
Comparative Efficacy of Antifungal Agents Used in the Treatment of Oropharyngeal Candidiasis among HIV-Infected Adults: A Systematic Review and Network Meta-Analysis



Abstract
1. Introduction
2. Material and Methods
2.1. Search Strategy and Study Selection
2.2. Inclusion Criteria
- Participants had to be HIV-infected adults with OPC;
- Interventions were any class of antifungal agents (at any dose), or complementary medicine tested for the treatment of OPC;
- Comparisons were other classes of the antifungal agent or other active interventions which were used;
- The primary outcome was the number of patients who achieved clinical cure;
- The secondary outcomes were the number of patients who achieved mycological cure from OPC, adverse events and the rate of OPC relapse.
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
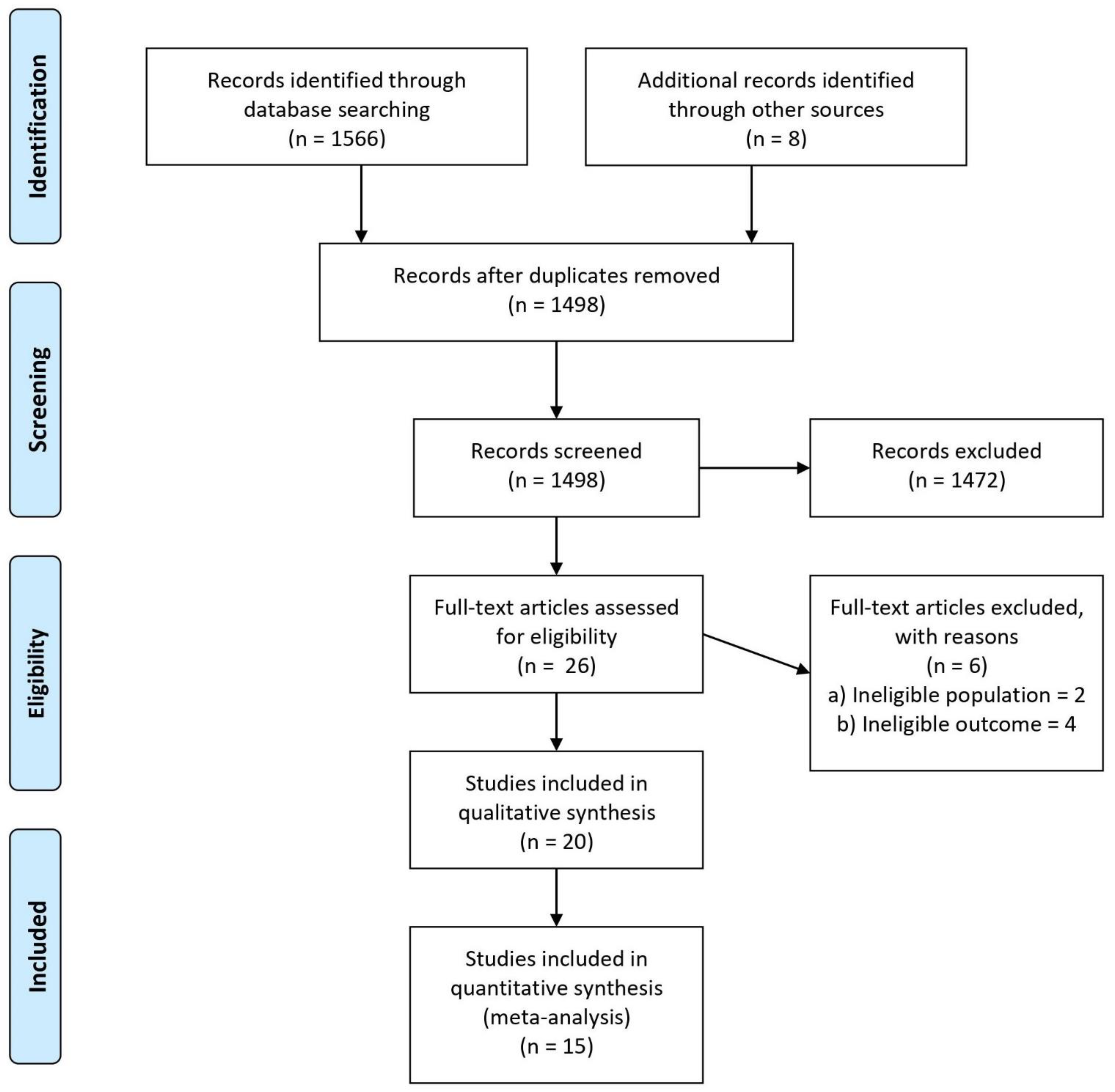
3.1. Search Results
3.2. Study Characteristics
3.3. Risk of Bias
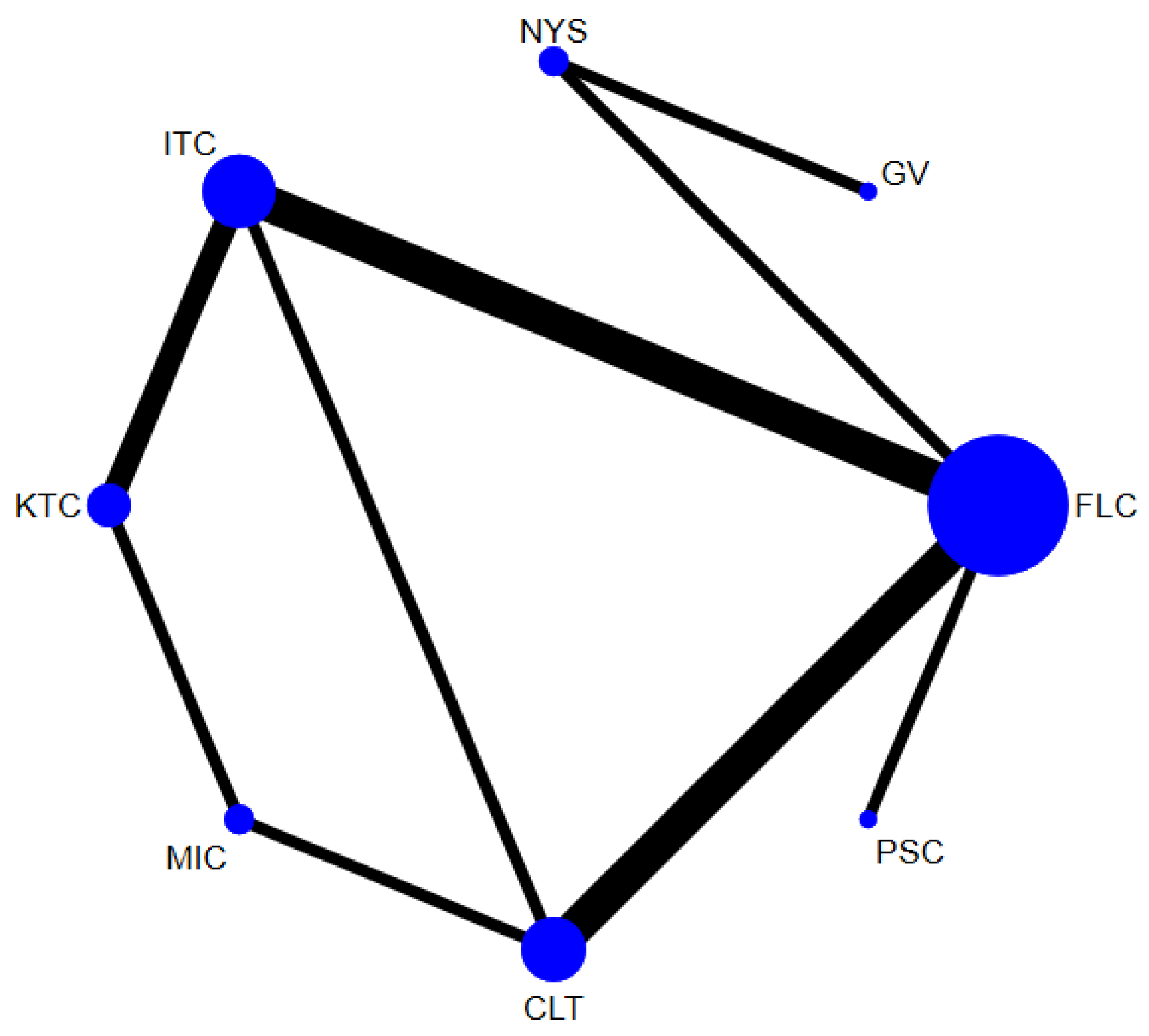
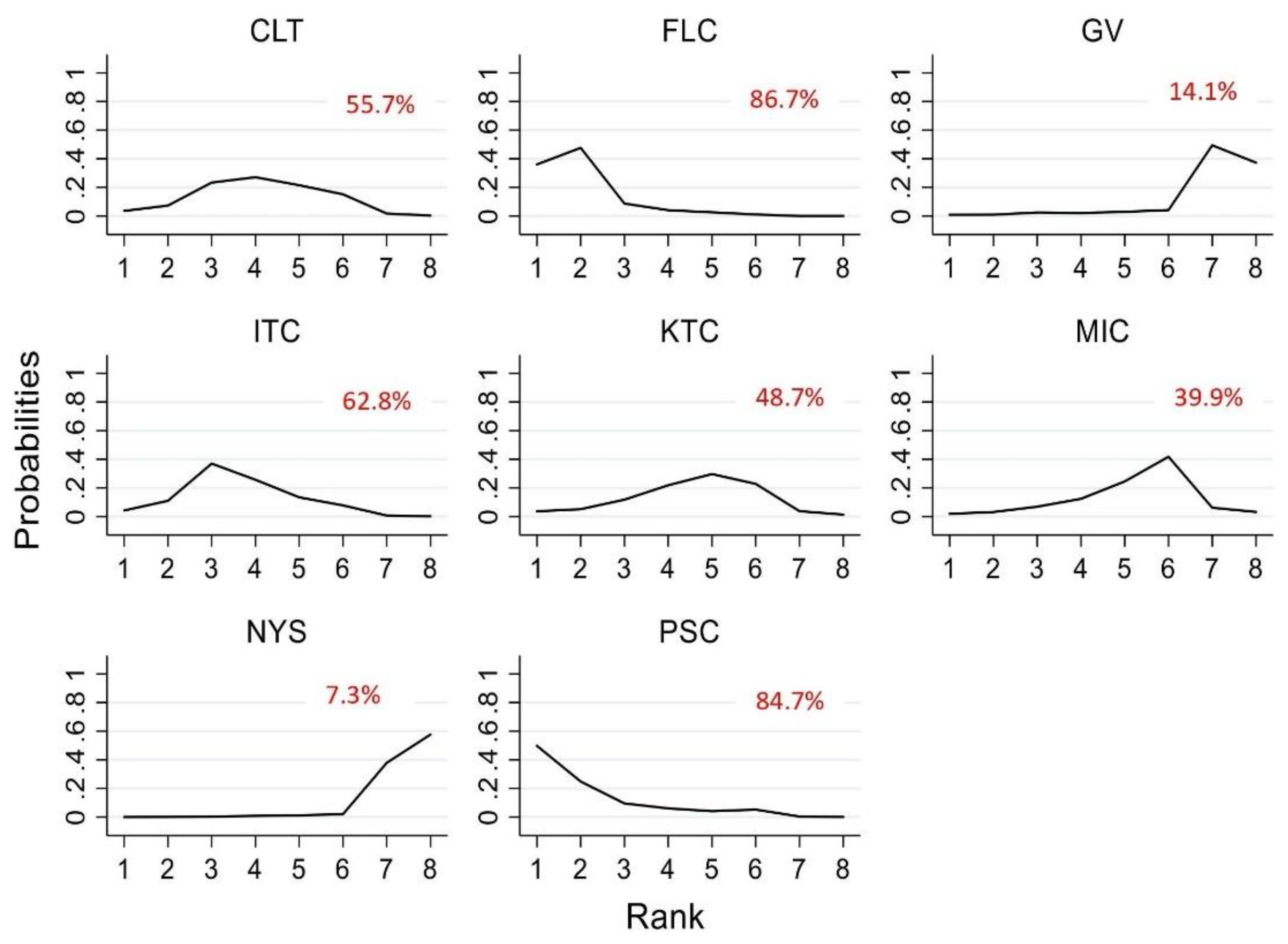
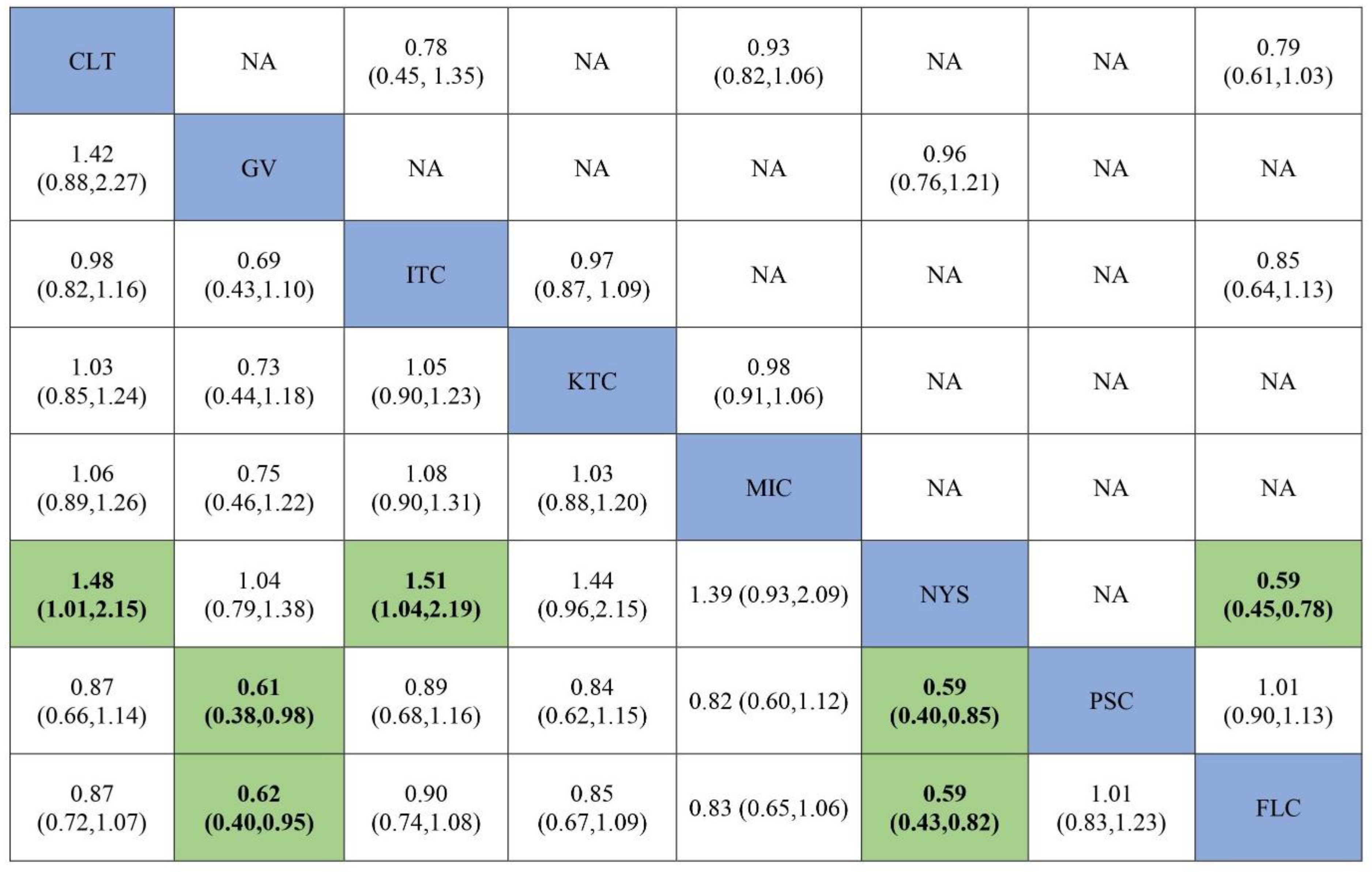
3.4. Efficacy of Antifungal Agents Used in the Treatment of OPC to Achieve Clinical Cure (Network Meta-Analysis)
3.5. Efficacy of Antifungal Agents Used in the Treatment of OPC to Achieve Clinical Cure (Pairwise Meta-Analysis)
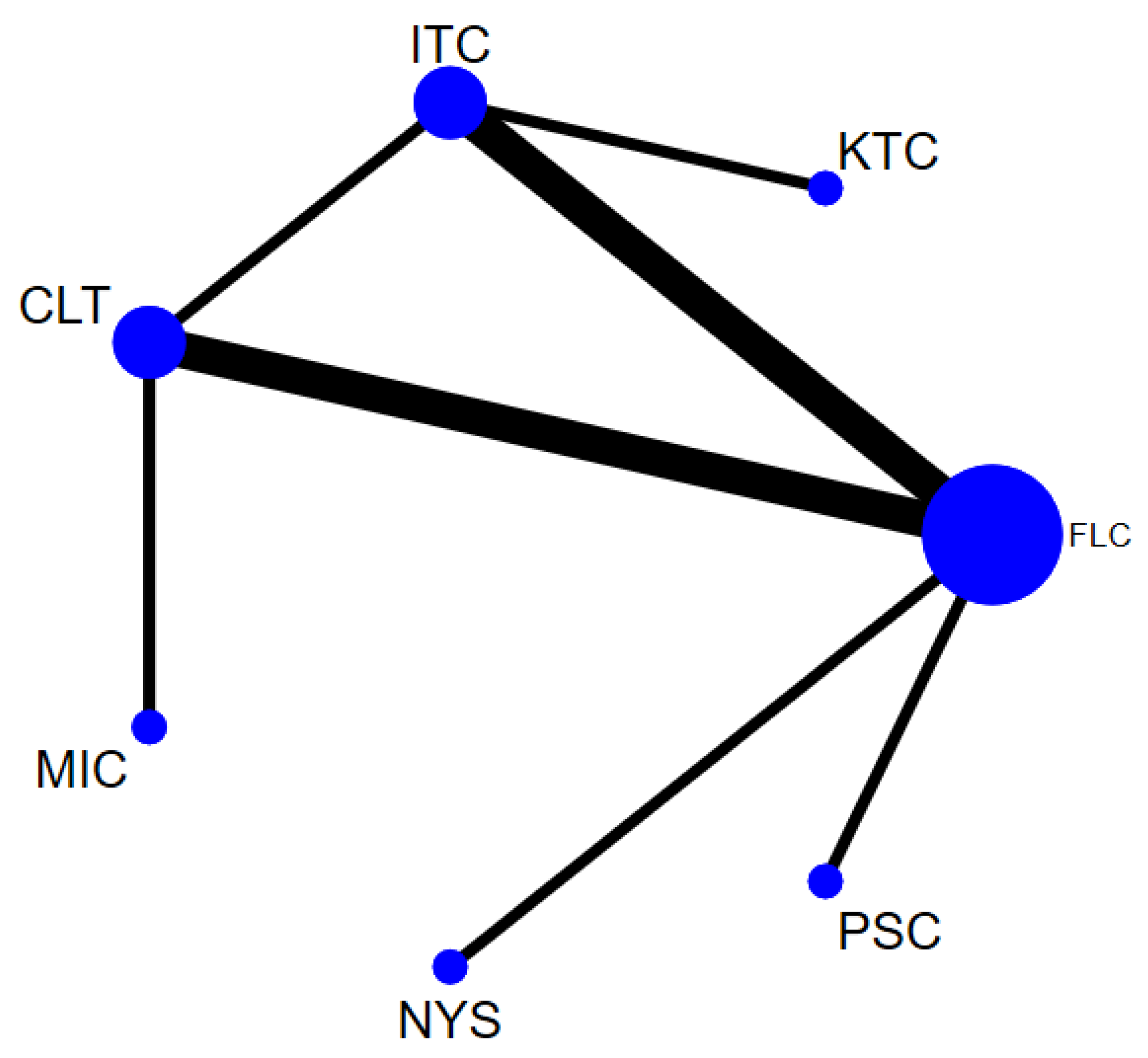
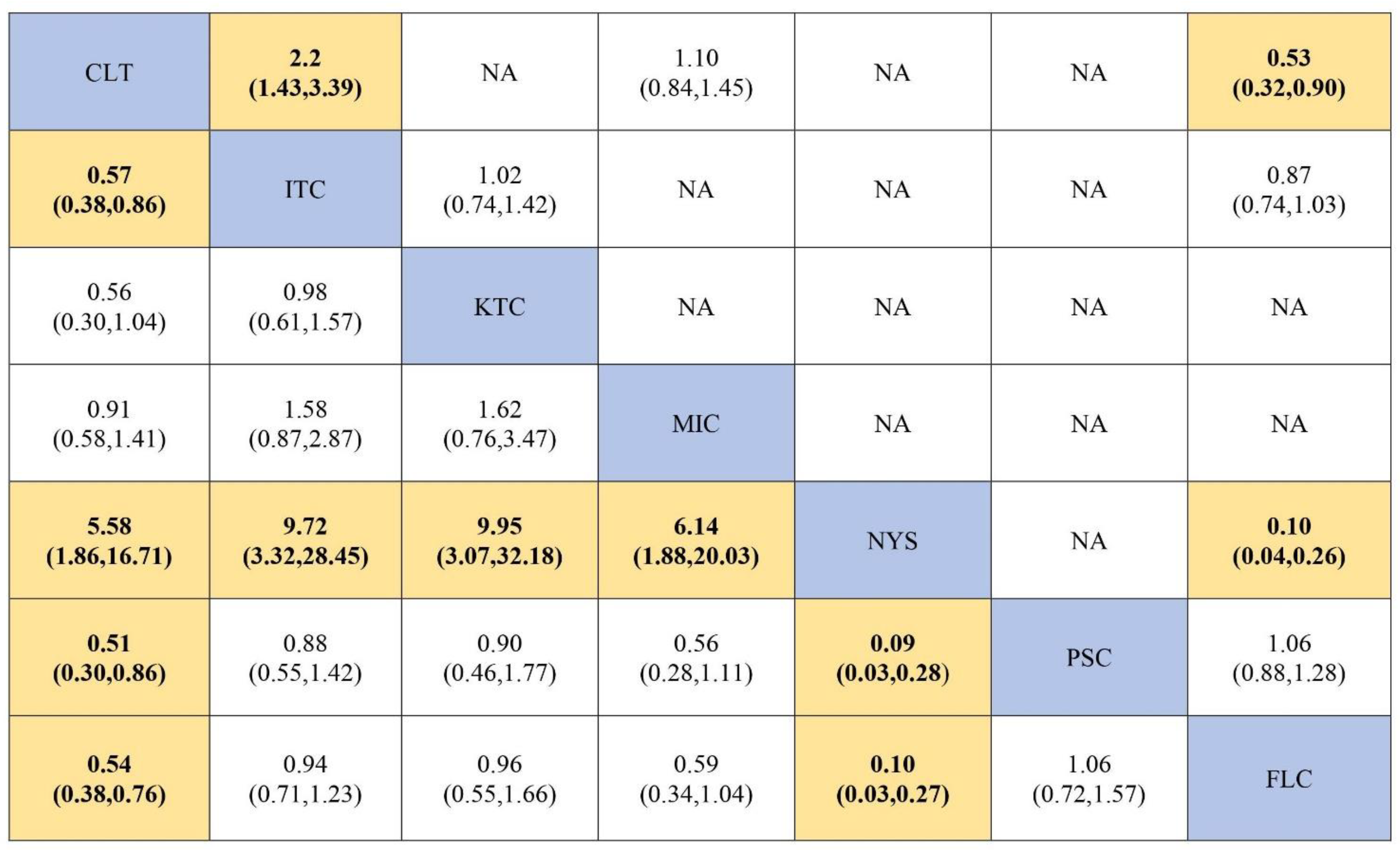
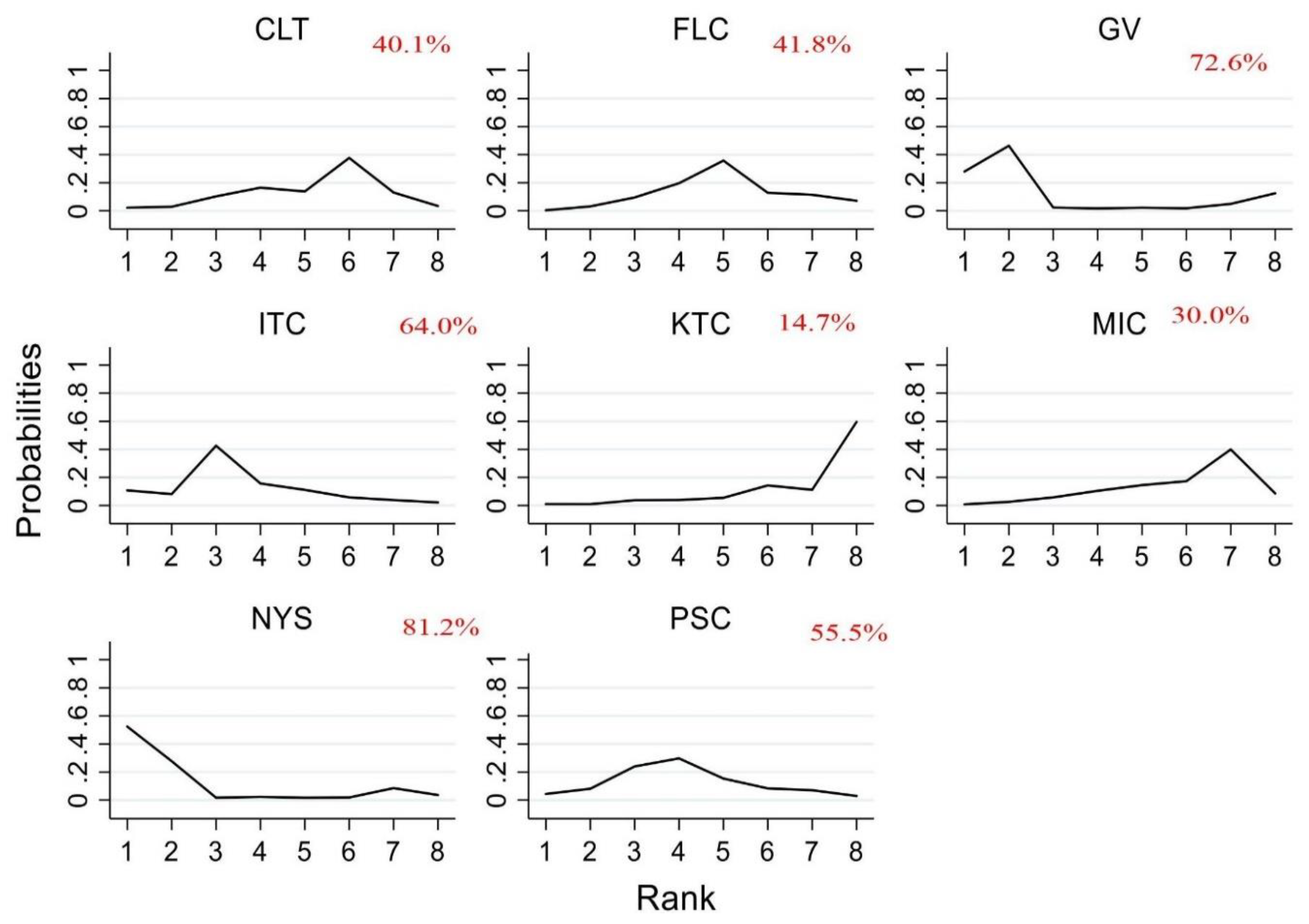
