
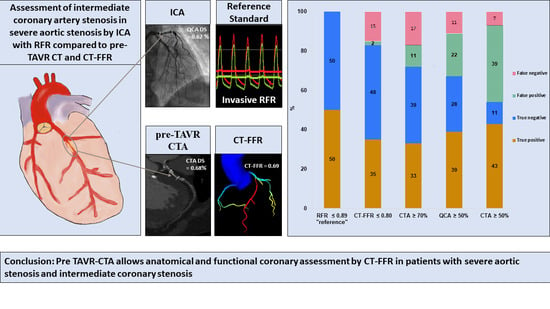
Feasibility and Comparison of Resting Full-Cycle Ratio and Computed Tomography Fractional Flow Reserve in Patients with Severe Aortic Valve Stenosis

 , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Acquisition and Analysis CT Datasets (CT-TAVR Image Reconstruction)
2.3. CT-FFR Analysis
2.4. Invasive Coronary Angiogram and Resting Full Cycle Ratio Measurement
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Scan Demographics and CT-Assessment
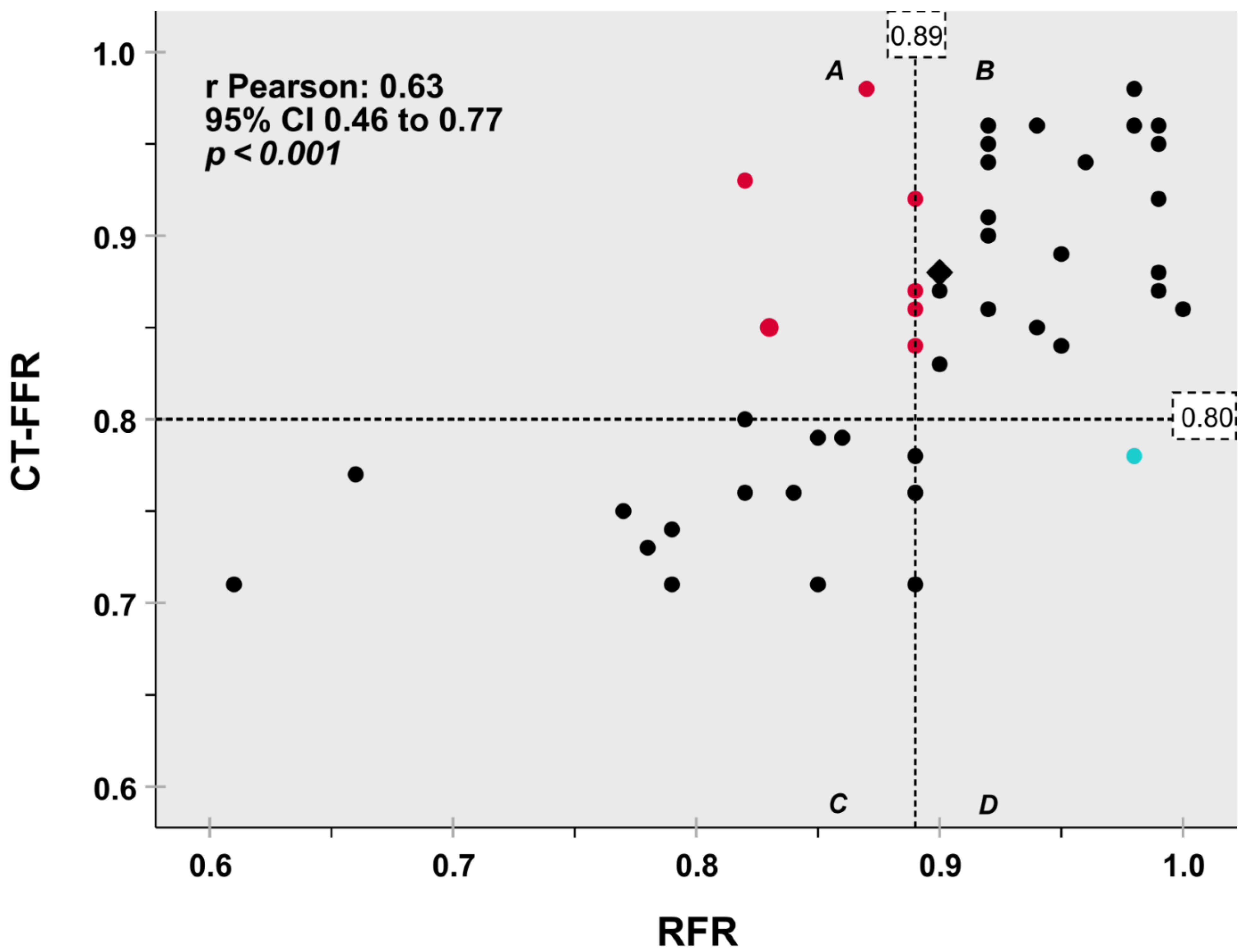
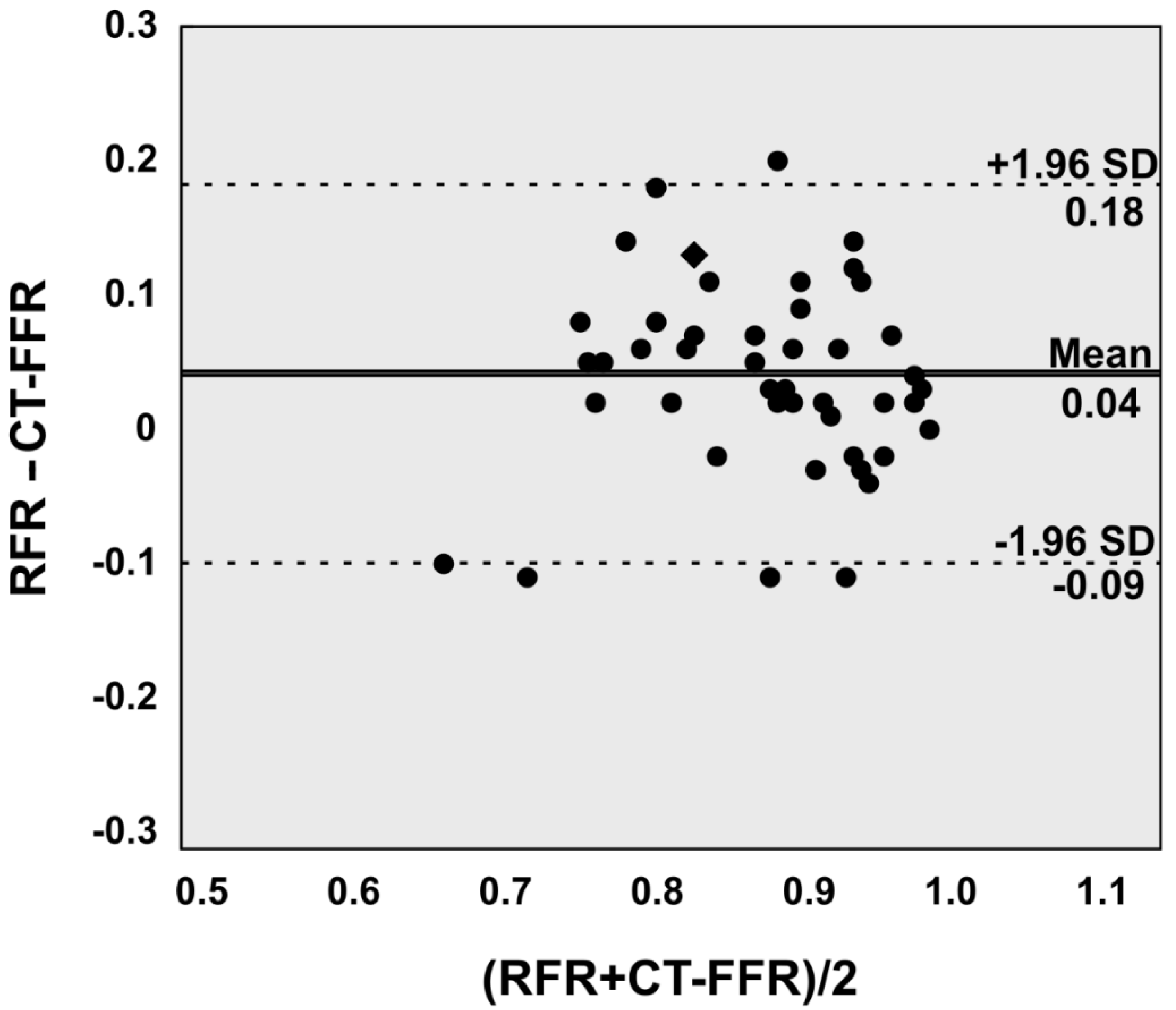
3.3. Correlation between CT-FFR and RFR and Anatomic Grading
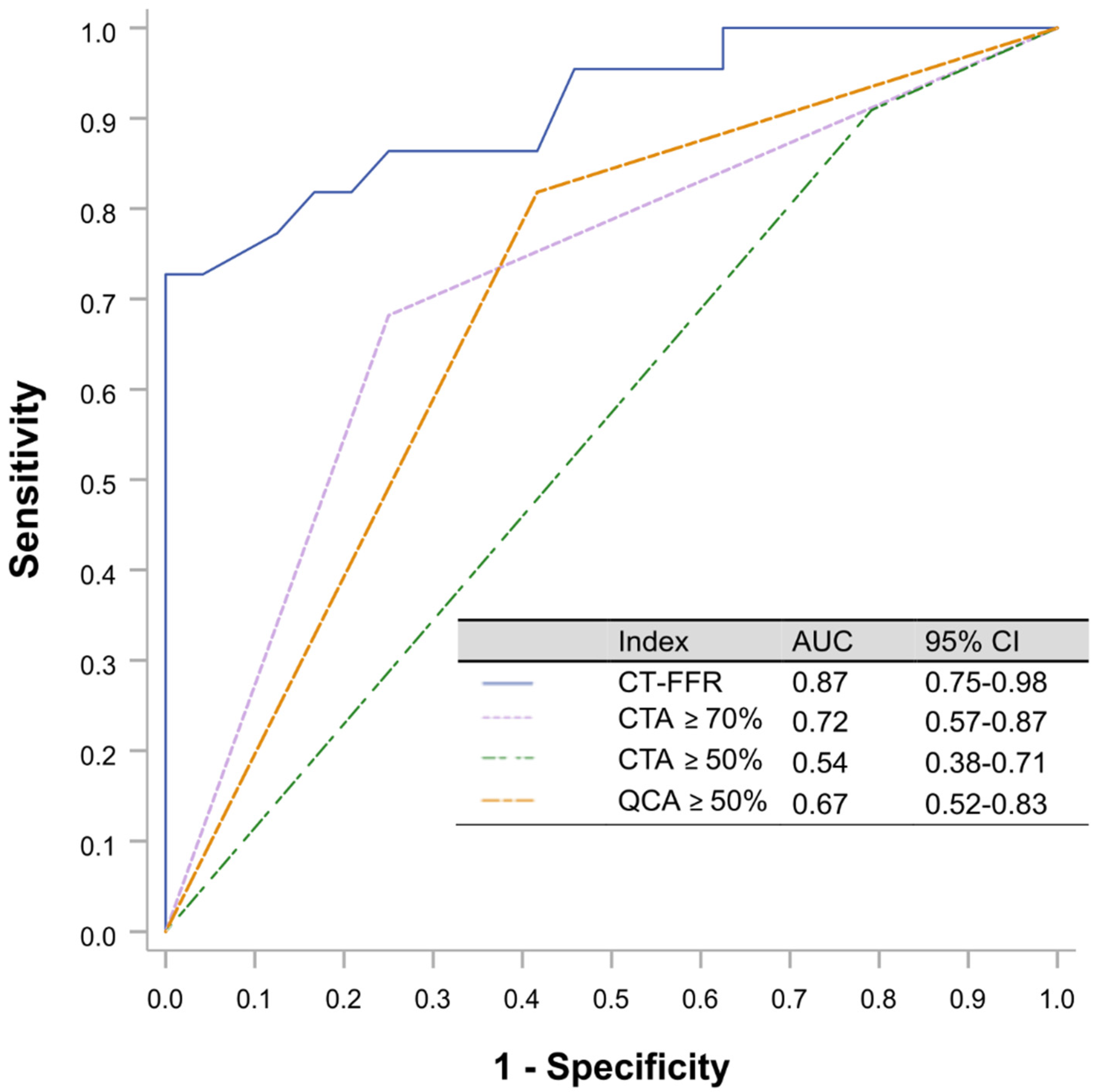
3.4. Diagnostic Accuracy of CT-FFR and CT
4. Discussion
- (i)
- The utilization of routine TAVR-CTs for the analysis of CT-FFR is technically feasible and allows for the assessment of CAD in patients with AS even without a specific coronary imaging protocol.
- (ii)
- Compared with anatomical assessment, either by CT or QCA, functional assessment utilizing CT-FFR is superior in predicting ischemic lesions as classified by invasive physiological assessment with RFR.
