
The First Case of Fusarium falciforme Eumycetoma in Sudan and an Extensive Literature Review about Treatment Worldwide

 , , and
, , and 
Abstract
1. Introduction
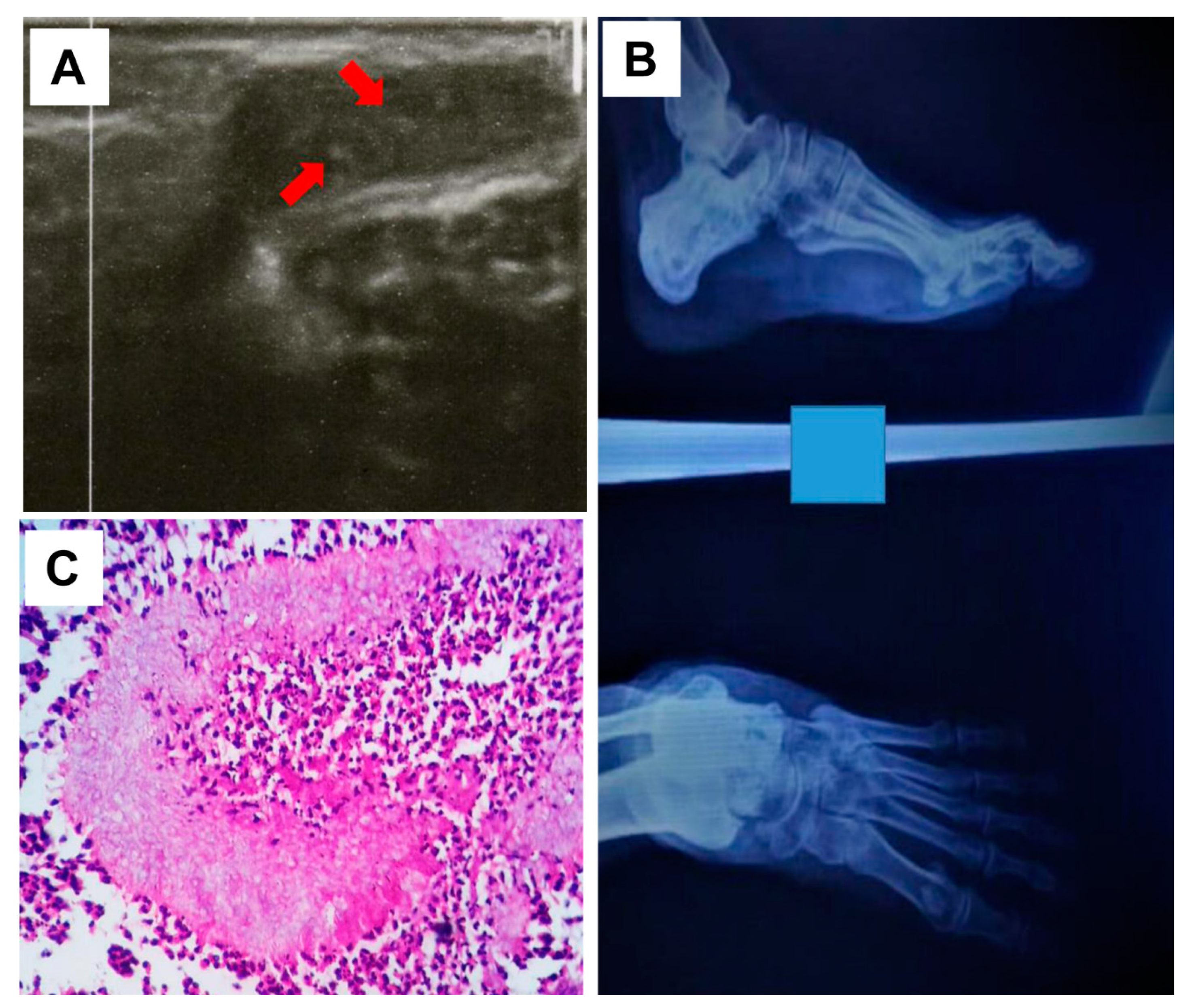
2. Case Report
3. Literature Review to Improve Our Case Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siddig, E.E.; Ahmed, A.; Ali, Y.; Bakhiet, S.M.; Mohamed, N.S.; Ahmed, E.S.; Fahal, A.H. Eumycetoma Medical Treatment: Past, Current Practice, Latest Advances and Perspectives. Microbiol. Res. 2021, 12, 899–906. [Google Scholar] [CrossRef]
- Siddig, E.E.; Mhmoud, N.A.; Bakhiet, S.M.; Abdallah, O.B.; Mekki, S.O.; El Dawi, N.I.; Van de Sande, W.; Fahal, A.H. The Accuracy of Histopathological and Cytopathological Techniques in the Identification of the Mycetoma Causative Agents. PLoS Negl. Trop. Dis. 2019, 13, e0007056. [Google Scholar] [CrossRef] [PubMed]
- van de Sande, W.W. Global burden of human mycetoma: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2013, 7, e2550. [Google Scholar] [CrossRef] [PubMed]
- Siddig, E.E.; Ahmed, A.; Hassan, O.B.; Bakhiet, S.M.; Verbon, A.; Fahal, A.H.; van de Sande, W.W.J. Using a Madurella mycetomatis-specific PCR on grains obtained via non-invasive fine-needle aspirated material is more accurate than cytology. Mycoses 2023, 66, 477–482. [Google Scholar] [CrossRef]
- Nucci, M.; Anaissie, E. Cutaneous infection by Fusarium species in healthy and immunocompromised hosts: Implications for diagnosis and management. Clin. Infect. Dis. 2002, 35, 909–920. [Google Scholar] [CrossRef]
- Venugopal, P.V.; Venugopal, T.V. Pale grain eumycetomas in Madras. Australas. J. Dermatol. 1995, 36, 149–151. [Google Scholar] [CrossRef]
- Lim, W.; Siddig, E.; Eadie, K.; Nyuykonge, B.; Ahmed, S.; Fahal, A.; Verbon, A.; Smit, S.; Van De Sande, W.W. The development of a novel diagnostic PCR for Madurella mycetomatis using a comparative genome approach. PLoS Negl. Trop. Dis. 2020, 14, e0008897. [Google Scholar] [CrossRef]
- Siddig, E.E.; Verbon, A.; Bakhiet, S.; Fahal, A.H.; van de Sande, W.W. The developed molecular biological identification tools for mycetoma causative agents: An update. Acta Trop. 2022, 225, 106205. [Google Scholar] [CrossRef]
- Mariat, F. Sur la distribution ge´ographique et la re´partition des agents de myce´tomes. Bull. Soc. Pathol. Exot. 1963, 56, 35–45. [Google Scholar]
- Gamet, A.; Brottes, H.; Essomba, R. Nouveaux cas de mycétomes dépistés au Cameroun [New cases of mycetoma detected in Cameroun]. Bull. Soc. Pathol. Exot. Filiales. 1964, 57, 1191–1195. [Google Scholar]
- Peloux, Y.; Segretain, G. Myce´tomes a` Fusarium. Bull. Soc. Fr. Mycol. Med. 1966, 1, 31–32. [Google Scholar]