3.6. Efficacy of Antifungal Agents Used in the Treatment of OPC to Achieve Mycological Cure (Network Meta-Analysis)
3.7. Efficacy of Antifungal Agents Used in the Treatment of OPC to Achieve Mycological Cure (Pairwise Meta-Analysis)
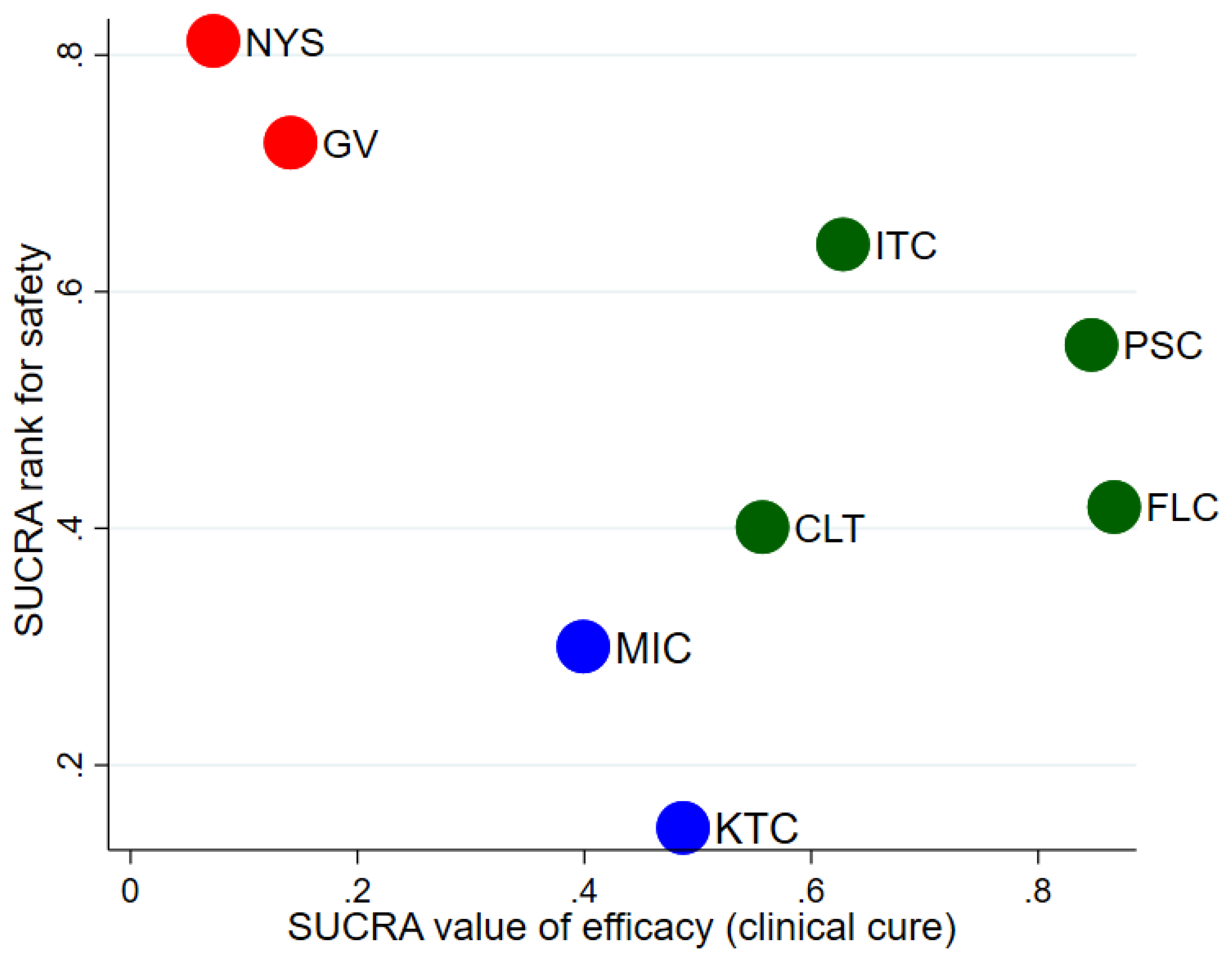
3.8. Safety of Antifungal Agents Used in Treating OPC
3.9. Rate of OPC Relapse upon Treatment Completion
3.10. GRADE Quality Assessment
3.11. Network Consistency and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Samaranayake, L.P.; Holmstrup, P. Oral candidiasis and human immunodeficiency virus infection. J. Oral Pathol. Med. 1989, 18, 554–564. [Google Scholar] [CrossRef]
- Samaranayake, L.P. Oral mycoses in HIV infection. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 171–180. [Google Scholar] [CrossRef]
- De Repentigny, L.; Lewandowski, D.; Jolicoeur, P. Immunopathogenesis of Oropharyngeal Candidiasis in Human Immunodeficiency Virus Infection. Clin. Microbiol. Rev. 2004, 17, 729–759. [Google Scholar] [CrossRef]
- Flint, S.; Tappuni, A.; Leigh, J.; Schmidt-Westhausen, A.-M.; MacPhail, L. (B3) Markers of Immunodeficiency and Mechanisms of HAART Therapy on Oral Lesions. Adv. Dent. Res. 2006, 19, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Nicolatou-Galitis, O.; Velegraki, A.; Paikos, S.; Economopoulou, P.; Stefaniotis, T.; Papanikolaou, I.; Kordossis, T. Effect of PI-HAART on the prevalence of oral lesions in HIV-1 infected patients. A Greek study. Oral Dis. 2004, 10, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Low, A.; Gavriilidis, G.; Larke, N.; B-Lajoie, M.