
Congenital Heart Disease and the Risk of Cancer: An Update on the Genetic Etiology, Radiation Exposure Damage, and Future Research Strategies


Abstract
:1. Introduction
2. Research Design and Methods
3. Cancer Risk in CHD Patients
4. Genetic Etiology
5. Radiation Exposure and Cancer Risk in CHD
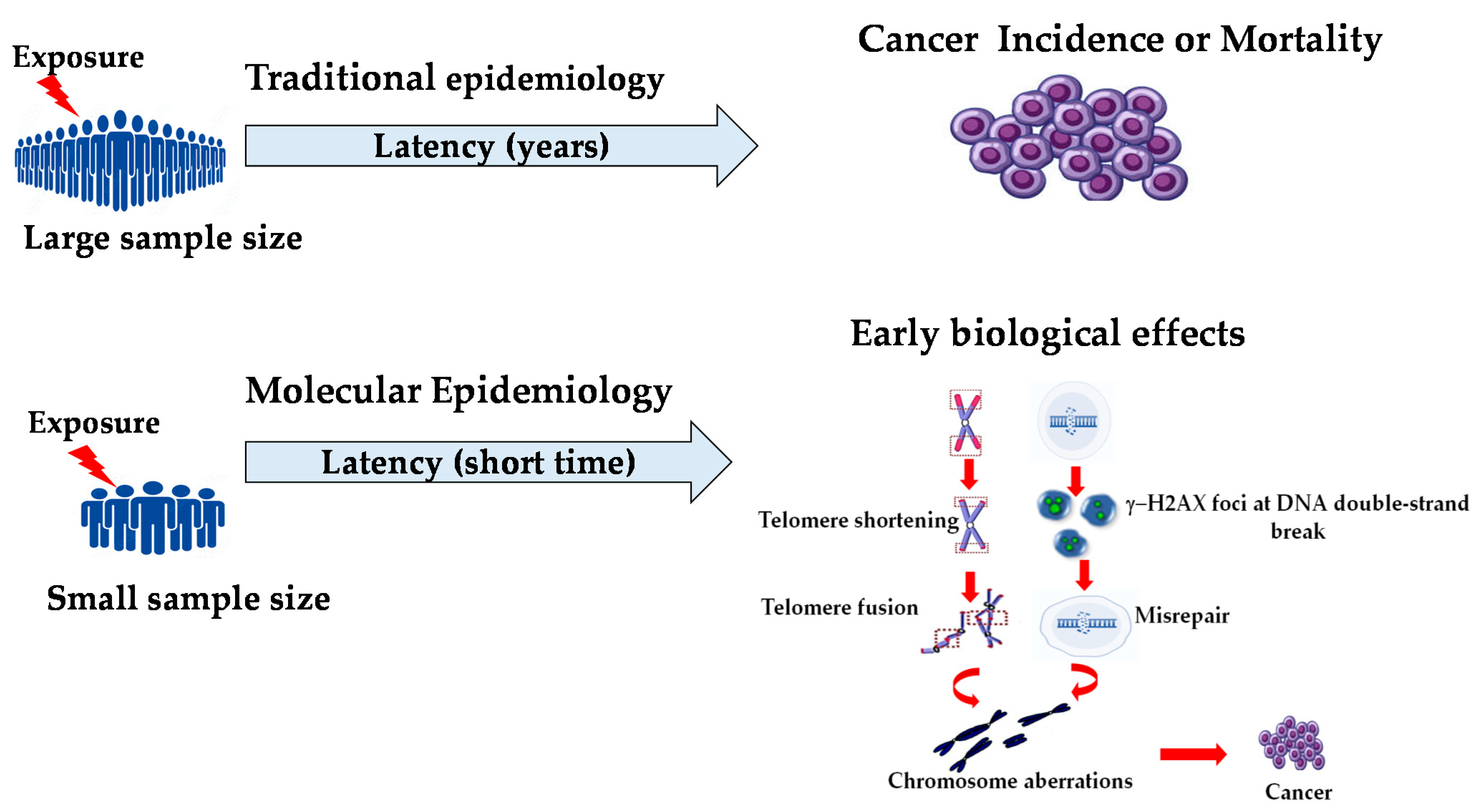
6. Molecular Epidemiology and Biomarkers for an Early Biological Effect
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandalenakis, Z.; Giang, K.W.; Eriksson, P.; Liden, H.; Synnergren, M.; Wåhlander, H.; Fedchenko, M.; Rosengren, A.; Dellborg, M. Survival in children with congenital heart disease: Have we reached a peak at 97%? J. Am. Heart Assoc. 2020, 9, e017704. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.W. Relation between cancer and congenital defects in man. N. Engl. J. Med. 1996, 275, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Agha, M.M.; Williams, J.I.; Marrett, L.; To, T.; Zipursky, A.; Dodds, L. Congenital abnormalities and childhood cancer. Cancer 2005, 103, 1939–1948. [Google Scholar] [CrossRef] [PubMed]
- Carozza, S.E.; Langlois, P.H.; Miller, E.A.; Canfield, M. Are children with birth at higher risk of childhood cancers? Am. J. Epidemiol. 2012, 175, 1217–1224. [Google Scholar] [CrossRef] [Green Version]
- Bjorge, T.; Cnattingius, S.; Lie, R.T.; Tretli, S.; Engeland, A. Cancer risk in children with birth defects and in their families: A population based cohort study of 5.2 million children from Norway and Sweden. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 500–506. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Overvad, K.; Olsen, J. Cancer risks in children with congenital malformations in the nervous and circulatory system-A population based cohort study. Cancer Epidemiol. 2014, 38, 393–400. [Google Scholar] [CrossRef]
- Botto, L.D.; Flood, T.; Little, J.; Fluchel, M.N.; Krikov, S.; Feldkamp, M.L.; Wu, Y.; Goedken, R.; Puzhankara, S.; Romitti, P.A. Cancer risk in children and adolescents with birth defects: A Population-Based Cohort Study. PLoS ONE 2013, 8, e69077. [Google Scholar] [CrossRef] [Green Version]
- Collins, R.T., II; Von Behren, J.; Yang, W.; Carmichael, S.L.; Reynolds, P.; Fisher, P.G.; Shaw, G.M. Congenital heart disease complexity and childhood cancer risk. Birth Defects Res. 2018, 110, 1314–1321. [Google Scholar] [CrossRef]
- Kampitsi, C.E.; Mogensen, H.; Feychting, M.; Tettamanti, G. The relationship between congenital heart disease and cancer in Swedish children: A population-based cohort study. PLoS Med. 2022, 19, e1003903. [Google Scholar] [CrossRef]
