
The Relevance of Heart Rate Fluctuation When Evaluating Atrial Substrate Electrical Features in Catheter Ablation of Paroxysmal Atrial Fibrillation

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Methods
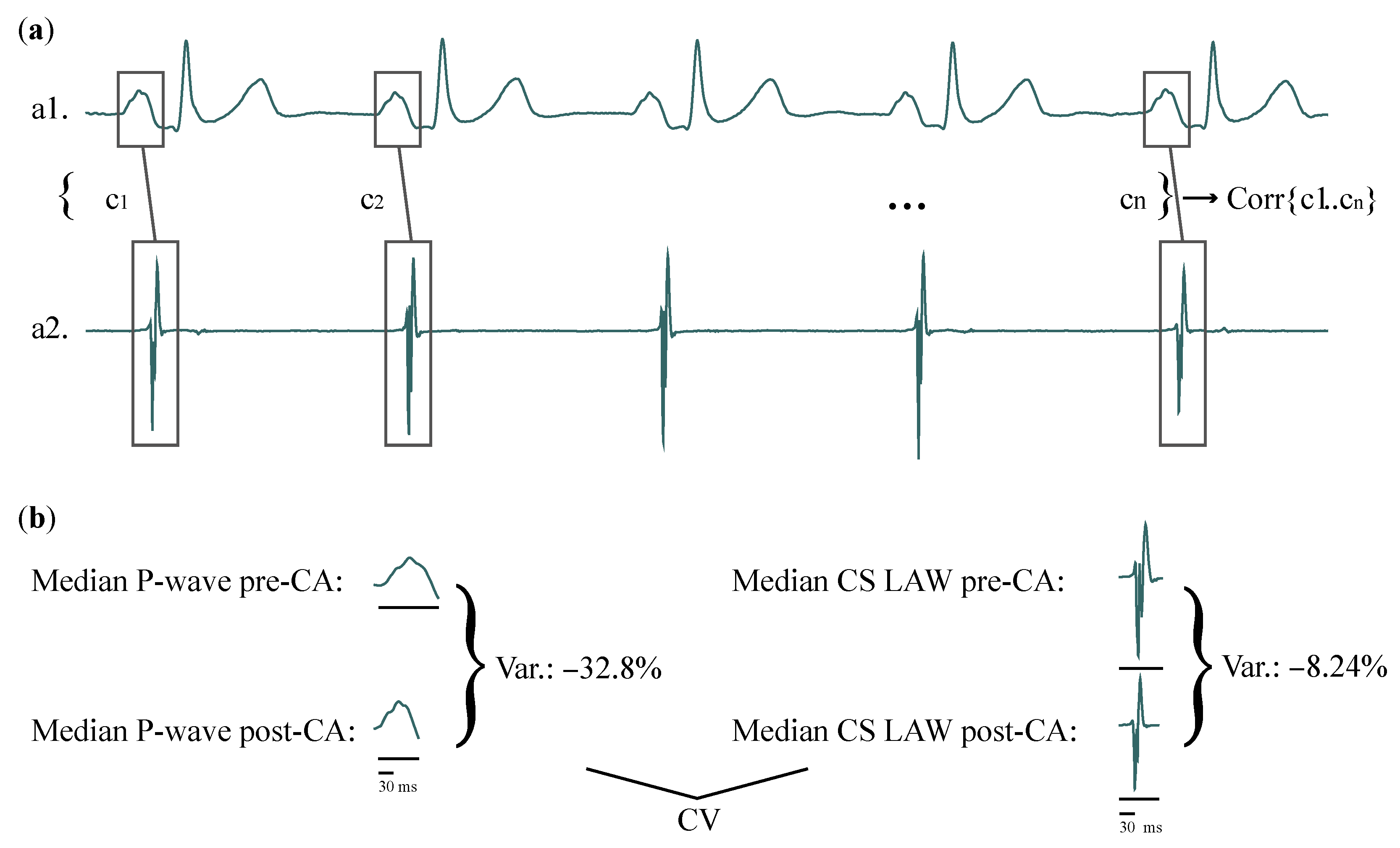
2.1. Preprocessing
2.2. Data Analysis
- Duration: Once delineated, the interval between the onset and offset of each activation was considered as its duration.
- Amplitude: Maximum () and peak-to-peak (PP) amplitudes. For ECGs, P-wave and PP concur, since P-waves in lead II are positive. The root mean square (RMS) is the quadratic mean of the function that defines each activation.
- Area: Area of the positive parts of the signal (PosAr), calculated by the integration over the time interval of the amplitude of each activation with the trapezoidal method.
- Slope rate: Increasing or decreasing rhythm at of total duration of each P-wave/LAW, as well as at its maximum point, calculated as:where is the amplitude at or the peak of the activation, is the amplitude at the onset, and and are the sample points at or the peak and the onset, respectively. Slope rate is always positive for P-waves, as their peaks always present a positive amplitude. For LAWs, slope rate can be negative as well.