-R.; Drouin, O.; Stover, J.; Muhe, L.; Easterbrook, P. Incidence of Opportunistic Infections and the Impact of Antiretroviral Therapy Among HIV-Infected Adults in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2016, 62, 1595–1603. [Google Scholar] [CrossRef]
- Yengopal, V.; Naidoo, S. Do oral lesions associated with HIV affect quality of life? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 106, 66–73. [Google Scholar] [CrossRef]
- Thompson, G.R.; Patel, P.; Kirkpatrick, W.R.; Westbrook, S.D.; Berg, D.; Erlandsen, J.; Redding, S.W.; Patterson, T.F. Oropharyngeal candidiasis in the era of antiretroviral therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 488–495. [Google Scholar] [CrossRef]
- Gaitan-Cepeda, L.A.; Sanchez-Vargas, L.O.; Pavia-Ruz, N.; Munoz-Hernandez, R.; Villegas-Ham, J.; Caballos-Salobrena, A. Oral candida in Mexican children with malnutrition, social marginalization, or HIV/AIDS. Rev. Panam. De Salud Públi. 2012, 31, 48–53. [Google Scholar] [CrossRef]
- Darouiche, R.O. Oropharyngeal and Esophageal Candidiasis in Immunocompromised Patients: Treatment Issues. Clin. Infect. Dis. 1998, 26, 259–272. [Google Scholar] [CrossRef]
