
Incidence of Chronic Pulmonary Aspergillosis in Patients with Suspected or Confirmed NTM and TB—A Population-Based Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
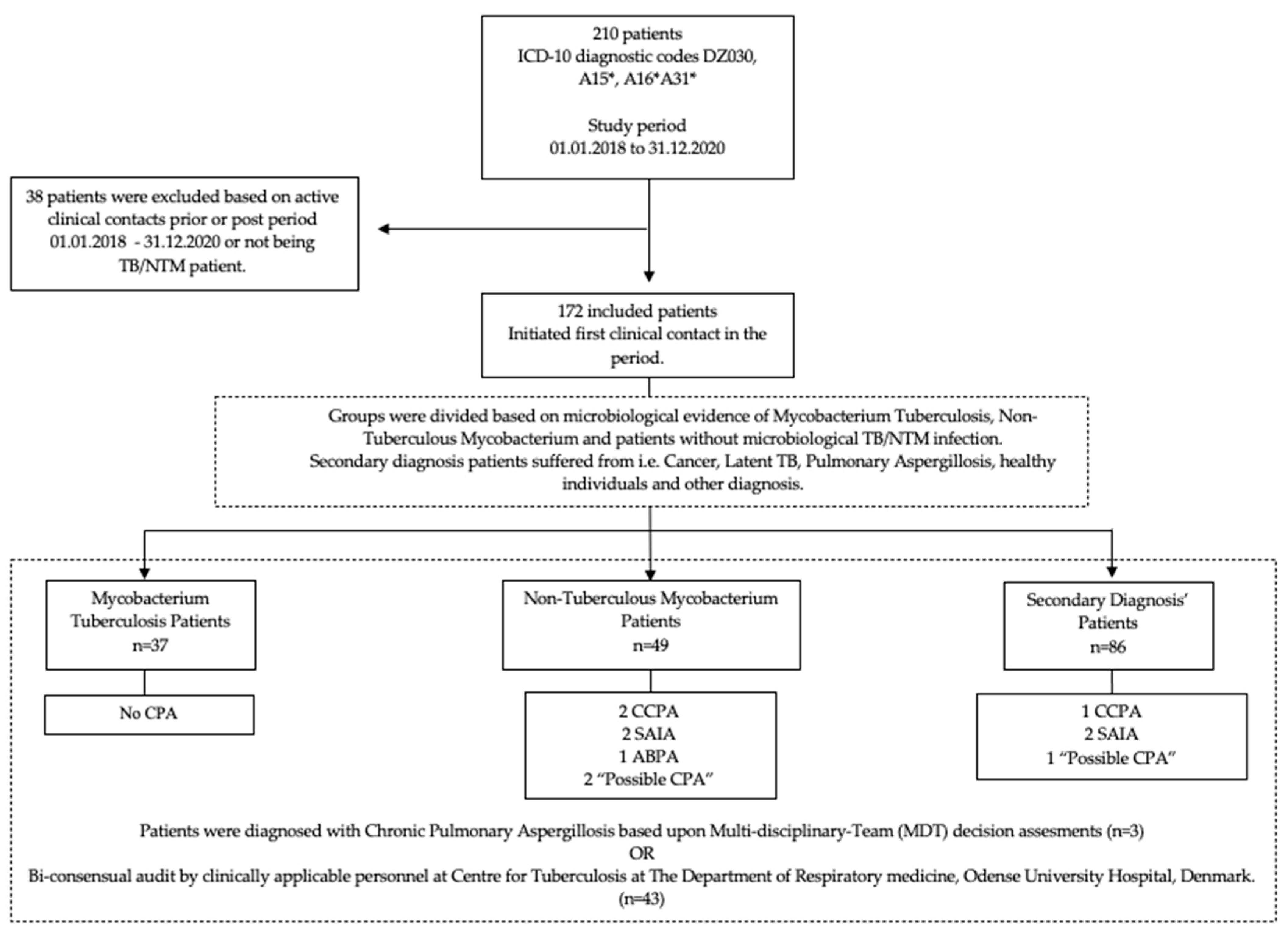
2.2. Participant Identification and Data Management
- A15*—Mycobacterium tuberculosis infections;
- A16*—Pulmonary mycobacterium tuberculosis;
- A31*—Non-tuberculous mycobacterium infection;
- Z030—Suspicion of tuberculosis.
2.3. Criteria of CPA and CPA Subtyping
- Pulmonary symptoms (i.e., cough, sputum, haemoptysis, dyspnoea) persistent for more than 3 months, with or without progression.
