
Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial

 ,
,  , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
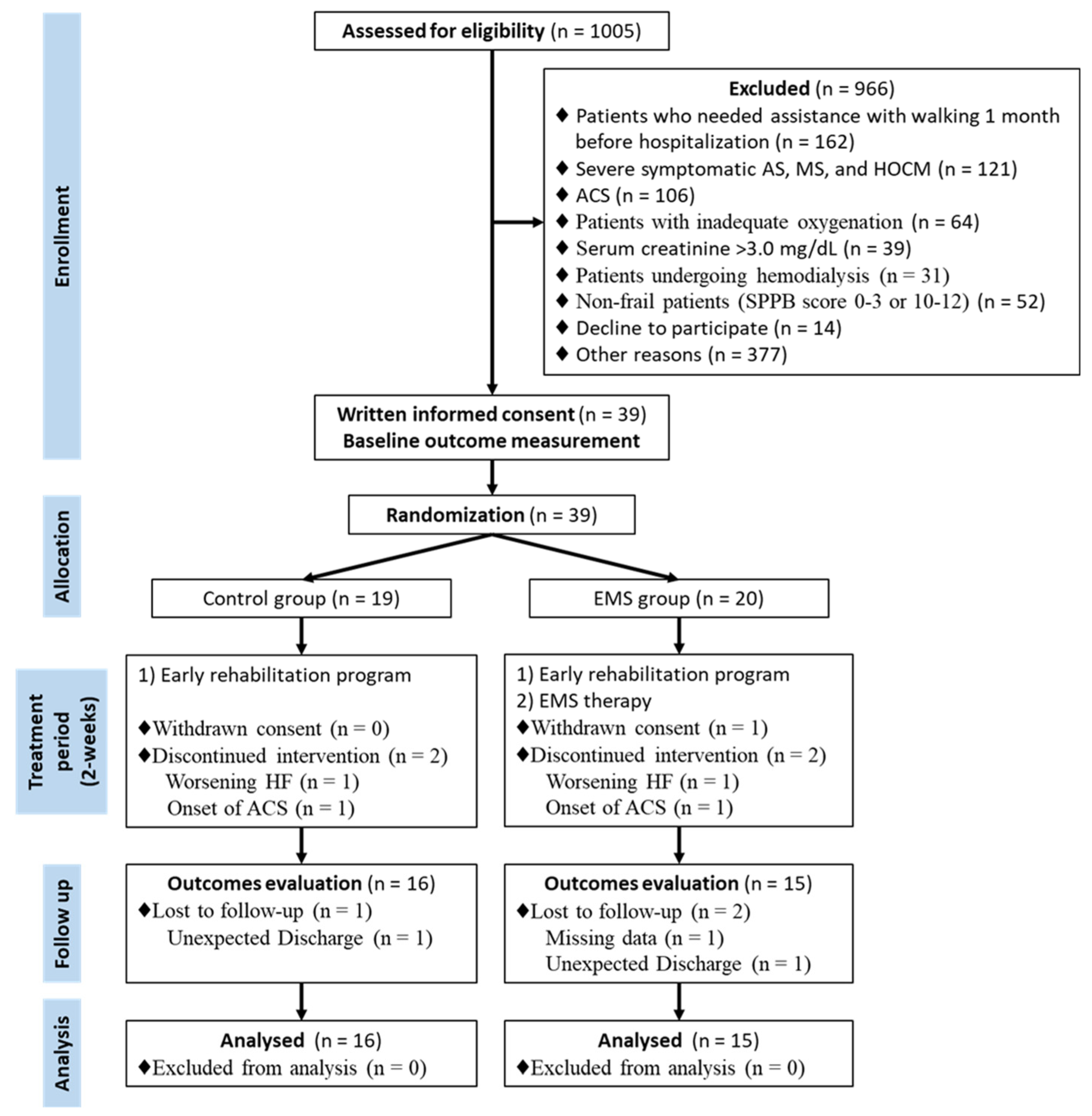
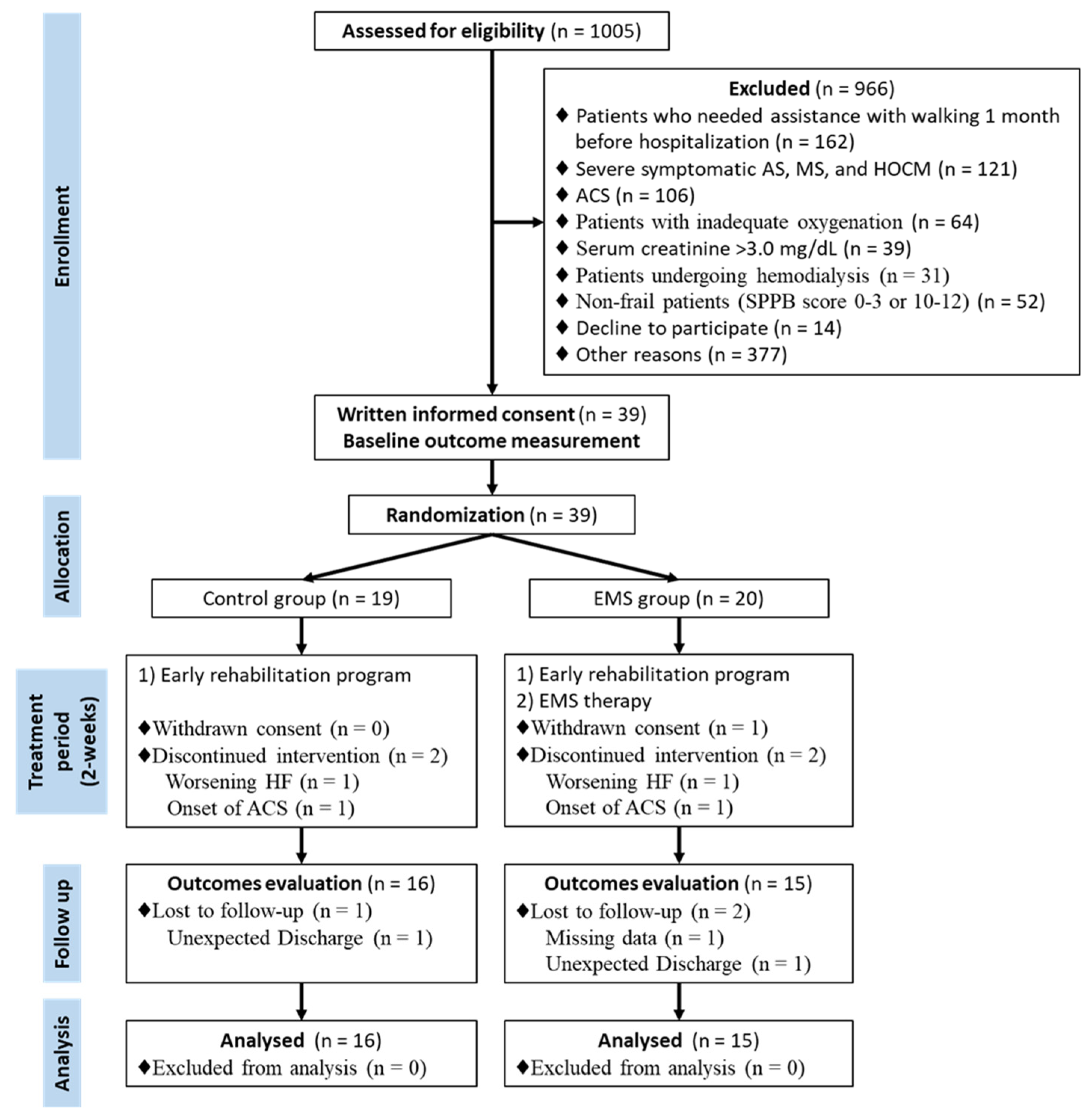
2.2. Patients and Randomization
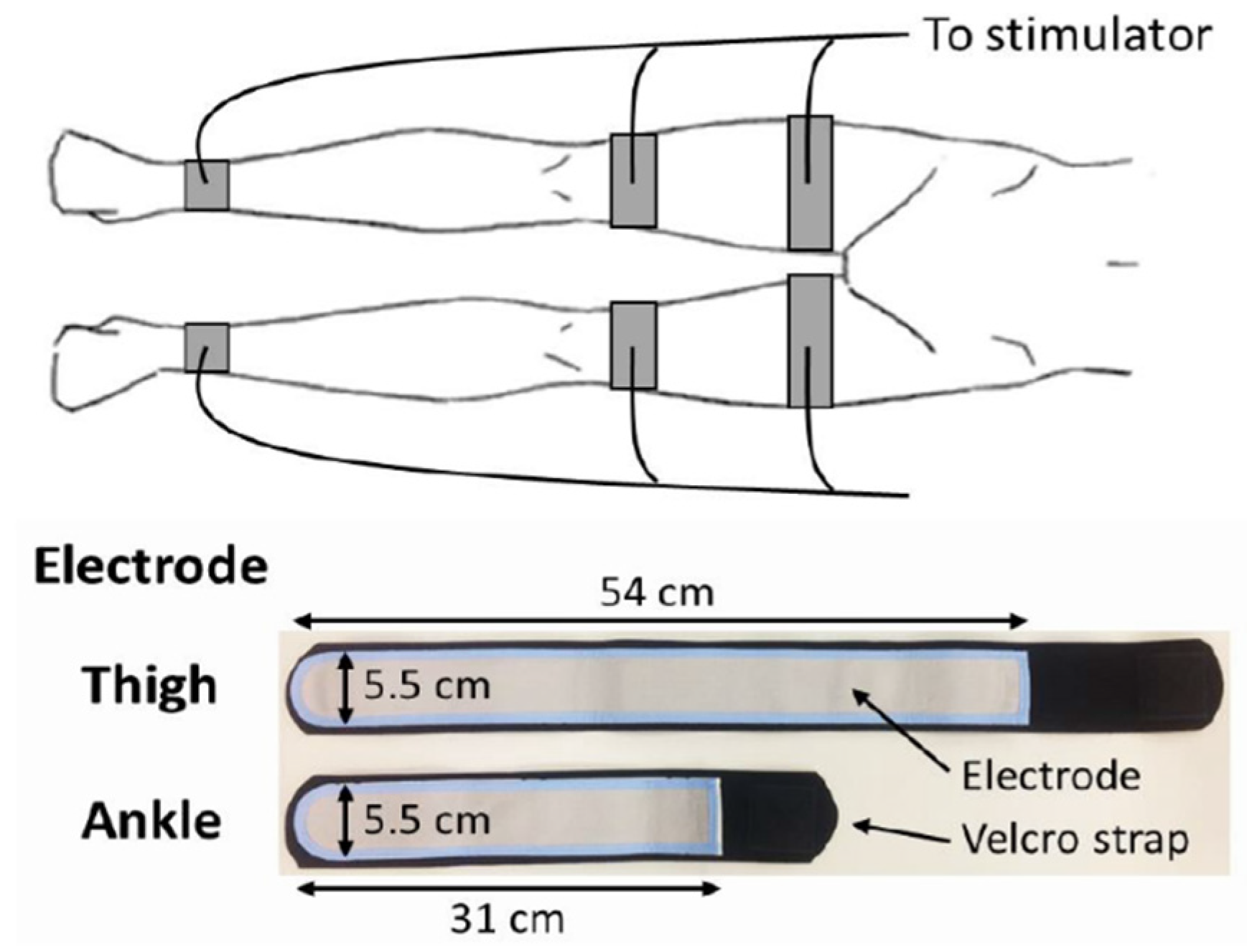
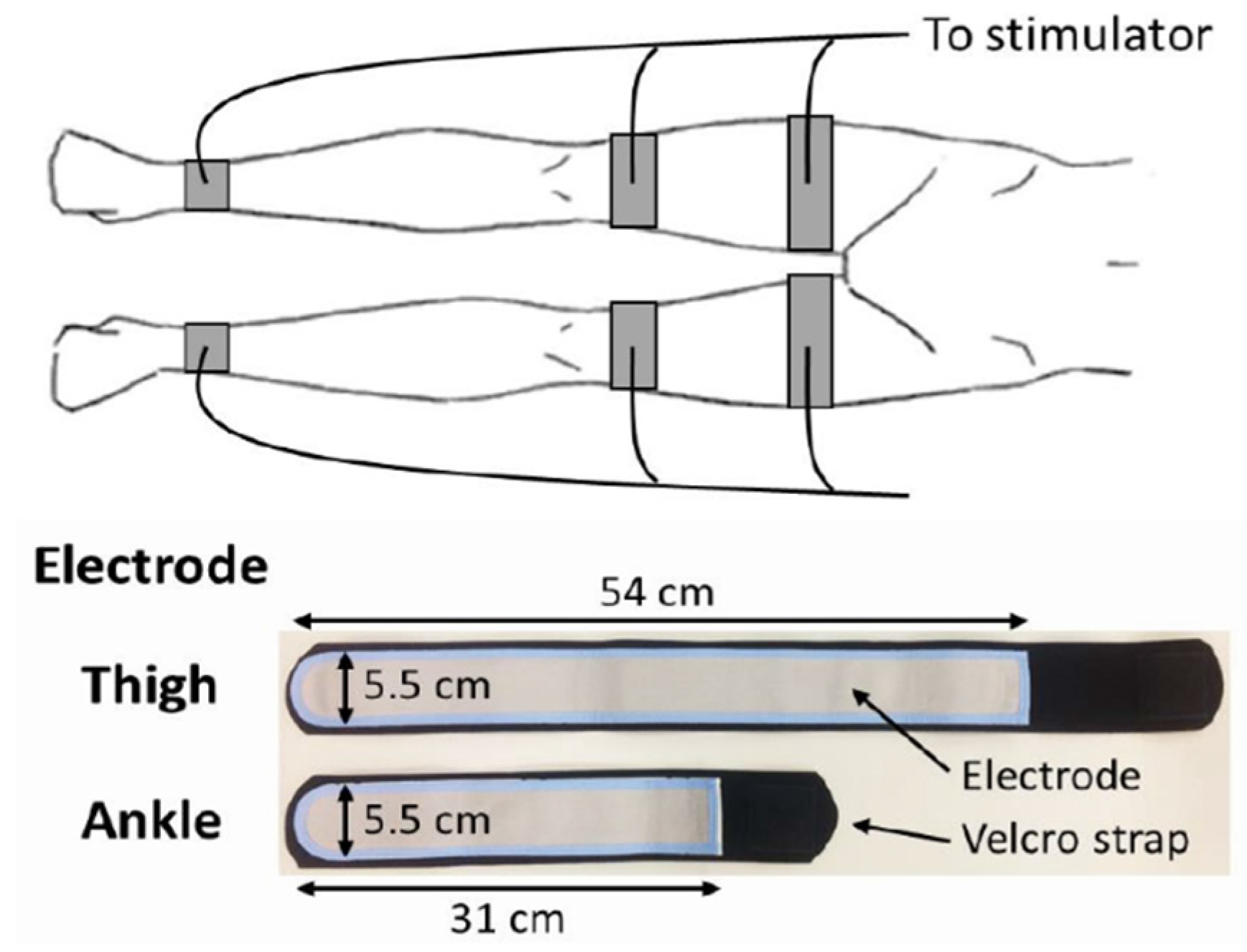
2.3. EMS Protocol
2.4. Early Rehabilitation Program
2.5. Outcomes
2.6. Sample Size Calculation
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afilalo, J.; Alexander, K.P.; Mack, M.J.; Maurer, M.S.; Green, P.; Allen, L.A.; Popma, J.J.; Ferrucci, L.; Forman, D.E. Frailty assessment in the cardiovascular care of older adults. J. Am. Coll. Cardiol. 2014, 63, 747–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, A.; Kitzman, D.; Reeves, G. Frailty Is Intertwined With Heart Failure: Mechanisms, Prevalence, Prognosis, Assessment, and Management. JACC Heart Fail. 2019, 7, 1001–1011. [Google Scholar] [CrossRef]
- Bueno, H.; Ross, J.S.; Wang, Y.; Chen, J.; Vidán, M.T.; Normand, S.L.; Curtis, J.P.; Drye, E.E.; Lichtman, J.H.; Keenan, P.S.; et al. Trends in length of stay and short-term outcomes among Medicare patients hospitalized for heart failure, 1993–2006. JAMA 2010, 303, 2141–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, S.; Yamashita, M.; Saito, H.; Kamiya, K.; Maeda, D.; Konishi, M.; Matsue, Y. Multidomain Frailty in Heart Failure: Current Status and Future Perspectives. Curr. Heart. Fail. Rep. 2021, 18, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Neto, M.; Durães, A.R.; Conceição, L.S.R.; Roever, L.; Silva, C.M.; Alves, I.G.N.; Ellingsen, Ø.; Carvalho, V.O. Effect of combined aerobic and resistance training on peak oxygen consumption, muscle strength and health-related quality of life in patients with heart failure with reduced left ventricular ejection fraction: A systematic review and meta-analysis. Int. J. Cardiol. 2019, 293, 165–175. [Google Scholar] [CrossRef]
