randomness in the search for optimal homography | • Local distortions when the number of images increases • Non-robust estimation of the global similarity trans- formation (unnatural rotation or scaling) | • Computationally expen- sive | • Fails on important parallax issues | • Bottleneck of optical flow computation | • Do not address the projective distortions. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guy, S.; Haberbusch, J.-L.; Promayon, E.; Mancini, S.; Voros, S. Qualitative Comparison of Image Stitching Algorithms for Multi-Camera Systems in Laparoscopy. J. Imaging 2022, 8, 52. https://doi.org/10.3390/jimaging8030052
Guy S, Haberbusch J-L, Promayon E, Mancini S, Voros S. Qualitative Comparison of Image Stitching Algorithms for Multi-Camera Systems in Laparoscopy. Journal of Imaging. 2022; 8(3):52. https://doi.org/10.3390/jimaging8030052
Chicago/Turabian StyleGuy, Sylvain, Jean-Loup Haberbusch, Emmanuel Promayon, Stéphane Mancini, and Sandrine Voros. 2022. "Qualitative Comparison of Image Stitching Algorithms for Multi-Camera Systems in Laparoscopy" Journal of Imaging 8, no. 3: 52. https://doi.org/10.3390/jimaging8030052
APA StyleGuy, S., Haberbusch, J.-L., Promayon, E., Mancini, S., & Voros, S. (2022). Qualitative Comparison of Image Stitching Algorithms for Multi-Camera Systems in Laparoscopy. Journal of Imaging, 8(3), 52. https://doi.org/10.3390/jimaging8030052