
Serum and Vascular Stiffness Biomarkers Associated with the Severity of Degenerative Aortic Valve Stenosis and Cardiovascular Outcomes

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
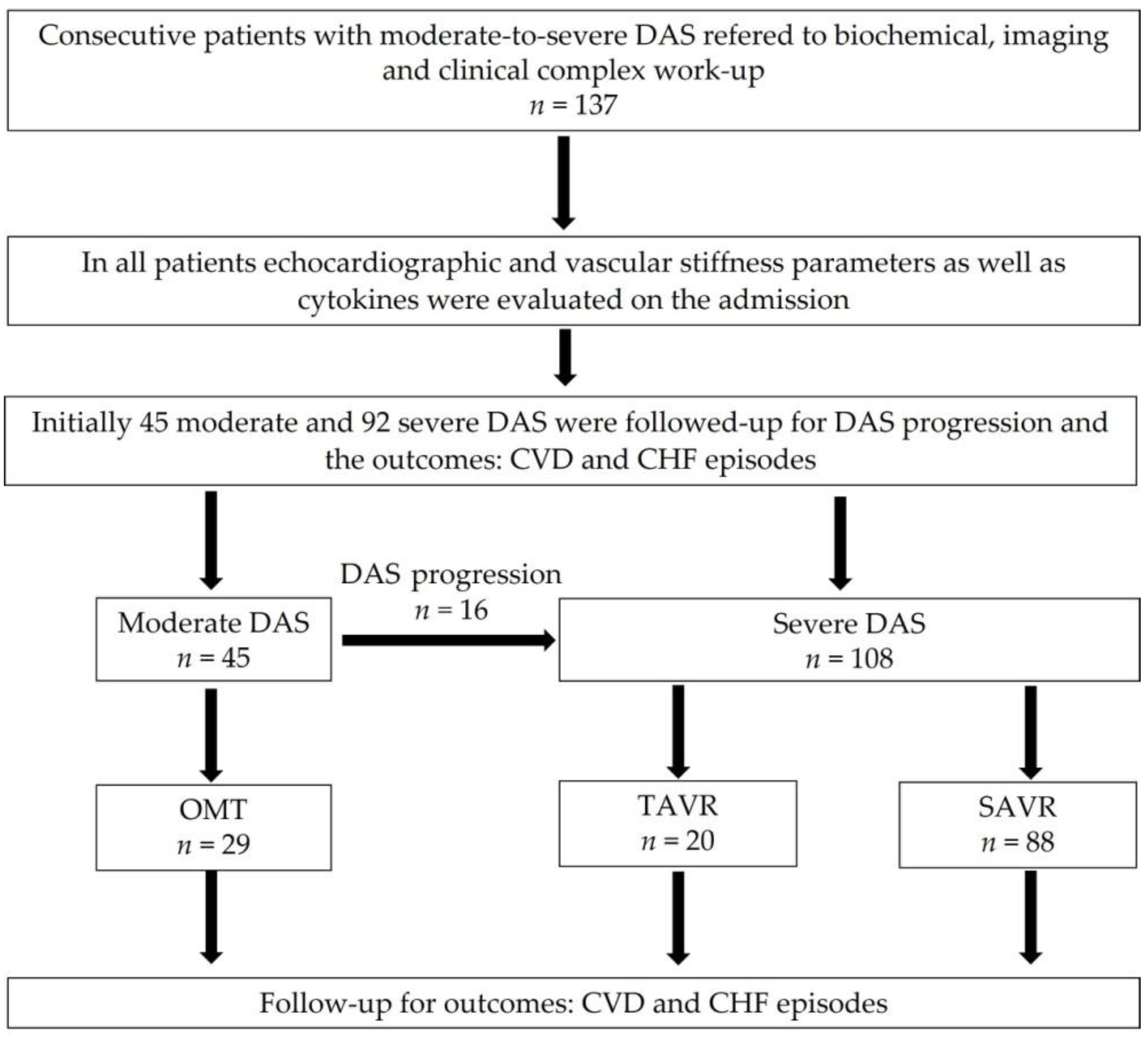
2.1. Study Population
2.2. Cardiovascular Risk Factors and Echocardiographic Study
2.3. Vascular Stiffness Assessment
2.4. Cytokines Assessment
2.5. Follow-Up Period
2.6. Statistical Analysis
3. Results
3.1. Baseline Patients’ Characteristics
3.2. Associations between DAS Severity and DAS Progression with Serum Biomarkers, Echocardiographic and VS Parameters
3.3. Comparison of Studied Parameters between SAVR, TAVR, and OMT Groups
3.4. Cardiovascular Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Naqvi, S.Y.; Giri, J.; Goldberg, S. Aortic Stenosis: Pathophysiology, Diagnosis, and Therapy. Am. J. Med. 2017, 130, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Baran, J.; Podolec, J.; Tomala, M.; Nawrotek, B.; Niewiara, Ł.; Gackowski, A.; Przewłocki, T.; Żmudka, K.; Kabłak-Ziembicka, A. Increased risk profile in the treatment of patients with symptomatic degenerative aortic valve stenosis over the last 10 years. Adv. Interv. Cardiol. 2018, 14, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowski, M.; Pyłko, A.; Chmielak, Z.; Kwieciński, J.; Kukuła, K.; Wysocki, K.; Mazurek, Ł.; Tołwiński, I.; Tyczyński, P.; Skowroński, J.; et al. Comparison of transcatheter aortic valve implantation outcomes in patients younger than 85 years and those aged 85 years or older: A single-center study. Pol. Arch. Intern. Med. 2021, 131, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Small, A.; Kiss, D.; Giri, J.; Anwaruddin, S.; Siddiqi, H.; Guerraty, M.; Chirinos, J.A.; Ferrari, G.; Rader, D.J. Biomarkers of Calcific Aortic Valve Disease. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 623–632. [Google Scholar] [CrossRef] [Green Version]
- Podolec, J.; Baran, J.; Siedlinski, M.; Urbanczyk, M.; Krupinski, M.; Bartus, K.; Niewiara, L.; Podolec, M.; Guzik, T.; Tomkiewicz-Pajak, L.; et al. Serum rantes, transforming growth factor-β1 and interleukin-6 levels correlate with cardiac muscle fibrosis in patients with aortic valve stenosis. J. Physiol. Pharmacol. 2018, 69, 615–623. [Google Scholar] [CrossRef]
- Baran, J.; Kleczyński, P.; Niewiara, Ł.; Podolec, J.; Badacz, R.; Gackowski, A.; Pieniążek, P.; Legutko, J.; Żmudka, K.; Przewłocki, T.; et al. Importance of Increased Arterial Resistance in Risk Prediction in Patients with Cardiovascular Risk Factors and Degenerative Aortic Stenosis. J. Clin. Med. 2021, 10, 2109. [Google Scholar] [CrossRef]
- Ferrari, E.; Gallo, M.; Wang, C.; Zhang, L.; Taramasso, M.; Maisano, F.; Pirelli, L.; Berdajs, D.; von Segesser, L.K. Three-dimensional printing in adult cardiovascular medicine for surgical and transcatheter procedural planning, teaching and technological innovation. Interact. CardioVascular Thorac. Surg. 2020, 30, 203–214. [Google Scholar] [CrossRef]
- Pasta, S.; Agnese, V.; Gallo, A.; Cosentino, F.; Di Giuseppe, M.; Gentile, G.; Raffa, G.M.; Maalouf, J.F.; Michelena, H.I.; Bellavia, D.; et al. Shear Stress and Aortic Strain Associations with Biomarkers of Ascending Thoracic Aortic Aneurysm. Ann. Thorac. Surg. 2020, 110, 1595–1604. [Google Scholar] [CrossRef]
- Pasta, S.; Gentile, G.; Raffa, G.M.; Scardulla, F.; Bellavia, D.; Luca, A.; Pilato, M.; Scardulla, C. Three-dimensional parametric modeling of bicuspid aortopathy and comparison with computational flow predictions. Artif. Organs 2017, 41, E92–E102. [Google Scholar] [CrossRef]