- One or more cavities or nodules characteristic of Aspergillus on radiological imaging, with or without progression.
- Direct or indirect serology evidence, such as Aspergillus serology indicative of a relevant immunological response and/or culture, microbiology, or pathological respiratory samples, characteristic of Aspergillus infection. Serology was assessed using Aspergillus fumigatus IgG and IgE (ImmunoCap, Phadia, Thermo Fischer Scientific, Sweden) with chosen cut-off values of IgG > 75 mg/L, Aspergillus fumigatus IgE > 0.35 × 103 IU/L, and total IgE > 115 × 103 IU/L.
2.4. Audit
2.5. Primary and Secondary Outcome Variables
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Generalisability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Page, I.D.; Byanyima, R.; Hosmane, S.; Onyachi, N.; Opira, C.; Richardson, M.; Sawyer, R.; Sharman, A.; Denning, D.W. Chronic Pulmonary Aspergillosis Commonly Complicates Treated Pulmonary Tuberculosis with Residual Cavitation. Eur. Respir. J. 2019, 53, 1801184. [Google Scholar] [CrossRef] [PubMed]
- Davidsen, J.R.; Rosenvinge, F.S.; Assing, K.; Laursen, C.B. Chronic pulmonary aspergillosis. Ugeskr. Laeg. 2018, 180, 257–270. [Google Scholar]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic Pulmonary Aspergillosis: Rationale and Clinical Guidelines for Diagnosis and Management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Predictors of Mortality in Chronic Pulmonary Aspergillosis. European Respiratory Society. Available online: https://erj.ersjournals.com/content/49/2/1601062.long (accessed on 22 July 2020).
- Medicine, T.L.R. Chronic Pulmonary Aspergillosis: Help Is on the Way. Lancet Respir. Med. 2016, 4, 83. [Google Scholar] [CrossRef]
- Mortensen, K.L.; Denning, D.W.; Arendrup, M.C. The Burden of Fungal Disease in Denmark. Mycoses 2015, 58 (Suppl. S5), 15–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laursen, C.B.; Davidsen, J.R.; Van Acker, L.; Salzer, H.J.F.; Seidel, D.; Cornely, O.A.; Hoenigl, M.; Alastruey-Izquierdo, A.; Hennequin, C.; Godet, C.; et al. CPAnet Registry—An International Chronic Pulmonary Aspergillosis Registry. J. Fungi 2020, 6, 96. [Google Scholar] [CrossRef] [PubMed]
- van Kampen, S.C.; Wanner, A.; Edwards, M.; Harries, A.D.; Kirenga, B.J.; Chakaya, J.; Jones, R. International Research and Guidelines on Post-Tuberculosis Chronic Lung Disorders: A Systematic Scoping Review. BMJ Glob. Health 2018, 3, e000745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, N.L.; Denning, D.W. Underlying Conditions in Chronic Pulmonary Aspergillosis Including Simple Aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global Burden of Chronic Pulmonary Aspergillosis as a Sequel to Pulmonary Tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef] [PubMed]
- Fløe, A.; Hilberg, O.; Seersholm, N.; Løkke, A.; Jensen, S.G. National Guidelines for the Treatment of Mycobacterium Tuberculosis. Available online: https://www.lungemedicin.dk/fagligt/75-tb-behandling.html#behandlingskontrol (accessed on 22 July 2020).
- Fløe, A.; Jensen, S.G.; Løkke, A.; Seersholm, N.; Hilberg, O. National Guidelines for the Diagnostics of Mycobacterium Tuberculosis. Available online: https://www.lungemedicin.dk/fagligt/76-diagnostik-af-tuberkulose.html#aetiologi (accessed on 22 July 2020).
- Meyer, C. National Guidelines for Diagnostics and Treatment of Non-Mycobacterium Tuberculosis. Available online: https://www.lungemedicin.dk/fagligt/65-non-tb-mykobakteriel-lungeinfektion.html (accessed on 22 July 2020).
