Paracoccidioidomycosis Diagnosed in Europe—A Systematic Literature Review

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Information Sources and Literature Search
2.2. Eligibility Criteria and Study Selection
2.3. Data Collection Process and Evidence Synthesis
3. Results
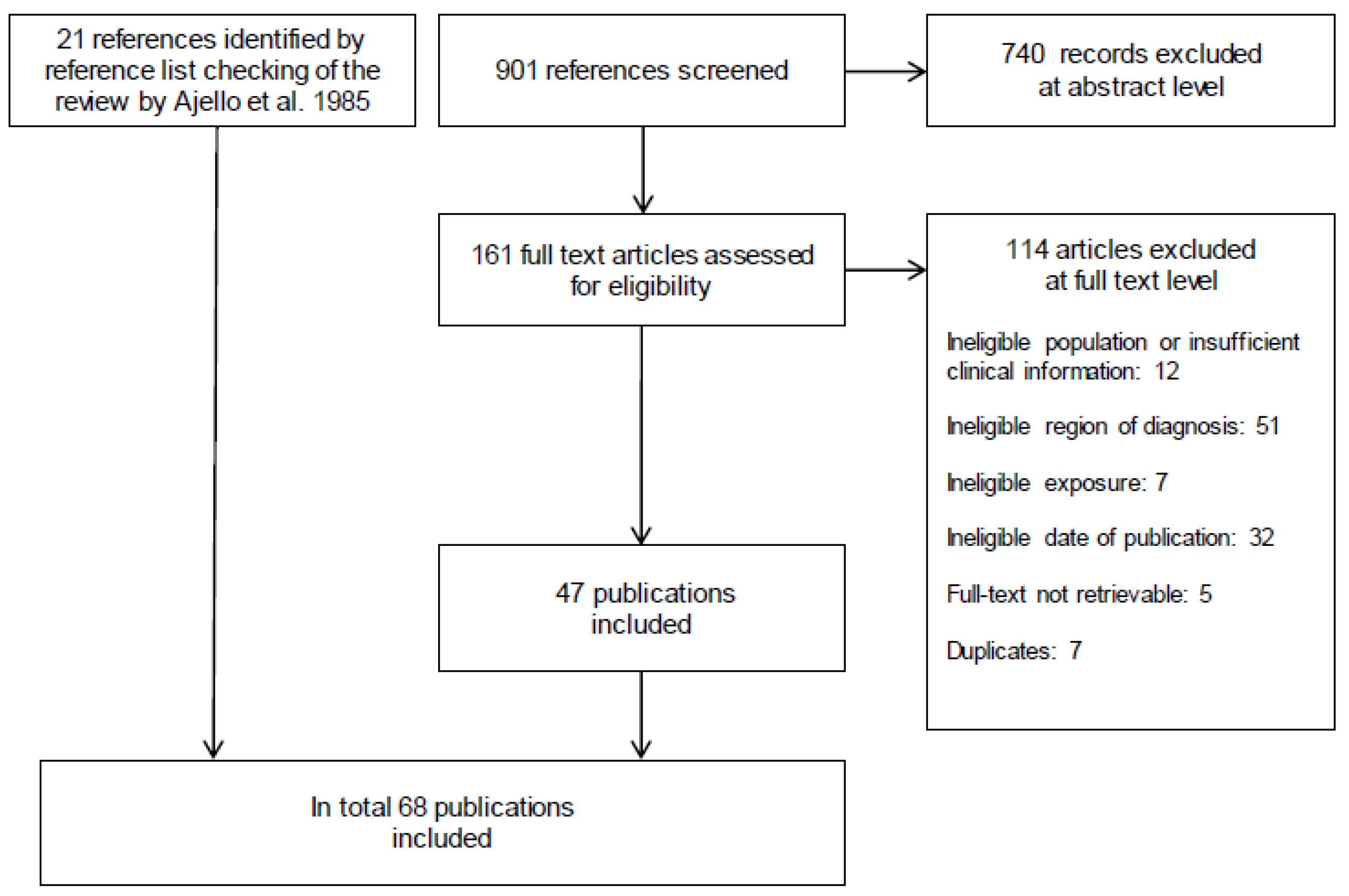
3.1. Study Selection and Characteristics
3.2. Clinical Patient Characteristics
3.3. Differential Diagnosis
3.4. Diagnostic Work-up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| PCR | polymerase chain reaction |
| PCM | paracoccidioidomycosis |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
Appendix A

{kind=link}
{kind=link}
| Search Number | Query | Results |
|---|---|---|
| 1 | “Paracoccidioidomycosis” [Mesh] | 1833 |
| 2 | Paracoccidioidomycos* [tiab] | 1782 |
| 3 | Paracoccidioides brasiliensis [tiab] | 1611 |
| 4 | paracoccidioidal granuloma [tiab] | 9 |
| 5 | south american blastomycosis [tiab] | 272 |
| 6 | #1 OR #2 OR #3 OR #4 OR #5 | 2858 |
| 7 | “Europe” [Mesh] | 1,408,827 |
| 8 | “Emigrants and Immigrants” [Mesh] | 12,277 |
| 9 | “Travel” [Mesh:NoExp] | 24,916 |
| 10 | (Albania* [tiab] OR Andorra* [tiab] OR Armenia* [tiab] OR Austria* [tiab] OR Azerbaijan* [tiab] OR Belarus* [tiab] OR Belgi* [tiab] OR Bosnia* [tiab] OR Herzegov* [tiab] OR Bulgaria* [tiab] OR Croatia* [tiab] OR Cypr* [tiab] OR Czech [tiab] OR Denmark [tiab] OR danish [tiab] OR Estonia* [tiab] OR Finland [tiab] OR finnish [tiab] OR France [tiab] OR french [tiab] OR Georgia* [tiab] OR German* [tiab] OR Greece [tiab] OR greek [tiab] OR Hungar* [tiab] OR Iceland* [tiab] OR Ireland [tiab] OR irish [tiab] OR Italy [tiab] OR italian [tiab] OR Kazak* [tiab] OR Kosov* [tiab] OR Latvia* [tiab] OR Liechtenstein* [tiab] OR Lithuania* [tiab] OR Luxembourg* [tiab] OR Macedonia* [tiab] OR Malta [tiab] OR maltese [tiab] OR Moldov* [tiab] OR Monac* [tiab] OR Montenegr* [tiab] OR Netherlands [tiab] OR dutch [tiab] OR Norway [tiab] OR norwegian [tiab] OR Poland [tiab] OR polish [tiab] OR Portug* [tiab] OR Romania* [tiab] OR Russia* [tiab] OR San Marino [tiab] OR Serbia* [tiab] OR Slovakia* [tiab] OR Slovenia* [tiab] OR Spain [tiab] OR spanish [tiab] OR Sweden [tiab] OR swedish [tiab] OR Switzerland [tiab] OR swiss [tiab] OR Turkey [tiab] OR turkish [tiab] OR Ukrain* [tiab] OR United Kingdom [tiab] OR britain [tiab] OR british [tiab]) | 1,082,126 |
| 11 | (Albania* [ad] OR Andorra* [ad] OR Armenia* [ad] OR Austria* [ad] OR Azerbaijan* [ad] OR Belarus* [ad] OR Belgi* [ad] OR Bosnia* [ad] OR Herzegov* [ad] OR Bulgaria* [ad] OR Croatia* [ad] OR Cypr* [ad] OR Czech [ad] OR Denmark [ad] OR danish [ad] OR Estonia* [ad] OR Finland [ad] OR finnish [ad] OR France [ad] OR french [ad] OR Georgia* [ad] OR German* [ad] OR Greece [ad] OR greek [ad] OR Hungar* [ad] OR Iceland* [ad] OR Ireland [ad] OR irish [ad] OR Italy [ad] OR italian [ad] OR Kazak* [ad] OR Kosov* [ad] OR Latvia* [ad] OR Liechtenstein* [ad] OR Lithuania* [ad] OR Luxembourg* [ad] OR Macedonia* [ad] OR Malta [ad] OR maltese [ad] OR Moldov* [ad] OR Monac* [ad] OR Montenegr* [ad] OR Netherlands [ad] OR dutch [ad] OR Norway [ad] OR norwegian [ad] OR Poland [ad] OR polish [ad] OR Portug* [ad] OR Romania* [ad] OR Russia* [ad] OR San Marino [ad] OR Serbia* [ad] OR Slovakia* [ad] OR Slovenia* [ad] OR Spain [ad] OR spanish [ad] OR Sweden [ad] OR swedish [ad] OR Switzerland [ad] OR swiss [ad] OR Turkey [ad] OR turkish [ad] OR Ukrain* [ad] OR United Kingdom [ad] OR britain [ad] OR british [ad]) | 5,875,438 |
| 12 | europ* [tiab] OR immigrant* [tiab] OR travel* [tiab] | 383,712 |
| 13 | non endemic [tiab] OR nonendemic [tiab] | 4492 |
| 14 | #13 OR #12 OR #11 OR #10 OR #9 OR #8 OR #7 | 7,173,281 |
| 15 | #6 AND #14 | 204 |
| 16 | (“Animals” [Mesh] NOT “Humans” [Mesh]) | 4,707,502 |
| 17 | #15 NOT #16 | 175 |
| No. | Query | Results |
|---|---|---|
| #1 | ‘south american blastomycosis’/exp OR ‘paracoccidioides brasiliensis’/exp | 3026 |
| #2 | paracoccidioidomycos*:ab,ti OR ‘paracoccidioides brasiliensis’:ab,ti OR ‘paracoccidioidal granuloma’:ab,ti OR ‘south american blastomycosis’:ab,ti | 3075 |
| #3 | #1 OR #2 | 3620 |
| #4 | ‘europe’/exp OR ‘immigrant’/exp OR ‘travel’/exp | 1,695,885 |
| #5 | albania*:ca,ab,ti OR andorra*:ca,ab,ti OR armenia*:ca,ab,ti OR austria*:ca,ab,ti OR azerbaijan*:ca,ab,ti OR belarus*:ca,ab,ti OR belgi*:ca,ab,ti OR bosnia*:ca,ab,ti OR herzegov*:ca,ab,ti OR bulgaria*:ca,ab,ti OR croatia*:ca,ab,ti OR cypr*:ca,ab,ti OR czech:ca,ab,ti OR denmark:ca,ab,ti OR danish:ca,ab,ti OR estonia*:ca,ab,ti OR finland:ca,ab,ti OR finnish:ca,ab,ti OR france:ca,ab,ti OR french:ca,ab,ti OR georgia*:ca,ab,ti OR german*:ca,ab,ti OR greece:ca,ab,ti OR greek:ca,ab,ti OR hungar*:ca,ab,ti OR iceland*:ca,ab,ti OR ireland:ca,ab,ti OR irish:ca,ab,ti OR italy:ca,ab,ti OR italian:ca,ab,ti OR kazak*:ca,ab,ti OR kosov*:ca,ab,ti OR latvia*:ca,ab,ti OR liechtenstein*:ca,ab,ti OR lithuania*:ca,ab,ti OR luxembourg*:ca,ab,ti OR macedonia*:ca,ab,ti OR malta:ca,ab,ti OR maltese:ca,ab,ti OR moldov*:ca,ab,ti OR monac*:ca,ab,ti OR montenegr*:ca,ab,ti OR netherlands:ca,ab,ti OR dutch:ca,ab,ti OR norway:ca,ab,ti OR norwegian:ca,ab,ti OR poland:ca,ab,ti OR polish:ca,ab,ti OR portug*:ca,ab,ti OR romania*:ca,ab,ti OR russia*:ca,ab,ti OR ‘san marino’:ca,ab,ti OR serbia*:ca,ab,ti OR slovakia*:ca,ab,ti OR slovenia*:ca,ab,ti OR spain:ca,ab,ti OR spanish:ca,ab,ti OR sweden:ca,ab,ti OR swedish:ca,ab,ti OR switzerland:ca,ab,ti OR swiss:ca,ab,ti OR turkey:ca,ab,ti OR turkish:ca,ab,ti OR ukrain*:ca,ab,ti OR ‘united kingdom’:ca,ab,ti OR britain:ca,ab,ti OR british:ca,ab,ti | 10,276,132 |
| #6 | europ* OR ‘non endemic’ OR nonendemic OR travel*:ab,ti OR imported:ti | 2,203,591 |
| #7 | immigrant* | 34,244 |
| #8 | #4 OR #5 OR #6 OR #7 | 11,651,119 |
| #9 | #3 AND #8 | 457 |
| #10 | ‘animal’/exp NOT ‘human’/exp | 5,449,241 |
| #11 | #9 NOT #10 | 405 |
| #12 | ‘groups by age’/exp NOT ‘adult’/exp | 2,775,185 |