- Tavitian, A.; Raufman, J.P.; Rosenthal, L.E. Oral Candidiasis as a Marker for Esophageal Candidiasis in the Acquired Immunodeficiency Syndrome. Ann. Intern. Med. 1986, 104, 54–55. Available online: http://pubmed.ncbi.nlm.nih.gov/3940505/ (accessed on 2 December 2020). [CrossRef] [PubMed]
- Walker, A.S.; Mulenga, V.; Sinyinza, F.; Lishimpi, K.; Nunn, A.; Chintu, C.; Gibb, D. Determinants of Survival Without Antiretroviral Therapy After Infancy in HIV-1-Infected Zambian Children in the CHAP Trial. JAIDS J. Acquir. Immune Defic. Syndr. 2006, 42, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Koletar, S.L.; Russell, J.A.; Fass, R.J.; Plouffe, J.F. Comparison of oral fluconazole and clotrimazole troches as treatment for oral candidiasis in patients infected with human immunodeficiency virus. Antimicrob. Agents Chemother. 1990, 34, 2267–2268. [Google Scholar] [CrossRef]
- Redding, S.W.; Farinacci, G.C.; Smith, J.A.; Fothergill, A.W.; Rinaldi, M.G. A comparison between fluconazole tablets and clotrimazole troches for the treatment of thrush in HIV infection. Spéc. Care Dent. 1992, 12, 24–27. [Google Scholar] [CrossRef]
- Graybill, J.R.; Vazquez, J.; Darouiche, R.O.; Morhart, R.; Greenspan, D.; Tuazon, C.; Wheat, L.; Carey, J.; Leviton, I.; Hewitt, R.G.; et al. Randomized Trial of Itraconazole Oral Solution for Oropharyngeal Candidiasis in HIV/AIDS Patients. Am. J. Med. 1998, 104, 33–39. [Google Scholar] [CrossRef]