- Mathieu, P.; Bouchareb, R.; Boulanger, M.C. Innate and Adaptive Immunity in Calcific Aortic Valve Disease. J. Immunol. Res. 2015, 2015, 851945. [Google Scholar] [CrossRef] [PubMed]
- Bartoli-Leonard, F.; Zimmer, J.; Aikawa, E. Innate and adaptive immunity: The understudied driving force of heart valve disease. Cardiovasc. Res. 2021, 117, 2506–2524. [Google Scholar] [CrossRef] [PubMed]
- Galeone, A.; Paparella, D.; Colucci, S.; Grano, M.; Brunetti, G. The role of TNF-α and TNF superfamily members in the pathogenesis of calcific aortic valvular disease. Sci. World J. 2013, 2013, 875363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkovskiy, A.; Malashicheva, A.; Sullivan, G.; Bogdanova, M.; Kostareva, A.; Stensløkken, K.O.; Fiane, A.; Vaage, J. Valve Interstitial Cells: The Key to Understanding the Pathophysiology of Heart Valve Calcification. J. Am. Heart Assoc. 2017, 6, e006339. [Google Scholar] [CrossRef]
- Plunde, O.; Bäck, M. Fatty acids and aortic valve stenosis. Kardiol. Pol. 2021, 79, 614–621. [Google Scholar] [CrossRef]
- Sádaba, J.R.; Martínez-Martínez, E.; Arrieta, V.; Álvarez, V.; Fernández-Celis, A.; Ibarrola, J.; Melero, A.; Rossignol, P.; Cachofeiro, V.; López-Andrés, N. Role for Galectin-3 in Calcific Aortic Valve Stenosis. J. Am. Heart Assoc. 2016, 5, e004360. [Google Scholar] [CrossRef] [Green Version]
- Badacz, R.; Przewłocki, T.; Gacoń, J.; Stępień, E.; Enguita, F.; Karch, I.; Żmudka, K.; Kabłak-Ziembicka, A. Circulating miRNA levels differ with respect to carotid plaque characteristics and symptom occurrence in patients with carotid artery stenosis and provide information on future cardiovascular events. Postępy Kardiol Interwencyjnej 2018, 14, 75–84. [Google Scholar] [CrossRef]
- O’Neill, B.P.; Guerrero, M.; Thourani, V.H.; Kodali, S.; Heldman, A.; Williams, M.; Xu, K.; Pichard, A.; Mack, M.; Babaliaros, V.; et al. Prognostic value of serial B-type natriuretic peptide measurement in transcatheter aortic valve replacement (from the PARTNER Trial). Am. J. Cardiol. 2015, 115, 1265–1272. [Google Scholar] [CrossRef]
- Clavel, M.A.; Malouf, J.; Michelena, H.I.; Suri, R.M.; Jaffe, A.S.; Mahoney, D.W.; Enriquez-Sarano, M. B-type natriuretic peptide clinical activation in aortic stenosis: Impact on long-term survival. J. Am. Coll. Cardiol. 2014, 63, 2016–2025. [Google Scholar] [CrossRef] [Green Version]
- Fabiani, I.; Santoni, T.; Angelillis, M.; Petricciuolo, S.; Colli, A.; Pellegrini, G.; Mazzei, D.; Pugliese, N.R.; Petronio, A.S.; De Caterina, R. Growth Differentiation Factor 15 in Severe Aortic Valve Stenosis: Relationship with Left Ventricular Remodeling and Frailty. J. Clin. Med. 2020, 9, 2998. [Google Scholar] [CrossRef]
- Jonik, S.; Marchel, M.; Pedzich-Placha, E.; Huczek, Z.; Kochman, J.; Ścisło, P.; Czub, P.; Wilimski, R.; Hendzel, P.; Opolski, G.; et al. Heart Team for Optimal Management of Patients with Severe Aortic Stenosis-Long-Term Outcomes and Quality of Life from Tertiary Cardiovascular Care Center. J. Clin. Med. 2021, 10, 5408. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F., Jr.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2017, 30, 372–392. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinf. 2011, 12, 77. [Google Scholar] [CrossRef]