2.3. Statistical Analysis
3. Results
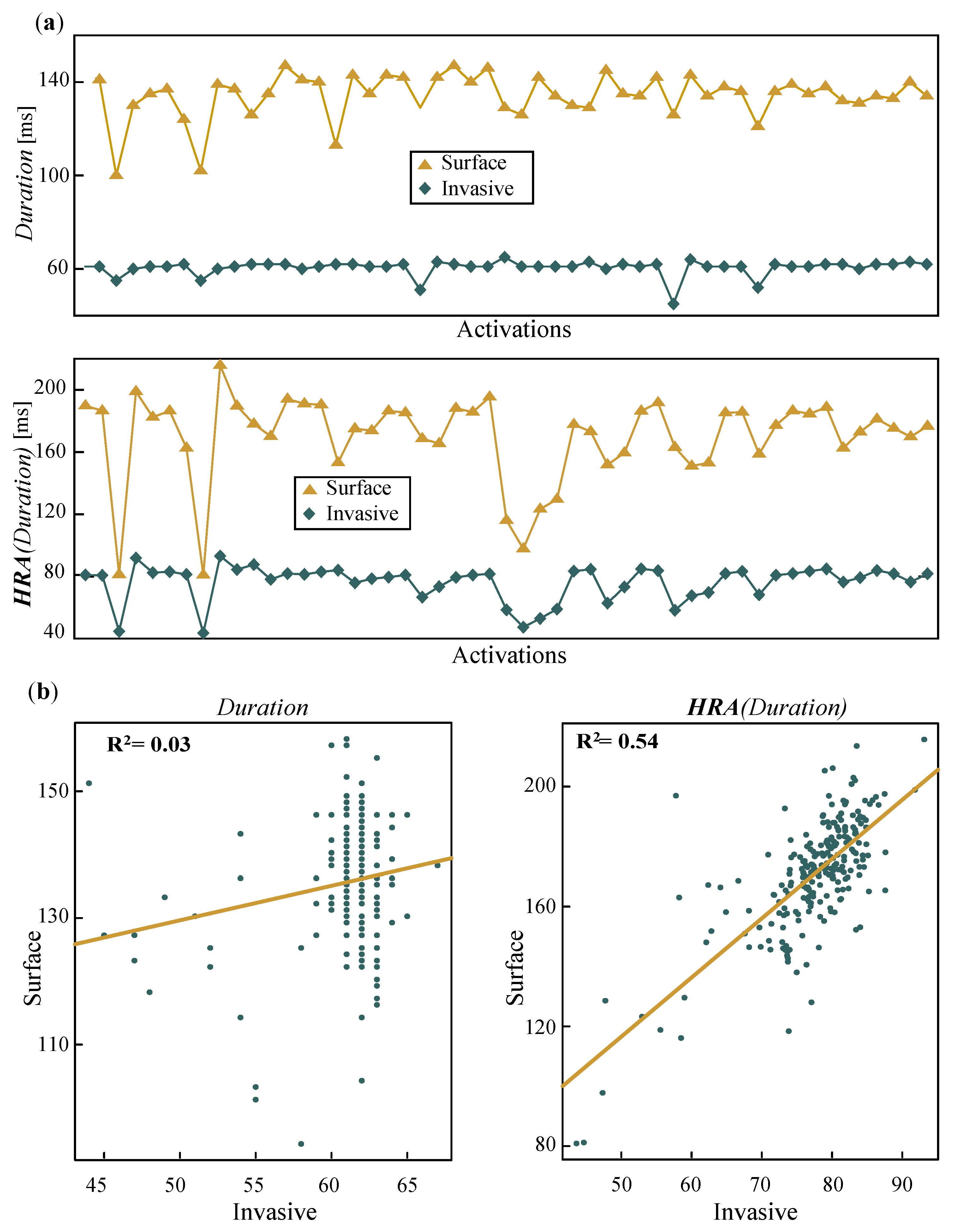
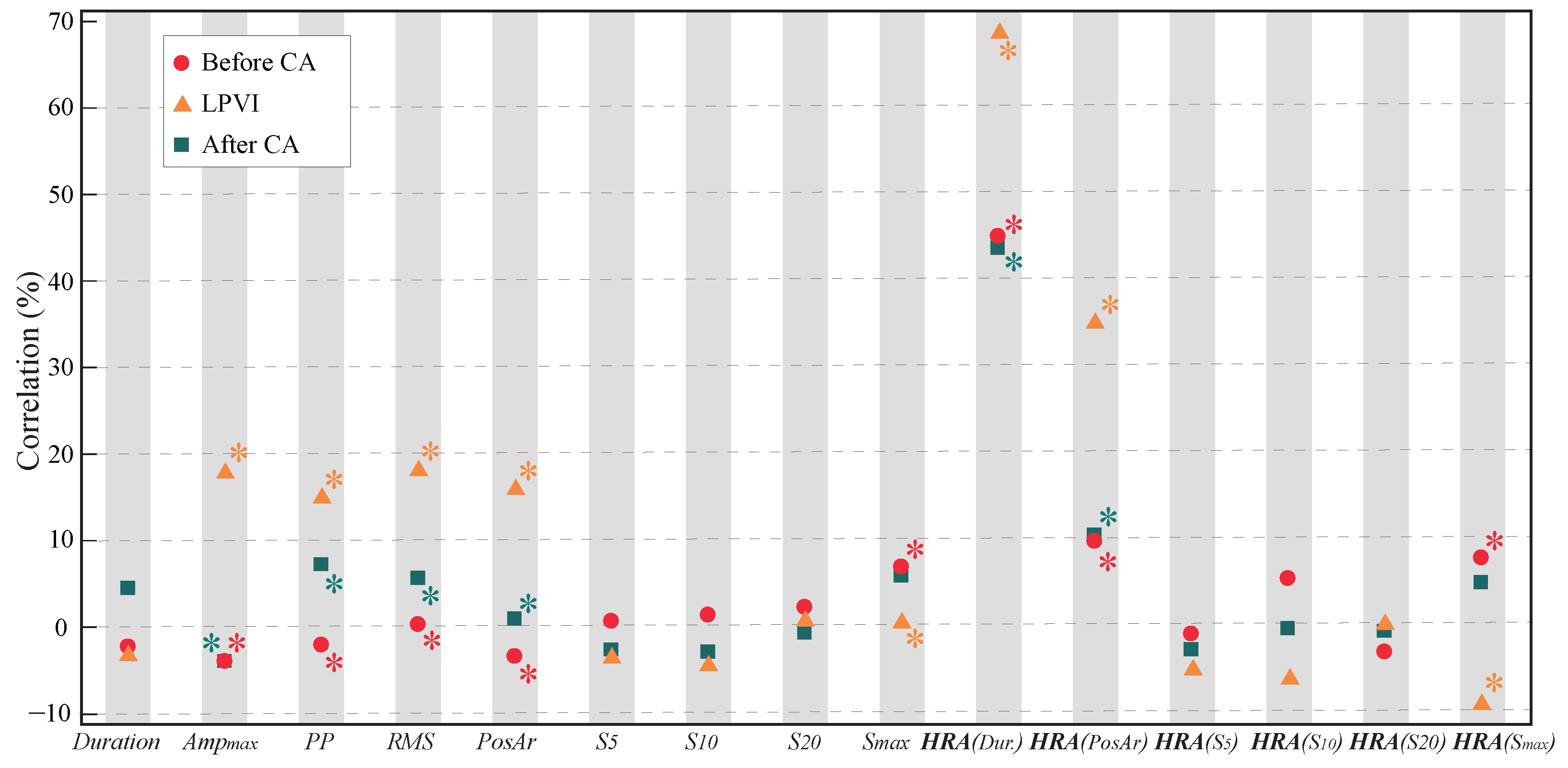
3.1. Linear Analysis
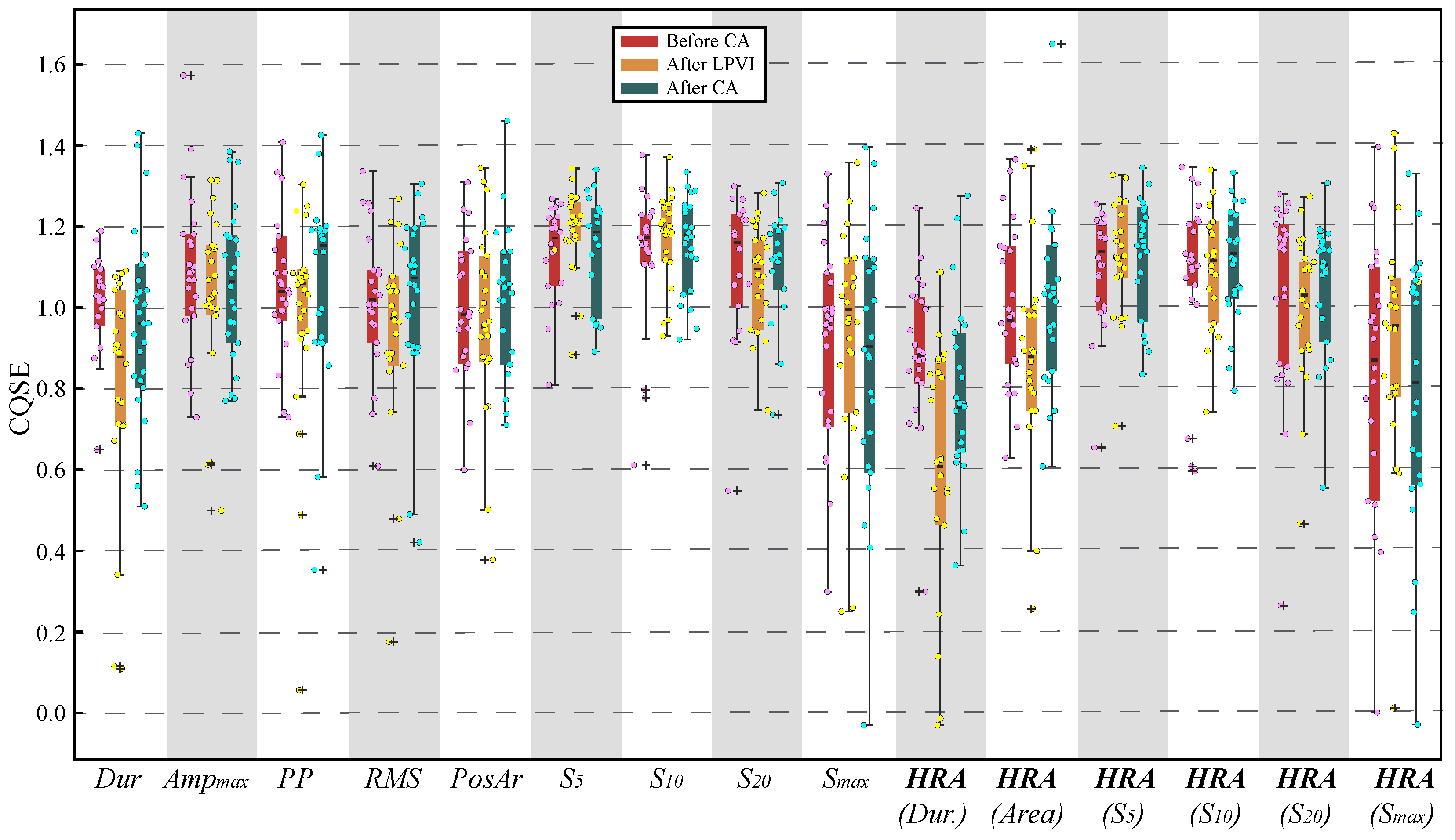
3.2. Nonlinear Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstro, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 374–498. [Google Scholar] [CrossRef]
- Haissaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D.; Haïssaguerre, M.; Jaïs, P. Catheter Ablation of Pulmonary Vein Foci for Atrial Fibrillation. Thorac. Cardiovasc. Surg. 1999, 47, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Oral, H.; Knight, B.; Tada, H. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. ACC Curr. J. Rev. 2002, 11, 83. [Google Scholar] [CrossRef]
- Cheng, W.H.; Lo, L.W.; Lin, Y.J.; Chang, S.L.; Hu, Y.F.; Hung, Y.; Chung, F.P.; Liao, J.N.; Tuan, T.C.; Chao, T.F.; et al. Ten-year ablation outcomes of patients with paroxysmal atrial fibrillation undergoing pulmonary vein isolation. Heart Rhythm 2019, 16, 1327–1333. [Google Scholar] [CrossRef]
- Lau, D.H.; Linz, D.; Schotten, U.; Mahajan, R.; Sanders, P.; Kalman, J.M. Pathophysiology of Paroxysmal and Persistent Atrial Fibrillation: Rotors, Foci and Fibrosis. Heart Lung Circ. 2017, 26, 887–893. [Google Scholar] [CrossRef]
- Thomas, L.; Abhayaratna, W.P. Left Atrial Reverse Remodeling: Mechanisms, Evaluation, and Clinical Significance. JACC Cardiovasc. Imaging 2017, 10, 65–77. [Google Scholar] [CrossRef]
- Knecht, S.; Pradella, M.; Reichlin, T.; Mühl, A.; Bossard, M.; Stieltjes, B.; Conen, D.; Bremerich, J.; Osswald, S.; Kühne, M.; et al. Left atrial anatomy, atrial fibrillation burden, and P-wave duration-relationships and predictors for single-procedure success after pulmonary vein isolation. EP Eur. 2018, 20, 271–278. [Google Scholar] [CrossRef]
- Maille, B.; Das, M.; Hussein, A.; Shaw, M.; Chaturvedi, V.; Williams, E.; Morgan, M.; Ronayne, C.; Snowdon, R.L.; Gupta, D. Reverse electrical and structural remodelling of the left atrium occurs early after pulmonary vein isolation for persistent atrial fibrillation. J. Interv. Card. Electrophysiol. 2020, 58, 9–19. [Google Scholar] [CrossRef]
- Wen, S.; Indrabhinduwat, M.; Brady, P.A.; Pislaru, C.; Miller, F.A.; Ammash, N.M.; Nkomo, V.T.; Padang, R.; Pislaru, S.V.; Lin, G. Post Procedural Peak Left Atrial Contraction Strain Predicts Recurrence of Arrhythmia after Catheter Ablation of Atrial Fibrillation. Cardiovasc. Ultrasound 2021, 19, 22. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.T.; Lee, H.L.; Wo, H.T.; Chang, P.C.; Wen, M.S.; Lin, F.C.; Yeh, S.J.; Chou, C.C. P wave duration ≥ 150 ms predicts poor left atrial function and ablation outcomes in non-paroxysmal atrial fibrillation. J. Electrocardiol. 2021, 69, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Vraka, A.; Bertomeu-González, V.; Fácila, L.; Moreno-Arribas, J.; Alcaraz, R.; Rieta, J.J. The Dissimilar Impact in Atrial Substrate Modificationof Left and Right Pulmonary Veins Isolation after Catheter Ablation of Paroxysmal Atrial Fibrillation. J. Pers. Med. 2022, 12, 462. [Google Scholar] [CrossRef] [PubMed]