- Destombes, P.; Mariat, F.; Rosati, L.; Segretain, G. Les mycétomes en Somalie—Conclusions d′une enquête menée de 1959 à 1964 [Mycetoma in Somalia—Results of a survey done from 1959 to 1964]. Acta Trop. 1977, 34, 355–373. [Google Scholar] [PubMed]
- Hay, R.J.; Mackenzie, D.W. The histopathological features of pale grain eumycetoma. Trans. R. Soc. Trop. Med. Hyg. 1982, 76, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.J.; Mackenzie, D.W. Mycetoma (madura foot) in the United Kingdom—A survey of forty-four cases. Clin. Exp. Dermatol. 1983, 8, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Thianprasit, M.; Sivayathorn, A. Black dot mycetoma. Mykosen 1984, 27, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ajello, L.; Padhye, A.; Chandler, F.; McGinnis, M.; Morganti, L.; Alberici, F. Fusarium moniliforme, a new mycetoma agent. Restudy of a European case. Eur. J. Epidemiol. 1985, 1, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Baudraz-Rosselet, F.; Monod, M.; Borradori, L.; Ginalsky, J.; Vion, B.; Boccard, C.; Frenk, E. Mycetoma of the foot due to Fusarium sp. treated with oral ketoconazole. Dermatology 1992, 184, 303–305. [Google Scholar] [CrossRef]
- Buiting, A.G.; Visser, L.G.; Barge, R.M.; van’t Wout, J.W. Mycetoom van de voet; een ziekte uit de tropen [Mycetoma of the foot; a disease from the tropics]. Ned. Tijdschr. Geneeskd. 1993, 137, 1513–1515. [Google Scholar]
- de Hoog, G.S.; Buiting, A.; Tan, C.S.; Stroebel, A.B.; Ketterings, C.; de Boer, E.J.; Naafs, B.; Brimicombe, R.; Nohlmans-Paulssen, M.K.; Fabius, G.T.; et al. Diagnostic problems with imported cases of mycetoma in The Netherlands. Mycoses 1993, 36, 81–87. [Google Scholar] [CrossRef]
- Tomimori-Yamashita, J.; Ogawa, M.M.; Hirata, S.H.; Fischman, O.; Michalany, N.S.; Yamashita, H.K.; Alchorne, M.M. Mycetoma caused by Fusarium solani with osteolytic lesions on the hand: Case report. Mycopathologia 2002, 153, 11–14. [Google Scholar] [CrossRef]
- Yera, H.; Bougnoux, M.E.; Jeanrot, C.; Baixench, M.T.; De Pinieux, G.; Dupouy-Camet, J. Mycetoma of the foot caused by Fusarium solani: Identification of the etiologic agent by DNA sequencing. J. Clin. Microbiol. 2003, 41, 1805–1808. [Google Scholar] [CrossRef] [PubMed]