- Taylor, R.S.; Long, L.; Mordi, I.R.; Madsen, M.T.; Davies, E.J.; Dalal, H.; Rees, K.; Singh, S.J.; Gluud, C.; Zwisler, A.D. Exercise-Based Rehabilitation for Heart Failure: Cochrane Systematic Review, Meta-Analysis, and Trial Sequential Analysis. JACC Heart Fail. 2019, 7, 691–705. [Google Scholar] [CrossRef] [PubMed]
- Parissis, J.; Farmakis, D.; Karavidas, A.; Arapi, S.; Filippatos, G.; Lekakis, J. Functional electrical stimulation of lower limb muscles as an alternative mode of exercise training in chronic heart failure: Practical considerations and proposed algorithm. Eur. J. Heart Fail. 2015, 17, 1228–1230. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Oliveira, F.A.; Reis, H.F.; de Sousa Rodrigues, E., Jr.; Bittencourt, H.S.; Oliveira Carvalho, V. Effects of Neuromuscular Electrical Stimulation on Physiologic and Functional Measurements in Patients With Heart Failure: A systematic review with meta-analysis. J. Cardiopulm. Rehabil. Prev. 2016, 36, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Groehs, R.V.; Antunes-Correa, L.M.; Nobre, T.S.; Alves, M.J.; Rondon, M.U.; Barreto, A.C.; Negrão, C.E. Muscle electrical stimulation improves neurovascular control and exercise tolerance in hospitalised advanced heart failure patients. Eur. J. Prev. Cardiol. 2016, 23, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Forestieri, P.; Bolzan, D.W.; Santos, V.B.; Moreira, R.S.L.; de Almeida, D.R.; Trimer, R.; de Souza Brito, F.; Borghi-Silva, A.; de Camargo Carvalho, A.C.; Arena, R.; et al. Neuromuscular electrical stimulation improves exercise tolerance in patients with advanced heart failure on continuous intravenous inotropic support use-randomized controlled trial. Clin. Rehabil. 