- Olsen, M.; Garne, E.; Sværke, C.; Søndergaard, L.; Nissen, H.; Andersen, H.Ø.; Hjortdal, V.E.; Johnsen, S.P.; Videbæk, J. Cancer risk among patients with congenital heart defects: A nationwide follow–up study. Cardiol. Young 2014, 24, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Chen, Y.T.; Jeng, M.J.; Tsao, P.C.; Yen, H.J.; Lee, P.C.; Li, S.Y.; Liu, C.J.; Chen, T.J.; Chou, P.; et al. The risk of cancer in patients with congenital heart disease: A nationwide population-based cohort study in Taiwan. PLoS ONE 2015, 10, e0116844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandalenakis, Z.; Karazisi, C.; Skoglund, K.; Rosengren, A.; Lappas, G.; Eriksson, P.; Dellborg, M. Risk of cancer among children and young adults with congenital heart disease compared with healthy controls. JAMA Netw. Open 2019, 2, 7. [Google Scholar] [CrossRef]
- Gurvitz, M.; Ionescu–Ittu, R.; Guo, L.; Eisenberg, M.J.; Abrahamowicz, M.; Pilote, L.; Marelli, A.J. Prevalence of Cancer in Adults with Congenital Heart Disease Compared with the General Population. Am. J. Cardiol. 2016, 118, 1742–1750. [Google Scholar] [CrossRef] [PubMed]
- Karazisi, C.; Dellborg, M.; Mellgren, K.; Giang, K.W.; Skoglund, K.; Eriksson, P.; Mandalenakis, Z. Risk of cancer in young and older patients with congenital heart disease and the excess risk of cancer by syndromes, organ transplantation and cardiac surgery: Swedish Health Registry Study (1930−2017). Lancet Reg. Health Eur. 2022, 18, 100407. [Google Scholar] [CrossRef] [PubMed]
- Gudmundsdottir, J.; SÖoderling, J.; Berggren, H.; Óskarsdóttir, S.; Neovius, M.; Stephansson, O.; Ekwall, O. Long-term clinical effects of early thymectomy: Associations with autoimmune diseases, cancer, infections, and atopic diseases. J. Allergy Clin. Immunol. 2018, 141, 2294–2297. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Gurvitz, M.Z.; Beauséjour-Ladouceur, V.; Lawler, P.R.; Therrien, J.; Marelli, A.J. Cancer risk in congenital heart disease—What is the evidence? Can. J. Cardiol. 2019, 35, 1750–1761. [Google Scholar] [CrossRef]
- Moore, S.W. Developmental genes and cancer in children. Pediatr. Blood Cancer 2009, 52, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Fisher, P.G.; Reynolds, P.; Von Behren, J.; Carmichael, S.L.; Rasmussen, S.A.; Shaw, G.M. Cancer in children with nonchromosomal birth defects. J. Pediatr. 2012, 160, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Hasle, H.; Clemmensen, I.H.; Mikkelsen, M. Risks of leukaemia and solid tumours in individuals with Down’s syndrome. Lancet 2000, 355, 165–169. [Google Scholar] [CrossRef]
- Marino, B.; Digilio, M.C.; Toscano, A.; Giannotti, A.; Dallapiccola, B. Congenital heart defects in patients with DiGeorge/velocardiofacial syndrome and del22q11. Genet. Couns. 1999, 10, 25–33. [Google Scholar] [PubMed]
- Lambert, M.P.; Arulselvan, A.; Schott, A.; Markham, S.J.; Crowley, T.B.; Zackai, E.H.; McDonald-McGinn, D.M. The 22q11.2 deletion syndrome: Cancer predisposition, platelet abnormalities and cytopenias. Am. J. Med. Genet. A 2018, 176, 2121–2127. [Google Scholar] [CrossRef] [PubMed]
