
Determination of the Round Window Niche Anatomy Using Cone Beam Computed Tomography Imaging as Preparatory Work for Individualized Drug-Releasing Implants

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alzamil, K.S.; Linthicum, F.H. Extraneous Round Window Membranes And Plugs: Possible Effect On Intratympanic Therapy. Ann. Owl. Rhinol. Laryngol. 2000, 109. [Google Scholar] [CrossRef]
- Boenninghaus, H.-G.; Lenarz, T. Hals-Nasen- Ohren-Heilkunde; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Bird, P.A.; Begg, E.J.; Zhang, M.; Keast, A.T.; Murray, D.P.; Balkany, T.J. Intratympanic Versus Intravenous Delivery of Methylprednisolone to Cochlear Perilymph. Otol. Neurotol. 2007, 28, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Patel, M. Intratympanic corticosteroids in Ménière‘s disease: A mini-review. J. Otol. 2017, 117–124. [Google Scholar] [CrossRef]
- Plontke, S.K.; Glien, A.; Rahne, T.; Mader, K.; Salt, A.N. Controlled release dexamethasone implants in the round window niche for salvage treatment of idiopathic sudden sensorineural hearing loss. Otol. Neurotol. 2014, 35, 1168–1171. [Google Scholar] [CrossRef]
- McCall, A.A.; Swan, E.E.L.; Borenstein, J.T.; Sewell, W.F.; Kujawa, S.G.; McKenna, M.J. Drug Delivery for Treatment of Inner Ear Disease: Current State of Knowledge. Ear Hear. 2010, 31, 156–165. [Google Scholar] [CrossRef]
- Schwab, B.; Lenarz, T.; Heermann, R. Use of the round window micro cath for inner ear therapy—Results of a placebo-controlled, prospective study on chronic tinnitus. Laryngorhinootologie 2004, 83, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Schoendorf, J.; Neugebauer, P.; Michel, O. Continuous Intratympanic Infusion of Gentamicin Via a Microcatheter in Menière’s Disease. Otolaryngol. Head Neck Surg. 2016, 124, 203–207. [Google Scholar] [CrossRef]
- Seidman, M. Continuous Gentamicin Therapy Using an IntraEAR Microcatheter for Meniere’s Disease: A Retrospective Study. Otolaryngol. Head Neck Surg. 2016, 126, 244–256. [Google Scholar] [CrossRef] [PubMed]
- She, W.; Dai, Y.; Du, X.; Yu, C.; Chen, F.; Wang, J.; Qin, X. Hearing evaluation of intratympanic methylprednisolone perfusion for refractory sudden sensorineural hearing loss. Otolaryngol. Head Neck Surg. 2010, 142, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Paulson, D.P.; Abuzeid, W.; Jiang, H.; Oe, T.; O’Malley, B.W.; Li, D. A novel controlled local drug delivery system for inner ear disease. Laryngoscope 2008, 118, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Borden, R.C.; Saunders, J.E.; Berryhill, W.E.; Krempl, G.A.; Thompson, D.M.; Queimado, L. Hyaluronic acid hydrogel sustains the delivery of dexamethasone across the round window membrane. Audiol. Neurootol. 2011, 16, 1–11. [Google Scholar] [CrossRef]