- Palmore, T.N.; Shea, Y.R.; Childs, R.W.; Sherry, R.M.; Walsh, T.J. Fusarium proliferatum soft tissue infection at the site of a puncture by a plant: Recovery, isolation, and direct molecular identification. J. Clin. Microbiol. 2010, 48, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Dutta, P.; Premkumar, A.; Chakrabarti, A.; Shah, V.N.; Behera, A.; De, D.; Rudramurthy, S.M.; Bhansali, A. Fusarium falciforme infection of foot in a patient with type 2 diabetes mellitus: A case report and review of the literature. Mycopathologia 2013, 176, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Al-Hatmi, A.M.; Bonifaz, A.; Tirado-Sánchez, A.; Meis, J.F.; de Hoog, G.S.; Ahmed, S.A. Fusarium species causing eumycetoma: Report of two cases and comprehensive review of the literature. Mycoses 2017, 60, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Katkar, V.J.; Tankhiwale, S.S.; Kurhade, A. Fusarium soloni mycetoma. Indian. J. Dermatol. 2011, 56, 315–317. [Google Scholar] [PubMed]
- Campos-Macías, P.; Arenas-Guzmán, R.; Hernández-Hernández, F. Fusarium subglutinans: A new eumycetoma agent. Med. Mycol. Case Rep. 2013, 2, 128–131. [Google Scholar] [CrossRef]
- Nakar, C.; Livny, G.; Levy, I.; Samra, Z.; Linder, N.; Ashkenazi, S.; Livne, P.; Sirota, L.; Tikva, P. Mycetoma of the renal pelvis caused by Fusarium species. Pediatr. Infect. Dis. J. 2001, 20, 1182–1183. [Google Scholar] [CrossRef] [PubMed]
- Klokke, A.H. Mycetoma of the foot, a disease from the tropics. Ned. Tijdschr. Geneeskd. 1993, 137, 2056–2057. [Google Scholar]
- Prinja, A.; Roberts, C.; Doherty, T.; Oddy, M.J. An unusual cause of an ankle mass. BMJ Case Rep. 2014, 2014, bcr2014204253. [Google Scholar] [CrossRef]
- Xiujiao, X.; Hong, S.; Ai-e, X. Eumycetoma due to Acremonium falciforme acquired in China. Mycoses 2012, 55, e4–e7. [Google Scholar] [CrossRef]
- Van Etta, L.L.; Peterson, L.R.; Gerding, D.N. Acremonium falciforme (Cephalosporium falciforme) mycetoma in a renal transplant patient. Arch. Dermatol. 1983, 119, 707–708. [Google Scholar] [CrossRef] [PubMed]
- Kudur, M.H.; Prakash, P.; Savitha, M. Fusarium solani causing quasi-invasive infection of the foot in an immunocompetent middle-aged man from South India. Indian. J. Dermatol. 2013, 58, 241. [Google Scholar] [CrossRef] [PubMed]
- Mercuţ, D.; Tiţa, C.; Ianoşi, G.; Ianoşi, S.; Tiţa, M. Piciorul de Madura (micetomul) [Madura’s foot (mycetoma)]. Chirurgia 2003, 98, 261–264. [Google Scholar] [PubMed]
- Resnik, B.I.; Burdick, A.E. Improvement of eumycetoma with itraconazole. J. Am. Acad. Dermatol. 1995, 33 Pt 2, 917–919. [Google Scholar] [CrossRef] [PubMed]
- Luque, A.G.; Mujica, M.T.; D’anna, M.L.; Alvarez, D.P. Micetoma podal por fusarium solani (Mart.) Appel & Wollenweber. Boletín Micológico 1991, 6, 1–2. [Google Scholar]
- Destombes, P.; Mariat, F.; Rosati, L.; Segretain, G. Les mycétomes en République de Somalie [Mycetomas in the Republic of Somalia]. C. R. Acad. Hebd. Seances Acad. Sci. D 1966, 263, 2062–2064. [Google Scholar]