- Jongmans, M.C.; van der Burgt, I.; Hoogerbrugge, P.M.; Noordam, K.; Yntema, H.G.; Nillesen, W.M.; Kuiper, R.P.; Ligtenberg, M.J.; van Kessel, A.G.; van Krieken, J.H.; et al. Cancer risk in patients with Noonan syndrome carrying a PTPN11 mutation. Eur. J. Hum. Genet. 2011, 19, 870–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegfried, A.; Cances, C.; Denuelle, M.; Loukh, N.; Tauber, M.; Cavé, H.; Delisle, M.B. Noonan syndrome, PTPN11 mutations, and brain tumors. A clinical report and review of the literature. Am. J. Med. Genet. A 2017, 173, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Seidman, C.E.; Morton, S.U.; Shimamura, A.; Opotowsky, A.R.; Quiat, D.; Pereira, A.C.; Jin, S.C.; Gurvitz, M.; Brueckner, M.; Chung, W.K.; et al. Association of damaging variants in genes with increased cancer risk among patients congenital heart disease. JAMA Cardiol. 2021, 6, 457–462. [Google Scholar]
- Knudson, A.G. Two genetic hits [more or less] to cancer. Nat. Rev. Cancer 2001, 1, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Andreassi, M.G.; Picano, E. Reduction of radiation to children: Our responsibility to change. Circulation 2014, 130, 135–137. [Google Scholar] [CrossRef] [Green Version]
- Picano, E.; Vano, E.; Rehani, M.; Cuocolo, A.; Mont, L.; Bodi, V.; Bar, O.; Maccia, C.; Pierard, L.; Sicari, R.; et al. The appropriate and justified use of medical radiation in cardiovascular imaging: A position document of the ESC Associations of cardiovascular imaging, Percutaneous cardiovascular interventions and electrophysiology. Eur. Heart J. 2014, 35, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Ait-Ali, L.; Andreassi, M.G.; Foffa, I.; Spadoni, I.; Vano, E.; Picano, E. Cumulative patient effective dose and acute radiation-induced chromosomal DNA damage in children with congenital heart disease. Heart 2010, 96, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Gherardi, G.G.; Iball, G.R.; Darby, M.J.; Thomson, J.D. Cardiac computed tomography and conventional angiography in the diagnosis of congenital cardiac disease in children: Recent trends and radiation doses. Cardiol. Young 2011, 21, 616–622. [Google Scholar] [CrossRef]
- Glatz, A.C.; Patel, A.; Zhu, X.; Dori, Y.; Hanna, B.D.; Gillespie, M.J.; Rome, J.J. Patient radiation exposure in a modern, large-volume, pediatric cardiac catheterization laboratory. Pediatr. Cardiol. 