- Luo, J.; Xu, L. Distribution of gentamicin in inner ear after local administration via a chitosan glycerophosphate hydrogel delivery system. Ann. Otol. Rhinol. Laryngol. 2012, 121, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Rathnam, C.; Chueng, S.-T.D.; Ying, Y.-L.M.; Lee, K.-B.; Kwan, K. Development in Bio-Inspired Nanomaterials for Therapeutic Delivery to Treat Hearing Loss. Front. Cell. Neurosci. 2019, 13. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Matin, F.; Weber, C.; John, S.; Lenarz, T.; Scheper, V. High Variability of Postsurgical Anatomy Supports the Need for Individualized Drug-Eluting Implants to Treat Chronic Rhinosinusitis. Life 2020, 10, 353. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Schurzig, D.; Timm, M.E.; Batsoulis, C.; Salcher, R.; Sieber, D.; Jolly, C.; Lenarz, T.; Zoka-Assadi, M. A Novel Method for Clinical Cochlear Duct Length Estimation toward Patient-Specific Cochlear Implant Selection. OTO Open 2018, 2, 2473974X18800238. [Google Scholar] [CrossRef]
- Verbist, B.M.; Skinner, M.W.; Cohen, L.T.; Leake, P.A.; James, C.; Boëx, C.; Holden, T.A.; Finley, C.C.; Roland, P.S.; Roland, J.T.; et al. Consensus Panel on a Cochlear Coordinate System Applicable in Histologic, Physiologic, and Radiologic Studies of the Human Cochlea. Otol. Neurotol. 2010, 31, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Crane, B.T.; Minor, L.B.; Della Santina, C.C.; Carey, J.P. Middle Ear Exploration in Patients With Ménière’s Disease Who Have Failed Outpatient Intratympanic Gentamicin Therapy. Otol. Neurotol. 2009, 30, 619–624. [Google Scholar] [CrossRef]
- Bowe, S.N.; Jacob, A. Round window perfusion dynamics: Implications for intracochlear therapy. Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 377–385. [Google Scholar] [CrossRef]
- Silverstein, H.; Rowan, P.T.; Olds, M.J.; Rosenberg, S.I. Inner ear perfusion and the role of round window patency. Am. J. Otol. 1997, 5, 586–589. [Google Scholar]
- Rossberg, W.; Goetz, F.; Timm, M.E.; Lenarz, T.; Helmstaedter, V. Intratympanic application of triamcinolone in sudden hearing loss-radiologic anatomy in cone beam CT and its’ correlation to clinical outcome. Eur. Arch. Otorhinolaryngol. 2020, 277, 1931–1937. [Google Scholar] [CrossRef]
- Proctor, B.; Bollobas, B.; Niparko, J.K. Anatomy of the round window niche. Ann. Otol. Rhinol. Laryngol. 1986, 95, 444–446. [Google Scholar] [CrossRef] [PubMed]
- Bollobas, B. A Halloszerv Microchirurgiai Anutomiaja; Medicina Könyvkiado: Budapest, Hungary, 1972. [Google Scholar]
- Li, P.M.; Wang, H.; Northrop, C.; Merchant, S.N.; Nadol, J.B., Jr. Anatomy of the round window and hook region of the cochlea with implications for cochlear implantation and other endocochlear surgical procedures. Otol. Neurotol. 2007, 28, 641–648. [Google Scholar] [CrossRef]
- Leong, A.C.; Jiang, D.; Agger, A.; Fitzgerald-O’Connor, A. Evaluation of round window accessibility to cochlear implant insertion. Eur. Arch. Otorhinolaryngol. 2012, 270, 1237–1242. [Google Scholar] [CrossRef]
- Atturo, F.; Barbara, M.; Rask-Andersen, H. Is the human round window really round? An anatomic study with surgical implications. Otol. Neurotol. 2014, 35, 1354–1360. [Google Scholar] [CrossRef]