- Velissaris, D.; Zareifopoulos, N.; Koniari, I.; Karamouzos, V.; Bousis, D.; Gerakaris, A.; Platanaki, C.; Kounis, N. Soluble Urokinase Plasminogen Activator Receptor as a Diagnostic and Prognostic Biomarker in Cardiac Disease. J. Clin. Med. Res. 2021, 13, 133–142. [Google Scholar] [CrossRef]
- Hodges, G.W.; Bang, C.N.; Eugen-Olsen, J.; Olsen, M.H.; Boman, K.; Ray, S.; Kesäniemi, A.Y.; Jeppesen, J.L.; Wachtell, K. SuPAR predicts postoperative complications and mortality in patients with asymptomatic aortic stenosis. Open Heart 2018, 5, e000743. [Google Scholar] [CrossRef]
- Arangalage, D.; Nguyen, V.; Robert, T.; Melissopoulou, M.; Mathieu, T.; Estellat, C.; Codogno, I.; Huart, V.; Duval, X.; Cimadevilla, C.; et al. Determinants and prognostic value of Galectin-3 in patients with aortic valve stenosis. J. Am. Heart Assoc. 2016, 102, 862–868. [Google Scholar] [CrossRef]
- Bobrowska, B.; Wieczorek-Surdacka, E.; Kruszelnicka, O.; Chyrchel, B.; Surdacki, A.; Dudek, D. Clinical Correlates and Prognostic Value of Plasma Galectin-3 Levels in Degenerative Aortic Stenosis: A Single-Center Prospective Study of Patients Referred for Invasive Treatment. Int. J. Mol. Sci. 2017, 18, 947. [Google Scholar] [CrossRef]
- Arrieta, V.; Sádaba, J.R.; Álvarez, V.; Rodríguez, J.A.; López-Andrés, N. Galectin-3 as a novel biotarget in cardiovascular alterations associated to development of severe aortic stenosis. An. Sist. Sanit. Navar. 2019, 42, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Calvier, L.; Martinez-Martinez, E.; Miana, M.; Cachofeiro, V.; Rousseau, E.; Sádaba, J.R.; Zannad, F.; Rossignol, P.; López-Andrés, N. The impact of galectin-3 inhibition on aldosterone-induced cardiac and renal injuries. JACC Heart Fail. 2015, 3, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ibarrola, J.; Martínez-Martínez, E.; Sádaba, J.R.; Arrieta, V.; García-Peña, A.; Álvarez, V.; Fernández-Celis, A.; Gainza, A.; Rossignol, P.; Cachofeiro Ramos, V.; et al. Beneficial Effects of Galectin-3 Blockade in Vascular and Aortic Valve Alterations in an Experimental Pressure Overload Model. Int. J. Mol. Sci. 2017, 18, 1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karadimou, G.; Plunde, O.; Pawelzik, S.C.; Carracedo, M.; Eriksson, P.; Franco-Cereceda, A.; Paulsson-Berne, G.; Bäck, M. TLR7 Expression Is Associated with M2 Macrophage Subset in Calcific Aortic Valve Stenosis. Cells 2020, 9, 1710. [Google Scholar] [CrossRef] [PubMed]
- Kablak-Ziembicka, A.; Przewlocki, T.; Tracz, W.; Podolec, P.; Stopa, I.; Kostkiewicz, M.; Sadowski, J.; Mura, A.; Kopeć, G. Prognostic Value of Carotid Intima-Media Thickness in Detection of Coronary Atherosclerosis in Patients with Calcified Aortic Valve Stenosis. J. Ultrasound Med. 2005, 24, 461–467. [Google Scholar] [CrossRef]
- Ma, X.; Zhao, D.; Yuan, P.; Li, J.; Yun, Y.; Cui, Y.; Zhang, T.; Ma, J.; Sun, L.; Ma, H.; et al. Endothelial-to-Mesenchymal Transition in Calcific Aortic Valve Disease. Acta Cardiol. Sin. 2020, 3, 183–194. [Google Scholar]
- Bäz, L.; Dannberg, G.; Grün, K.; Westphal, J.; Möbius-Winkler, S.; Jung, C.; Pfeil, A.; Schulze, P.C.; Franz, M. Serum Biomarkers of Cardiovascular Remodelling Reflect Extra-Valvular Cardiac Damage in Patients with Severe Aortic Stenosis. Int. J. Mol. Sci. 2020, 21, 4174. [Google Scholar] [CrossRef]
- Généreux, P.; Pibarot, P.; Redfors, B.; Mack, M.J.; Makkar, R.R.; Jaber, W.A.; Svensson, L.G.; Kapadia, S.; Tuzcu, E.M.; Thourani, V.H.; et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur. Heart J. 2017, 38, 3351–3358. [Google Scholar] [CrossRef] [Green Version]