2018, 32, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Kamiya, K.; Matsue, Y.; Yonezawa, R.; Saito, H.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Yamashita, M.; Wakaume, K.; et al. Effects of electrical muscle stimulation on physical function in frail older patients with acute heart failure: A randomized controlled trial. Eur. J. Prev. Cardiol. 2022; >in press. [Google Scholar] [CrossRef] [PubMed]
- Kitzman, D.W.; Whellan, D.J.; Duncan, P.; Pastva, A.M.; Mentz, R.J.; Reeves, G.R.; Nelson, M.B.; Chen, H.; Upadhya, B.; Reed, S.D.; et al. Physical Rehabilitation for Older Patients Hospitalized for Heart Failure. N. Engl. J. Med. 2021, 385, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Sato, Y.; Takahashi, T.; Tsuchihashi-Makaya, M.; Kotooka, N.; Ikegame, T.; Takura, T.; Yamamoto, T.; Nagayama, M.; Goto, Y.; et al. Multidisciplinary Cardiac Rehabilitation and Long-Term Prognosis in Patients With Heart Failure. Circ. Heart. Fail. 2020, 13, e006798. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Yamamoto, T.; Tsuchihashi-Makaya, M.; Ikegame, T.; Takahashi, T.; Sato, Y.; Kotooka, N.; Saito, Y.; Tsutsui, H.; Miyata, H.; et al. Nationwide Survey of Multidisciplinary Care and Cardiac Rehabilitation for Patients With Heart Failure in Japan—An Analysis of the AMED-CHF Study. Circ. J. 2019, 83, 1546–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, A.; Keshvani, N.; Zhong, L.; Mentz, R.J.; Piña, I.L.; DeVore, A.D.; Yancy, C.; Kitzman, D.W.; Fonarow, G.C. Temporal Trends and Factors Associated With Cardiac Rehabilitation Participation Among Medicare Beneficiaries With Heart Failure. JACC Heart Fail. 2021, 9, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Reeves, G.R.; Whellan, D.J.; Patel, M.J.; O’Connor, C.M.; Duncan, P.; Eggebeen, J.D.; Morgan, T.M.; Hewston, L.A.; Pastva, A.M.; Kitzman, D.W. Comparison of Frequency of Frailty and Severely Impaired Physical Function in Patients ≥ 60 Years Hospitalized With Acute Decompensated Heart Failure Versus Chronic Stable Heart Failure With Reduced and Preserved Left Ventricular Ejection Fraction. Am. J. Cardiol. 2016, 117, 1953–1958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saitoh, M.; Takahashi, Y.; Okamura, D.; Akiho, M.; Suzuki, H.; Noguchi, N.; Yamaguchi, Y.; Hori, K.; Adachi, Y.; Takahashi, T. Prognostic impact of hospital-acquired disability in elderly patients with heart failure. ESC Heart Fail. 2021, 8, 1767–1774. [Google Scholar] [CrossRef]
- Kaneko, H.; Itoh, H.; Kamiya, K.; Morita, K.; Sugimoto, T.; Konishi, M.; Kiriyama, H.; Kamon, T.; Fujiu, K.; Michihata, N.; et al. Acute-phase initiation of cardiac rehabilitation and clinical outcomes in hospitalized patients for acute heart failure. Int. J. Cardiol. 2021, 340, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Kamiya, K.; Matsue, Y.; Yonezawa, R.; Saito, H.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Wakaume, K.; Endo, Y.; et al. Effects of Acute Phase Intensive Electrical Muscle Stimulation in Frail Elderly Patients With Acute Heart Failure (ACTIVE-EMS): Rationale and protocol for a multicenter randomized controlled trial. Clin. Cardiol. 2017, 40, 1189–1196. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P. Methods and processes of the CONSORT Group: Example of an extension for trials assessing nonpharmacologic treatments. Ann. Intern. Med. 2008, 148, W60–W66. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. A. Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Numata, H.; Nakase, J.; Inaki, A.; Mochizuki, T.; Oshima, T.; Takata, Y.; Kinuya, S.; Tsuchiya, H. Effects of the belt electrode skeletal muscle electrical stimulation system on lower extremity skeletal muscle activity: Evaluation using positron emission tomography. J. Orthop. Sci. 2016, 21, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, T.; Kamada, H.; Tamaki, A.; Moritani, T. Low-intensity electrical muscle stimulation induces significant increases in muscle strength and cardiorespiratory fitness. Eur. J. Sport. Sci. 2016, 16, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kihata, A.; Naraba, H.; Kanda, N.; Takahashi, Y.; Sonoo, T.; Hashimoto, H.; Morimura, N. Efficacy of belt electrode skeletal muscle electrical stimulation on reducing the rate of muscle volume loss in critically ill patients: A randomized controlled trial. J. Rehabil. Med. 2019, 51, 705–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamiya, K.; Mezzani, A.; Hotta, K.; Shimizu, R.; Kamekawa, D.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; Masuda, T. Quadriceps isometric strength as a predictor of exercise capacity in coronary artery disease patients. Eur. J. Prev. Cardiol. 2014, 21, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Maekawa, E.; Reed, J.L.; Noda, C.; et al. Quadriceps Strength and Mortality in Older Patients With Heart Failure. Can. J. Cardiol. 2021, 37, 476–483. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Man, W.D.; Gao, W.; Higginson, I.J.; Wilcock, A.; Maddocks, M. Neuromuscular electrical stimulation for muscle weakness in adults with advanced disease. Cochrane Database Syst. Rev. 2016, 10, Cd009419. [Google Scholar] [CrossRef] [Green Version]