- Callebaut, G.; Hooghe, L.; Dratwa, M. Madura′s foot in a renal transplant patient: Report of a case. NDT Plus 2011, 4, 397–398. [Google Scholar] [CrossRef]
- Salas-Coronas, J.; Cabezas-Fernández, T.; Martínez-Lage, M.J.; Villarejo-Ordóñez, A. Micetoma por Fusarium solani [Mycetoma caused by Fusarium solani]. Rev. Clin. Esp. 2011, 211, e16–e18. [Google Scholar] [CrossRef]
- Bonifaz, A.; Saldaña, M.; Araiza, J.; Mercadillo, P.; Tirado-Sánchez, A. Two simultaneous mycetomas caused by Fusarium verticillioides and Madurella mycetomatis. Rev. Inst. Med. Trop. Sao Paulo 2017, 59, e55. [Google Scholar] [CrossRef]
- Ahmed, A.; Mohamed, N.S.; Siddig, E.E.; Algaily, T.; Sulaiman, S.; Ali, Y. The impacts of climate change on displaced populations: A call for action. J. Clim. Chang. Health 2021, 3, 100057. [Google Scholar] [CrossRef]
- Das, L.; Dahiya, D.; Gupta, K.; Prakash, M.; Malhotra, B.; Rastogi, A.; Choudhary, H.; Rudramurthy, S.M.; Dutta, P. Eumycetoma of the Foot due to Fusarium solani in a Person with Diabetes Mellitus: Report of a Case and Review of Literature. Mycopathologia 2021, 186, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Batista, B.G.; De Chaves, M.A.; Reginatto, P.; Saraiva, O.J.; Fuentefria, A.M. Human fusariosis: An emerging infection that is difficult to treat. Rev. Soc. Bras. Med. Trop. 2020, 53, e20200013. [Google Scholar] [CrossRef] [PubMed]
- Martínez López, D.; Pérez Blasco, A.; García Ferrer, L.; Camarena, J.J.; González, R.; Rodrigo Perez, J.L. Eumicetomas por Fusarium oxysporum y Madurella mycetomatis. Descripción de dos casos y revisión de la bibliografía [Eumycetomas by Fusarium oxysporum and Madurella mycetomatis. Description of two cases and literature review]. Rev. Esp. Quimioter. 2022, 35, 566–569. [Google Scholar] [PubMed]
- Hashizume, H.; Taga, S.; Sakata, M.K.; Taha, M.H.M.; Siddig, E.E.; Minamoto, T.; Fahal, A.H.; Kaneko, S. Detection of multiple mycetoma pathogens using fungal metabarcoding analysis of soil DNA in an endemic area of Sudan. PLoS Negl. Trop. Dis. 2022, 16, e0010274. [Google Scholar] [CrossRef]
- Correia, C.; Ferreira, J.; Soares-de-Almeida, L.; Filipe, P. An Unusual Cause of Eumycetoma—Fusarium Solani Keratoplasticum. Actas Dermosifiliogr. 2022, 113, 899. [Google Scholar] [CrossRef] [PubMed]
- Al-Hatmi, A.M.S.; Curfs-Breuker, I.; De Hoog, G.S.; Meis, J.F.; Verweij, P.E. Antifungal Susceptibility Testing of Fusarium: A Practical Approach. J. Fungi 2017, 3, 19. [Google Scholar] [CrossRef]
- Da Rosa, P.D.; Ramirez-Castrillon, M.; Borges, R.; Aquino, V.; Fuentefria, A.M.; Goldani, L.Z. Epidemiological aspects and characterization of the resistance profile of Fusarium spp. in patients with invasive fusariosis. J. Med. Microbiol. 2019, 68, 1489–1496. [Google Scholar] [CrossRef]