- De Repentigny, L.; Ratelle, J. Comparison of Itraconazole and Ketoconazole in HIV-Positive Patients with Oropharyngeal or Esophageal Candidiasis. Chemotherapy 1996, 42, 374–383. [Google Scholar] [CrossRef]
- De Wit, S.; Goossens, H.; Weerts, D.; Clumeck, N. Comparison of fluconazole and ketoconazole for oropharyngeal candidiasis in AIDS. Lancet 1989, 333, 746–748. [Google Scholar] [CrossRef]
- Hernández-Sampelayo, T. A Multicentre Study Group Fluconazole versus ketoconazole in the treatment of oropharyngeal candidiasis in HIV-infected children. Eur. J. Clin. Microbiol. Infect. Dis. 1994, 13, 340–344. [Google Scholar] [CrossRef]
- Shen, L.Y.; Yee, W.T.; Veettil, S.K.; Wong, P.S.; Gopinath, D.; Ching, M.S.; Menon, R.K. Antifungal agents in preventing oral candidiasis in clinical oncology: A network meta-analysis. Oral Dis. 2020. [Google Scholar] [CrossRef]
- Vazquez, J.A.; Skiest, D.J.; Nieto, L.; Northland, R.; Sanne, I.; Gogate, J.; Greaves, W.; Isaacs, R. A Multicenter Randomized Trial Evaluating Posaconazole versus Fluconazole for the Treatment of Oropharyngeal Candidiasis in Subjects with HIV/AIDS. Clin. Infect. Dis. 2006, 42, 1179–1186. [Google Scholar] [CrossRef]
- Caldwell, D.M.; Ades, T.; Higgins, J. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ 2005, 331, 897–900. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook/current (accessed on 26 December 2020).