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; Bonis, M.; de Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Sankaramangalam, K.; Banerjee, K.; Kandregula, K.; Mohananey, D.; Parashar, A.; Jones, B.M.; Jobanputra, Y.; Mick, S.; Krishnaswamy, A.; Svensson, L.G.; et al. Impact of Coronary Artery Disease on 30-Day and 1-Year Mortality in Patients Undergoing Transcatheter Aortic Valve Replacement: A Meta-Analysis. J. Am. Heart Assoc. 2017, 6, e006092. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Bartorelli, A.L.; Ballerini, G.; Bertella, E.; Segurini, C.; Conte, E.; Annoni, A.; Baggiano, A.; et al. Diagnostic accuracy of multidetector computed tomography coronary angiography in 325 consecutive patients referred for transcatheter aortic valve replacement. Am. Heart J. 2014, 168, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Meier, D.; Depierre, A.; Topolsky, A.; Roguelov, C.; Dupré, M.; Rubimbura, V.; Eeckhout, E.; Qanadli, S.D.; Muller, O.; Mahendiran, T.; et al. Computed Tomography Angiography for the Diagnosis of Coronary Artery Disease Among Patients Undergoing Transcatheter Aortic Valve Implantation. J. Cardiovasc. Trans. Res. 2021, 14, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Chava, S.; Gentchos, G.; Abernethy, A.; Leavitt, B.; Terrien, E.; Dauerman, H.L. Routine CT angiography to detect severe coronary artery disease prior to transcatheter aortic valve replacement. J. Thromb Thrombolysis 2017, 44, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.L.; Bruyne, B.; de Pijls, N.H.J.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.L.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; Maccarthy, P.A.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Götberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.-E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to Guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef]
- Pijls, N.H.; Bruyne, B.; de Peels, K.; van der Voort, P.H.; Bonnier, H.J.; Bartunek JKoolen, J.J.; Koolen, J.J. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N. Engl. J. Med. 1996, 334, 1703–1708. [Google Scholar] [CrossRef]
- Svanerud, J.; Ahn, J.-M.; Jeremias, A.; van’t Veer, M.; Gore, A.; Maehara, A.; Crowley, A.; Pijls, N.H.J.; Bruyne, B.; de Johnson, N.P.; et al. Validation of a novel non-hyperaemic index of coronary artery stenosis severity: The Resting Full-cycle Ratio (VALIDATE RFR) study. EuroIntervention 2018, 14, 806–814. [Google Scholar] [CrossRef]
- Marin, F.; Scarsini, R.; Kotronias, R.A.; Printzios, D.T.; Burrage, M.K.; Bray, J.J.H.; Ciofani, J.L.; Venturi, G.; Pighi, M.; Maria GL de Banning, A.P. Aortic Valve Disease and Associated Complex CAD: The Interventional Approach. J. Clin. Med. 2021, 10, 946. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.-K.; Erglis, A.; Doh, J.-H.; Daniels, D.V.; Jegere, S.; Kim, H.-S.; Dunning, A.; DeFrance, T.; Lansky, A.; Leipsic, J.; et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J. Am. Coll. Cardiol. 2011, 58, 1989–1997. [Google Scholar] [PubMed]
- Nørgaard, B.L.; Leipsic, J.; Gaur, S.; Seneviratne, S.; Ko, B.S.; Ito, H.; Jensen, J.M.; Mauri, L.; Bruyne, B.; de Bezerra, H.; et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: The NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps). J. Am. Coll. Cardiol. 2014, 63, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Michail, M.; Ihdayhid, A.R.; Brown, A.J.; Ko, B. Discordance of intracoronary pressure-based indices in severe angiographic stenosis: Are we missing the flow? Cardiovasc. Interv. Ther. 2020, 35, 304–305. [Google Scholar] [CrossRef] [PubMed]