- Takeda, K.; Imamura, Y.; Takazono, T.; Yoshida, M.; Ide, S.; Hirano, K.; Tashiro, M.; Saijo, T.; Kosai, K.; Morinaga, Y.; et al. The Risk Factors for Developing of Chronic Pulmonary Aspergillosis in Nontuberculous Mycobacteria Patients and Clinical Characteristics and Outcomes in Chronic Pulmonary Aspergillosis Patients Coinfected with Nontuberculous Mycobacteria. Med. Mycol. 2016, 54, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phoompoung, P.; Chayakulkeeree, M. Chronic Pulmonary Aspergillosis Following Nontuberculous Mycobacterial Infections: An Emerging Disease. J. Fungi 2020, 6, 346. [Google Scholar] [CrossRef] [PubMed]
- Raats, D.; Aldhaheri, S.M.S.; Marras, T.K.; Mehrabi, M.; Brode, S.K. Aspergillus Isolation in Nontuberculous Mycobacterial Pulmonary Disease: Associated with Antimycobacterial Treatment Initiation but Not Response. Respir. Med. 2021, 179, 106338. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Kida, H. New/Different Look at the Presence of Aspergillus in Mycobacterial Pulmonary Diseases. Long-Term Retrospective Cohort Study. Microorganisms 2021, 9, 270. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All Patients | Non-Tuberculous Mycobacterium Patients | Mycobacterium Tuberculosis Patients | Secondary Diagnosis Patients | p-Value | |
|---|---|---|---|---|---|
| Subjects (n) | 172 (100) | 49 (28.5) | 37 (21.5) | 86 (50.0) | |
| Male sex | 91 (52.9) | 22 (44.9) | 25 (67.6) | 44 (51.2) | 0.096 |
| Age (years) mean (min; max) | 52 (0; 88) | 70 (26; 86) | 42 (18; 62) | 46 (0; 88) | <0.001 |
| BMI (kg/m2) median | 22.19 (21.68–22.60) | 21.84 (20.28–22.49) | 22.28 (21.22–23.55) | 22.6 (21.68–24.50) | 0.566 |
| Alcohol > 14 (male sex) > 7 (female sex) pr. week | 17 (9.9) | 3 (6.1) | 9 (24.3) | 5 (5.8) | 0.008 |
| Smoking (active) | 58 (33.7) | 14 (28.6) | 22 (59.5) | 22 (25.6) | <0.001 |
| Substance abuse (current) | 9 (5.2) | 1 (2.0) | 3 (8.1) | 5 (5.8) | 0.393 |
| Substance abuse (prior) | 5 (2.9) | 3 (6.1) | 1 (2.7) | 1 (1.2) | 0.180 |
| Comorbidities | |||||
| Asthma | 14 (8.1) | 8 (16.3) | 1 (2.7) | 5 (5.8) | 0.054 |
| COPD | 27 (15.7) | 20 (40.8) | 2 (5.4) | 5 (5.8) | <0.001 |
| Structural, interstitial and infectious lung disease | 37 (21.5) | 21 (42.9) | 2 (5.4) | 14 (16.3) | <0.001 |
| Diabetes mellitus | 13 (7.6) | 7 (14.3) | 2 (5.4) | 4 (4.7) | 0.159 |
| Immunosuppressive disease | 3 (1.7) | 3 (6.1) | 0.031 | ||
| Autoimmune/rheumatic disease | 14 (8.1) | 8 (16.3) | 1 (2.7) | 5 (5.8) | 0.054 |
| Cancer former/current | 25 (14.5) | 12 (24.5) | 1 (2.7) | 12 (14.0) | 0.013 |
| No known illnesses | 35 (20.3) | 1 (2.0) | 11 (29.7) | 23 (26.7) | <0.001 |
| Medications | |||||
| Inhaled corticosteroid | 34 (19.8) | 22 (44.9) | 1 (2.7) | 11 (12.8) | <0.001 |
| Systemic steroid | 10 (5.8) | 4 (8.2) | 6 (7.0) | 0.216 | |
| Immunosuppressants (non-steroid) | 8 (4.7) | 1 (2.0) | 7 (8.1) | 0.112 | |
| Diabetics medication | 11 (6.4) | 7 (14.3) | 1 (2.7) | 3 (3.5) | 0.041 |
| Antibiotics use chronic/intermittent | 7 (4.1) | 4 (8.2) | 2 (5.4) | 1 (1.2) | 0.085 |
| No medicine at baseline | 32 (18.6) | 2 (4.1) | 9 (24.3) | 21 (24.4) | 0.003 |