| #13 | #11 NOT #12 | 397 |
| #14 | ‘case report’/exp OR ‘case study’/exp OR ‘letter’/exp | 3,471,553 |
| #15 | case:ab,ti OR cases:ab,ti | 4,628,697 |
| #16 | ‘review’/exp OR ‘evidence based medicine’/exp | 3,575,830 |
| #17 | review:ab,ti OR systematic:ab,ti OR search*:ab,ti OR ‘meta analy*’:ab,ti OR metaanaly*:ab,ti | 2,588,995 |
| #18 | #14 OR #15 OR #16 OR #17 | 10,847,515 |
| #19 | #13 AND #18 | 256 |
| Author, Year | Symptoms and Signs | Differential Diagnosis | Specimen for Histopathology | Histo-Logy 1 | Micro-Biology 2 | Sero-Logy | PCR |
|---|---|---|---|---|---|---|---|
| AUSTRIA | |||||||
| Wagner et al. 2016 [21] | Chest and abdominal pain, weight loss, night sweats, cough | Tuberculosis | Left adrenal gland biopsy, extirpation of a right cervical lymph node | + | + | NR | + |
| Mayr et al. 2004 [22] | Cough, lymphadenopathy, weight loss | Tuberculosis, Wegener’s granulomatosis, sarcoidosis, mycosis | Lung biopsy | + | + | + | NR |
| BULGARIA | |||||||
| Balabanov et al. 1964 [23] | Ulcerous oral and cutaneous lesions, lymphadenopathy | Tuberculosis | Peribuccal lesion biopsy | + | + | NR | NR |
| GERMANY | |||||||
| Kayser et al. 2019 [24] | Cough, dyspnea | Sarcoidosis, histoplasmosis | Lung biopsy | + | + | + | + |
| Slevogt et al. 2004 [25] | Bilateral cervical and axillary lymphadenopathy, weight loss | Tuberculosis | Cervical lymph node biopsy | + | + | NR | NR |
| Horré et al. 2002 [26] | Erythematous and swollen lips, mucocutaneous pustules and ulcerations, oral nodules, occasional night sweats | Leishmaniosis, tropical pulmonary mycosis, gammopathy | Oral lesion biopsy | + | + | + | + |
| Köhler et al. 1988 [27] | Cheilitis, erosive stomatitis, loss of teeth, dysphagia, aphonia, cough, night sweats, weight loss | Tropical disease | NR | NR | + | + | NR |
| Neveling 1988 [28] | Flue like symptoms, dry cough | Coccidiosis, histoplasmosis, North American blastomycosis | NR | NR | NR | + | NR |
| NR | NR | NR | NR | NR | + | ||
| NR | NR | NR | NR | NR | + | ||
| Braeuninger et al. 1985 [29], Hastra et al. 1985 [30] | Flue like symptoms, cervical lymphadenopathy, skin lesions, cough, dyspnea, pain in the left leg | Tuberculosis, sarcoidosis | Lymph node biopsy | + | + | + | NR |
| Altmeyer 1976 [31] | Respiratory insufficiency, cervical lymphadenopathy, painful infiltrations of the soft palate, hypersalivation, ulcerations of the feet, weight loss, dysphagia, dysphonia | Tuberculosis, Wegner’s granulomatosis | Lung and skin lesion biopsy | + | − | NR | NR |
| PORTUGAL | |||||||
| Ferreira et al. 2017 [32] | Labial lesion, dry cough, inguinal and axillary lymphadenopathy, weight loss | Cryptococcosis | Lip lesion and lung biopsy, inguinal lymph node resection | + | − | NR | + |
| Coelho et al. 2013 [33] | Odynophagia, dysphagia, irregular and ulcerated oral mucosa | NR | Oropharyngeal mucosa biopsy | + | NR | NR | NR |
| Alves et al. 2013 [34] | Skin lesion, oral mucosal ulcerations | Coccidioidomycosis, cutaneous tuberculosis | Skin lesion and oral mucosa biopsy | + | + | NR | NR |
| Armas et al. 2012 [35] | Ulcerated skin and nasal mucosa lesion | NR | Skin lesion biopsy | + | + | NR | NR |
| Carvalho et al. 2009 [36] | Fever, epigastric pain, anorexia, fatigue, lymphadenopathy, skin lesions | Skin biopsy and lymph node | + | NR | NR | NR | |
| Villar et al. 1963 [37] | Full-text not available | ||||||
| Oliveira et al. 1960 [38] | Full-text not available | ||||||
| SPAIN | |||||||
| Chamorro-Tojeiro et al. 2020 [20] | Fever, arthralgia, myalgia, dyspnea, dry cough, sweating, general cutaneous rash | Bacterial respiratory infection | NR | NR | − | + | NR |
| Agirre et al. 2019 [19] | Fever, productive cough, exertional dyspnea | Bacterial respiratory infection | NR | NR | − | + | NR |
| Fever, myalgia, asthenia | NR | NR | NR | − | + | NR | |
| Molina-Morant et al. 2018 [18] | NR | NR | NR | NR | NR | NR | NR |
| Navascués et al. 2013 [39] | Productive cough, weight loss, asthenia, lymphadenopathy, skin lesions | NR | Lung biopsy | + | − | + | + |
| Buitrago et al. 2011 [40] 3 | Fever, asthenia, ulcerated pustular skin lesions, extremities | NR | Skin biopsy | + | NR | + | + |
| Productive cough | NR | NR | + | NR | + | + | |
| NR | NR | Cerebral biopsy | + | NR | + | + | |
| NR | NR | NR | + | NR | + | + | |
| NR | NR | Lung biopsy | NR | + | NR | + | |
| NR | NR | Oral mucosa biopsy | + | NR | + | + | |
| Pujol-Riqué et al. 2011 [41] | Productive cough, hemoptysis, night sweats, skin lesions | Sarcoidosis | Lung and skin biopsy | − | + | NR | NR |
| Ramírez-Olivencia et al. 2010 [42] | Fever, dyspnea, productive cough, hemoptysis, night sweats, loss of appetite, weight loss | NR | Lung biopsy | NR | − | + | + |
| Botas-Velasco et al. 2010 [43] | Cough, fever, weight loss, retromolar mass | Sarcoidosis | Retromolar mass and laryngeal biopsy | + | + | + | NR |
| Mayayo et al. 2007 [44] | Skin lesions | Blastomycosis | Skin lesion biopsy | + | NR | NR | NR |
| López Castro et al. 2005 [45] | Dyspnea, dry cough, fever, weight loss, skin lesions | Sarcoidosis | Lung and skin biopsy | + | NR | − | NR |
| Ginarte et al. 2003 [46] | Ulcerative lesions from upper left jaw to labial mucosa and nasal grave | Squamous cell carcinoma | Lesion biopsy | + | + | + | NR |
| Ulcerative lesions left cheek mucosa, periodontitis with loss of several teeth | Tuberculosis, squamous cell carcinoma | Lesion biopsy | + | + | NR | NR | |
| Mass and ulcerative lesions in cheek mucosa | Squamous cell carcinoma | Lesion biopsy | + | + | NR | NR | |
| Garcia Bustínduy et al. 2000 [47] | Ulcerative skin lesion | NR | Skin lesion biopsy | + | + | + | NR |
| Del Pozo et al. 1998 [48] | Lesions upper labial mucosa and nasal fossa | NR | Lesion biopsy | + | + | NR | NR |
| Garcia et al. 1997 [49] | Lesions of labial and palatal mucosa | NR | Lesion biopsy | + | + | + | NR |