- Chin, C.W.; Messika-Zeitoun, D.; Shah, A.S.; Lefevre, G.; Bailleul, S.; Yeung, E.N.; Koo, M.; Mirsadraee, S.; Mathieu, T.; Semple, S.I.; et al. A clinical risk score of myocardial fibrosis predicts adverse outcomes in aortic stenosis. Eur. Heart J. 2016, 37, 713–723. [Google Scholar] [CrossRef] [Green Version]
- Chin, C.W.; Shah, A.S.; McAllister, D.A.; Joanna Cowell, S.; Alam, S.; Langrish, J.P.; Strachan, F.E.; Hunter, A.L.; Maria Choy, A.; Lang, C.C.; et al. High-sensitivity troponin I concentrations are a marker of an advanced hypertrophic response and adverse outcomes in patients with aortic stenosis. Eur. Heart J. 2014, 35, 2312–2321. [Google Scholar] [CrossRef]
- Przewłocki, T.; Kabłak-Ziembicka, A.; Kozanecki, A.; Rzeźnik, D.; Pieniążek, P.; Musiałek, P.; Piskorz, A.; Sokołowski, A.; Rosławiecka, A.; Tracz, W. Polyvascular extracoronary atherosclerotic disease in patients with coronary artery disease. Kardiol. Pol. 2009, 67, 978–984. [Google Scholar]
- Badacz, R.; Przewłocki, T.; Pieniążek, P.; Rosławiecka, A.; Kleczyński, P.; Legutko, J.; Żmudka, K.; Kabłak-Ziembicka, A. MicroRNA-134-5p and the Extent of Arterial Occlusive Disease Are Associated with Risk of Future Adverse Cardiac and Cerebral Events in Diabetic Patients Undergoing Carotid Artery Stenting for Symptomatic Carotid Artery Disease. Molecules 2022, 27, 2472. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Muntner, P.; Lloyd, A.; Manns, B.J.; Klarenbach, S.; Pannu, N.; James, M.T.; Hemmelgarn, B.R.; Alberta Kidney Disease Network. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: A population-level cohort study. Lancet 2012, 380, 807–814. [Google Scholar] [CrossRef]
- Goody, P.R.; Hosen, M.R.; Christmann, D.; Niepmann, S.T.; Zietzer, A.; Adam, M.; Bönner, F.; Zimmer, S.; Nickenig, G.; Jansen, F. Aortic Valve Stenosis: From Basic Mechanisms to Novel Therapeutic Targets. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 885–900. [Google Scholar] [CrossRef] [PubMed]
- Broeders, W.; Bekkering, S.; El Messaoudi, S.; Joosten, L.; van Royen, N.; Riksen, N.P. Innate immune cells in the pathophysiology of calcific aortic valve disease: Lessons to be learned from atherosclerotic cardiovascular disease? Basic Res. Cardiol. 2022, 117, 28. [Google Scholar] [CrossRef]


{kind=link}
| All Study Participants N = 137 | Moderate DAS N = 45 | Severe DAS N = 92 | p-Value * | |
|---|---|---|---|---|
| Demographic data | ||||
| Age, years, ± SD | 69.5 ± 8.5 | 69.2 ± 8.37 | 69.7 ± 8.66 | 0.727 |
| BMI, ± SD | 29.6 ± 5.60 | 30.9 ± 5.28 | 28.9 ± 5.69 | 0.062 |
| Female, n (%) | 67 (48.9%) | 25 (55.6%) | 42 (45.7%) | 0.364 |
| Hypertension, n (%) | 130 (94.9%) | 44 (97.8%) | 44 (97.8%) | 0.426 |
| Type 2 Diabetes, n (%) | 40 (29.2%) | 13 (28.9%) | 27 (29.3%) | 1 |
| Hyperlipidemia, n (%) | 132 (96.4%) | 41 (91.1%) | 91 (98.9%) | 0.04 |
| Paroxysmal atrial fibrillation, n (%) | 21 (15.4%) | 7 (15.6%) | 14 (15.4%) | 1 |
| Smoking history, n (%) | 36 (26.3%) | 12 (26.7%) | 24 (26.1%) | 1 |
| Previous MI, n (%) | 11 (8.03%) | 2 (4.44%) | 9 (9.78%) | 0.339 |
| COPD, n (%) | 11 (8.03%) | 5 (11.1%) | 6 (6.52%) | 0.504 |
| CAD, n (%) ** | 45 (32.8%) | 17 (37.8%) | 28 (30.4%) | 0.545 |
| Previous PCI, n (%) | 28 (20.4%) | 13 (28.9%) | 15 (16.3%) | 0.136 |
| Previous CABG, n (%) | 2 (1.46%) | 1 (2.22%) | 1 (1.09%) | 0.551 |
| LEAD, n (%) | 27 (19.7%) | 14 (31.1%) | 13 (14.1%) | 0.034 |