| All Patients | Non-Tuberculous Mycobacterium Patients | Mycobacterium Tuberculosis Patients | Secondary Diagnosis Patients | p-Value | |
|---|---|---|---|---|---|
| Subjects (n) | 172 (100) | 49 (28.5) | 37 (21.5) | 86 (50.0) | |
| CCPA | 3 (1.7 (0.5–4.6)) | 2 (4.1 (0.9–12.5)) | - | 1 (1.2 (0.1–5.3)) | 0.313 |
| SAIA | 4 (2.3 (0.8–5.4)) | 2 (4.1 (0.9–12.5)) | - | 2 (2.3 (0.5–7.3)) | 0.669 |
| CPA | 7 (4.1 (1.8–7.8)) | 4 (8.2 (2.8–18.2)) | 0 (0 (0.92–1)) a | 3 (3.5 (1.0–9.0)) | 0.171 |
| Possible CPA | 3 (1.7 (0.5–4.6)) | 2 (4.1 (0.9–12.5)) | - | 1 (1.2 (0.1–5.3)) | 0.313 |
| ABPA | 1 (0.6 (0.1–2.7)) | 1 (2.0 (0.2–9.1)) | - | - | 0.500 |
| All Patients | Non-Tuberculous Mycobacterium Patients | Mycobacterium Tuberculosis Patients | Secondary Diagnosis Patients | p-Value | |
|---|---|---|---|---|---|
| Subjects (n) | 172 (100) | 49 (28.5) | 37 (21.5) | 86 (50.0) | |
| Observational FU time (days) Mean n (95CI) | 600 (556–645) | 541 (458–624) | 508 (418–599) | 673 (610–737) | 0.004 |
| FU time–clinical duration (days) Mean n (95CI) | 316 (278–354) | 405 (327–483) | 345 (300–391) | 253 (197–309) | 0.002 |
| Symptoms at baseline | |||||
| Symptom duration > 3 months | 55 (32.0) | 16 (43.2) | 23 (46.9) | 16 (18.6) | <0.001 |
| Dyspnoea | 47 (27.3) | 6 (16.2) | 28 (57.1) | 13 (15.1) | <0.001 |
| Cough | 110 (64.0) | 27 (73.0) | 35 (71.4) | 48 (55.8) | 0.091 |
| Fever | 21 (12.2) | 7 (18.9) | 6 (12.2) | 8 (9.3) | 0.346 |
| Lymphadenitis | 4 (2.3) | 2 (5.4) | 2 (2.3) | 0.254 | |
| Haemoptysis | 19 (11.0) | 7 (18.9) | 7 (14.3) | 5 (5.8) | 0.057 |
| Night sweats | 14 (8.1) | 5 (13.5) | 3 (6.1) | 6 (7.0) | 0.415 |
| Weight loss (unwanted/pathological > 5%/6 months) | 38 (22.1) | 20 (54.1) | 11 (22.4) | 7 (8.1) | <0.001 |
| Non-pulmonary/other symptoms | 78 (45.3) | 25 (67.6) | 24 (49.0) | 29 (33.7) | 0.002 |
| Asymptomatic | 28 (16.3) | 1 (2.7) | 3 (6.1) | 24 (27.9) | <0.001 |
| Symptoms during FU | |||||
| Progressive symptoms during FU | 12 (7.0) | 11 (22.4) | 1 (1.2) | <0.001 | |
| Unchanged symptoms during FU | 42 (24.4) | 7 (14.3) | 27 (73.0) | 32 (37.2) | <0.001 |
| Aspergillus serology | |||||
| Aspergillus serology at baseline | 90 (52.3) | 29 (59.2) | 29 (78.4) | 32 (37.2) | <0.001 |
| Aspergillus serology during FU | 14 (8.1) | 5 (10.2) | 2 (5.4) | 7 (8.1) | 0.766 |
| IgE > 115 × 103 IU/L | 42 (24.7) | 14 (28.6) | 16 (43.2) | 12 (14.3) | 0.002 |
| Asp. IgE > 0.35 × 103 IU/L | 6 (3.5) | 5 (10.2) | 1 (1.2) | 0.020 | |
| Asp. IgG > 75 mg/L | 14 (8.1) | 8 (16.3) | 3 (8.1) | 3 (3.5) | 0.054 |
| Aspergillus histology/cytology | |||||
| Respiratory sample tested for Aspergillus (any time) | 71 (41.3) | 38 (77.6) | 22 (59.5) | 11 (12.8) | <0.001 |
| Positive aspergillosis test at baseline | 7 (4.1) | 4 (8.2) | 1 (2.7) | 2 (2.3) | 0.267 |
| Positive aspergillosis test during FU | 7 (4.1) | 4 (8.2) | 3 (3.5) | 0.171 | |
| BAL/BL/Serum AGM positive | 8 (4.7) | 3 (6.1) | 1 (2.7) | 4 (4.7) | 0.803 |
| Baseline Radiology | |||||
| Radiology > 1 cavity/nodule/infiltrate at baseline | 122 (70.9) | 48 (98.0) | 37 (100) | 37 (43.0) | <0.001 |