| Pereiro et al. 1996 [50] | Tumoral mass of the upper jaw, ulcerated lesion in the upper left jaw, extended to the lip mucosa and the nasal grave | Epidermoid carcinoma | Lesion biopsy | + | + | + | NR |
| Miguélez et al. 1995 [17] | Fever, weight loss, dyspnea, ulcerated mass right tonsil, lymphadenopathy | Pulmonary fibrosis | Ulcerated mass biopsy | + | + | NR | NR |
| Palatal mass, cervical lymphadenopathy | NR | Palatal mass biopsy | + | + | NR | NR | |
| Pereiro Miguens et al. 1987 [16] | Oral mucosal lesions, gingivitis | Tuberculosis | Mucosa biopsy | + | + | + | NR |
| Simon Merchán et al. 1970 [15] | Full-text not available | ||||||
| Pereiro Miguens et al. 1974 [14], Pereiro Miguens et al. 1972 [51] | Epididymitis, gingivitis, oral ulcerative lesion | Tuberculosis | Epididymis and oral lesion biopsy | + | + | + | NR |
| Asthenia, ulcerative oral lesions, labial edema | NR | Oral lesion biopsy | + | + | NR | NR | |
| Vivancos et al. 1969 [13] | Oral mucosal lesions | Pseudoneoplasia | Oral lesion biopsy | + | + | NR | NR |
| GREAT BRITAIN | |||||||
| De Cordova et al. 2012 [52] | Submandibular mass, oral ulcerative lesions | NR | Oral lesion and submandibular mass biopsy | + | + | NR | NR |
| Sierra et al. 2011 [53] | Dyspnea, lip lesion, ulcer on tonsil and uvula | Malignancy, sarcoidosis, squamous cell carcinoma | Lip lesion excision, ulcer biopsy | + | NR | + | NR |
| Walker et al. 2008 [54] | Cough, dyspnea, plantar pruritus, painful skin lesions on his legs, face and feet, hepatomegaly, weight loss | NR | Skin biopsy | + | + | + | NR |
| Bowler et al. 1986 [55] | Cough, dyspnea, and wheeze on exertion | Lymphangitis carcinomatosa | Lung biopsy | + | NR | + | NR |
| Symmers 1966 [56] | Asymptomatic | NR | Spleen (autopsy) | + | NR | NR | NR |
| Skin ulceration | NR | Skin lesion excision | + | NR | NR | NR | |
| ITALY | |||||||
| Borgia et al. 2000 [57] | Fever, pain, and inflammation of left knee | Malignancy | Left femur biopsy | + | + | NR | NR |
| Pecoraro et al. 1998 [58] | Weight loss, night sweat, pain left knee | NR | Left femur biopsy | + | NR | NR | NR |
| Solaroli et al. 1998 [59] | Skin lesion, asthenia, fever, loss of vision | NR | Skin lesion excision | + | + | NR | NR |
| Fulciniti et al. 1996 [60] | Weight loss, night, sweats, pain in left knee | Metastatic lung cancer | Left femur biopsy | + | + | NR | NR |
| Cuomo et al. 1985 [61] | Productive cough, weight loss, asthenia, skin lesions | Tuberculosis, lupus vulgaris | Lung and skin lesion biopsy | + | + | + | NR |
| Benoldi et al. 1985 [62] | Ulcerative skin lesions, cough, fatigue, malaise, weight loss | Tuberculosis, lupus vulgaris | Skin lesion biopsy | + | + | + | NR |
| Finzi et al. 1980 [63] | Full-text not available | ||||||
| Velluti et al. 1979 [64] | Cough, dyspnea | Bronchitis, tuberculosis | Lung biopsy | + | + | + | NR |
| Lasagni et al. 1979 [65] | Full-text not available | ||||||
| Scarpa et al. 1965 [66] | Cough, asthenia, weight loss, night sweats, lymphadenitis, ulcerative oral lesions | Tuberculosis | Lymph node and lung biopsy | + | + | NR | NR |
| Schiraldi et al. 1963 [67] | Full-text not available | ||||||
| Molese et al. 1956 [68] | Oral mucosa lesions, cervical lymphadenopathy, fever, cough | Tuberculosis, leishmaniosis, pneumoconiosis, lues, malignancy | Oral mucosa and tonsillar biopsy | + | NR | NR | NR |
| Farris 1955 [69] | Full-text not available | ||||||
| Bertaccini 1934 [70] | Full-text not available | ||||||
| Dalla Favera 1914 [71] | Full-text not available | ||||||
| FRANCE | |||||||
| Heleine et al. 2020 [72] | Skin lesions, ulcero-nodular lesions lips and mouth, cough, fever, inguinal lymphadenopathy, asthenia, weight loss | HIV, tuberculosis | Skin biopsy | − | + | NR | NR |
| Dang et al. 2017 [73] | Nodular slightly painful, nonulcerated lesion of the tongue, cervical lymphadenopathy | NR | Lingual lesion biopsy | + | NR | NR | + |
| Sambourg et al. 2014 [74] | Partially ulcerous and crusted erythematous lesion left auricle extending to the pre-auricular region | Leishmaniosis | Skin lesion biopsy | + | + | − | + |
| Laccourreye et al. 2010 [75] | Dysphonia, laryngitis | Chronic laryngitis | Laryngeal biopsy, removed mucosa | + | + | NR | NR |
| Poisson et al. 2007 [76] | Seizures | Brain tumor | Single cerebral lesion surgically excised | + | + | + | NR |
| NETHERLANDS | |||||||
| Van Damme et al. 2006 [77] | Dyspnea, cough, wheezing, weight loss, tiredness, fever, night sweats, periodontitis, oral ulceration, macrohematuria | Sarcoidosis, bronchiolitis obliterans organizing pneumonia, oral carcinoma | Lung and oral mucosa biopsy | + | + | + | NR |
| NORWAY | |||||||
| Maehlen et al. 2001 [78] | Dizziness, nausea, headache, hearing loss, hemiplegia | Cerebral tuberculosis | Brain biopsy | + | + | NR | NR |
| SWITZERLAND | |||||||
| Stanisic et al. 1979 [79], Wegmann et al. 1959 [80] | Submandibular and cervical lymphadenopathy, oral ulceration | Tuberculosis, Morbus Wegener, lues, bartonellosis, Morbus Hodgkin, neoplasma, blastomycosis, sporotrichosis, cryptococcosis | Oral mucosa and cervical lymph node biopsy | + | + | NR | NR |
References
- Bocca, A.L.; Amaral, A.C.; Teixeira, M.M.; Sato, P.; Yasuda, S.M.A.; Felipe, S.M.S. Paracoccidioidomycosis: Eco-epidemiology, taxonomy and clinical and therapeutic issues. Future Microbiol. 2013, 8, 1177–1191. [Google Scholar] [CrossRef]
- Hrycyk, M.F.; Garces, G.H.; Bosco, S.D.M.G.; de Oliveira, S.L.; Marques, S.A.; Bagagli, E. Ecology of Paracoccidioides brasiliensis, P. lutzii and related species: Infection in armadillos, soil occurrence and mycological aspects. Med. Mycol. 2018, 56, 950–962. [Google Scholar] [CrossRef] [PubMed]
- Turissini, D.A.; Gomez, O.M.; Teixeira, M.M.; McEwen, J.G.; Matute, D.R. Species boundaries in the human pathogen Paracoccidioides. Fungal Genet. Biol. FG B 2017, 106, 9–25. [Google Scholar] [CrossRef]
- Ameen, M.; Talhari, C.; Talhari, S. Advances in paracoccidioidomycosis. Clin. Exp. Dermatol. 2010, 35, 576–580. [Google Scholar] [CrossRef]