- Santangeli, P.; Marchlinski, F.E. Techniques for the provocation, localization, and ablation of non–pulmonary vein triggers for atrial fibrillation. Heart Rhythm 2017, 14, 1087–1096. [Google Scholar] [CrossRef] [Green Version]
- Young, M.L.; Niu, J. Using coronary sinus ostium as the reference for the slow pathway ablation of atrioventricular nodal reentrant tachycardia in children. J. Arrhythmia 2020, 36, 712–719. [Google Scholar] [CrossRef]
- Antz, M.; Otomo, K.; Arruda, M.; Scherlag, B.J.; Pitha, J.; Tondo, C.; Lazzara, R.; Jackman, W.M. Electrical conduction between the right atrium and the left atrium via the musculature of the coronary sinus. Circulation 1998, 98, 1790–1795. [Google Scholar] [CrossRef] [Green Version]
- Tritto, M.; Zardini, M.; De Ponti, R.; Salerno-Uriarte, J.A. Iterative atrial tachycardia originating from the coronary sinus musculature. J. Cardiovasc. Electrophysiol. 2001, 12, 1187–1189. [Google Scholar] [CrossRef]
- Giudici, M.; Winston, S.; Kappler, J.; Shinn, T.; Singer, I.; Scheiner, A.; Berrier, H.; Herner, M.; Sample, R. Mapping the coronary sinus and great cardiac vein. PACE 2002, 25, 414–419. [Google Scholar] [CrossRef]
- Ahmed, N.; Perveen, S.; Mehmood, A.; Rani, G.F.; Molon, G. Coronary Sinus Ablation Is a Key Player Substrate in Recurrence of Persistent Atrial Fibrillation. Cardiology 2019, 143, 107–113. [Google Scholar] [CrossRef]
- Razeghian-Jahromi, I.; Natale, A.; Nikoo, M.H. Coronary sinus diverticulum: Importance, function, and treatment. PACE 2020, 43, 1582–1587. [Google Scholar] [CrossRef]
- Morita, H.; Zipes, D.P.; Morita, S.T.; Wu, J. The role of coronary sinus musculature in the induction of atrial fibrillation. Heart Rhythm 2012, 9, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Oral, H.; Ozaydin, M.; Chugh, A.; Scharf, C.; Tada, H.; Hall, B.; Cheung, P.; Pelosi, F.; Knight, B.P.; Morady, F. Role of the coronary sinus in maintenance of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2003, 14, 1329–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haïssaguerre, M.; Hocini, M.; Takahashi, Y.; O’Neill, M.D.; Pernat, A.; Sanders, P.; Jonsson, A.; Rotter, M.; Sacher, F.; Rostock, T.; et al. Impact of catheter ablation of the coronary sinus on paroxysmal or persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2007, 18, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Ulfarsson, M.; Tada, H.; Chugh, A.; Good, E.; Kuhne, M.; Crawford, T.; Sarrazin, J.F.; Chalfoun, N.; Wells, D.; et al. Complex electrograms within the coronary sinus: Time- and frequency-domain characteristics, effects of antral pulmonary vein isolation, and relationship to clinical outcome in patients with paroxysmal and persistent atrial fibrillation. J. Cardiovasc. Electrophysiol. 2008, 19, 1017–1023. [Google Scholar] [CrossRef] [Green Version]
- Marco, L.Y.D.; Raine, D.; Bourke, J.P.; Langley, P. Characteristics of atrial fibrillation cycle length predict restoration of sinus rhythm by catheter ablation. Heart Rhythm 2013, 10, 1303–1310. [Google Scholar] [CrossRef]