2014, 35, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.N.; Hornik, C.P.; Li, J.S.; Benjamin, D.K.; Yoshizumi, T.T.; Reiman, R.E.; Frush, D.P.; Hill, K.D. Cumulative radiation exposure and cancer risk estimation in children with heart disease. Circulation 2014, 130, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.J.; Hall, E.J. Computed tomography—An increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreassi, M.G. Radiation risk from pediatric cardiac catheterization: Friendly fire on children with congenital heart disease. Circulation 2009, 120, 1847–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spengler, R.F.; Cook, D.H.; Clarke, E.A.; Olley, P.M.; Newman, A.M. Cancer mortality following cardiac catheterization: A preliminary follow-up study on 4,891 irradiated children. Pediatrics 1983, 71, 235–239. [Google Scholar] [CrossRef]
- McLaughlin, J.R.; Kreiger, N.; Sloan, M.P.; Benson, L.N.; Hilditch, S.; Clarke, E.A. An historical cohort study of cardiac catheterization during childhood and the risk of cancer. Int. J. Epidemiol. 1993, 22, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Modan, B.; Keinan, L.; Blumstein, T.; Sadetzki, S. Cancer following cardiac catheterization in childhood. Int. J. Epidemiol. 2000, 29, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Liu, A.; Gurvitz, M.; Guo, L.; Therrien, J.; Laprise, C.; Kaufman, J.S.; Abrahamowicz, M.; Marelli, A.J. Exposure to low-dose ionizing radiation from cardiac procedures and malignancy risk in adults with congenital heart disease. Circulation 2018, 137, 1334–1345. [Google Scholar] [CrossRef]
- Harbron, R.W.; Chapple, C.-L.; O’Sullivan, J.J.; Lee, C.; McHugh, K.; Higueras, M.; Pearce, M.S. Cancer incidence among children and young adults who have undergone X-ray guided cardiac catheterization procedures. Eur. J. Epidemiol. 2018, 33, 393–401. [Google Scholar] [CrossRef] [Green Version]
- Stern, H.; Seidenbusch, M.; Hapfelmeier, A.; Meierhofer, C.; Naumann, S.; Schmid, I.; Spix, C.; Ewert, P. Increased Cancer Incidence Following up to 15 Years after Cardiac Catheterization in Infants under One Year between 1980 and 1998-A Single Center Observational Study. J. Clin. Med. 2020, 9, 315. [Google Scholar] [CrossRef] [Green Version]
- Abalo, K.D.; Malekzadeh-Milani, S.; Hascoët, S.; Dreuil, S.; Feuillet, T.; Cohen, S.; Dauphin, C.; Filippo, S.D.; Douchin, S.; Godart, F.; et al. Exposure to low-dose ionising radiation from cardiac catheterisation and risk of cancer: The COCCINELLE study cohort profile. BMJ Open 2021, 11, e048576. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Doll, R.; Goodhead, D.T.; Hall, E.J.; Land, C.E.; Little, J.B.; Lubin, J.H.; Preston, D.L.; Preston, R.J.; Puskin, J.S.; et al. Cancer risks attributable to low doses of ionizing radiation: Assessing what we really know. Proc. Natl. Acad. Sci. USA 2003, 100, 13761–13766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbron, R.W.; Thierry-Chef, I.; Pearce, M.S.; Bernier, M.O.; Dreuil, S.; Rage, E.; Andreassi, M.G.; Picano, E.; Dreger, S.; Zeeb, H.; et al. The HARMONIC project: Study design for assessment of cancer risks following cardiac fluoroscopy in childhood. J. Radiol. Prot. 2020, 40, 1074. [Google Scholar] [CrossRef] [PubMed]