- Martinez, R. New trends in paracoccidioidomycosis epidemiology. J. Fungi 2017, 3. [Google Scholar] [CrossRef]
- Shankar, J.; Restrepo, A.; Clemons, K.V.; Stevens, D.A. Hormones and the Resistance of Women to Paracoccidioidomycosis. Clin. Microbiol. Rev. 2011, 24, 296. [Google Scholar] [CrossRef]
- Brummer, E.; Castaneda, E.; Restrepo, A. Paracoccidioidomycosis: An update. Clin. Microbiol. Rev. 1993, 6, 89–117. [Google Scholar] [CrossRef]
- Wanke, B.; Aidé, M.A. Chapter 6-paracoccidioidomycosis. J. Bras. Pneumol. 2009, 35, 1245–1249. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Salzer, H.J.F.; Burchard, G.; Cornely, O.A.; Lange, C.; Rolling, T.; Schmiedel, S.; Libman, M.; Capone, D.; Le, T.; Dalcolmo, M.P.; et al. Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease. Respiration 2018, 96, 283–301. [Google Scholar] [CrossRef]
- Ajello, L.; Polonelli, L. Imported paracoccidioidomycosis: A public health problem in non-endemic areas. Eur. J. Epidemiol. 1985, 1, 160–165. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Innovation, V.H. Covidence Systematic Review Software. Available online: www.covidence.org (accessed on 2 June 2019).
- Vivancos, G.; Marrero, B.; Hernández, B.; Padrón, G. La blastomicosis sudamericana en España. Primera observación en las Islas Canarias. In Proceedings of the VV. AA. Actas VII Congreso Hispano-Portugués de Dermatología Médico Quirúrgica, Granada, Spain, 22–25 October 1969; pp. 330–335. [Google Scholar]
- Pereiro, M.M. Two cases of South American blastomycosis observed in Spain. Actas Dermo Sifiliogr. 1974, 65, 509–522. [Google Scholar]
- Merchán, S.A.; Escudero, R.; Lavin, R. Un caso de blastomicosis sudamericana observado en España. Med. Cutan. Iber. Lat. Am. 1970, 5, 631–636. [Google Scholar]
- Miguens, P.M.; Ferreiros, P.M.M. A propósito de un nuevo caso de paracoccidioidomicosis observado en España. Ver. Iber. Micol. 1987, 4, 149–157. [Google Scholar]
- Miguélez, M.; Amerigo, M.J.; Perera, A.; Rosquete, J. Imported paracoccidioidomycosis. Apropos of 2 cases. Med. Clin. (Barc) 1995, 105, 756. [Google Scholar]
- Morant, M.D.; Montalvá, S.A.; Salvador, F.; Avilés, S.A.; Molina, I. Imported endemic mycoses in Spain: Evolution of hospitalized cases, clinical characteristics and correlation with migratory movements, 1997–2014. PLoS Negl. Trop. Dis. 2018, 12, 6245. [Google Scholar] [CrossRef]
- Agirre, E.; Osorio, A.; de Tejerina, C.F.J.M.; Arrondo, R.F.; Bermejo, S.Y. Bilateral interstitial pneumonia after recent trip to Peru. Enferm. Infecc. Microbiol. Clin. 2019, 37, 609–610. [Google Scholar] [CrossRef] [PubMed]
- Tojeiro, C.S.; Sarria, G.A.; Pedrosa, E.G.G.; Buitrago, M.J.; Vélez, L.R. Acute Pulmonary Paracoccidioidomycosis in a Traveler to Mexico. J. Travel. Med. 2020. [Google Scholar] [CrossRef]
- Wagner, G.; Moertl, D.; Eckhardt, A.; Sagel, U.; Wrba, F.; Dam, K.; Willinger, B. Chronic Paracoccidioidomycosis with adrenal involvement mimicking tuberculosis—A case report from Austria. Med. Mycol. Case Rep. 2016, 14, 12–16. [Google Scholar] [CrossRef]
- Mayr, A.; Kirchmair, M.; Rainer, J.; Rossi, R.; Kreczy, A.; Tintelnot, K.; Dierich, M.P.; Flörl, L.C. Chronic paracoccidioidomycosis in a female patient in Austria. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 916–919. [Google Scholar] [CrossRef]
- Balabanov, K.; Balabanoff, V.A.; Angelov, N. South American Blastomycosis in a Bulgarian Laborer Returning after 30 Years in Brazil. Mycopathol. Mycol. Appl. 1964, 24, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Kayser, M.; Rickerts, V.; Drick, N.; Gerkrath, J.; Kreipe, H.; Soudah, B.; Welte, T.; Suhling, H. Chronic progressive pulmonary paracoccidioidomycosis in a female immigrant from Venezuela. Ther. Adv. Respir. Dis. 2019, 13, 4913. [Google Scholar] [CrossRef]
- Slevogt, H.; Tintelnot, K.; Seybold, J.; Suttorp, N. Lymphadenopathy in a pregnant woman from Brazil. Lancet 2004, 363, 1282. [Google Scholar] [CrossRef]
- Horré, R.; Schumacher, G.; Alpers, K.; Seitz, H.M.; Adler, S.; Lemmer, K.; De Hoog, G.S.; Schaal, K.P.; Tintelnot, K. A case of imported paracoccidioidomycosis in a German legionnaire. Med. Mycol. 2002, 40, 213–216. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kohler, C.; Klotz, M.; Daus, H.; Schwarze, G.; Dette, S. Visceral paracoccidioidomycosis in a gold-digger from Brasil. Mycoses 1988, 31, 395–403. [Google Scholar] [CrossRef]
- Neveling, F. Paracoccidioidomycosis infections caused by an adventure vacation in the Amazon. Prax. Klin. Pneumol. 1988, 42, 722–725. [Google Scholar] [PubMed]
- Brauninger, W.; Hastra, K.; Rubin, R. Paracoccidioidomycosis, an imported tropical disease. Hautarzt 1985, 36, 408–411. [Google Scholar] [PubMed]
- Hastra, K.; Schulz, V.; Brauninger, A. South American blastomycosis in the Federal Republic of Germany. Prax. Klin. Pneumol. 1985, 39, 905. [Google Scholar]
- Altmeyer, P. A contribution to South American blastomycosis Blastomyces brasiliensis. Mykosen 1976, 19, 265–270. [Google Scholar] [CrossRef]
- Ferreira, A.; Silva, A.; Cruz, M.; Sabino, R.; Veríssimo, C. Labial lesion in a Portuguese man returned from Brazil-The role of molecular diagnosis. Travel Med. Infect. Dis. 2018, 22, 80–81. [Google Scholar] [CrossRef]
- Coelho, H.; Vaz De Castro, J.; Brito, D.; Oliveira Neta, J.; Aleixo, M.J.; André, C.; Antunes, L.; Brito, M.J. A case of imported paracoccidioidomycosis. Virchows Arch. 2013, 463, 170–171. [Google Scholar]
- Alves, R.; Marote, J.; Armas, M.; Freitas, C.; Almeida, L.S.; Sequeira, H.; Gomes, M.A.; Verissimo, C.; Rosado, M.L.; Faria, A. Paracoccidioidiomycosis: Case report. Med. Cutanea Ibero Lat. Am. 2013, 41, 63–66. [Google Scholar]
- Armas, M.; Ruivo, C.; Alves, R.; Gonçalves, M.; Teixeira, L. Pulmonary paracoccidioidomycosis: A case report with high-resolution computed tomography findings. Rev. Port. Pneumol. 2012, 18, 190–193. [Google Scholar] [CrossRef]