| Anemia ***, n (%) | 26 (19%) | 6 (13.3%) | 20 (21.7%) | 0.239 |
| Clinical symptom | ||||
| NYHA III vs. I + II, n (%) | 29 (21.2%) | 1 (2.22%) | 28 (30.4%) | <0.001 |
| Echocardiographic data | ||||
| Aortic valve area (cm2) ± SD | 0.94 ± 0.31 | 1.28 ± 0.24 | 0.77 ± 0.17 | <0.001 |
| Peak aortic velocity (m/s) ± SD | 4.29 ± 0.86 | 3.46 ± 0.57 | 4.70 ± 0.67 | <0.001 |
| Mean aortic gradient (mmHg) ± SD | 47.6 ±19.8 | 28.9 ± 9.91 | 56.7 ± 16.9 | <0.001 |
| LVEF (%) ± SD | 62.8 ± 7.33 | 64.7 ± 7.37 | 61.9 ± 7.17 | 0.038 |
| LVEDD (mm) ± SD | 47.4 ± 5.12 | 47.7 ± 4.87 | 47.2 ± 5.27 | 0.598 |
| IVS thickness in diastole (mm) ± SD | 13.5 ± 2.18 | 12.7 ± 1.72 | 14.0 ± 2.27 | <0.001 |
| PW thickness in diastole (mm) ± SD | 12.0 ± 1.73 | 11.6 ± 1.48 | 12.2 ± 1.81 | 0.04 |
| Left atrium (cm2) ± SD | 24.4 ± 4.65 | 24.4 ± 5.18 | 24.5 ± 4.37 | 0.967 |
| e’ medial velocity (cm/s) ± SD | 6.71 ± 1.85 | 7.67 ± 1.67 | 6.21 ± 1.76 | 0.024 |
| e’ lateral velocity (cm/s) ± SD | 7.49 ± 2.59 | 7.94 ± 1.98 | 7.27 ± 2.86 | 0.475 |
| E/e’, 1 ± SD | 11.8 ± 2.81 | 12.2 ± 3.10 | 11.6 ± 2.65 | 0.319 |
| Tricuspid regurgitant velocity (m/s) ± SD | 2.63 ± 0.43 | 2.61 ± 0.42 | 2.65 ± 0.44 | 0.696 |
| Vascular stiffness parameters | ||||
| Resistive Index, median [Q1; Q3] | 0.68 [0.63; 0.72] | 0.70 [0.64; 0.72] | 0.67 [0.61; 0.71] | 0.09 |
| Pulsatile Index, median [Q1; Q3] | 1.24 [1.08; 1.37] | 1.31 [1.13; 1.39] | 1.24 [1.05; 1.37] | 0.087 |
| Biochemical parameters | ||||
| RANTES/CCL5 (ng/mL), median [Q1; Q3] | 29.9 [21.8; 40.9] | 28.5 [21.8; 36.4] | 30.5 [21.8; 42.2] | 0.272 |
| ET-1 (pg/mL), median [Q1; Q3] | 1.67 [1.42; 2.09] | 1.56 [1.34; 1.88] | 1.86 [1.44; 2.11] | 0.001 |
| Gal-3 (ng/mL), median [Q1; Q3] | 11.9 [9.55; 15.4] | 10.5 [8.68; 14.0] | 12.3 [10.3;15.5] | 0.169 |
| GDF-15 (ng/mL), median [Q1; Q3] | 0.98 [0.62; 1.45] | 1.05 [0.62; 1.50] | 0.87 [0.62; 1.27] | 0.512 |
| hsTnT (pg/mL), median [Q1; Q3] | 14 [11; 22] | 15 [10; 24] | 13 [11; 22] | 0.779 |
| IL-6R ά (ng/mL), median [Q1; Q3] | 46.8 [38.8; 58.9] | 51.9 [44.4; 68.1] | 43.1 [36.1; 54.3] | <0.001 |
| PCSK9 (ng/mL), median [Q1; Q3] | 308 [243; 352] | 326 [244; 377] | 286 [243; 333] | 0.122 |
| NT-pro-BNP (pg/mL), median [Q1; Q3] | 487 [188; 823] | 325 [143; 681] | 571 [234; 1098] | 0.004 |
| uPAR (ng/mL), median [Q1; Q3] | 1.44 [1.19; 1.86] | 1.61 [1.28; 2.21] | 1.42 [1.14; 1.73] | 0.031 |
| Creatinine (µmol/L), median [Q1; Q3] | 79.0 [69.0; 95.0] | 78.0 [66.0; 95.0] | 80.5 [70.0; 95.2] | 0.403 |
| eGFR (mL/min/1.73 m2), median [Q1; Q3] | 76.0 [64.0; 88.0] | 79.0 [65.0; 87.0] | 74.5 [63.0; 89.0] | 0.67 |
| Hemoglobin (mg/dL), median [Q1; Q3] | 13.8 [12.6; 15.1] | 13.7 [12.6; 14.9] | 13.9 [12.7; 15.1] | 0.971 |
| hs-CRP (mg/L), median [Q1; Q3] | 1.88 [0.98; 3.29] | 2.36 [1.17; 5.06] | 1.62 [0.93; 3.05] | 0.052 |
| Biomarkers | Progression | Non-Progression | |
|---|---|---|---|
| n = 16 | n = 29 | ||
| Serum biomarkers | |||
| RANTES/CCL5 (ng/mL), median [Q1; Q3] | 32.2 [26.4; 40.8] | 26.7 [17.0; 36.6] | 0.006 |
| ET-1 (pg/mL), median [Q1; Q3] | 1.55 [1.25; 2.09] | 1.56 [1.31; 1.87] | 0.657 |
| Gal-3 (ng/mL), median [Q1; Q3] | 13.1 [9.6; 17.4] | 10.0 [8.6; 13.5] | 0.897 |
| GDF-15 (ng/mL), median [Q1; Q3] | 0.94 [0.64; 1.47] | 1.04 [0.52; 1.53] | 0.849 |
| hsTnT (pg/mL), median [Q1; Q3] | 15 [12; 17.5] | 14 [10; 28] | 0.841 |
| IL-6R ά (ng/mL), median [Q1; Q3] | 68.5 [49.8; 82.1] | 50.2 [42.2; 57.1] | 0.726 |