- Tesche, C.; Cecco CN de Baumann, S.; Renker, M.; McLaurin, T.W.; Duguay, T.M.; Bayer, R.R.; Steinberg, D.H.; Grant, K.L.; Canstein, C.; Schwemmer, C.; et al. Coronary CT Angiography-derived Fractional Flow Reserve: Machine Learning Algorithm versus Computational Fluid Dynamics Modeling. Radiology 2018, 288, 64–72. [Google Scholar] [CrossRef]
- Achenbach, S.; Delgado, V.; Hausleiter, J.; Schoenhagen, P.; Min, J.K.; Leipsic, J.A. SCCT expert consensus document on computed tomography imaging before transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR). J. Cardiovasc. Comput. Tomogr. 2012, 6, 366–380. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Davies, J.E.; Sen, S.; Dehbi, H.-M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef]
- Bruyne, B.; de Fearon, W.F.; Pijls, N.H.J.; Barbato, E.; Tonino, P.; Piroth, Z.; Jagic, N.; Mobius-Winckler, S.; Rioufol, G.; Witt, N.; et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N. Engl. J. Med. 2014, 371, 1208–1217. [Google Scholar] [CrossRef]
- Yamanaka, F.; Shishido, K.; Ochiai, T.; Moriyama, N.; Yamazaki, K.; Sugitani, A.; Tani, T.; Tobita, K.; Mizuno, S.; Tanaka, Y.; et al. Instantaneous Wave-Free Ratio for the Assessment of Intermediate Coronary Artery Stenosis in Patients With Severe Aortic Valve Stenosis: Comparison With Myocardial Perfusion Scintigraphy. JACC Cardiovasc. Interv. 2018, 11, 2032–2040. [Google Scholar] [CrossRef]
- Ahmad, Y.; Götberg, M.; Cook, C.; Howard, J.P.; Malik, I.; Mikhail, G.; Frame, A.; Petraco, R.; Rajkumar, C.; Demir, O.; et al. Coronary Hemodynamics in Patients With Severe Aortic Stenosis and Coronary Artery Disease Undergoing Transcatheter Aortic Valve Replacement: Implications for Clinical Indices of Coronary Stenosis Severity. JACC Cardiovasc. Interv. 2018, 11, 2019–2031. [Google Scholar] [CrossRef] [PubMed]
- Wiegerinck, E.M.A.; van de Hoef, T.P.; Rolandi, M.C.; Yong, Z.; van Kesteren, F.; Koch, K.T.; Vis, M.M.; Mol BAJM de Piek, J.J.; Baan, J. Impact of Aortic Valve Stenosis on Coronary Hemodynamics and the Instantaneous Effect of Transcatheter Aortic Valve Implantation. Circ. Cardiovasc. Interv. 2015, 8, e002443. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, M.; Yonetsu, T.; Sugiyama, T.; Kanaji, Y.; Hamaya, R.; Kanno, Y.; Hada, M.; Yamaguchi, M.; Sumino, Y.; Usui, E.; et al. All Resting Physiological Indices May Not Be Equivalent—Comparison Between the Diastolic Pressure Ratio and Resting Full-Cycle Ratio. Circ. J. 2020, 84, 1147–1154. [Google Scholar] [CrossRef]
- Rajappan, K.; Rimoldi, O.E.; Dutka, D.P.; Ariff, B.; Pennell, D.J.; Sheridan, D.J.; Camici, P.G. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation 2002, 105, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Lumley, M.; Williams, R.; Asrress, K.N.; Arri, S.; Briceno, N.; Ellis, H.; Rajani, R.; Siebes, M.; Piek, J.J.; Clapp, B.; et al. Coronary Physiology During Exercise and Vasodilation in the Healthy Heart and in Severe Aortic Stenosis. J. Am. Coll. Cardiol. 2016, 68, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Sabbah, M.; Joshi, F.R.; Minkkinen, M.; Holmvang, L.; Tilsted, H.-H.; Pedersen, F.; Ahtarovski, K.; Sørensen, R.; Thue Olsen, N.; Søndergaard, L.; et al. Long-Term Changes in Invasive Physiological Pressure Indices of Stenosis Severity Following Transcatheter Aortic Valve Implantation. Circ. Cardiovasc. Interv. 2021, 15, e011331. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Du, X.-M.; Jin, Z.-T.; Peng, Z.-H.; Ding, J.; Li, L. The diagnostic performance of coronary artery angiography with 64-MSCT and post 64-MSCT: Systematic review and meta-analysis. PLoS ONE 2014, 9, e84937. [Google Scholar] [CrossRef]