- Carvalho, R.; Branquinho, F.; Theias, R.; Perloiro, M. Paracoccidiodomicose Brasiliensis: A propósito de um caso clínico. Rev. Soc. Port. Med. Int. 2009, 16, 170–172. [Google Scholar]
- Villar, T.; Neves, H.; Soares, N.; Duarte, S. Blastomicose sul-americana. Forma mista, cutâneo-mucosa e pulmonar. J. Médico 1963, 51, 181–194. [Google Scholar]
- Oliveria, H.; Baptista, A. Um caso de blastomicosis Sudamericana (23 anos in Cubacao. A cao de sulfametoxipiridoxina). Coimbra Med. 1960, 7, 661. [Google Scholar]
- Navascués, A.; Rubio, M.T.; Monzón, F.J. Paracoccidioidomycosis in an Ecuadorian immigrant. Enferm. Infecc. Microbiol. Clin. 2013, 31, 415–416. [Google Scholar] [CrossRef]
- Buitrago, M.J.; Martínez, B.L.; Castelli, M.V.; Tudela, R.J.L.; Estrella, C.M. Histoplasmosis and paracoccidioidomycosis in a non-endemic area: A review of cases and diagnosis. J. Travel Med. 2011, 18, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Riqué, P.M.; Ruiz, S.; Tarrés, A.C.; Cañete, C. Pulmonary mycosis caused by Paracoccidioides brasiliensis: Dangerous confusion with sarcoidosis. Radiologia 2011, 53, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Olivencia, R.G.; Rubio, R.O.; González, R.P.; Herrero, D.M.; Puente, P.S. Paracoccidioidomycosis in a Spanish missionary. J. Travel Med. 2010, 17, 139–140. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Velasco, B.M.; Diaz, J.F.; de la Duccase, O.T.V.; García, M.C. Imported paracoccidioidomycosis in Spain. Enferm. Infecc. Microbiol. Clin. 2010, 28, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Mayayo, E.; Aracil, G.V.; Torres, F.B.; Mayayo, R.; Domínguez, M. Report of an imported cutaneous disseminated case of paracoccidioidomycosis. Rev. Iberoam. Micol. 2007, 24, 44–46. [Google Scholar] [CrossRef]
- Castro, L.J.; Perez, B.J.J.; Quintairos, S.C.; Pestonit, C.M. Infection by Paracoccidioides brasiliensis in an immigrant from Venezuela. Med. Clin. (Barc) 2005, 125, 39. [Google Scholar] [CrossRef] [PubMed]
- Ginarte, M.; Pereiro, M., Jr.; Toribio, J. Imported paracoccidioidomycosis in Spain. Mycoses 2003, 46, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Bustínduy, G.M.; Guimerá, F.; Arévalo, P.; Castro, C.; Sáez, M.; Alom, D.S.; Noda, A.; Flores, D.L.; Montelongo, G.R. Cutaneous primary paracoccidioidomycosis. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 113–117. [Google Scholar] [CrossRef]
- Del Pozo, J.; Almagro, M.; Pereiro, M.; Martinez, W.; Arnal, F.; Silva, G.J.; Fonseca, E. Paracoccidioidomycosis. Report of a case imported into spain. Actas Dermo Sifiliogr. 1998, 89, 121–124. [Google Scholar]
- García, A.; Suárez, M.M.; Gándara, J.M.; Pereiro, M., Jr.; Pardo, F.; Diz, P. Importación de paracoccidioidomicosis a España por un emigrante gallego en Venezuela. Med. Oral 1997, 2, 39–43. [Google Scholar] [PubMed]
- Pereiro, M., Jr.; Pereiro, M.; Garcia, A.G.; Toribio, J. Immunological features of chronic adult paracoccidioidomycosis: Report of a case treated with fluconazole. Acta Derm. Venereol. 1996, 76, 84–85. [Google Scholar] [PubMed]
- Miguens, P.M.; Nunez, V.R.; Nunez, S.J.M. Blastomicosis sudamericana. Rev. Med. Galicia 1972, 10, 631–636. [Google Scholar]
- De Cordova, J.; Richards, O.; Southall, P.; Muscat, I.; Siodlak, M. First reported case of Paracoccidiodomicosis in Great Britain. Clin. Otolaryngol. 2012, 37, 14. [Google Scholar]
- Sierra, R.; Houston, A.; Appleton, M.; Lucas, S.; Legg, J. Paracoccidioides brasiliensis, an undeclared import. J. Infect. 2011, 63, 505–506. [Google Scholar] [CrossRef]
- Walker, S.L.; Pembroke, A.C.; Lucas, S.B.; Lopez, V.F. Paracoccidioidomycosis presenting in the U.K. Br. J. Dermatol. 2008, 158, 624–626. [Google Scholar] [CrossRef]
- Bowler, S.; Woodcock, A.; Da Costa, P.; Warwick, T.M. Chronic pulmonary paracoccidioidomycosis masquerading as lymphangitis carcinomatosa. Thorax 1986, 41, 72–73. [Google Scholar] [CrossRef][Green Version]
- Symmers, W.S. Deep-seated fungal infections currently seen in the histopathologic service of a medical school laboratory in Britain. Am. J. Clin. Pathol. 1966, 46, 514–537. [Google Scholar] [CrossRef]
- Borgia, G.; Reynaud, L.; Cerini, R.; Ciampi, R.; Schioppa, O.; Dello Russo, M.; Gentile, I.; Piazza, M. A case of paracoccidioidomycosis: Experience with long-term therapy. Infection 2000, 28, 119–120. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Solaroli, C.; Alol, F.; Becchis, G.; Zina, A.; Pippione, M. Paracoceidioidomycosis. Description of a case. G. Ital. Dermatol. Venereol. 1998, 133, 51–54. [Google Scholar]
- Fulciniti, F.; Troncone, G.; Fazioli, F.; Vetrani, A.; Zeppa, P.; Manco, A.; Palombini, L. Osteomyelitis by Paracoccidioides brasiliensis (south american blastomycosis): Cytologic diagnosis on fine-needle aspiration biopsy smears: A case report. Diagn. Cytopathol. 1996, 15, 442–446. [Google Scholar] [CrossRef]
- Cuomo, A.; Capra, R.; Di Gregorio, A.; Garavaldi, G. On one case of South American Blastomycosis with peculiar evolution. Riv. Patol. Clin. Tuberc. Pneumol. 1985, 56, 453–472. [Google Scholar]
- Benoldi, D.; Alinovi, A.; Pezzarossa, E. Paracoccidioidomycosis (South American blastomycosis): A report of an imported case previously diagnosed as tuberculosis. Eur. J. Epidemiol. 1985, 1, 150–152. [Google Scholar] [CrossRef]
- Finzi, F.F.; Bubola, D.; Lasagni, A. Blastomicosi sudamericana. Ann. Ital. Dermatol. Clin. Sper. 1980, 34, 277–285. [Google Scholar]
- Velluti, G.; Mazzoni, A.; Kaufman, L.; Covi, M. Physiopathological, clinical and therapeutical notes on a case of paracoccidioidomycosis. Gazz. Med. Ital. 1979, 138, 297–304. [Google Scholar]
- Lasagni, A.; Innocenti, M. Su un caso di blastomicosi sud americana. Chemioter. Antimicrob. 1979, 2, 188–190. [Google Scholar]
- Scarpa, C.; Nini, G.; Gualdi, G. Clinico-radiological contribution to the study of paracoccidioidomycosis. Minerva Dermatol. 1965, 40, 413–421. [Google Scholar] [PubMed]