- Yin, X.; Zhao, Z.; Gao, L.; Chang, D.; Xiao, X.; Zhang, R.; Chen, Q.; Cheng, J.; Yang, Y.; Xi, Y.; et al. Frequency Gradient Within Coronary Sinus Predicts the Long-Term Outcome of Persistent Atrial Fibrillation Catheter Ablation. J. Am. Heart Assoc. 2017, 6, e004869. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Chugh, A.; Good, E.; Crawford, T.; Myles, J.; Veerareddy, S.; Billakanty, S.; Wong, W.S.; Ebinger, M.; Pelosi, F.; et al. A critical decrease in dominant frequency and clinical outcome after catheter ablation of persistent atrial fibrillation. Heart Rhythm 2010, 7, 295–302. [Google Scholar] [CrossRef]
- Teh, A.W.; Kalman, J.M.; Kistler, P.M.; Lee, G.; Sutherland, F.; Morton, J.B.; Vohra, J.K.; Sparks, P.B. Prevalence of fractionated electrograms in the coronary sinus: Comparison between patients with persistent or paroxysmal atrial fibrillation and a control population. Heart Rhythm 2010, 7, 1200–1204. [Google Scholar] [CrossRef]
- Kanemaru, Y.; Arima, Y.; Kaikita, K.; Kiyama, T.; Kaneko, S.; Ito, M.; Yamabe, H.; Motozato, K.; Yamanaga, K.; Fujisue, K.; et al. Elongation of the high right atrium to coronary sinus conduction time predicts the recurrence of atrial fibrillation after radiofrequency catheter ablation. Int. J. Cardiol. 2020, 300, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Boles, U.; Gul, E.E.; Enriquez, A.; Starr, N.; Haseeb, S.; Abdollah, H.; Simpson, C.; Baranchuk, A.; Redfearn, D.; Michael, K.; et al. Coronary Sinus Electrograms May Predict New-onset Atrial Fibrillation After Typical Atrial Flutter Radiofrequency Ablation (CSE-AF). J. Atr. Fibrillation 2018, 11, 1809. [Google Scholar] [CrossRef]
- McGuinness, S.; McKee, A.; Sidebotham, D. Chapter 8—Monitoring. In Cardiothoracic Critical Care; Butterworth-Heinemann: Oxford, UK, 2007; pp. 120–137. [Google Scholar] [CrossRef]
- Stafford, P.J.; Vincent, R. Spectrotemporal and spectral turbulence analysis of the signal-averaged P wave in paroxysmal atrial fibrillation. J. Electrocardiol. 1997, 30, 79–86. [Google Scholar] [CrossRef]
- Van Beeumen, K.; Houben, R.; Tavernier, R.; Ketels, S.; Duytschaever, M. Changes in P-wave area and P-wave duration after circumferential pulmonary vein isolation. EP Eur. 2010, 12, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Vassilikos, V.; Dakos, G.; Chatzizisis, Y.S.; Chouvarda, I.; Karvounis, C.; Maynard, C.; Maglaveras, N.; Paraskevaidis, S.; Stavropoulos, G.; Styliadis, C.I.; et al. Novel non-invasive P wave analysis for the prediction of paroxysmal atrial fibrillation recurrences in patients without structural heart disease: A prospective pilot study. Int. J. Cardiol. 2011, 153, 165–172. [Google Scholar] [CrossRef]
- Salah, A.; Zhou, S.; Liu, Q.; Yan, H. P wave indices to predict atrial fibrillation recurrences post pulmonary vein isolation. Arq. Bras. Cardiol. 2013, 101, 519–527. [Google Scholar] [CrossRef]
- Maan, A.; Mansour, M.; Ruskin, J.N.; Heist, E.K. Impact of catheter ablation on P-wave parameters on 12-lead electrocardiogram in patients with atrial fibrillation. J. Electrocardiol. 2014, 47, 725–733. [Google Scholar] [CrossRef]
- Alcaraz, R.; Martínez, A.; Rieta, J.J. The P Wave Time-Frequency Variability Reflects Atrial Conduction Defects before Paroxysmal Atrial Fibrillation. Ann. Noninvasive Electrocardiol. 2015, 20, 433–445. [Google Scholar] [CrossRef] [PubMed]