- Karavidas, A.; Parissis, J.T.; Matzaraki, V.; Arapi, S.; Varounis, C.; Ikonomidis, I.; Grillias, P.; Paraskevaidis, I.; Pirgakis, V.; Filippatos, G.; et al. Functional electrical stimulation is more effective in severe symptomatic heart failure patients and improves their adherence to rehabilitation programs. J. Card. Fail. 2010, 16, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Landers, K.A.; Hunter, G.R.; Wetzstein, C.J.; Bamman, M.M.; Weinsier, R.L. The interrelationship among muscle mass, strength, and the ability to perform physical tasks of daily living in younger and older women. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, B443–B448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbat-Artigas, S.; Rolland, Y.; Cesari, M.; Abellan van Kan, G.; Vellas, B.; Aubertin-Leheudre, M. Clinical relevance of different muscle strength indexes and functional impairment in women aged 75 years and older. J. Gerontol. A. Biol. Sci. Med. Sci. 2013, 68, 811–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Working Group on Functional Outcome Measures for Clinical Trials. Functional outcomes for clinical trials in frail older persons: Time to be moving. J. Gerontol. A. Biol. Sci. Med. Sci. 2008, 63, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosy, A.P.; Cerbin, L.P.; Armstrong, P.W.; Butler, J.; Coles, A.; DeVore, A.D.; Dunlap, M.E.; Ezekowitz, J.A.; Felker, G.M.; Fudim, M.; et al. Body Weight Change During and After Hospitalization for Acute Heart Failure: Patient Characteristics, Markers of Congestion, and Outcomes: Findings from the ASCEND-HF Trial. JACC Heart Fail. 2017, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | EMS Group | ||
|---|---|---|---|
| (n = 16) | (n = 15) | ||
| Age, years | 83.3 ± 5.5 | 82.5 ± 4.0 | |
| ≥85 | 9 (56.2) | 7 (46.7) | |
| Male | 8 (50.0) | 6 (40.0) | |
| Height, cm | 156.1 ± 11.1 | 159.2 ± 10.6 | |
| Body weight at admission, kg | 56.6 ± 13.7 | 54.4 ± 9.9 | |