- Schiraldi, O.; Grimaldi, N. Granulomatosi paracoccidioide. Policlinico 1963, 70, 65–84. [Google Scholar]
- Molese, A.; Pagano, A.; Pane, A.; Vingiani, A. Case of paracoccidioidal granulomatosis; Lutz-Splendore-Almeida disease. Riforma Med. 1956, 70, 1009–1014. [Google Scholar]
- Farris, G. Report on a case of paracoccidioidomycosis (so-called Brazilian blastomycosis). Atti della Società italiana di dermatologia e sifilografia e delle sezioni interprovinciali. Soc. Ital. Dermatol. Sifilogr. 1955, 96, 321–358. [Google Scholar]
- Bertaccini, G. Contributo allo studio della cosi detta ≪blastomicosa sud-americana≫. Giorn. Ital. Dermatol. Sifil. 1934, 75, 783–828. [Google Scholar]
- Dalla Favera, G.B. Per la conoscenza della cosidetta blastomicosi cutanea (con un’osservazione personale di oidiomicosi (Gilchrist, Bushke) zimonematosi (de Beurmann et Gougerot). Giorn. Ital. Mal. Ven. Pelle 1914, 55, 650–729. [Google Scholar]
- Heleine, M.; Blaizot, R.; Cissé, H.; Labaudinière, A.; Guerin, M.; Demar, M.; Blanchet, D.; Couppie, P. A case of disseminated paracoccidioidomycosis associated with cutaneous lobomycosis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e18–e20. [Google Scholar] [CrossRef] [PubMed]
- Dang, J.; Chanson, N.; Charlier, C.; Bonnal, C.; Jouvion, G.; Goulenok, T.; Papo, T.; Sacre, K. A 54-Year-Old Man with Lingual Granuloma and Multiple Pulmonary Excavated Nodules. Chest 2017, 151, e13–e16. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sambourg, E.; Demar, M.; Simon, S.; Blanchet, D.; Dufour, J.; Marie, S.D.; Fior, A.; Carme, B.; Aznar, C.; Couppie, P. Paracoccidioidomycosis of the external ear. Ann. Dermatol. Venereol. 2014, 141, 514–517. [Google Scholar] [CrossRef]
- Laccourreye, O.; Mirghani, H.; Brasnu, D.; Badoual, C. Imported acute and isolated glottic paracoccidioidomycosis. Ann. Otol. Rhinol. Laryngol. 2010, 119, 89–92. [Google Scholar] [CrossRef]
- Poisson, D.M.; Heitzmann, A.; Mille, C.; Muckensturm, B.; Dromer, F.; Dupont, B.; Hocqueloux, L. Paracoccidioides brasiliensis in a brain abscess: First French case. J. Mycol. Med. 2007, 17, 114–118. [Google Scholar] [CrossRef]
- Van Damme, P.A.; Bierenbroodspot, F.; Telgt, D.S.C.; Kwakman, J.M.; De Wilde, P.C.M.; Meis, J.F.G.M. A case of imported paracoccidioidomycosis: An awkward infection in the Netherlands. Med. Mycol. 2006, 44, 13–18. [Google Scholar] [CrossRef][Green Version]
- Maehlen, J.; Strøm, E.H.; Gerlyng, P.; Heger, B.H.; Orderud, W.J.; Syversen, G.; Solgaard, T. South American blastomycosis--a differential diagnosis to tuberculous meningitis. Tidsskr. Nor. Laegeforening 2001, 121, 33–34. [Google Scholar]
- Stanisic, M.; Wegmann, T.; Kuhn, E. South American blastomycosis (paracoccidioidomycosis) in Switzerland. Clinical course and morphological findings in a case following long-term therapy. Schweiz. Med. Wochenschr. 1979, 109, 693–699. [Google Scholar] [PubMed]
- Wegmann, T.; Zollinger, H.U. Tuberkuloide Granulome in Mundschleimhaut und Halslymphknoten: Sudamerikanische Blastomykose. Schweiz. Med. Wochenschr. 1959, 89, 2–8. [Google Scholar]
- Bonifaz, A.; González, V.D.; Ortiz, P.A.M. Endemic systemic mycoses: Coccidioidomycosis, histoplasmosis, paracoccidioidomycosis and blastomycosis. J. Ger. Soc. Dermatol. 2011, 9, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Buitrago, M.J.; Estrella, C.M. Current epidemiology and laboratory diagnosis of endemic mycoses in Spain. Enferm. Infecc. Microbiol. Clin. 2012, 30, 407–413. [Google Scholar] [CrossRef]
- Júnior, Q.R.; Tde, G.A.; Massucio, R.A.; De Capitani, E.M.; Sde, R.M.; Balthazar, A.B. Association between paracoccidioidomycosis and tuberculosis: Reality and misdiagnosis. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. Tisilogia 2007, 33, 295–300. [Google Scholar] [CrossRef]
- Telles, Q.F.V.; Pietrobom, P.P.M.; Júnior, R.M.; Baptista, R.M.; Peçanha, P.M. New Insights on Pulmonary Paracoccidioidomycosis. Semin. Respir. Crit. Care Med. 2020, 41, 53–68. [Google Scholar] [CrossRef]
- Pecoraro, C.; Pinto, A.; Tortora, G.; Ginolfi, F. South American blastomycosis of the lung and bone: A case report. Radiol. Med. 1998, 95, 521–523. [Google Scholar] [PubMed]
- Buitrago, M.J.; Merino, P.; Puente, S.; Lopez, G.A.; Arribi, A.; Oliveira, Z.R.M.; Gutierrez, M.C.; Tudela, R.J.L.; Estrella, C.M. Utility of Real-time PCR for the detection of Paracoccidioides brasiliensis DNA in the diagnosis of imported paracoccidioidomycosis. Med. Mycol. 2009, 47, 879–882. [Google Scholar] [CrossRef] [PubMed][Green Version]


| Inclusion | Exclusion | |
|---|---|---|
| Population |
|
|
|
| |
| Region |
|
|
| Study design |
| - |
| Publication type |
| - |
| Language |
| - |
| Country of Diagnosis | No. of Publications | No. of Reported Cases |
|---|---|---|
| Austria | 2 | 2 |
| Bulgaria | 1 | 1 |
| France | 5 | 5 |
| Germany | 8 | 9 |
| Great Britain | 5 | 6 |
| Italy | 15 | 15 |
| Netherlands | 1 | 1 |
| Norway | 1 | 1 |
| Portugal | 7 | 7 |
| Spain | 21 | 35 1 |
| Switzerland | 2 | 1 |
| Total | 68 | 83 |
| Author, Year | Study Design Language | No. of Cases | Age Years, Gender | Suspected Country of Exposure | Latency Period 1 | Occupation | Affected Organ(s) | Systemic Antimycotic Therapy | Treatment Response |
|---|---|---|---|---|---|---|---|---|---|
| AUSTRIA | |||||||||
| Wagner et al. 2016 [21] | Case report English | 1 | 62, M | Peru | 6 years | Construction worker | Adrenal glands, brain, lung, lymph node | Amphotericin B, itraconazole, posaconazole | Clinical improvement during hospital stay |
| Mayr et al. 2004 [22] | Case report English | 1 | 43, F | Brazil, Venezuela or Mexico | 4 years | Government employee | Lung, lymph node | Amphotericin B, voriconazole | Clinical improvement |
| BULGARIA | |||||||||
| Balabanov et al. 1964 [23] | Case report * French | 1 | 67, M | Brazil | 30 years | Worked in the jungle | Lung, oral mucosa | Sulfonamide, trimethoprim | Complete remission |