- Nicol, E.D.; Schultz, C.; Stirrup, J.; Roughton, M.; Padley, S.P.G.; Rubens, M.B.; Davies, S.W.; Di Mario, C. Defining the appropriate CTA stenosis threshold for gatekeeping to invasive angiography: 50% or 70%? Int. J. Cardiol. 2010, 144, 297–298. [Google Scholar] [CrossRef]
- Budoff, M.J.; Nakazato, R.; Mancini, G.B.J.; Gransar, H.; Leipsic, J.; Berman, D.S.; Min, J.K. CT Angiography for the Prediction of Hemodynamic Significance in Intermediate and Severe Lesions: Head-to-Head Comparison With Quantitative Coronary Angiography Using Fractional Flow Reserve as the Reference Standard. JACC Cardiovasc. Imaging 2016, 9, 559–564. [Google Scholar] [CrossRef]
- Tu, S.; Barbato, E.; Köszegi, Z.; Yang, J.; Sun, Z.; Holm, N.R.; Tar, B.; Li, Y.; Rusinaru, D.; Wijns, W.; et al. Fractional flow reserve calculation from 3-dimensional quantitative coronary angiography and TIMI frame count: A fast computer model to quantify the functional significance of moderately obstructed coronary arteries. JACC Cardiovasc. Interv. 2014, 7, 768–777. [Google Scholar] [CrossRef]
- Xu, B.; Tu, S.; Qiao, S.; Qu, X.; Chen, Y.; Yang, J.; Guo, L.; Sun, Z.; Li, Z.; Tian, F.; et al. Diagnostic Accuracy of Angiography-Based Quantitative Flow Ratio Measurements for Online Assessment of Coronary Stenosis. J. Am. Coll. Cardiol. 2017, 70, 3077–3087. [Google Scholar] [CrossRef] [PubMed]
- Westra, J.; Andersen, B.K.; Campo, G.; Matsuo, H.; Koltowski, L.; Eftekhari, A.; Liu, T.; Di Serafino, L.; Di Girolamo, D.; Escaned, J.; et al. Diagnostic Performance of In-Procedure Angiography-Derived Quantitative Flow Reserve Compared to Pressure-Derived Fractional Flow Reserve: The FAVOR II Europe-Japan Study. J. Am. Heart Assoc. 2018, 7, e009603. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Tu, S.; Song, L.; Jin, Z.; Yu, B.; Fu, G.; Zhou, Y.; Wang, J.; Chen, Y.; Pu, J.; et al. Angiographic quantitative flow ratio-guided coronary intervention (FAVOR III China): A multicentre, randomised, sham-controlled trial. Lancet 2021, 398, 2149–2159. [Google Scholar] [CrossRef]
- Mejía-Rentería, H.; Nombela-Franco, L.; Paradis, J.-M.; Lunardi, M.; Lee, J.M.; Amat-Santos, I.J.; Veiga Fernandez, G.; Kalra, A.; Bansal, E.J.; La Torre Hernandez, J.M.; et al. Angiography-based quantitative flow ratio versus fractional flow reserve in patients with coronary artery disease and severe aortic stenosis. EuroIntervention 2020, 16, e285–e292. [Google Scholar] [CrossRef]
- Opolski, M.P.; Kim, W.-K.; Liebetrau, C.; Walther, C.; Blumenstein, J.; Gaede, L.; Kempfert, J.; van Linden, A.; Walther, T.; Hamm, C.W.; et al. Diagnostic accuracy of computed tomography angiography for the detection of coronary artery disease in patients referred for transcatheter aortic valve implantation. Clin. Res. Cardiol. 2015, 104, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Gohmann, R.F.; Pawelka, K.; Seitz, P.; Majunke, N.; Heiser, L.; Renatus, K.; Desch, S.; Lauten, P.; Holzhey, D.; Noack, T.; et al. Combined Coronary CT-Angiography and TAVR Planning for Ruling Out Significant Coronary Artery Disease: Added Value of Machine-Learning-Based CT-FFR. JACC Cardiovasc. Imaging 2021, 15, 476–486. [Google Scholar] [CrossRef] [PubMed]