| Body mass index, kg/m2 | 23.1 ± 4.4 | 21.6 ± 3.7 | |
| NYHA III/IV at admission, % | 14 (87.5) | 12 (80.0) | |
| Systolic blood pressure, mm Hg | 112 ± 20 | 111 ± 21 | |
| Diastolic blood pressure, mm Hg | 58 ± 12 | 57 ± 11 | |
| Heart rate, beats/min | 70 ± 12 | 82 ± 11 | |
| LVEF, % | 43.2 ± 15.4 | 43.6 ± 19.9 | |
| ≥50 | 5 (31.2) | 5 (33.3) | |
| Diabetes, % | 3 (18.8) | 4 (26.7) | |
| Hypertension, % | 8 (50.0) | 10 (66.7) | |
| Dyslipidemia, % | 5 (31.2) | 6 (40.0) | |
| Current smoker, % | 7 (31.2) | 3 (20.0) | |
| COPD, % | 2 (12.5) | 2 (13.3) | |
| Atrial fibrillation, % | 5 (31.2) | 6 (40.0) | |
| Chronic renal failure, % | 11 (68.8) | 12 (80.0) | |
| Anemia, % | 11 (68.8) | 6 (40.0) | |
| Prior HF admission, % | 5 (31.2) | 3 (20.0) | |
| Charlson comorbidity index, points | 1.9 ± 1.0 | 2.5 ± 1.4 | |
| Laboratory data at admission | |||
| BNP, pg/mL | 1048 [616, 1480] | 664 [296, 1033] | |
| Albumin, g/dL | 3.4 ± 0.5 | 3.5 ± 0.5 | |
| Hemoglobin, g/dL | 11.4 ± 2.1 | 12.0 ± 2.2 | |
| Creatinine, mg/dL | 1.3 ± 0.6 | 1.2 ± 0.4 | |
| eGFR, mL/min/1.73 m2 | 45.8 ± 19.5 | 44.0 ± 21.0 | |
| Geriatric assessments | |||
| Mini-Cog, points | 3.4 ± 1.4 | 2.9 ± 1.3 | |
| SF-36 PF, points | 54 ± 30 | 56 ± 21 | |
| Frailty score, points | 2.5 ± 1.1 | 2.0 ± 1.1 | |
| SARC-F, points | 3.5 ± 2.2 | 3.5 ± 1.7 | |
| Physical function | |||
| Maximal QIS, %BW | 29.8 ± 8.1 | 25.0 ± 11.1 | |
| Handgrip strength, kg | 20.1 ± 6.9 | 18.3 ± 5.6 | |
| SPPB, points | 7.6 ± 1.5 | 5.9 ± 1.9 | |
| Usual gait speed, m/s | 0.53 ± 0.13 | 0.48 ± 0.16 | |
| 6-min walking distance, m | 173 ± 81 | 155 ± 90 | |
| DSST, points | 26.8 ± 9.7 | 20.1 ± 8.5 | |
| Δ 6MWD | Δ Gait Speed | Δ SPPB | Δ Handgrip Strength | Δ BNP | Δ Body Weight | Δ QIS | |