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 62, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.; Elbers, R.G.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Mbuagbaw, L.; Rochwerg, B.; Jaeschke, R.; Heels-Andsell, D.; Alhazzani, W.; Thabane, L.; Guyatt, G.H. Approaches to interpreting and choosing the best treatments in network meta-analyses. Syst. Rev. 2017, 6, 79. [Google Scholar] [CrossRef]
- Hoaglin, D.C.; Hawkins, N.; Jansen, J.P.; Scott, D.A.; Itzler, R.; Cappelleri, J.C.; Boersma, C.; Thompson, D.; Larholt, K.M.; Diaz, M.; et al. Conducting Indirect-Treatment-Comparison and Network-Meta-Analysis Studies: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 2. Value Health 2011, 14, 429–437. [Google Scholar] [CrossRef]
- Dersimonian, R.; Laird, N. N: Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Vasiliadis, H.S.; Higgins, J.; Salanti, G. Evaluation of inconsistency in networks of interventions. Int. J. Epidemiol. 2013, 42, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Jackson, D.; Barrett, J.; Lu, G.; Ades, A.E.; White, I.R. Consistency and inconsistency in network meta-analysis: Concepts and models for multi-arm studies. Res. Synth. Methods 2012, 3, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Ades, A.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Chaimani, A.; Higgins, J.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical Tools for Network Meta-Analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef]
- Puhan, M.A.; Schünemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H. For the GRADE Working Group A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef]
- Nyst, M.J.; Perriens, J.H.; Kimputu, L.; Lumbila, M.; Nelson, A.M.; Piot, P. Gentian violet, ketoconazole and nystatin in oropharyngeal and esophageal candidiasis in Zairian AIDS patients. Ann. Soc. Belg. Med. Trop. 1992, 72, 45–52. [Google Scholar]
- Skiest, D.J.; Vazquez, J.A.; Anstead, G.M.; Graybill, J.R.; Reynes, J.; Ward, D.; Hare, R.; Boparai, N.; Isaacs, R. Posaconazole for the Treatment of Azole-Refractory Oropharyngeal and Esophageal Candidiasis in Subjects with HIV Infection. Clin. Infect. Dis. 2007, 44, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Arathoon, E.G.; Gotuzzo, E.; Noriega, L.M.; Berman, R.S.; DiNubile, M.J.; Sable, C.A. Randomized, Double-Blind, Multicenter Study of Caspofungin versus Amphotericin B for Treatment of Oropharyngeal and Esophageal Candidiases. Antimicrob. Agents Chemother. 2002, 46, 451–457. [Google Scholar] [CrossRef]
- Chavanet, P.Y.; Garry, I.; Charlier, N.; Caillot, D.; Kisterman, J.P.; D’Athis, M.; Portier, H. Trial of glucose versus fat emulsion in preparation of amphotericin for use in HIV infected patients with candidiasis. BMJ 1992, 305, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Scwingel, A.R.; Barcessat, A.R.; Nunez, S.C.; Ribeiro, M.S. Antimicrobial Photodynamic Therapy in the Treatment of Oral Candidiasis in HIV-Infected Patients. Photomed. Laser Surg. 2012, 30, 429–432. [Google Scholar] [CrossRef] [PubMed]
- Pons, V.; Greenspan, D.; DeBruin, M. Therapy for oropharyngeal candidiasis in HIV-infected patients: A randomized, prospective multicenter study of oral fluconazole versus clotrimazole troches. The Multicenter Study Group. JAIDS J. Acquir. Immune Defic. Syndr. 1993, 6, 1311–1316. [Google Scholar]
- De Wit, S.; O’Doherty, E.; De Vroey, C.; Clumeck, N. Safety and Efficacy of Single-Dose Fluconazole Compared with a 7-Day Regimen of Itraconazole in the Treatment of AIDS-Related Oropharyngeal Candidiasis. J. Int. Med. Res. 1998, 26, 159–170. [Google Scholar] [CrossRef]
- Phillips, P.; De Beule, K.; Frechette, G.; Tchamouroff, S.; Vandercam, B.; Weitner, L.; Hoepelman, A.; Stingl, G.; Clotet, B. A double-blind comparison of itraconazole oral solution and fluconazole capsules for the treatment of oropharyngeal candidiasis in patients with AIDS. Clin. Infect. Dis. 1998, 26, 1368–1373. [Google Scholar] [CrossRef][Green Version]
- Smith, D.E.; Midgley, J.; Allan, M.; Connolly, G.M.; Gazzard, B.G. Itraconazole versus Ketaconazole in the Treatment of Oral and Oesophageal Candidosis in Patients Infected with HIV. AIDS 1991, 5, 1367–1371. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.A.; Koletar, S.L.; Mallegol, I.; Wu, J.; Moskovitz, B.L. Itraconazole oral solution versus clotrimazole troches for the treatment of oropharyngeal candidiasis in immunocompromised patients. Clin. Ther. 1997, 19, 471–480. [Google Scholar] [CrossRef]
- Linpiyawan, R.; Jittreprasert, K.; Sivayathorn, A. Clinical trial: Clotrimazole troche vs. itraconazole oral solution in the treatment of oral candidosis in AIDS patients. Int. J. Dermatol. 2000, 39, 859–861. [Google Scholar] [CrossRef] [PubMed]
- De Wit, S.; Goossens, H.; Clumeck, N. Single-Dose versus 7 Days of Fluconazole Treatment for Oral Candidiasis in Human Immunodeficiency Virus-Infected Patients: A Prospective, Randomized Pilot Study. J. Infect. Dis. 1993, 168, 1332–1333. [Google Scholar] [CrossRef]
- Hamza, O.J.M.; Matee, M.I.N.; Brüggemann, R.J.M.; Moshi, M.; Simon, E.N.M.; Mugusi, F.; Mikx, F.H.M.; Van Der Lee, H.A.L.; Verweij, P.; Van Der Ven, A.J.A.M. Single-Dose Fluconazole versus Standard 2-Week Therapy for Oropharyngeal Candidiasis in HIV-Infected Patients: A Randomized, Double-Blind, Double-Dummy Trial. Clin. Infect. Dis. 2008, 47, 1270–1276. [Google Scholar] [CrossRef]
- De Wit, S.; Dupont, B.; Cartledge, J.D.; Hawkins, D.A.; Gazzard, B.G.; Clumeck, N.; Denning, D.W. A dose comparison study of a new triazole antifungal (D0870) in HIV-positive patients with oral candidiasis. AIDS 1997, 11, 759–763. [Google Scholar] [CrossRef]
- Vazquez, J.A.; Patton, L.; Epstein, J.B.; Ramlachan, P.; Mitha, I.; Noveljic, Z.; Fourie, J.; Conway, B.; Lalla, R.V.; Barasch, A.; et al. Randomized, Comparative, Double-Blind, Double-Dummy, Multicenter Trial of Miconazole Buccal Tablet and Clotrimazole Troches for the Treatment of Oropharyngeal Candidiasis: Study of Miconazole Lauriad® Efficacy and Safety (SMiLES). HIV Clin. Trials 2010, 11, 186–196. [Google Scholar] [CrossRef]
- Pons, V.; Greenspan, D.; Lozada-Nur, F.; McPhail, L.; Gallant, J.E.; Tunkel, A.; Johnson, C.C.; Mccarty, J.; Panzer, H.; Levenstein, M.; et al. Oropharyngeal Candidiasis in Patients with AIDS: Randomized Comparison of Fluconazole Versus Nystatin Oral Suspensions. Clin. Infect. Dis. 1997, 24, 1204–1207. [Google Scholar] [CrossRef]