- Singla, A.; Sahni, D.; Gupta, A.K.; Loukas, M.; Aggarwal, A. Surgical anatomy of round window and its implications for cochlear implantation. Clin. Anat. 2014, 27, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Gaurkar, S.; Deshmukh, P.T.; Khatri, M.; Kalambe, S.; Lakhotia, P.; Chandravanshi, D.; Disawal, A. Applied anatomy of round window and adjacent structures of tympanum related to cochlear implantation. Braz. J. Otorhinolaryngol. 2019, 85, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Cornwall, H.L.; Marway, P.S.; Bance, M. A Micro-Computed Tomography Study of Round Window Anatomy and Implications for Atraumatic Cochlear Implant Insertion. Otol. Neurotol. 2021, 42, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Avato, I.; Manfrin, M.; Simoncelli, A.M.; Magnetto, M.; Rebecchi, E.; Tinelli, C.; Neri, M.; Beltrame, M.A.; Benazzo, M. Anatomic variations of the round window niche: Radiological study and related endoscopic anatomy. Surg. Radiol. Anat. 2019, 41, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Takagi, A.; Sando, I. Computer-aided three-dimensional reconstruction and measurement of the round window and its membrane. Otolaryngol. Head Neck Surg. 1989, 101, 517–521. [Google Scholar] [CrossRef]
- Labadie, R.F.; Noble, J.H. Preliminary Results With Image-guided Cochlear Implant Insertion Techniques. Otol. Neurotol. 2018, 39, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Jamroz, W.; Szafraniec, J.; Kurek, M.; Jachowicz, R. 3D Printing in Pharmaceutical and Medical Applications—Recent Achievements and Challenges. Pharm Res. 2018, 35, 176. [Google Scholar] [CrossRef] [PubMed]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
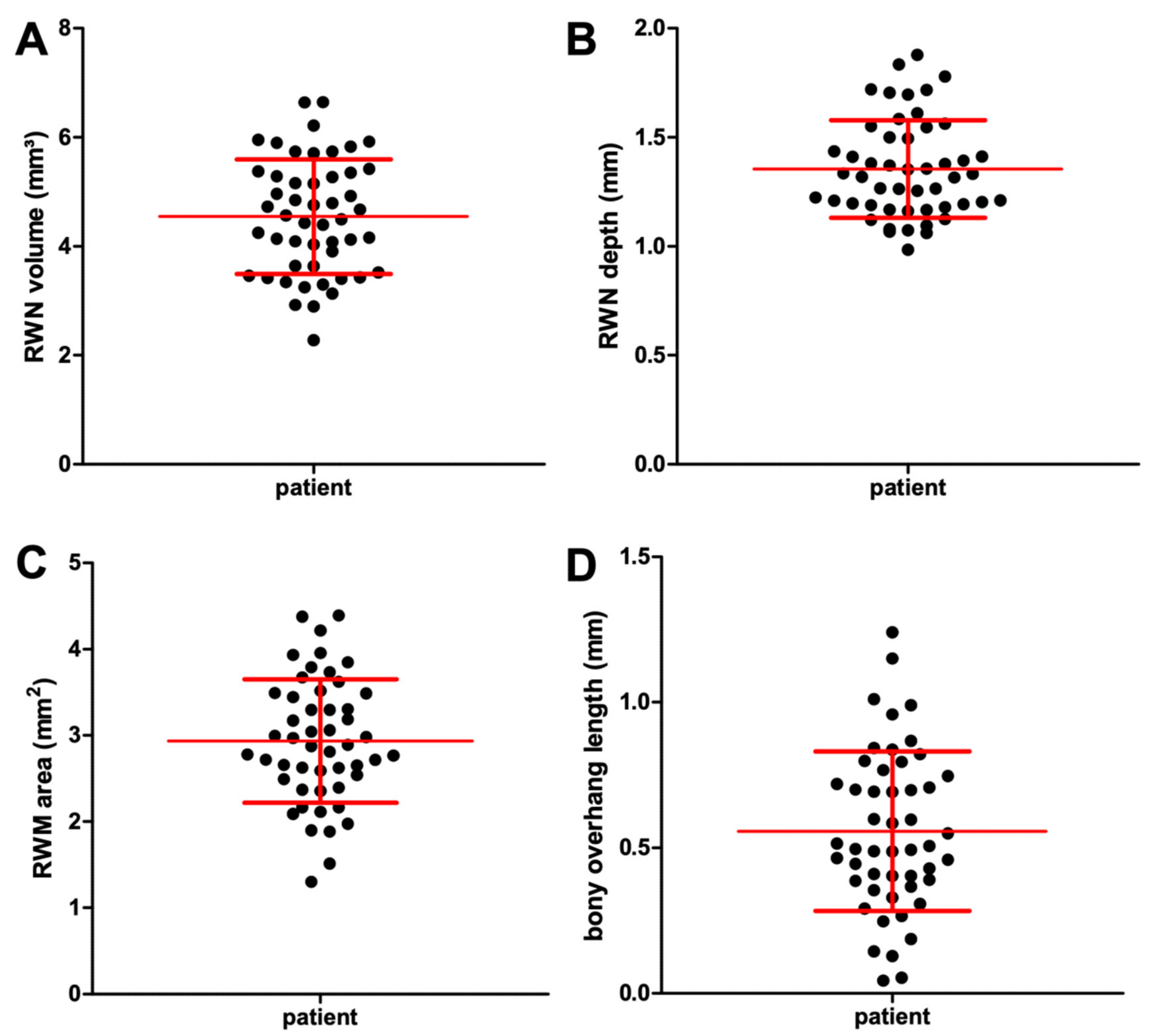
| Mean | Min | Max | Std | |
|---|---|---|---|---|
| Vol | 4.54 | 2.28 | 6.64 | 1.05 |
| A | 2.93 | 1.30 | 4.39 | 0.72 |
| oh | 0.56 | 0.04 | 1.24 | 0.27 |
| d | 1.35 | 0.98 | 1.88 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matin, F.; Gao, Z.; Repp, F.; John, S.; Lenarz, T.; Scheper, V. Determination of the Round Window Niche Anatomy Using Cone Beam Computed Tomography Imaging as Preparatory Work for Individualized Drug-Releasing Implants. J. Imaging 2021, 7, 79. https://doi.org/10.3390/jimaging7050079
Matin F, Gao Z, Repp F, John S, Lenarz T, Scheper V. Determination of the Round Window Niche Anatomy Using Cone Beam Computed Tomography Imaging as Preparatory Work for Individualized Drug-Releasing Implants. Journal of Imaging. 2021; 7(5):79. https://doi.org/10.3390/jimaging7050079
Chicago/Turabian StyleMatin, Farnaz, Ziwen Gao, Felix Repp, Samuel John, Thomas Lenarz, and Verena Scheper. 2021. "Determination of the Round Window Niche Anatomy Using Cone Beam Computed Tomography Imaging as Preparatory Work for Individualized Drug-Releasing Implants" Journal of Imaging 7, no. 5: 79. https://doi.org/10.3390/jimaging7050079
APA StyleMatin, F., Gao, Z., Repp, F., John, S., Lenarz, T., & Scheper, V. (2021). Determination of the Round Window Niche Anatomy Using Cone Beam Computed Tomography Imaging as Preparatory Work for Individualized Drug-Releasing Implants. Journal of Imaging, 7(5), 79. https://doi.org/10.3390/jimaging7050079