- Brandt, V.; Schoepf, U.J.; Aquino, G.J.; Bekeredjian, R.; Varga-Szemes, A.; Emrich, T.; Bayer, R.R.; Schwarz, F.; Kroencke, T.J.; Tesche, C.; et al. Impact of machine-learning-based coronary computed tomography angiography–derived fractional flow reserve on decision-making in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Radiol. 2022. [Google Scholar] [CrossRef]
- Koo, B.-K.; Yang, H.-M.; Doh, J.-H.; Choe, H.; Lee, S.-Y.; Yoon, C.-H.; Cho, Y.-K.; Nam, C.-W.; Hur, S.-H.; Lim, H.-S.; et al. Optimal intravascular ultrasound criteria and their accuracy for defining the functional significance of intermediate coronary stenoses of different locations. JACC Cardiovasc. Interv. 2011, 4, 803–811. [Google Scholar] [CrossRef]
- Patel, M.R.; Nørgaard, B.L.; Fairbairn, T.A.; Nieman, K.; Akasaka, T.; Berman, D.S.; Raff, G.L.; Hurwitz Koweek, L.M.; Pontone, G.; Kawasaki, T.; et al. 1-Year Impact on Medical Practice and Clinical Outcomes of FFRCT: The ADVANCE Registry. JACC Cardiovasc. Imaging. 2020, 13, 97–105. [Google Scholar] [CrossRef]
- Baumann, S.; Hirt, M.; Rott, C.; Özdemir, G.H.; Tesche, C.; Becher, T.; Weiss, C.; Hetjens, S.; Akin, I.; Schoenberg, S.O.; et al. Comparison of Machine Learning Computed Tomography-Based Fractional Flow Reserve and Coronary CT Angiography-Derived Plaque Characteristics with Invasive Resting Full-Cycle Ratio. J. Clin. Med. 2020, 9, 714. [Google Scholar] [CrossRef]
- Baumann, S.; Hirt, M.; Schoepf, U.J.; Rutsch, M.; Tesche, C.; Renker, M.; Golden, J.W.; Buss, S.J.; Becher, T.; Bojara, W.; et al. Correlation of machine learning computed tomography-based fractional flow reserve with instantaneous wave free ratio to detect hemodynamically significant coronary stenosis. Clin. Res. Cardiol. 2020, 109, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, S.; Kawasaki, T.; Kumamaru, K.K.; Kawaguchi, Y.; Dohi, T.; Okonogi, T. Diagnostic performance of on-site computed CT-fractional flow reserve based on fluid structure interactions: Comparison with invasive fractional flow reserve and instantaneous wave-free ratio. Eur. Heart J. Cardiovasc. Imaging 2018, 20, 343–352. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | |
| Age (years) | 80.9 ± 6.2 |
| Body-mass index | 26.6 ± 5.1 |
| Body-surface area | 1.8 ± 0.2 |
| Female sex | 19 (46.3) |
| Cardiovascular risk factors and concomitant diseases | |
| Hypertension | 34 (82.9) |
| Dyslipidemia | 23 (56.1) |
| Diabetes mellitus | 14 (34.1) |
| Peripheral artery disease or extracardiac arteriopathy | 7 (17.1) |
| Prior myocardial infarction | 1 (2.4) |
| Atrial fibrillation | 8 (19.5) |
| Chronic obstructive lung disease | 5 (12.2) |
| Baseline blood values | |
| Serum creatinine—mg/dL | 1.1 ± 0.4 |
| Hemoglobin—g/dL | 12.7 ± 1.59 |
| Echocardiography | |
| Ejection fraction | |
| Normal (>50%) | 38 (92.7) |
| Mild dysfunction (41–50%) | 3 (7.3) |
| Aortic valve mean gradient—mmHg | 48.1 ± 14.4 |
| Aortic valve maximum gradient—mmHg | 77.5 ± 20.2 |
| Peak aortic jet velocity—cm/s | 431.6 ± 63.0 |
| Aortic valve area—cm2 | 0.74 ± 0.17 |
| Risk Scores | |
| LogEuroSCORE I—% | 14.3 ± 8.8 |
| EuroSCORE II—% | 3.5 ± 2.7 |
| Values are mean ± SD or n (%) | |
| Lesion Characteristics and Physiological Assessments (n = 46) | |
|---|---|
| Prior revascularisation in any vessel | 3 (6.5) |
| Prior stents in examined vessel | 0 |
| Measured vessel location territory | |