- Vazquez, J.A.; Zawawi, A.A. Efficacy of alcohol-based and alcohol-free melaleuca oral solution for the treatment of fluconazole-refractory oropharyngeal candidiasis in patients with AIDS. HIV Clin. Trials 2002, 3. [Google Scholar] [CrossRef]
- Van Roey, J.H.M.; Kamya, M.; Lwanga, I.; Katabira, E. Comparative Efficacy of Topical Therapy with a Slow-Release Mucoadhesive Buccal Tablet Containing Miconazole Nitrate versus Systemic Therapy with Ketoconazole in HIV-Positive Patients with Oropharyngeal Candidiasis. JAIDS J. Acquir. Immune Defic. Syndr. 2004, 35, 144–150. [Google Scholar] [CrossRef]
- Mukherjee, P.K.; Chen, H.; Patton, L.; Evans, S.; Lee, A.; Kumwenda, J.; Hakim, J.; Masheto, G.; Sawe, F.; Pho, M.T.; et al. Topical gentian violet compared with nystatin oral suspension for the treatment of oropharyngeal candidiasis in HIV-1-infected participants. AIDS 2017, 31, 81–88. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wright, S.; Maree, J.; Sibanyoni, M. Treatment of oral thrush in HIV/AIDS patients with lemon juice and lemon grass (Cymbopogon citratus) and gentian violet. Phytomedicine 2009, 16, 118–124. [Google Scholar] [CrossRef]
- Pienaar, E.D.; Young, T.; Holmes, H. Interventions for the Prevention and Management of Oropharyngeal Candidiasis Associated with HIV Infection in Adults and Children. Cochrane Database Syst. Rev. Online 2010, 11, CD003940. [Google Scholar] [CrossRef] [PubMed]
- Patton, L.L.; Bonito, A.J.; Shugars, D.A. A systematic review of the effectiveness of antifungal drugs for the prevention and treatment of oropharyngeal candidiasis in HIV-positive patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2001, 92, 170–179. [Google Scholar] [CrossRef]
- Goa, K.L.; Barradell, L.B. Fluconazole. Drugs 1995, 50, 658–690. [Google Scholar] [CrossRef] [PubMed]
- Bodey, G.P. Azole Antifungal Agents. Clin. Infect. Dis. 1992, 14, S161–S169. [Google Scholar] [CrossRef] [PubMed]
- Debruyne, D. Clinical Pharmacokinetics of Fluconazole in Superficial and Systemic Mycoses. Clin. Pharmacokinet. 1997, 33, 52–77. [Google Scholar] [CrossRef]
- Vazquez, J. Optimal management of oropharyngeal and esophageal candidiasis in patients living with HIV infection. HIV/AIDS Res. Palliat. Care 2010, 2, 89–101. [Google Scholar] [CrossRef]
- Patil, S.; Rao, R.S.; Majumdar, B.; Anil, S. Clinical Appearance of Oral Candida Infection and Therapeutic Strategies. Front. Microbiol. 2015, 6, 1391. [Google Scholar] [CrossRef]
- Ianas, V.; Matthias, K.R.; Klotz, S.A. Role of Posaconazole in the Treatment of Oropharyngeal Candidiasis. Infect. Drug Resist. 2010, 3, 45–51. [Google Scholar]
- Gupta, A.K. The Safety Aspects of Systemic and Topical Antifungal Agents Used in the Management of Onychomycosis. In Hydroxy-Pyridones as Antifungal Agents with Special Emphasis on Onychomycosis; Shuster, S., Ed.; Springer: Berlin/Heidelberg, Germany, 1999; pp. 96–102. ISBN 978-3-540-65494-0. [Google Scholar]
- Wang, J.-L.; Chang, C.-H.; Young-Xu, Y.; Chan, K. Systematic Review and Meta-Analysis of the Tolerability and Hepatotoxicity of Antifungals in Empirical and Definitive Therapy for Invasive Fungal Infection. Antimicrob. Agents Chemother. 2010, 54, 2409–2419. [Google Scholar] [CrossRef]
- Berberi, A.; Noujeim, Z.; Aoun, G. Epidemiology of Oropharyngeal Candidiasis in Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome Patients and CD4+ Counts. J. Int. Oral Health 2015, 7, 20–23. [Google Scholar]
- Oxman, D.A.; Chow, J.K.; Frendl, G.; Hadley, S.; Hershkovitz, S.; Ireland, P. Candidaemia associated with decreased in vitro fluconazole susceptibility: Is Candida speciation predictive of the susceptibility pattern? J. Antimicrob. Chemother. 2010, 65, 1460–1465. [Google Scholar] [CrossRef]
- Lee, I.; Fishman, N.O.; Zaoutis, T.E.; Morales, K.H.; Weiner, M.G.; Synnestvedt, M.; Nachamkin, I.; Lautenbach, E. Risk Factors for Fluconazole-Resistant Candida glabrata Bloodstream Infections. Arch. Intern. Med. 2009, 169, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.I.; Choi, C.W.; Lee, K.M.; Kim, Y.K.; Kim, T.U.; Kim, E.C. National surveillance of antifungal susceptibility of Candida species in South Korean hospitals. Med. Mycol. 2009, 47, 554–558. [Google Scholar] [CrossRef]
- Carrizosa, M.M.; Sanchez-Reus, F.; March, F.; Coll, P. Fungemia in a Spanish hospital: The role of Candida parapsilosis over a 15-year period. Scand. J. Infect. Dis. 2014, 46, 454–461. [Google Scholar] [CrossRef]
- Gong, X.; Luan, T.; Wu, X.; Li, G.; Qiu, H.; Kang, Y.; Qin, B.; Fang, Q.; Cui, W.; Qin, Y.; et al. Invasive candidiasis in intensive care units in China: Risk factors and prognoses of Candida albicans and non–albicans Candida infections. Am. J. Infect. Control. 2016, 44, e59–e63. [Google Scholar] [CrossRef]
- Blot, S.; Janssens, R.; Claeys, G.; Hoste, E.; Buyle, F.; De Waele, J.J. Effect of fluconazole consumption on long-term trends in can-didal ecology. J. Antimicrob. Chemother. 2016, 58, 474–477. [Google Scholar] [CrossRef]
- Quindós, G.; Gil-Alonso, S.; Marcos-Arias, C.; Sevillano, E.; Mateo, E.; Jauregizar, N.; Eraso, E. Therapeutic tools for oral can-didiasis: Current and new antifungal drugs. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e172–e180. [Google Scholar]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L. Clinical practice guideline for the management of candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Ghannoum, M.A.; Elewski, B. Successful Treatment of Fluconazole-Resistant Oropharyngeal Candidiasis by a Combination of Fluconazole and Terbinafine. Clin. Diagn. Lab. Immunol. 1999, 6, 921–923. [Google Scholar] [CrossRef]
- Sugar, A.M. Use of amphotericin B with azole antifungal drugs: What are we doing? Antimicrob. Agen. Chemother. 1995, 39, 1907–1912. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krause, D.S.; Simjee, A.E.; Van Rensburg, C.; Viljoen, J.; Walsh, T.J.; Goldstein, B.P.; Wible, M.; Henkel, T. A Randomized, Double-Blind Trial of Anidulafungin versus Fluconazole for the Treatment of Esophageal Candidiasis. Clin. Infect. Dis. 2004, 39, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A.; Gotuzzo, E.; Arathoon, E.G.; Noriega, L.; Kartsonis, N.A.; Lupinacci, R.J.; Smietana, J.M.; Di Nubile, M.J.; Sable, C.A. A randomized double-blind study of caspofungin versus fluconazole for the treatment of esophageal candidiasis. Am. J. Med. 2002, 113, 294–299. [Google Scholar] [CrossRef]