- Kizilirmak, F.; Demir, G.G.; Gokdeniz, T.; Gunes, H.M.; Cakal, B.; Guler, E.; Karaca, I.O.; Omaygenç, M.O.; Yılmaz, F.; Olgun, F.E.; et al. Changes in Electrocardiographic P Wave Parameters after Cryoballoon Ablation and Their Association with Atrial Fibrillation Recurrence. Ann. Noninvasive Electrocardiol. 2016, 21, 580–587. [Google Scholar] [CrossRef]
- Ortigosa, N.; Ayala, G.; Cano, Ó. Variation of P-wave indices in paroxysmal atrial fibrillation patients before and after catheter ablation. Biomed. Signal Process. Control 2021, 66, 102500. [Google Scholar] [CrossRef]
- Simpson, R.J.; Foster, J.R.; Gettes, L.S. Atrial excitability and conduction in patients with interatrial conduction defects. Am. J. Cardiol. 1982, 50, 1331–1337. [Google Scholar] [CrossRef]
- Chen, Q.; Mohanty, S.; Trivedi, C.; Gianni, C.; Della Rocca, D.G.; Canpolat, U.; Burkhardt, J.D.; Sanchez, J.E.; Hranitzky, P.; Gallinghouse, G.J.; et al. Association between prolonged P wave duration and left atrial scarring in patients with paroxysmal atrial fibrillation. J. Cardiovasc. Electrophysiol. 2019, 30, 1811–1818. [Google Scholar] [CrossRef]
- Pranata, R.; Yonas, E.; Vania, R. Prolonged P-wave duration in sinus rhythm pre-ablation is associated with atrial fibrillation recurrence after pulmonary vein isolation-A systematic review and meta-analysis. Ann. Noninvasive Electrocardiol. 2019, 24, e12653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vraka, A.; Bertomeu-González, V.; Hornero, F.; Quesada, A.; Alcaraz, R.; Rieta, J.J. Splitting the P-Wave: Improved Evaluation of Left Atrial Substrate Modification after Pulmonary Vein Isolation of Paroxysmal Atrial Fibrillation. Sensors 2022, 22, 290. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Perkiömäki, J.; Ukkola, O.; Kiviniemi, A.; Tulppo, M.; Ylitalo, A.; Kesäniemi, Y.A.; Huikuri, H. Heart rate variability findings as a predictor of atrial fibrillation in middle-aged population. J. Cardiovasc. Electrophysiol. 2014, 25, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Habibi, M.; Chahal, H.; Greenland, P.; Guallar, E.; Lima, J.A.C.; Soliman, E.Z.; Alonso, A.; Heckbert, S.R.; Nazarian, S. Resting Heart Rate, Short-Term Heart Rate Variability and Incident Atrial Fibrillation (from the Multi-Ethnic Study of Atherosclerosis (MESA)). Am. J. Cardiol. 2019, 124, 1684–1689. [Google Scholar] [CrossRef]
- Huikuri, H.V.; Mäkikallio, T.H.; Perkiömäki, J. Measurement of heart rate variability by methods based on nonlinear dynamics. J. Electrocardiol. 2003, 36 (Suppl. 1), 95–99. [Google Scholar] [CrossRef]
- Hsieh, M.H.; Chiou, C.W.; Wen, Z.C.; Wu, C.H.; Tai, C.T.; Tsai, C.F.; Ding, Y.A.; Chang, M.S.; Chen, S.A. Alterations of heart rate variability after radiofrequency catheter ablation of focal atrial fibrillation originating from pulmonary veins. Circulation 1999, 100, 2237–2243. [Google Scholar] [CrossRef]