- Ahmed, A.; Ali, Y.; Siddig, E.E.; Hamed, J.; Mohamed, N.S.; Khairy, A.; Zinsstag, J. Hepatitis E Virus Outbreak among Tigray War Refugees from Ethiopia, Sudan. Emerg. Infect. Dis. 2022, 28, 1722. [Google Scholar] [CrossRef]
- Ahmed, A.; Ali, Y.; Elmagboul, B.; Mohamed, O.; Elduma, A.; Bashab, H.; Mahamoud, A.; Khogali, H.; Elaagip, A.; Higazi, T. Dengue fever in the Darfur area, Western Sudan. Emerg. Infect. Dis. 2019, 25, 2125. [Google Scholar] [CrossRef]
- Ahmed, A.; Mahmoud, I.; Eldigail, M.; Elhassan, R.M.; Weaver, S.C. The emergence of Rift Valley Fever in gedaref state urges the need for a cross-border one health strategy and enforcement of the international health regulations. Pathogens 2021, 10, 885. [Google Scholar] [CrossRef]
- Paugh, K.R.; Del Castillo Múnera, J.; Swett, C.L. First Report of Fusarium falciforme (FSSC 3 + 4) Causing Rot of Industrial Hemp (Cannabis sativa) in California. Plant. Dis. 2022, 106, 1753. [Google Scholar] [CrossRef] [PubMed]
- Qiu, R.; Li, X.; Li, C.; Li, C.; Xue, C.; Fang, W.; Zhang, Y.; Song, R.; Xu, M.; He, L.; et al. First Report of Tobacco Root Rot Caused by Fusarium falciforme in China. Plant. Dis. 2022, 107, 960. [Google Scholar] [CrossRef] [PubMed]
- Velarde Felix, S.; Valenzuela, V.; Ortega, P.; Fierros, G.; Rojas, P.; López Orona, C.A.; Retes Manjarrez, J.E. First report of Fusarium falciforme (FSSC 3+4) causing root rot on chickpea in Mexico. Plant. Dis. 2021, 106, 329. [Google Scholar] [CrossRef]
- Sarwadnya, K.; Bhat, G.; Bangi, S.; Jeevitha, D.; Shivakumar, G.; Madalageri, B.B.; Noojibail, P.; Anandalakshmi, R. First report of Fusarium falciforme causing basal rot of onion (Allium cepa) in India. Plant. Dis. 2023, 107, 228. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Nájera, J.F.; Ayvar-Serna, S.; Mena-Bahena, A.; Baranda-Cruz, E.; Vargas-Hernández, M.; Alvarado-Gómez, O.G.; Fuentes-Aragón, D. First report of Fusarium falciforme (FSSC 3+4) causing wilt disease of Phaseolus vulgaris in Mexico. Plant. Dis. 2020, 105, 710. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.; Feng, C.; Liu, L.; Shi, R.; Han, S.; Song, Y.; Wang, J.; Han, Z.; Zhang, J.; Li, Y.; et al. First report of Fusarium falciforme causing root rot of soybean (Glycine max L.) in Henan, China. Plant Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento-Ramirez, J.M.; Abella-Perez, E.; Phillott, A.D.; Sim, J.; Van West, P.; Martin, M.P.; Marco, A.; Dieguez-Uribeondo, J. Global distribution of two fungal pathogens threatening endangered sea turtles. PLoS ONE 2014, 9, e85853. [Google Scholar] [CrossRef] [PubMed]