| Left anterior descending | 32 (69.6) |
| Left circumflex artery | 8 (17.4) |
| Ramus intermedius | 1 (2.2) |
| Right coronary artery | 5 (10.9) |
| Multivessel disease (n = 41) | 19 (46.3) |
| SYNTAX Score (n = 41) | 11.2 ± 6.2 |
| Quantitative coronary angiography | |
| Diameter stenosis, % | 48.6 ± 9.2 |
| Cardiac computed tomography angiography | |
| Diameter stenosis, % | |
| 20–49% | 4 (8.7) |
| 50–69% | 29 (63.0) |
| 70–90% | 13 (28.3) |
| Functional indexes | |
| Resting full-cycle ratio | |
| Left anterior descending | 0.87 ± 0.08 |
| 0.89 (0.84–0.92) | |
| Left circumflex artery | 0.92 ± 0.06 |
| 0.94 (0.86–0.98) | |
| Ramus intermedius | 0.94 |
| Right coronary artery | 0.91 ± 0.08 |
| 0.92 (0.82–0.99) | |
| CT-Fractional Flow Reserve | |
| Left anterior descending | 0.84 ± 0.08 |
| 0.85 (0.76–0.91) | |
| Left circumflex artery | 0.84 ± 0.1 |
| 0.82 (0.76–0.94) | |
| Ramus intermedius | 0.85 |
| Right coronary artery | 0.88 ± 0.06 |
| 0.87 (0.83–0.93) | |
| CT-FFR ≤ 0.80 | CTA ≥ 50% | CTA ≥ 70% | QCA ≥ 50% | |
|---|---|---|---|---|
| % Sensitivity | 69.6 (47.1−86.8) | 86.9 (66.4−97.2) | 65.2 (42.7−83.6) | 78.3 (56.3−92.5) |
| % Specificity | 95.7 (78.1−99.9) | 21.7 (7.5−43.7) | 78.3 (56.3−92.5) | 56.4 (34.5−76.7) |
| Positive Likelihood Ratio | 16.0 (2.3−110.9) | 1.1 (0.9−1.5) | 3.0 (1.3−6.9) | 1.8 (1.1−3.0) |
| Negative Likelihood Ratio | 0.32 (0.17−0.59) | 0.60 (0.16−2.22) | 0.44 (0.24−0.81) | 0.38 (0.16−0.90) |
| % Positive predictive value | 94.1 (69.8−99.1) | 52.6 (45.9−59.2) | 75 (56.7−87.3) | 64.3 (51.9−75) |
| % Negative predictive value | 75.9 (62.7−85.4) | 62.5 (31−86.1) | 69.2 (55.3−80.4) | 72.2 (52.5−85.9) |
| % Accuracy | 82.6 (68.6−92.2) | 54.4 (39−69.1) | 71.7 (56.5−84.0) | 67.4 (51.9−80.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wienemann, H.; Langenbach, M.C.; Mauri, V.; Banazadeh, M.; Klein, K.; Hohmann, C.; Lee, S.; Breidert, I.; Hof, A.; Eghbalzadeh, K.; et al. Feasibility and Comparison of Resting Full-Cycle Ratio and Computed Tomography Fractional Flow Reserve in Patients with Severe Aortic Valve Stenosis. J. Cardiovasc. Dev. Dis. 2022, 9, 116. https://doi.org/10.3390/jcdd9040116
Wienemann H, Langenbach MC, Mauri V, Banazadeh M, Klein K, Hohmann C, Lee S, Breidert I, Hof A, Eghbalzadeh K, et al. Feasibility and Comparison of Resting Full-Cycle Ratio and Computed Tomography Fractional Flow Reserve in Patients with Severe Aortic Valve Stenosis. Journal of Cardiovascular Development and Disease. 2022; 9(4):116. https://doi.org/10.3390/jcdd9040116
Chicago/Turabian StyleWienemann, Hendrik, Marcel C. Langenbach, Victor Mauri, Maryam Banazadeh, Konstantin Klein, Christopher Hohmann, Samuel Lee, Isabel Breidert, Alexander Hof, Kaveh Eghbalzadeh, and et al. 2022. "Feasibility and Comparison of Resting Full-Cycle Ratio and Computed Tomography Fractional Flow Reserve in Patients with Severe Aortic Valve Stenosis" Journal of Cardiovascular Development and Disease 9, no. 4: 116. https://doi.org/10.3390/jcdd9040116
APA StyleWienemann, H., Langenbach, M. C., Mauri, V., Banazadeh, M., Klein, K., Hohmann, C., Lee, S., Breidert, I., Hof, A., Eghbalzadeh, K., Kuhn, E., Halbach, M., Maintz, D., Baldus, S., Bunck, A., & Adam, M. (2022). Feasibility and Comparison of Resting Full-Cycle Ratio and Computed Tomography Fractional Flow Reserve in Patients with Severe Aortic Valve Stenosis. Journal of Cardiovascular Development and Disease, 9(4), 116. https://doi.org/10.3390/jcdd9040116