- Zhu, Z.; Wang, W.; Cheng, Y.; Wang, X.; Sun, J. The predictive value of heart rate variability indices tested in early period after radiofrequency catheter ablation for the recurrence of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2020, 31, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Călburean, P.A.; Osorio, T.G.; Sorgente, A.; Almorad, A.; Pannone, L.; Monaco, C.; Miraglia, V.; Al Housari, M.; Mojica, J.; Bala, G.; et al. High vagal tone predicts pulmonary vein reconnection after cryoballoon ablation for paroxysmal atrial fibrillation. PACE 2021, 44, 2075–2083. [Google Scholar] [CrossRef]
- Sörnmo, L.; Laguna, P. Electrocardiogram (ECG) Signal Processing. In Wiley Encyclopedia of Biomedical Engineering; John Wiley and Sons: Hoboken, NJ, USA, 2006; Volume 2, pp. 1298–1313. [Google Scholar] [CrossRef]
- García, M.; Martínez-Iniesta, M.; Ródenas, J.; Rieta, J.J.; Alcaraz, R. A novel wavelet-based filtering strategy to remove powerline interference from electrocardiograms with atrial fibrillation. Physiol. Meas. 2018, 39, 115006. [Google Scholar] [CrossRef]
- Martínez, A.; Alcaraz, R.; Rieta, J.J. Detection and removal of ventricular ectopic beats in atrial fibrillation recordings via principal component analysis. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4693–4696. [Google Scholar] [CrossRef]
- Choi, A.; Shin, H. Quantitative Analysis of the Effect of an Ectopic Beat on the Heart Rate Variability in the Resting Condition. Front. Physiol. 2018, 9, 922. [Google Scholar] [CrossRef]
- Martinez, A.; Alcaraz, R.; Rieta, J.J. A new method for automatic delineation of ECG fiducial points based on the Phasor Transform. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 4586–4589. [Google Scholar] [CrossRef]
- González, F.; Alcaraz, R.; Rieta, J.J. Electrocardiographic P-wave delineation based on adaptive slope Gaussian detection. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Alcaraz, R.; Rieta, J.J. Adaptive singular value cancelation of ventricular activity in single-lead atrial fibrillation electrocardiograms. Physiol. Meas. 2008, 29, 1351–1369. [Google Scholar] [CrossRef]
- Martínez-Iniesta, M.; Ródenas, J.; Rieta, J.J.; Alcaraz, R. The stationary wavelet transform as an efficient reductor of powerline interference for atrial bipolar electrograms in cardiac electrophysiology. Physiol. Meas. 2019, 40, 075003. [Google Scholar] [CrossRef]
- Osorio, D.; Alcaraz, R.; Rieta, J.J. A fractionation-based local activation wave detector for atrial electrograms of atrial fibrillation. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar] [CrossRef]
- Vraka, A.; Bertomeu-González, V.; Osca, J.; Ravelli, F.; Alcaraz, R.; Rieta, J.J. Study on How Catheter Ablation Affects Atrial Structures in Patients with Paroxysmal Atrial Fibrillation: The Case of the Coronary Sinus. In Proceedings of the 2020 International Conference on e-Health and Bioengineering (EHB), Iasi, Romania, 29–30 October 2020; pp. 1–4. [Google Scholar] [CrossRef]
- Toman, O.; Hnatkova, K.; Smetana, P.; Huster, K.M.; Šišáková, M.; Barthel, P.; Novotný, T.; Schmidt, G.; Malik, M. Physiologic heart rate dependency of the PQ interval and its sex differences. Sci. Rep. 2020, 10, 2551. [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples); Oxford University Press: Oxford, UK, 1965; Volume 52, pp. 591–611. [Google Scholar]