|---|---|---|---|---|---|---|---|
| Δ QIS | 0.606 * | 0.404 * | 0.547 * | 0.069 | 0.035 | −0.352 | 1 |
| Δ Body weight | −0.511 * | −0.045 | −0.265 | −0.041 | −0.237 | 1 | |
| Δ BNP | 0.266 | 0.293 | −0.029 | 0.057 | 1 | ||
| Δ Handgrip strength | −0.035 | −0.021 | −0.042 | 1 | |||
| Δ SPPB | 0.521 * | 0.585 * | 1 | ||||
| Δ Gait speed | 0.558 * | 1 | |||||
| Δ 6MWD | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, S.; Kamiya, K.; Matsue, Y.; Yonezawa, R.; Saito, H.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Yamashita, M.; Wakaume, K.; et al. Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial. J. Cardiovasc. Dev. Dis. 2022, 9, 99. https://doi.org/10.3390/jcdd9040099
Tanaka S, Kamiya K, Matsue Y, Yonezawa R, Saito H, Hamazaki N, Matsuzawa R, Nozaki K, Yamashita M, Wakaume K, et al. Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial. Journal of Cardiovascular Development and Disease. 2022; 9(4):99. https://doi.org/10.3390/jcdd9040099
Chicago/Turabian StyleTanaka, Shinya, Kentaro Kamiya, Yuya Matsue, Ryusuke Yonezawa, Hiroshi Saito, Nobuaki Hamazaki, Ryota Matsuzawa, Kohei Nozaki, Masashi Yamashita, Kazuki Wakaume, and et al. 2022. "Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial" Journal of Cardiovascular Development and Disease 9, no. 4: 99. https://doi.org/10.3390/jcdd9040099
APA StyleTanaka, S., Kamiya, K., Matsue, Y., Yonezawa, R., Saito, H., Hamazaki, N., Matsuzawa, R., Nozaki, K., Yamashita, M., Wakaume, K., Endo, Y., Maekawa, E., Yamaoka-Tojo, M., Shiono, T., Inomata, T., & Ako, J. (2022). Efficacy and Safety of Acute Phase Intensive Electrical Muscle Stimulation in Frail Older Patients with Acute Heart Failure: Results from the ACTIVE-EMS Trial. Journal of Cardiovascular Development and Disease, 9(4), 99. https://doi.org/10.3390/jcdd9040099