| PCSK9 (ng/mL), median [Q1; Q3] | 339.8 [275.9; 418.2] | 314.3 [230.9; 371.3] | 0.682 |
| NT-pro-BNP (pg/mL), median [Q1; Q3] | 158.0 [99; 407] | 421.5 [147; 757] | 0.177 |
| uPAR (ng/mL), median [Q1; Q3] | 1.63 [1.30; 2.21] | 1.54 [1.18; 2.36] | 0.897 |
| LDL cholesterol (mmol/L), median [Q1; Q3] | 2.96 [2.67; 3.96] | 2.57 [2.23; 3.40] | 0.465 |
| Serum creatinine (µmol/L), median [Q1; Q3] | 85 [70.2; 95.0] | 72 [64.5; 99] | 0.234 |
| eGFR (mL/min/1.73 m2), median [Q1; Q3] | 78 [57; 85] | 80 [64; 88] | 0.308 |
| Hemoglobin (mg/dL), median [Q1; Q3] | 13.7 [13.3; 14.4] | 13.4 [12.4; 14.6] | 0.976 |
| hs-CRP (mg/L), median [Q1; Q3] | 1.85 [0.95; 4.66] | 2.87 [1.11; 5.62] | 0.742 |
| Vascular stiffness biomarkers | |||
| PI, median [Q1; Q3] | 1.33 [1.11; 1.44] | 1.29 [1.20; 1.39] | 0.968 |
| RI, median [Q1; Q3] | 0.70 [0.65; 0.74] | 0.69 [0.66; 0.72] | 0.936 |
| Echocardiographic data | |||
| LVEF (%), median [Q1; Q3] | 65.5 [62.8; 72.3] | 65 [61; 67.9] | 0.258 |
| LVEDD (mm), median [Q1; Q3] | 46 [43.4; 49] | 49 [46; 52] | 0.048 |
| IVS thickness in diastole (mm), median [Q1; Q3] | 13 [12; 15] | 12 [11; 13] | 0.105 |
| PW thickness in diastole (mm), median [Q1; Q3] | 12 [11; 13] | 11 [10; 12] | 0.054 |
| Left atrium area (cm2), median [Q1; Q3] | 23 [21; 26] | 24 [22; 27] | 0.352 |
| e’ medial velocity, median [Q1; Q3] | 7 [6.0; 9.0] | 8 [5.8; 9.3] | 0.89 |
| e’ lateral velocity, median [Q1; Q3] | 5.8 [5.0; 7.6] | 9.0 [6.8; 10.3] | 0.028 |
| E/e’, median [Q1; Q3] | 14 [9.0; 15.8] | 9.7 [8.0; 12.5] | 0.509 |
| OMT | SAVR | TAVR | p-Value | |
|---|---|---|---|---|
| N = 29 | N = 88 | N = 20 | ||
| Demographic data | ||||
| Age, years, ± SD | 69.8 ± 8.36 | 67.1 ± 7.46 | 79.7 ± 5.46 | <0.001 |
| BMI, ± SD | 30.7 ± 5.49 | 29.3 ± 5.84 | 29.5 ± 4.64 | 0.516 |
| Female, n (%) | 16 (53.3%) | 39 (44.3%) | 12 (63.2%) | 0.284 |
| Hypertension, n (%) | 28 (96.6%) | 82 (93.2%) | 20 (100%) | 0.626 |
| Type 2 Diabetes, n (%) | 8 (27.6%) | 27 (30.7%) | 5 (25.0%) | 0.86 |
| Hyperlipidemia, n (%) | 26 (89.7%) | 86 (97.7%) | 20 (100%) | 0.104 |
| Paroxysmal atrial fibrillation, n (%) | 6 (20.7%) | 7 (8.05%) | 8 (40.0%) | 0.001 |
| Smoking history, n (%) | 7 (24.1%) | 22 (25.0%) | 7 (35.0%) | 0.629 |
| Previous MI, n (%) | 1 (3.45%) | 8 (9.09%) | 2 (10.0%) | 0.65 |
| COPD, n (%) | 4 (13.8%) | 5 (5.68%) | 2 (10.0%) | 0.297 |
| CAD, n (%) | 7 (24.1%) | 14 (15.9%) | 7 (35.0%) | 0.145 |
| Previous PCI, n (%) | 1 (3.45%) | 0 (0.00%) | 1 (5.00%) | 0.126 |
| Previous CABG, n (%) | 8 (27.6%) | 14 (15.9%) | 5 (25.0%) | 0.289 |
| LEAD, n (%) | ||||
| Clinical symptom | 0 (0.00%) | 19 (21.6%) | 10 (50.0%) | <0.001 |
| NYHA III vs. I + II, n (%) | ||||
| Echocardiographic data | ||||
| Aortic valve area (cm2) ± SD | 1.36 ± 0.24 | 0.83 ± 0.22 | 0.81 ± 0.16 | <0.001 |
| Peak aortic velocity (m/s), 1 ± SD | 3.21 ± 0.45 | 4.62 ± 0.70 | 4.42 ± 0.71 | <0.001 |
| Mean aortic gradient (mmHg) ± SD | 24.9 ± 7.83 | 54.7 ± 17.5 | 49.0 ± 17.3 | <0.001 |
| LVEF (%), 1 ± SD | 63.7 ± 7.59 | 63.0 ± 7.60 | 61.0 ± 5.44 | 0.44 |
| Left ventricular end-diastolic diameter (mm) ± SD | 48.7 ± 5.02 | 47.0 ± 5.15 | 46.9 ± 5.11 | 0.288 |
| IVS thickness in diastole (mm), 1 ± SD | 12.3 ± 1.72 | 13.9 ± 2.15 | 13.9 ± 2.39 | 0.003 |
| PW thickness in diastole (mm), 1 ± SD | 11.2 ± 1.50 | 12.2 ± 1.82 | 12.2 ± 1.31 | 0.03 |
| Left atrium (cm2), 1 ± SD | 24.2 ± 3.92 | 24.3 ± 3.99 | 23.6 ± 3.55 | 0.673 |
| e’ medial, 1 ± SD | 7.67 ± 1.86 | 6.59 ± 2.03 | 6.20 ± 0.40 | 0.349 |