- Yan, X.; Su, X.G. Simple Linear Regression. In Linear Regression Analysis: Theory and Computing; World Scientific: Singapore, 2009; pp. 9–39. [Google Scholar] [CrossRef]
- Pincus, S.M. Irregularity and asynchrony in biologic network signals. In Numerical Computer Methods, Part C; Academic Press: Cambridge, MA, USA, 2000; Volume 321, pp. 149–182. [Google Scholar] [CrossRef]
- Alcaraz, R.; Rieta, J.J. Nonlinear synchronization assessment between atrial and ventricular activations series from the surface ECG in atrial fibrillation. Biomed. Signal Process. Control 2013, 8, 1000–1007. [Google Scholar] [CrossRef]
- Lake, D.E.; Moorman, J.R. Accurate estimation of entropy in very short physiological time series: The problem of atrial fibrillation detection in implanted ventricular devices. Am. J. Physiol. 2011, 300, H319–H325. [Google Scholar] [CrossRef]
- Vraka, A.; Hornero, F.; Bertomeu-González, V.; Osca, J.; Alcaraz, R.; Rieta, J.J. Short-Time Estimation of Fractionation in Atrial Fibrillation with Coarse-Grained Correlation Dimension for Mapping the Atrial Substrate. Entropy 2020, 22, 232. [Google Scholar] [CrossRef] [Green Version]
- de Groot, N.; Shah, D.; Boyle, P.M.; Anter, E.; Clifford, G.D.; Deisenhofer, I.; Deneke, T.; van Dessel, P.; Doessel, O.; Dilaveris, P.; et al. Critical appraisal of technologies to assess electrical activity during atrial fibrillation: A position paper from the European Heart Rhythm Association and European Society of Cardiology Working Group on eCardiology in collaboration with the Heart Rhythm Society, Asia Pacific Heart Rhythm Society, Latin American Heart Rhythm Society and Computing in Cardiology. EP Eur. 2021, 24, 313–330. [Google Scholar] [CrossRef]
- Misek, J.; Belyaev, I.; Jakusova, V.; Tonhajzerova, I.; Barabas, J.; Jakus, J. Heart rate variability affected by radiofrequency electromagnetic field in adolescent students. Bioelectromagnetics 2018, 39, 277–288. [Google Scholar] [CrossRef]
- Misek, J.; Veternik, M.; Tonhajzerova, I.; Jakusova, V.; Janousek, L.; Jakus, J. Radiofrequency Electromagnetic Field Affects Heart Rate Variability in Rabbits. Physiol. Res. 2020, 69, 633–643. [Google Scholar] [CrossRef]
- Chen, P.S.; Chen, L.S.; Fishbein, M.C.; Lin, S.F.; Nattel, S. Role of the autonomic nervous system in atrial fibrillation: Pathophysiology and therapy. Circ. Res. 2014, 114, 1500–1515. [Google Scholar] [CrossRef] [Green Version]
- Martínez, A.; Alcaraz, R.; Rieta, J.J. Study on the P-wave feature time course as early predictors of paroxysmal atrial fibrillation. Physiol. Meas. 2012, 33, 1959–1974. [Google Scholar] [CrossRef]
- Rodrigo, M.; Climent, A.M.; Hernández-Romero, I.; Liberos, A.; Baykaner, T.; Rogers, A.J.; Alhusseini, M.; Wang, P.J.; Fernández-Avilés, F.; Guillem, M.S.; et al. Noninvasive Assessment of Complexity of Atrial Fibrillation: Correlation With Contact Mapping and Impact of Ablation. Circ. Arrhythmia Electrophysiol. 2020, 13, e007700. [Google Scholar] [CrossRef]