- Ali, Y.; Ahmed, A.; Siddig, E.E.; Mohamed, N.S. The role of integrated programs in the prevention of COVID-19 in a humanitarian setting. Trans. R. Soc. Trop. Med. Hyg. 2022, 116, 193–196. [Google Scholar] [CrossRef]
- Zinsstag, J.; Hediger, K.; Osman, Y.M.; Abukhattab, S.; Crump, L.; Kaiser-Grolimund, A.; Mauti, S.; Ahmed, A.; Hattendorf, J.; Bonfoh, B.; et al. The Promotion and Development of One Health at Swiss TPH and Its Greater Potential. Diseases 2022, 10, 65. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Hemaida, M.A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Sudden emergence and spread of cutaneous larva migrans in Sudan: A case series calls for urgent actions. IDCases 2023, 32, e01789. [Google Scholar] [CrossRef]
- Ahmed, A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Cutaneous tuberculosis of the foot clinically mimicking mycetoma: A case report. Clin. Case Rep. 2023, 11, e7295. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; El-Amin, R.; Musa, A.M.; Elsayed, M.A.; Fahal, L.A.; Ahmed, E.S.; Ali, Y.; Nebie, I.E.; Mohamed, N.S.; Zinsstag, J.; et al. Guillain-Barre syndrome associated with COVID-19 infection: A case series. Clin. Case Rep. 2023, 11, e6988. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Origin | Site | Duration in Years | Species | Treatment | Treatment Outcome | References |
|---|---|---|---|---|---|---|
| Cameroon | NA | NA | Fusarium sp. | NA | NA | [9] |
| Cameroon | Foot | NA | Fusarium sp. | Surgery | NA | [10] |
| Senegal | Foot | NA | Fusarium solani var. minus | NA | NA | [11] |
| Somalia | NA | NA | Fusarium sp. | NA | NA | [12] |
| NA | NA | NA | Fusarium solani | NA | NA | [13] |
| NA | NA | NA | F. oxysporum | NA | NA | [13] |
| Jamaica | NA | NA | Fusarium sp. | NA | NA | [14] |
| India | NA | NA | Fusarium sp. | NA | NA | [14] |
| Thailand | Ankle | NA | Fusarium solani var. coeruleum | Antibiotics | unsatisfactory | [15] |
| Italy | Foot and ankle | 5 | F. moniliforme | Antibacterial antibiotics | NA | [16] |
| Nigeria | Foot | 1 | Fusarium sp. | Ketoconazole | cured | [17] |
| Surinam | Foot | NA | Fusarium sp. | Surgery and itraconazole | NA | [18] |
| Surinam | Foot | 36 | F. solani | Itraconzaole | Improved | [19] |
| Brazil | Hand | 11 | F. solani | Ketoconazole | Lost follow-up | [20] |
| France | Foot | 3 | F. solani | Itraconazole (800 mg/day) | Cured | [21] |
| United State of America | Hand | NA | F. proliferatum | Voriconazole | cured | [22] |
| India | Foot | 0.5 | F. falciforme | Voriconazole | Cured | [23] |
| Mexico | Ankle | 2 | F. keratoplasticum | Itraconazole (400 mg/day) Terbinafine (250 mg/day) | Relapse Cured | [24] |