| e’ lateral, 1 ± SD | 8.67 ± 1.86 | 6.89 ± 2.68 | 8.10 ± 2.84 | 0.307 |
| E/e’, 1 ± SD | 11.7 ± 3.01 | 11.8 ± 2.71 | 11.9 ± 3.07 | 0.985 |
| Tricuspid regurgitant velocity (m/s), 1 ± SD | 2.56 ± 0.41 | 2.64 ± 0.45 | 2.73 ± 0.35 | 0.584 |
| Vascular stiffness parameters | ||||
| Resistive Index, median [Q1; Q3] | 0.69 [0.65; 0.72] | 0.67 [0.61; 0.71] | 0.74 [0.68; 0.77] | 0.018 |
| Pulsatile Index, median [Q1; Q3] | 1.29 [1.16; 1.39] | 1.22 [1.06; 1.36] | 1.46 [1.24; 1.59] | 0.02 |
| Biochemical parameters | ||||
| RANTES/CCL5 (ng/mL), median [Q1; Q3] | 26.7 [17.6; 36.3] | 29.9 [22.9; 40.7] | 32.8 [17.4; 45.1] | 0.591 |
| ET-1 (pg/mL), median [Q1; Q3] | 1.56 [1.44; 1.78] | 1.81 [1.59; 1.81] | 1.81 [1.81; 1.84] | 0.008 |
| Gal-3 (ng/mL), median [Q1; Q3] | 9.96 [8.7; 13.0] | 11.8 [9.6; 15.5] | 14.9 [11.7; 16.7] | 0.04 |
| GDF-15 (ng/mL), median [Q1; Q3] | 1.04 [0.53; 1.51] | 0.94 [0.62; 1.46] | 1.13 [0.84; 1.27] | 0.878 |
| hsTnT (pg/mL), median [Q1; Q3] | 14 [9.5; 22.0] | 13 [10.7; 20.0] | 17.5 [12.5; 33.2] | 0.085 |
| IL-6R ά (ng/mL), median [Q1; Q3] | 50.2 [42.3; 56.5] | 46.6 [38.8; 61.6] | 39.9 [31.6; 53.2] | 0.161 |
| PCSK9 (ng/mL), median [Q1; Q3] | 314 [232; 343] | 301 [253; 354] | 319 [296; 324] | 0.931 |
| NT-pro-BNP (pg/mL), median [Q1; Q3] | 422 [147; 757] | 392 [188; 784] | 998 [540; 1698] | 0.011 |
| uPAR (ng/mL), median [Q1; Q3] | 1.54 [1.19; 2.32] | 1.42 [1.15; 1.73] | 1.56 [1.23; 2.21] | 0.329 |
| Creatinine (µmol/L), median [Q1; Q3] | 72.0 [65.0; 98.0] | 79.0 [69.0; 92.2] | 88.5 [78.5; 107] | 0.026 |
| eGFR (mL/min/1.73 m2), median [Q1; Q3] | 80.0 [65.0; 88.0] | 77.0 [67.0; 89.0] | 56.5 [43.5; 69.8] | 0.001 |
| Hemoglobin (mg/dL), median [Q1; Q3] | 13.9 [12.6; 15.6] | 13.9 [13.0; 15.1] | 12.9 [11.9; 13.7] | 0.207 |
| Hs-CRP (mg/L), median [Q1; Q3] | 2.87 [1.27; 5.12] | 1.90 [1.06; 3.08] | 0.80 [0.55; 2.68] | 0.07 |
| Cardiovascular Death | CHF | |||
|---|---|---|---|---|
| Univariate Cox | Multivariate Cox | Univariate Cox | Multivariate Cox | |
| HR (95% CI), p-Value | HR (95% CI), p-Value | HR (95% CI), p-Value | HR (95% CI), p-Value | |
| Demographic data | ||||
| Age | 1.06 (1.0–1.13), 0.039 | 0.71 (0.54–0.90), 0.014 | 1.04 (0.98–1.09), 0.122 | - |
| BMI | 0.99 (0.90–1.10), 0.958 | - | 1.04 (0.96–1.12), 0.297 | - |
| Female gender | 0.91 (0.35–2.36), 0.846 | - | 3.20 (1.26–8.14), 0.014 | 1.69 (0.29–9.82), 0.556 |
| Hypertension | 0.76 (0.10–5.82), 0.800 | - | N/A | - |
| Diabetes | 1.01 (0.35–2.86), 0.987 | - | 1.13 (0.46–2.76), 0.782 | - |
| Paroxysmal atrial fibrillation | 2.25 (0.72–7.01), 0.161 | - | 3.66 (1.40–9.57), 0.008 | 0.95 (0.12–7.01), 0.957 |
| Smoking history | 1.58 (0.60–4.17), 0.352 | - | 0.59 (0.22–1.59), 0.299 | - |
| Previous MI | 0.78 (0.10–5.92), 0.812 | - | 1.39 (0.32–6.03), 0.659 | - |
| CAD | 1.19 (0.44–3.23), 0.729 | - | 1.45 (0.62–3.37), 0.380 | - |
| LEAD | 3.54 (1.36–9.23), 0.009 | 109 (4.06–2976), 0.005 | 0.75 (0.27–2.05), 0.581 | - |
| Clinical symptoms: | 2.88 (90.98–8.51), 0.055 | 0.05 (0.10–0.50), 0.023 | 1.23 (0.35–4.32), 0.743 | - |
| NYHA class III vs. I + II | ||||
| Echocardiographic data | ||||
| Aortic valve area | 1.17 (0.25–5.40), 0.840 | - | 1.03 (0.27-.396), 0.958 | - |
| LVEF | 1.00 (0.94–1.07), 0.890 | - | 1.02 (0.96–1.09), 0.474 | |
| LVEDD | 0.94 (0.84–1.04), 0.252 | - | 1.00 (0.92–1.09), 0.906 | - |
| IVS thickness in diastole | 1.19 (0.97–1.46), 0.080 | 1.00 (0.37–2.90), 0.928 | 1.03 90.86–1.25), 0.675 | - |