- Perera, F.P.; Weinstein, I.B. Molecular epidemiology and carcinogen-DNA adduct detection: New approaches to studies of human cancer causation. J. Chronic Dis. 1982, 35, 581–600. [Google Scholar] [CrossRef]
- Vineis, P.; Chadeau-Hyam, M. Integrating biomarkers into molecular epidemiological studies. Curr. Opin. Oncol. 2011, 23, 100–105. [Google Scholar] [CrossRef]
- Bonassi, S.; Znaor, A.; Norppa, H.; Hagmar, L. Chromosomal aberrations and risk of cancer in humans: An epidemiologic perspective. Cytogenet. Genome Res. 2004, 104, 376–382. [Google Scholar] [CrossRef]
- Boffetta, P.; van der Hel, O.; Norppa, H.; Fabianova, E.; Fucic, A.; Gundy, S.; Lazutka, J.; Cebulska-Wasilewska, A.; Puskailerova, D.; Znaor, A.; et al. Chromosomal aberrations and cancer risk: Results of a cohort study from Central Europe. Am. J. Epidemiol. 2007, 165, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Adams, F.H.; Norman, A.; Bass, D.; Oku, G. Chromosome damage in infants and children after cardiac catheterization and angiocardiography. Pediatrics 1978, 62, 312–316. [Google Scholar] [CrossRef]
- Andreassi, M.G.; Ait-Ali, L.; Botto, N.; Manfredi, S.; Mottola, G.; Picano, E. Cardiac catheterization and long-term chromosomal damage in children with congenital heart disease. Eur. Heart J. 2006, 27, 2703–2708. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Wang, P.; Su, Y.; Wang, Z.; Han, L.; Li, J.; Fu, Y.; Zhao, F.; Sun, Q.; Lyu, Y. Cardiac catheterization procedures in children with congenital heart disease: Increased chromosomal aberrations in peripheral lymphocytes. Mutat. Res. 2020, 852, 503163. [Google Scholar] [CrossRef]
- Vecoli, C.; Borghini, A.; Foffa, I.; Ait-Ali, L.; Picano, E.; Andreassi, M.G. Leukocyte telomere shortening in grown-up patients with congenital heart disease. Int. J. Cardiol. 2016, 204, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Calado, R.T.; Young, N.S. Telomere diseases. N. Engl. J. Med. 2009, 361, 2353–2365. [Google Scholar] [CrossRef] [PubMed]
- Beels, L.; Bacher, K.; De Wolf, D.; Werbrouck, J.; Thierens, H. gamma-H2AX foci as a biomarker for patient X-ray exposure in pediatric cardiac catheterization: Are we underestimating radiation risks? Circulation 2009, 120, 1903–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Report of the United States Nations Scientific Committee on the Effects of Atomic Radiation to the General Assembly. Annex G: Biological Effects at Low Radiation Doses. In Sources and Effects of Ionising Radiation; United Nations Scientific Committee on the Effects of Atomic Radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Volume II: Effects. New York: United Nations: 451-566. Available online: https://www.unscear.org/docs/publications/2000/UNSCEAR_2000_Annex-G.pdf (accessed on 28 June 2022).