| Bronchiectasis | 20 (11.6) | 10 (20.4) | 4 (10.8) | 6 (7.0) | 0.062 |
| Aspergilloma/fungal ball | 1 (0.6) | 1 (2.0) | 0.500 | ||
| Cavity/abscess without fungus | 28 (16.3) | 10 (20.4) | 14 (37.8) | 4 (4.7) | <0.001 |
| Unspecified consolidated/cavitating radiological abnormality | 87 (50.6) | 38 (77.6) | 25 (67.6) | 24 (27.9) | <0.001 |
| Nodule < 30 mm | 50 (29.1) | 20 (40.8) | 18 (48.6) | 12 (14.0) | <0.001 |
| Mass > 30 mm | 15 (8.7) | 7 (14.3) | 7 (18.9) | 1 (1.2) | <0.001 |
| Diffuse infiltrative changes | 21 (12.2) | 10 (20.4) | 7 (18.9) | 4 (4.7) | 0.006 |
| No baseline infiltrates | 48 (27.9) | 1 (2.0) | 47 (54.7) | <0.001 | |
| Pleural abnormalities | 42 (24.4) | 18 (36.7) | 9 (24.3) | 15 (17.4) | 0.049 |
| Radiological modalities | |||||
| Chest X-ray | 150 (87.2) | 41 (83.7) | 35 (94.6) | 74 (86.0) | 0.282 |
| CT | 58 (33.7) | 24 (49.0) | 17 (45.9) | 17 (19.8) | <0.001 |
| PET/CT | 39 (22.7) | 15 (30.6) | 18 (48.6) | 6 (7.0) | <0.001 |
| HRCT | 18 (10.5) | 15 (30.6) | 3 (3.5) | <0.001 | |
| No baseline radiology | 5 (2.9) | 5 (5.8) | 0.131 | ||
| No FU radiology | 36 (20.9) | 5 (10.2) | 1 (2.7) | 30 (34.9) | <0.001 |
| Radiology progression during FU | 29 (16.9) | 19 (38.8) | 4 (10.8) | 6 (7.0) | <0.001 |
| Anti-tuberculosis treatment during FU | 97 (56.4) | 35 (71.4) | 37 (100) | 25 (29.1) | <0.001 |
| Anti-fungal treatment during FU | 6 (3.5) | 3 (6.1) | 3 (3.5) | 0.408 | |
| Average treatment duration (days) Median | 149 | 266 (188–343) | 218 | 52 (34–70) | <0.001 |
| Deaths during FU | 11 (6.4) | 6 (12.2) | 5 (5.8) | 0.503 | |
| NTM microbiology–species * | |||||
| M. abscessus | 1 | 1 | |||
| M. avium | 22 | 20 | 2 | ||
| M. celatum | 1 | 1 | |||
| M. chelonae | 1 | 1 | |||
| M. chimaera | 12 | 12 | |||
| M. gordonae | 2 | 2 | |||
| M. heckeshornense | 1 | 1 | |||
| M. intracellulare | 2 | 2 | |||
| M. kansasii | 2 | 2 | |||
| M. malmoense | 1 | 1 | |||
| M. neoarum | 1 | 1 | |||
| M. parascrofulaceum | 1 | 1 | |||
| M. szulgai | 1 | 1 | |||
| M. xenopi | 2 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klinting, F.P.; Laursen, C.B.; Titlestad, I.L. Incidence of Chronic Pulmonary Aspergillosis in Patients with Suspected or Confirmed NTM and TB—A Population-Based Retrospective Cohort Study. J. Fungi 2022, 8, 301. https://doi.org/10.3390/jof8030301
Klinting FP, Laursen CB, Titlestad IL. Incidence of Chronic Pulmonary Aspergillosis in Patients with Suspected or Confirmed NTM and TB—A Population-Based Retrospective Cohort Study. Journal of Fungi. 2022; 8(3):301. https://doi.org/10.3390/jof8030301
Chicago/Turabian StyleKlinting, Frederik P., Christian B. Laursen, and Ingrid L. Titlestad. 2022. "Incidence of Chronic Pulmonary Aspergillosis in Patients with Suspected or Confirmed NTM and TB—A Population-Based Retrospective Cohort Study" Journal of Fungi 8, no. 3: 301. https://doi.org/10.3390/jof8030301
APA StyleKlinting, F. P., Laursen, C. B., & Titlestad, I. L. (2022). Incidence of Chronic Pulmonary Aspergillosis in Patients with Suspected or Confirmed NTM and TB—A Population-Based Retrospective Cohort Study. Journal of Fungi, 8(3), 301. https://doi.org/10.3390/jof8030301