- Liu, Z.; Hayano, M.; Hirata, T.; Tsukahara, K.; Quin, Y.; Nakao, K.; Nonaka, M.; Ishimatsu, T.; Ueyama, C.; Yano, K. Abnormalities of electrocardiographic P wave morphology and their relation to electrophysiological parameters of the atrium in patients with sick sinus syndrome. PACE 1998, 21, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Yahyazadeh, S.; Firoozabadi, S.; Haghjoo, M.; Parvaneh, S. Quantitative relation between chaotic features of surface electrocardiogram and Intracardiac Electrogram. In Proceedings of the 2010 Computing in Cardiology, Belfast, UK, 26–29 September 2010; pp. 593–596. [Google Scholar]
- Alcaraz, R.; Hornero, F.; Rieta, J.J. Validation of surface atrial fibrillation organization indicators through invasive recordings. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5519–5522. [Google Scholar] [CrossRef]
- Kharbanda, R.; Knops, P.; van der Does, L.; Kik, C.; Taverne, Y.; Roos-Serote, M.; Heida, A.; Oei, F.; Bogers, A.; de Groot, N. Simultaneous Endo-Epicardial Mapping of the Human Right Atrium: Unraveling Atrial Excitation. J. Am. Heart Assoc. 2020, 9, e017069. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Corrpre | CorrLPVI | Corrpost | ||||
|---|---|---|---|---|---|---|
| Feature | ρ [%] | p Value | ρ [%] | p Value | ρ [%] | p Value |
| Duration | ||||||
| PP | ||||||
| RMS | ||||||
| PosAr | ||||||
| Pre-CA | LPVI | Post-CA | ||||
|---|---|---|---|---|---|---|
| Feature | R2-adj [%] | p Value | R2-adj [%] | p Value | R2-adj [%] | p Value |
| Duration | ||||||
| PP | ||||||
| RMS | ||||||
| PosAr | ||||||
| CVpre CA−LPVI | CVpre−post CA | CVLPVI−post | ||||
|---|---|---|---|---|---|---|
| Feature | ρ [%] | p Value | ρ [%] | p Value | ρ [%] | p Value |
| Duration | ||||||
| PP | ||||||
| RMS | ||||||
| PosAr | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vraka, A.; Moreno-Arribas, J.; Gracia-Baena, J.M.; Hornero, F.; Alcaraz, R.; Rieta, J.J. The Relevance of Heart Rate Fluctuation When Evaluating Atrial Substrate Electrical Features in Catheter Ablation of Paroxysmal Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2022, 9, 176. https://doi.org/10.3390/jcdd9060176
Vraka A, Moreno-Arribas J, Gracia-Baena JM, Hornero F, Alcaraz R, Rieta JJ. The Relevance of Heart Rate Fluctuation When Evaluating Atrial Substrate Electrical Features in Catheter Ablation of Paroxysmal Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2022; 9(6):176. https://doi.org/10.3390/jcdd9060176
Chicago/Turabian StyleVraka, Aikaterini, José Moreno-Arribas, Juan M. Gracia-Baena, Fernando Hornero, Raúl Alcaraz, and José J. Rieta. 2022. "The Relevance of Heart Rate Fluctuation When Evaluating Atrial Substrate Electrical Features in Catheter Ablation of Paroxysmal Atrial Fibrillation" Journal of Cardiovascular Development and Disease 9, no. 6: 176. https://doi.org/10.3390/jcdd9060176
APA StyleVraka, A., Moreno-Arribas, J., Gracia-Baena, J. M., Hornero, F., Alcaraz, R., & Rieta, J. J. (2022). The Relevance of Heart Rate Fluctuation When Evaluating Atrial Substrate Electrical Features in Catheter Ablation of Paroxysmal Atrial Fibrillation. Journal of Cardiovascular Development and Disease, 9(6), 176. https://doi.org/10.3390/jcdd9060176