- Mone, S.M.; Gillman, M.W.; Miller, T.L.; Herman, E.H.; Lipshultz, S.E. Effects of environmental exposures on the cardiovascular system: Prenatal period through adolescence. Pediatrics 2004, 113, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Rosendahl Huber, A.; Van Hoeck, A.; Van Boxtel, R. The Mutagenic Impact of Environmental Exposures in Human Cells and Cancer: Imprints through Time. Front. Genet. 2021, 12, 760039. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Tarone, R.E.; Seguin, L.R.; Robbins, J.H. Hypersensitivity to ionizing radiation in cultured cells from Down syndrome patients. J. Neurol. Sci. 1985, 69, 103–112. [Google Scholar] [CrossRef]
- Giaccardi, M.; Del Rosso, A.; Guarnaccia, V.; Ballo, P.; Mascia, G.; Chiodi, L.; Colella, A. Near-zero X-ray in arrhythmia ablation using a 3-dimensional electroanatomic mapping system: A multicenter experience. Heart Rhythm 2016, 13, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study | Subjects | Design | Results |
|---|---|---|---|
| Olsen M, et al., 2014, [11] | 15,905 CHD children/young born from 1977 to 2008; 801 with Down syndrome or Fanconi anemia. Data sources: Danish National Registry of Patients and Danish Cancer Registry. | Register-based study. | Increased cancer risk in CHD cohort (SIR 1.63, 95%CI: 1.22–2.13). No association was found by excluding patients with Down syndrome or Fanconi anemia. |
| Lee YS, et al., 2015, [12] | 31,961 children/young adults, newly diagnosed from 1998 to 2006. Data sources: Taiwan National Health Insurance Research Database. | Population-based cohort study. | Increased cancer risk in CHD (SIR 1.45, 95%CI 1.25–1.67), particularly hematologic, CNS, and head/neck malignancies. Age and chronic liver disease are independent risk factors for cancer occurrence. |
| Gurvitz M, et al., 2016, [14] | 34,965 CHD adults alive in 2005. Data sources: Quebec Congenital Heart Disease Database from 1983 to 2005. | Population-based cohort study. | Twofold increased cancer prevalence in CHD compared to general population. Breast, colorectal, and uterine are the most common types for women; prostate, colorectal, and bladder for men. |
| Collins II RT, et al., 2018, [9] | 65,585 children with structural birth defects born from 1988 to 2004; 25,981 with CHD but without chromosomal anomalies. Data sources: California Birth Defects Monitoring Program Registry and California Cancer Registry. | Population-based cohort study. | Increased cancer risk in CHD compared to non-CHD (HR 2.6, 95% CI 1.9–3.6). Lymphoma is more than 8 times higher in CHD and correlated with disease complexity. |
| Mandalenakis Z, et al. 2019, [13] | 21,982 CHD and 219,816 without CHD born from 1970 to 1993. Data sources: Swedish Patient Register. | Registry-based prospective cohort study. | Increased cancer risk in CHD compared to controls (HR 2.24, 95% CI 2.01–2.48), higher among CHD from the most recent birth cohort. |
| Karazisi C, et al., 2022, [15] | 89,542 CHD and 890,472 controls without CHD, born between 1930 and 2017. Data sources: Swedish Health Registers and Swedish Total Population Register. | Register-based study. | The overall cancer risk is 23% higher in CHD compared to controls and 18% higher excluding those with syndromes and organ transplant recipients. The highest cancer risk was found in CHD cohort aged 0–17 years. |
| Kampitsi et al., 2022, [10] | 4,178,722 children born between 1973 and 2014; 66,892 CHD subjects. Data sources: Swedish Medical Birth Register, National Patient Register, and Swedish Cancer Register. | Population-based cohort study. | Increased risks of lymphomas and hepatoblastomas in CHD, even excluding subjects with Down syndrome. Stronger association was observed in complex CHD. |
| Procedure | Effective Dose (mSv) | Equivalent CXRs |
|---|---|---|
| Chest X-ray | 0.02 | 1 |
| Diagnostic catheterization | 6.0 | 300 |
| Patent ductus arteriosus occlusion | 7.6 | 360 |
| Closure of atrial septal defect | 2.8 | 280 |
| Aortic coarctation | 6.8 | 340 |
| Balloon valvuloplasty | 8.1 | 410 |
| Electrophysiological study | 3.2 | 160 |
| Regular PM or ICD implant | 4 | 200 |
| Ablation procedure | 15.2 | 760 |
| Study | Subjects | Design | Exposure Assessment | Results |
|---|---|---|---|---|