| PW thickness in diastole | 1.02 (0.78–1.35), 0.854 | - | 1.12 (0.91–1.39), 0.273 | - |
| Left atrium area | 1.04 (0.94–1.15), 0.369 | - | 1.09 (1.01–1.19), 0.039 | 1.05 (0.96–1.14), 0.221 |
| e’ medial | 0.69 (0.32–1.53), 0.368 | - | 1.04 (0.71–1.52), 0.825 | - |
| e’ lateral | 0.96 (0.58–1.59), 0.886 | - | 0.86 (0.58–1.27), 0.443 | - |
| E/e’ | 0.89 (0.70–1.15), 0.394 | - | 1.22 (1.04–1.42), 0.014 | 1.07 (0.86–1.32), 0.545 |
| Vascular stiffness parameters | ||||
| Increased VS (RI ≥ 0.7 and PI ≥ 1.3) | 1.72 (0.61–4.85), 0.304 | - | 2.80 (1.13–6.94), 0.026 | 2.25 (0.85–5.98), 0.110 |
| Biochemical parameters | ||||
| RANTES/CCL5 | 0.98 (0.95–1.02), 0.438 | - | 1.01 (0.99–1.03), 0.148 | - |
| ET-1 | 2.02 (0.96–4.25), 0.061 | 25.1 (1.03–611), 0.047 | 1.31 (0.57–2.94), 0.525 | - |
| Gal-3 > 11.5 ng/mL | 1.06 (0.96–1.17), 0.266 | - | 7.11 (2.11–24.0), 0.002 | 1.12 (1.01–1.25), 0.033 |
| GDF-15 | 1.74 (0.69–4.37), 0.237 | - | 0.75 (0.32–1.74), 0.508 | - |
| hsTnT | 1.97 (1.06–3.66), <0.001 | 1.12 (1.03–1.20), 0.010 | 1.01 (0.96–1.05), 0.959 | - |
| IL-6R ά | 1.03 (1.01–1.05), 0.009 | 1.07 (1.02–1.10), 0.006 | 1.01 (0.98–1.03), 0.481 | - |
| PCSK9 | 1.00 (0.99–1.01), 0.474 | - | 1.03 (0.99–1.08), 0.129 | - |
| NT-pro-BNP > 500 ng/mL | 5.21 (1.49–18.1), 0.009 | 1.54 (0.24–10.1), 0.647 | 1.00 (0.99–1.04), 0.345 | - |
| uPAR | 1.05 90.87–1.27), 0.581 | - | 0.99 (0.74–1.33), 0.987 | - |
| Serum creatinine | 1.02 (1.01–1.04), 0.009 | 1.06 (1.0–1.13), 0.039 | 1.01 (0.98–1.03), 0.326 | - |
| eGFR | 0.97 (0.95–0.99, 0.037 | 0.87 (0.78–1.00), 0.015 | 0.97 (0.95–1.04), 0.053 | 0.98 (0.96–1.01), 0.377 |
| LDL | 0.83 (0.49–1.41), 0.496 | - | 1.26 (0.85–1.87), 0.247 | - |
| HDL | 0.47 (0.11–2.09), 0.322 | - | 0.96 (0.29–3.07), 0.946 | - |
| hs-CRP | 0.86 (0.60–1.22), 0.407 | - | 1.00 (0.77–1.15), 0.947 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baran, J.; Niewiara, Ł.; Podolec, J.; Siedliński, M.; Józefczuk, E.; Bernacik, A.; Badacz, R.; Przewłocki, T.; Pieniążek, P.; Żmudka, K.; et al. Serum and Vascular Stiffness Biomarkers Associated with the Severity of Degenerative Aortic Valve Stenosis and Cardiovascular Outcomes. J. Cardiovasc. Dev. Dis. 2022, 9, 193. https://doi.org/10.3390/jcdd9060193
Baran J, Niewiara Ł, Podolec J, Siedliński M, Józefczuk E, Bernacik A, Badacz R, Przewłocki T, Pieniążek P, Żmudka K, et al. Serum and Vascular Stiffness Biomarkers Associated with the Severity of Degenerative Aortic Valve Stenosis and Cardiovascular Outcomes. Journal of Cardiovascular Development and Disease. 2022; 9(6):193. https://doi.org/10.3390/jcdd9060193
Chicago/Turabian StyleBaran, Jakub, Łukasz Niewiara, Jakub Podolec, Mateusz Siedliński, Ewelina Józefczuk, Anna Bernacik, Rafał Badacz, Tadeusz Przewłocki, Piotr Pieniążek, Krzysztof Żmudka, and et al. 2022. "Serum and Vascular Stiffness Biomarkers Associated with the Severity of Degenerative Aortic Valve Stenosis and Cardiovascular Outcomes" Journal of Cardiovascular Development and Disease 9, no. 6: 193. https://doi.org/10.3390/jcdd9060193
APA StyleBaran, J., Niewiara, Ł., Podolec, J., Siedliński, M., Józefczuk, E., Bernacik, A., Badacz, R., Przewłocki, T., Pieniążek, P., Żmudka, K., Legutko, J., & Kabłak-Ziembicka, A. (2022). Serum and Vascular Stiffness Biomarkers Associated with the Severity of Degenerative Aortic Valve Stenosis and Cardiovascular Outcomes. Journal of Cardiovascular Development and Disease, 9(6), 193. https://doi.org/10.3390/jcdd9060193