- Villanueva, A.; Arathoon, E.G.; Gotuzzo, E.; Berman, R.S.; DiNubile, M.J.; Sable, C.A. A Randomized Double-Blind Study of Caspofungin versus Amphotericin for the Treatment of Candidal Esophagitis. Clin. Infect. Dis. 2001, 33, 1529–1535. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, D.M.; George, T.; Chandra, J.; Mukherjee, P.K.; Ghannoum, M.A. Antifungal Susceptibility of Candida Biofilms: Unique Efficacy of Amphotericin B Lipid Formulations and Echinocandins. Antimicrob. Agents Chemother. 2002, 46, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, S.P.; VandeWalle, K.; Ramage, G.; Patterson, T.F.; Wickes, B.; Graybill, J.R.; López-Ribot, J.L. In Vitro Activity of Caspofungin against Candida albicans Biofilms. Antimicrob. Agents Chemother. 2002, 46, 3591–3596. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | No. of Randomized Participants | Study Design | Study Comparison | Gender | |
|---|---|---|---|---|---|---|
| Male | Female | |||||
| Koletar SL et al., 1990 | NM | 36 | RCT | Fluconazole s 100 mg OD vs. Clotrimazole t 10 mg 5× Daily day | 33 | 3 |
| Smith DE et al., 1991 | UK | 85 | RCT | Itraconazole s 200 mg OD vs. Ketoconazole s 200 mg BD | 85 | 0 |
| Redding S.W. et al., 1992 | US | 24 | RCT | Fluconazole s 100 mg OD vs. Clotrimazole t 10 mg 5× Daily | 24 | 0 |
| De Wit S et al., 1993 | NM | 56 | RCT | Single dose Fluconazole s 150 mg vs. Daily Fluconazole s 50 mg | NM | NM |
| Pons V et al., 1993 | NM | 334 | RCT | Fluconazole s 100 mg OD vs. Clotrimazole t 10 mg 5× a day | 308 | 26 |
| de Repentigny L et al., 1996 | Canada | 106 | RCT | Itraconazole s 200 mg OD vs. Ketoconazole s 200 mg OD | 93 | 5 |
| De Wit S et al., 1997 | Belgium, UK, France | 27 | RCT | D0870 s(100 mg/25 mg) vs. D0870 s (10 mg/10 mg) | 23 | 4 |
| Murray PA et al., 1997 | US | 162 | RCT | Itraconazole s 200 mg OD vs. Clotrimazole t 10 mg 5× a day | 120 | 29 |
| Pons V et al., 1997 | US | 167 | RCT | Fluconazole s 100 mg OD vs. Nystatin t 500,000 U QID | NM | NM |
| De Wit S et al., 1998 | Belgium | 40 | RCT | Single dose Fluconazole s 150 mg vs. Itraconazole s 100 mg OD | 32 | 8 |
| Graybill JR et al., 1998 | US | 190 | RCT | Itraconazole s 200 mg OD vs. Fluconazole s 100 mg OD | 166 | 13 |
| Phillips P et al., 1998 | Austria, Belgium, Canada, Germany, Netherlands, Spain, UK | 244 | RCT | Itraconazole s 100 mg OD/BD vs. Fluconazole s 100 mg OD | 221 | 23 |
| Linpiyawan R et al., 2000 | Thailand | 29 | RCT | Clotrimazole t 10 mg 5× Daily vs. Itraconazole s 100 mg BD | 20 | 9 |
| Vazquez JA et al., 2002 | US | 25 | RCT | Alcohol-based Melaleuca t 15 mL QID vs. Alcohol-free Melaleuca t 5 mL QID | 25 | 0 |
| Van Roey J et al., 2004 | Uganda | 357 | RCT | Miconazole t 10 mg OD vs. Ketoconazole s 400 mg OD | 82 | 275 |
| Vazquez JA et al., 2006 | US, Europe, Latin America, Canada, South Africa | 350 | RCT | Posaconazole s 200 mg Day 1, 100 mg OD vs. Fluconazole s 200 mg Day 1, 100 mg OD | 262 | 88 |
| Hamza OJM et al., 2008 | Tanzania | 220 | RCT | Single dose Fluconazole s 750 mg vs. Daily Fluconazole s 150 mg OD | 53 | 167 |
| Wright S.C. et al., 2009 | South Africa | 90 | RCT | Gentian violet t 0.5% TDS vs. Lemon juice t TDS vs. Lemongrass t BD | 22 | 60 |
| Vazquez JA et al., 2010 | US, Canada, South Africa | 578 | RCT | Miconazole t 10 mg OD vs. Clotrimazole t 10 mg 5× Daily | 236 | 341 |
| Mukherjee PK et al., 2017 | South Africa, India, Uganda, Kenya, Botswana, Malawi, Zimbabwe | 221 | RCT | Gentian violet t 0.00165% BD vs. Nystatin t 500,000 U QID | 93 | 128 |
| Intervention | All RCTs | ||
|---|---|---|---|
| RR [95% CI] | p-Value | SUCRA Rank | |
| Fluconazole | Reference | 1 | |
| Posaconazole | 1.01 (0.83,1.23) | 0.91 | 2 |
| Itraconazole | 0.89 (0.74,1.08) | 0.25 | 3 |
| Clotrimazole | 0.87 (0.7,1.06) | 0.19 | 4 |
| Ketoconazole | 0.85 (0.67,1.09) | 0.20 | 5 |
| Miconazole | 0.82 (0.64,1.05) | 0.13 | 6 |
| Gentian violet | 0.61 (0.40,0.94) | 0.02 | 7 |
| Nystatin | 0.59 (0.43,0.82) | 0.001 | 8 |
| Overall inconsistency Chi-square (p value) | 0.92 (0.6312) | ||
| Number of studies | 14 | ||
| Intervention | All RCTs | ||
|---|---|---|---|
| RR [95% CI] | p-Value | SUCRA Rank | |
| Posaconazole | 1.06 (0.71–1.56) | 0.77 | 1 |
| Fluconazole | Reference | 2 | |
| Ketoconazole | 0.95 (0.55–1.65) | 0.88 | 3 |
| Itraconazole | 0.93 (0.71–1.22) | 0.64 | 4 |
| Miconazole | 0.59 (0.34–1.04) | 0.06 | 5 |
| Clotrimazole | 0.54 (0.37–0.76) | 0.001 | 6 |
| Nystatin | 0.10 (0.03–0.27) | 0.00 | 7 |
| Overall inconsistency Chi-square (p value) | 3.35(0.674) | ||
| Number of studies | 11 | ||
| Intervention | All RCTs | ||
|---|---|---|---|
| RR [95% CI] | p-Value | SUCRA Rank | |
| Nystatin | 0.33 (0.03,3.10) | 0.33 | 1 |
| Gentian violet | 0.38 (0.04,3.94) | 0.42 | 2 |
| Itraconazole | 0.89 (0.71,1.12) | 0.30 | 3 |
| Posaconazole | 0.94 (0.81,1.09) | 0.43 | 4 |
| Fluconazole | Reference | 5 | |
| Clotrimazole | 1.07 (0.72,1.61) | 0.22 | 6 |
| Miconazole | 1.12 (0.73,1.73) | 0.59 | 7 |
| Ketoconazole | 1.29 (0.76,2.20) | 0.34 | 8 |
| Overall inconsistency Chi-square (p value) | 1.57 (0.2106) | ||
| Number of studies | 12 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajadurai, S.G.; Maharajan, M.K.; Veettil, S.K.; Gopinath, D. Comparative Efficacy of Antifungal Agents Used in the Treatment of Oropharyngeal Candidiasis among HIV-Infected Adults: A Systematic Review and Network Meta-Analysis. J. Fungi 2021, 7, 637. https://doi.org/10.3390/jof7080637
Rajadurai SG, Maharajan MK, Veettil SK, Gopinath D. Comparative Efficacy of Antifungal Agents Used in the Treatment of Oropharyngeal Candidiasis among HIV-Infected Adults: A Systematic Review and Network Meta-Analysis. Journal of Fungi. 2021; 7(8):637. https://doi.org/10.3390/jof7080637
Chicago/Turabian StyleRajadurai, Shamala Gopal, Mari Kannan Maharajan, Sajesh K. Veettil, and Divya Gopinath. 2021. "Comparative Efficacy of Antifungal Agents Used in the Treatment of Oropharyngeal Candidiasis among HIV-Infected Adults: A Systematic Review and Network Meta-Analysis" Journal of Fungi 7, no. 8: 637. https://doi.org/10.3390/jof7080637
APA StyleRajadurai, S. G., Maharajan, M. K., Veettil, S. K., & Gopinath, D. (2021). Comparative Efficacy of Antifungal Agents Used in the Treatment of Oropharyngeal Candidiasis among HIV-Infected Adults: A Systematic Review and Network Meta-Analysis. Journal of Fungi, 7(8), 637. https://doi.org/10.3390/jof7080637