| Spengler RF, et al., 1983, [35] | 4891 CHD children assessed by CC during 1946 to 1968. Data sources: records from the Hospital for Sick Children in Toronto and Ontario cancer death file. | A retrospective cohort study. | Estimation of radiation exposure per CC. | No excess of cancer mortality in children who underwent CC. |
| McLaughlin JR, et al., 1993, [36] | 3915 children < 18 years at the time of procedure who underwent CC between 1950–1965. Data sources: records from Ontario Hospital for Sick Children and Ontario Cancer registry. | Monocenter retrospective cohort study. | Number of procedures. Time period of the first CC per child. | No risk of cancer among the cohort and no association between exposure and increased cancer risk were found. |
| Modan B, et al., 2000, [37] | 674 children with congenital anomalies who underwent CC between 1950–1970. Data sources: records from 3 major Israeli medical centers and the National Cancer Registry. | Multicenter retrospective cohort study. | Number of procedures. | Increased risk of all cancers (SIR = 2.3; 95% CI: 1.2–4.1); lymphomas the most relevant. No dose–response association was observed. |
| Harbron RW, et al., 2018, [39] | 11,270 CHD patients who underwent CC before 22 years. Data sources: UK hospital records, NHS Central Register, NHS Transplant Registry. | Multicenter retrospective cohort study. | Number of CC and CT procedures. Estimated cumulative organ doses for CC and CT procedures. | Higher cancer rate in CHD compared to general population was found, especially in transplant recipients. The number of CC/CT or organ doses was associated with post-transplant cases. |
| Cohen S, et al., 2018, [38] | 24,833 CHD adult patients (18 to 64 years); 602 cancer cases. Patients with genetic disorders were excluded. Data sources: Quebec Congenital Heart Disease Database. | Retrospective, population-based cohort and control–case study. | Cumulative LDIR exposure. | Cumulative cancer incidence in CHD was 15.3% (95% CI, 14.2–16.5). Cases had more LDIR-related cardiac procedures than controls, and cumulative LDIR exposure was associated with cancer. |
| Stern H, et al., 2020, [40] | 2770 CHD children who underwent CC under 1 year of age between 1980–1998. Data sources: hospital database and German Childhood Cancer Registry. | Retrospective single-center observational study. | Effective radiation doses. | Increased cancer risk (SIR 4.4 95%CI: 2.5–7.2) in CHD in the first year of life. No significant association was found between cancers and effective radiation doses. |
| Abalo KD, et al., 2021, [41] | 17,104 CHD patients (<16 years) at first CC between 2000–2013. Data sources: Patient cohort comes from 15 France hospitals and the National Childhood Cancer Registry. | Multicenter retrospective cohort study. | Number of CC procedures. | Increased SIRs in CHD for all-cancer, leukemia, lymphoma, and solid cancers compared to general population. No difference in number of procedures between cancer and non-cancer cases were observed. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campolo, J.; Annoni, G.; Giaccardi, M.; Andreassi, M.G. Congenital Heart Disease and the Risk of Cancer: An Update on the Genetic Etiology, Radiation Exposure Damage, and Future Research Strategies. J. Cardiovasc. Dev. Dis. 2022, 9, 245. https://doi.org/10.3390/jcdd9080245
Campolo J, Annoni G, Giaccardi M, Andreassi MG. Congenital Heart Disease and the Risk of Cancer: An Update on the Genetic Etiology, Radiation Exposure Damage, and Future Research Strategies. Journal of Cardiovascular Development and Disease. 2022; 9(8):245. https://doi.org/10.3390/jcdd9080245
Chicago/Turabian StyleCampolo, Jonica, Giuseppe Annoni, Marzia Giaccardi, and Maria Grazia Andreassi. 2022. "Congenital Heart Disease and the Risk of Cancer: An Update on the Genetic Etiology, Radiation Exposure Damage, and Future Research Strategies" Journal of Cardiovascular Development and Disease 9, no. 8: 245. https://doi.org/10.3390/jcdd9080245
APA StyleCampolo, J., Annoni, G., Giaccardi, M., & Andreassi, M. G. (2022). Congenital Heart Disease and the Risk of Cancer: An Update on the Genetic Etiology, Radiation Exposure Damage, and Future Research Strategies. Journal of Cardiovascular Development and Disease, 9(8), 245. https://doi.org/10.3390/jcdd9080245