| GERMANY | |||||||||
| Kayser et al. 2019 [24] | Case report English | 1 | 57, F | Venezuela | 1 year | NR | Lung | Amphotericin B, itraconazole | Clinical improvement during hospital stay, remained under control |
| Slevogt et al. 2004 [25] | Case report English | 1 | 31, F | Brazil | 10 years | NR | Lymph nodes | Itraconazole | Complete remission |
| Horré et al. 2002 [26] | Case report English | 1 | 61, M | Brazil | 10 years | Legionnaire | Lung, oral mucosa, skin | Itraconazole | Complete remission |
| Köhler et al. 1988 [27] | Case report German | 1 | 49, M | Brazil | 15 years | Gold mine worker | Brain, lung, oral and laryngeal mucosa | Amphotericin B, ketoconazole, itraconazole | Clinical improvement during hospital stay, remained under control |
| Neveling 1988 [28] | Case series German | 3 | 38, F | Brazil | 1 month | Administrative employee | Lung | None | Clinical improvement, remained under control |
| 64, M | Brazil | 1 month | Gardener | Lung | NR | NR | |||
| 45, M | Brazil | 1 month | Librarian | Lung | NR | NR | |||
| Braeuninger et al. 1985 [29], Hastra et al. 1985 [30] | Case report German | 1 | 32, M | Peru | 6 years | NR | Lung, lymph nodes, oral mucosa, skin | Ketoconazole | Clinical improvement |
| Altmeyer 1976 [31] | Case report * German | 1 | 69, M | Paraguay | 22 years | Farm worker | Lung, lymph nodes, oral mucosa, skin | Imidazole | Patient deceased |
| PORTUGAL | |||||||||
| Ferreira et al. 2017 [32] | Case report English | 1 | 46, M | Brazil | 1 month | NR | Lung, lymph nodes, oral mucosa | Itraconazole | Clinical improvement |
| Coelho et al. 2013 [33] | Case report (Abstract only) English | 1 | 63, M | Brazil | 8 years | Gardener | Oral and pharyngeal mucosa | NR | NR |
| Alves et al. 2013 [34] | Case report Portuguese | 1 | 43, M | Venezuela | 6 years | NR | Lung, oral mucosa, skin | Itraconazole | Complete remission |
| Armas et al. 2012 [35] | Case report English | 1 | 43, M | Venezuela | NR | Farm worker | Lung, skin | Itraconazole | Clinical improvement |
| Carvalho et al. 2009 [36] | Case report Portuguese | 1 | 24, M | Brazil | 7 years | Construction worker | Lymph nodes, skin | Itraconazole | Clinical improvement |
| Villar et al. 1963 [37] | Case report ** | 1 | - | Brazil | 37 years | - | - | - | - |
| Oliveira et al. 1960 [38] | Case report ** Portuguese | 1 | - | Brazil | 23 years | - | - | - | - |
| SPAIN | |||||||||
| Chamorro-Tojeiro et al. 2020 [20] | Case report English | 1 | 42, M | Mexico | 6 days | NR | Lung | Itraconazole | Complete remission, remained under control |
| Agirre et al. 2019 [19] | Case series English | 2 | 29, F | Peru | 10 days | NR | Lung, lymph nodes | Itraconazole | Complete remission |
| 31, M | Peru | 10 days | NR | Lung | Itraconazole | Complete remission | |||
| Molina-Morant et al. 2018 [18] | Retrospective observational study English | 25 2 | Median 48 yrs (range 33 to 67), M 16 (64%) | This retrospective study reported 25 cases of paracoccidioidomycosis admitted to Spanish hospitals between 1 January 1997 to 31 December 2014. | |||||
| Navascués et al. 2013 [39] | Case report Spanish | 1 | 47, M | Ecuador | 11 years | NR | Lung, lymph nodes, skin | Amphotericin B, itraconazole | Complete remission |
| Buitrago et al. 2011 [40] | Case series English | 6 | 67, M | Ecuador | NR | ||||
| 57, M | Venezuela | NR | |||||||
| 44, M | Paraguay | NR | |||||||
| 51, M | Paraguay | NR | |||||||
| 31, M | Ecuador | NR | |||||||
| NR, M | NR | NR | |||||||
| Pujol-Riqué et al. 2011 [41] | Case report Spanish | 1 | 48, M | Brazil | 6 years | Worked in the jungle | Lung | Amphotericin B, itraconazole | Complete remission |
| Ramírez-Olivencia et al. 2010 [42] | Case report English | 1 | 56, M | Venezuela | 6 months | NR | Lung | Itraconazole, amphotericin B | Complete remission |
| Botas-Velasco et al. 2010 [43] | Case report Spanish | 1 | 43, M | Ecuador | NR | NR | Lung, oral and laryngeal mucosa | Itraconazole | Clinical improvement; disappearance of oral and laryngeal lesions |
| Mayayo et al. 2007 [44] | Case report English | 1 | 27, M | Ecuador | None | Farmer | Lymph nodes, skin | Itraconazole | Complete remission |
| López Castro et al. 2005 [45] | Case report Spanish | 1 | 63, M | Venezuela | 8 months | Shoemaker | Lung, skin | Amphotericin B | Patient deceased |
| Ginarte et al. 2003 [46] | Case series English | 3 | 72, M | Venezuela | 50 years | NR | Skin | Fluconazole | Remained under control |
| 67, M | Brazil | 1 year | NR | Oral mucosa, teeth | Itraconazole, sulfonamides | Complete remission | |||
| 65, M | Venezuela | 38 years | NR | Oral mucosa | Fluconazole | Remained under control | |||
| Garcia Bustínduy et al. 2000 [47] | Case report English | 1 | 59, M | Venezuela | 1 year | Taxi driver | Skin | Itraconazole | Complete remission |
| Del Pozo et al. 1998 [48] | Case report Spanish | 1 | 50, M | Venezuela | 13 years | NR | Skin, oral and nasal mucosa | Itraconazole | Complete remission |
| Garcia et al. 1997 [49] | Case report Spanish | 1 | 72, M | Venezuela | 50 years | NR | Lung, oral mucosa, skin | Fluconazole | Complete remission |
| Pereiro et al. 1996 [50] | Case report English | This case was also described by Ginarte et al. 2003 [46] and is therefore not presented here again. | |||||||
| Miguélez et al. 1995 [17] | Case report Spanish | 2 | 44, M | Venezuela | 2 years | NR | Brain, lung, lymph nodes | Itraconazole | Patient deceased (tuberculosis coinfection) |
| 53, M | Venezuela | 18 months | NR | Lung, lymph nodes, oral mucosa | Itraconazole | Clinical improvement | |||
| Pereiro Miguens et al. 1987 [16] | Case report Spanish | 1 | 51, M | Venezuela | 23 years | Construction worker | Oral mucosa, skin | Ketoconazole | Clinical improvement |
| Simon Merchán et al. 1970 [15] | Case report ** | 1 | - | Venezuela | 2 years | - | - | - | - |