| Mexico | Foot | 3 | F. pseudensiforme | Itraconazole (400 mg/day) | Lost follow-up | [25] |
| India | Buttock | 4 | F. solani | NA | NA | [26] |
| Mexico | Foot | 8 | F. subglutinans | Itraconazole | Improved | [27] |
| NA | Renal pelvic | NA | Fusarium sp. | Amphotericin B + Flucytosine and surgery | Cured | [28] |
| Surinam | NA | 30 | Fusarium sp. | Itraconazole and surgery | NA | [29] |
| NA | Ankle | 7 | F. solani | Antifungal | Improved | [30] |
| China | Foot | 15 | F. falciforme | Terbinafine | Improved but relapsed after one year | [31] |
| United State of America | Hand and Forearm | 1 | F. falciforme | Amphotericin B and ketoconazole | Diseased | [32] |
| India | Both feet | 15 | F. solani | Itraconazole | Improved | [33] |
| Romania | Foot | 22 | Fusarium sp. | Ketoconazole, penicillin, and surgery | Amputated | [34] |
| Cuba | Foot | 18 | Fusarium sp. | Itraconazole | Improved | [35] |
| Argentina | Foot | NA | F. solani | NA | NA | [36] |
| Somalia | NA | NA | Fusarium sp. | NA | NA | [37] |
| Somalia | Foot | NA | Fusarium sp. | Surgery | Cured | [38] |
| Guinea Bissau | Forearm | 9 | F. solani | Itraconazole, amphotericin B, and surgery | NA | [39] |
| Mexico | Foot and leg | 8 | F. verticillioides | Itraconazole and dapsone | Lost follow-up | [40] |
| India | Foot | NA | F. solani | Voriconazole and surgery | Cured | [41] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siddig, E.E.; Ahmed, A.; Eltigani, H.F.; Bakhiet, S.M.; van de Sande, W.W.J.; Fahal, A.H. The First Case of Fusarium falciforme Eumycetoma in Sudan and an Extensive Literature Review about Treatment Worldwide. J. Fungi 2023, 9, 730. https://doi.org/10.3390/jof9070730
Siddig EE, Ahmed A, Eltigani HF, Bakhiet SM, van de Sande WWJ, Fahal AH. The First Case of Fusarium falciforme Eumycetoma in Sudan and an Extensive Literature Review about Treatment Worldwide. Journal of Fungi. 2023; 9(7):730. https://doi.org/10.3390/jof9070730
Chicago/Turabian StyleSiddig, Emmanuel Edwar, Ayman Ahmed, Hala Fathi Eltigani, Sahar Mubarak Bakhiet, Wendy W. J. van de Sande, and Ahmed Hassan Fahal. 2023. "The First Case of Fusarium falciforme Eumycetoma in Sudan and an Extensive Literature Review about Treatment Worldwide" Journal of Fungi 9, no. 7: 730. https://doi.org/10.3390/jof9070730
APA StyleSiddig, E. E., Ahmed, A., Eltigani, H. F., Bakhiet, S. M., van de Sande, W. W. J., & Fahal, A. H. (2023). The First Case of Fusarium falciforme Eumycetoma in Sudan and an Extensive Literature Review about Treatment Worldwide. Journal of Fungi, 9(7), 730. https://doi.org/10.3390/jof9070730