| Pereiro Miguens 1974 [14], Pereiro Miguens et al. 1972 [51] | Case report * Spanish | 2 | 44, M | Venezuela | 7 years | NR | Lung, oral mucosa | Sulfonamide, trimethoprim | Clinical improvement |
| 49, M | Venezuela | 8 years | Gardener | Oral mucosa | Sulfonamide, trimethoprim | Clinical improvement | |||
| Vivancos et al. 1969 [13] | Case report * Spanish | 1 | 44, M | Venezuela | NR | Farmer | Oral mucosa | Sulfamethoxazole/trimethoprim, amphotericin B | Complete remission |
| GREAT BRITAIN | |||||||||
| De Cordova et al. 2012 [52] | Case report (Abstract only) English | 1 | 52, M | Venezuela | NR | Butcher | Oral mucosa | Itraconazole | Complete remission |
| Sierra et al. 2011 [53] | Case report (Abstract only) English | 1 | 77, M | Ecuador | NR | NR | Lung, lymph nodes, oral mucosa, skin | Itraconazole | NR |
| Walker et al. 2008 [54] | Case report English | 1 | 51, M | Venezuela | None | Accountant | Lung, oral mucosa, skin | Itraconazole | Clinical improvement, cutaneous lesions cleared |
| Bowler et al. 1986 [55] | Case report English | 1 | 57, F | Argentina, Venezuela | 17 years | Clerk | Lung | NR | NR |
| Symmers 1966 [56] | Case report * English | 1 | 42, M | Brazil | NR | Engineer | Skin | NR | NR |
| 1 | 46, M | Brazil | None | Businessman | Spleen (autopsy) | No therapy | Patient deceased (acute heart failure) | ||
| ITALY | |||||||||
| Borgia et al. 2000 [57] | Case report English | 1 | 61, M | Venezuela | NR | House- painter | Bones, lung | Itraconazole | Clinical improvement |
| Pecoraro et al. 1998 [58] | Case report Italian | 1 | 60, M | Venezuela | NR | Coffee plantations worker | Bones, lung | Ketoconazole | Clinical improvement |
| Solaroli et al. 1998 [59] | Case report Italian | 1 | 49, M | Brazil | NR | NR | Brain, lung, skin | Itraconazole | Clinical improvement |
| Fulciniti et al. 1996 [60] | Case report English | 1 | 60, M | Venezuela | NR | NR | Bones, lung | Itraconazole | Clinical improvement, remained under control |
| Cuomo et al. 1985 [61] | Case report Italian | 1 | 37, M | Venezuela | 2 years | Butcher | Lung, skin | Ketoconazole | Clinical improvement |
| Benoldi et al. 1985 [62] | Case report * English | 1 | 41, M | Venezuela | Few months | Butcher | Lung, lymph nodes, skin | Ketconazole, sulfamethoxy-pyridazine | Complete remission |
| Finzi et al. 1980 [63] | Case report ** | 1 | - | Brazil | 14 years | - | - | - | - |
| Velluti et al. 1979 [64] | Case report * Italian | 1 | 52, M | Venezuela | 17 years | Fabric retailer | Lung | Amphotericin B, miconazole | Clinical improvement |
| Lasagni et al. 1979 [65] | Case report ** Italian | 1 | - | Venezuela | NR | - | - | - | - |
| Scarpa et al. 1965 [66] | Case report * Italian | 1 | 43, M | Venezuela | 5 years | Farmer | Lung, oral mucosa, skin | Amphotericin B, sulfamethoxazole | Patient deceased |
| Schiraldi et al. 1963 [67] | Case report ** | 1 | - | Venezuela | None | - | - | - | - |
| Molese et al. 1956 [68] | Case report * Italian | 1 | 47, M | Venezuela | None | Painter | Lung, lymph nodes, oral mucosa | Nystatin | NR |
| Farris 1955 [69] | Case report ** | 1 | - | Brazil | 7 years | - | - | - | - |
| Bertaccini 1934 [70] | Case report ** | 1 | - | Brazil | None | - | - | - | - |
| Dalla Favera 1914 [71] | Case report ** | 1 | - | Brazil | None | - | - | - | - |
| FRANCE | |||||||||
| Heleine et al. 2020 [72] | Case report English | 1 | 48, M | Brazil | NR | Farmer | Lung, lymph nodes, oropharyngeal mucosa, skin | Itraconazole | Clinical improvement |
| Dang et al. 2017 [73] | Case report English | 1 | 54, M | Columbia, Venezuela | 12 years | Journalist | Lymph nodes, oropharyngeal mucosa | Itraconazole | Clinical improvement; almost complete resolution of the tongue lesion and lymhadenopathy |
| Sambourg et al. 2014 [74] | Case report French | 1 | 43, M | Brazil | NR | NR | Skin | NR | NR |
| Laccourreye et al. 2010 [75] | Case report English | 1 | 46, M | Venezuela | NR | Engineer | Laryngeal mucosa | Itraconazole | Complete remission |
| Poisson et al. 2007 [76] | Case report English | 1 | 70, M | Paraguay | 6 years | NR | Brain, lung | Fluconazole, itraconazole | Remained clinically stable |
| NETHERLANDS | |||||||||
| Van Damme et al. 2006 [77] | Case report English | 1 | 60, M | Peru, Ecuador | 8 years | Carpenter | Lung, oral mucosa, urinary tract | Itraconazole | Clinical improvement, remained under control |
| NORWAY | |||||||||
| Maehlen et al. 2001 [78] | Case report Norwegian | 1 | 51, F | Brazil | 23 years | NR | Brain | - | Patient deceased |
| SWITZERLAND | |||||||||
| Stanisic et al. 1979 [79], Wegmann et al. 1959 [80] | Case report * German | 1 | 47, M | Brazil | 5 years | Carpenter | Lung, lymph nodes, oral mucosa | Hydroxy-stilbamidine, amphotericin B, sulfonamide | Patient deceased (Cor pulmonale) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, G.; Moertl, D.; Glechner, A.; Mayr, V.; Klerings, I.; Zachariah, C.; Van den Nest, M.; Gartlehner, G.; Willinger, B. Paracoccidioidomycosis Diagnosed in Europe—A Systematic Literature Review. J. Fungi 2021, 7, 157. https://doi.org/10.3390/jof7020157
Wagner G, Moertl D, Glechner A, Mayr V, Klerings I, Zachariah C, Van den Nest M, Gartlehner G, Willinger B. Paracoccidioidomycosis Diagnosed in Europe—A Systematic Literature Review. Journal of Fungi. 2021; 7(2):157. https://doi.org/10.3390/jof7020157
Chicago/Turabian StyleWagner, Gernot, Deddo Moertl, Anna Glechner, Verena Mayr, Irma Klerings, Casey Zachariah, Miriam Van den Nest, Gerald Gartlehner, and Birgit Willinger. 2021. "Paracoccidioidomycosis Diagnosed in Europe—A Systematic Literature Review" Journal of Fungi 7, no. 2: 157. https://doi.org/10.3390/jof7020157
APA StyleWagner, G., Moertl, D., Glechner, A., Mayr, V., Klerings, I., Zachariah, C., Van den Nest, M., Gartlehner, G., & Willinger, B. (2021). Paracoccidioidomycosis Diagnosed in Europe—A Systematic Literature Review. Journal of Fungi, 7(2), 157. https://doi.org/10.3390/jof7020157