
Pediatric Left Posteroseptal Accessory Pathway Ablation from Giant Coronary Sinus with Persistent Left Superior Cava

 , ,
, ,  ,
, {kind=link}
Abstract
:1. Introduction
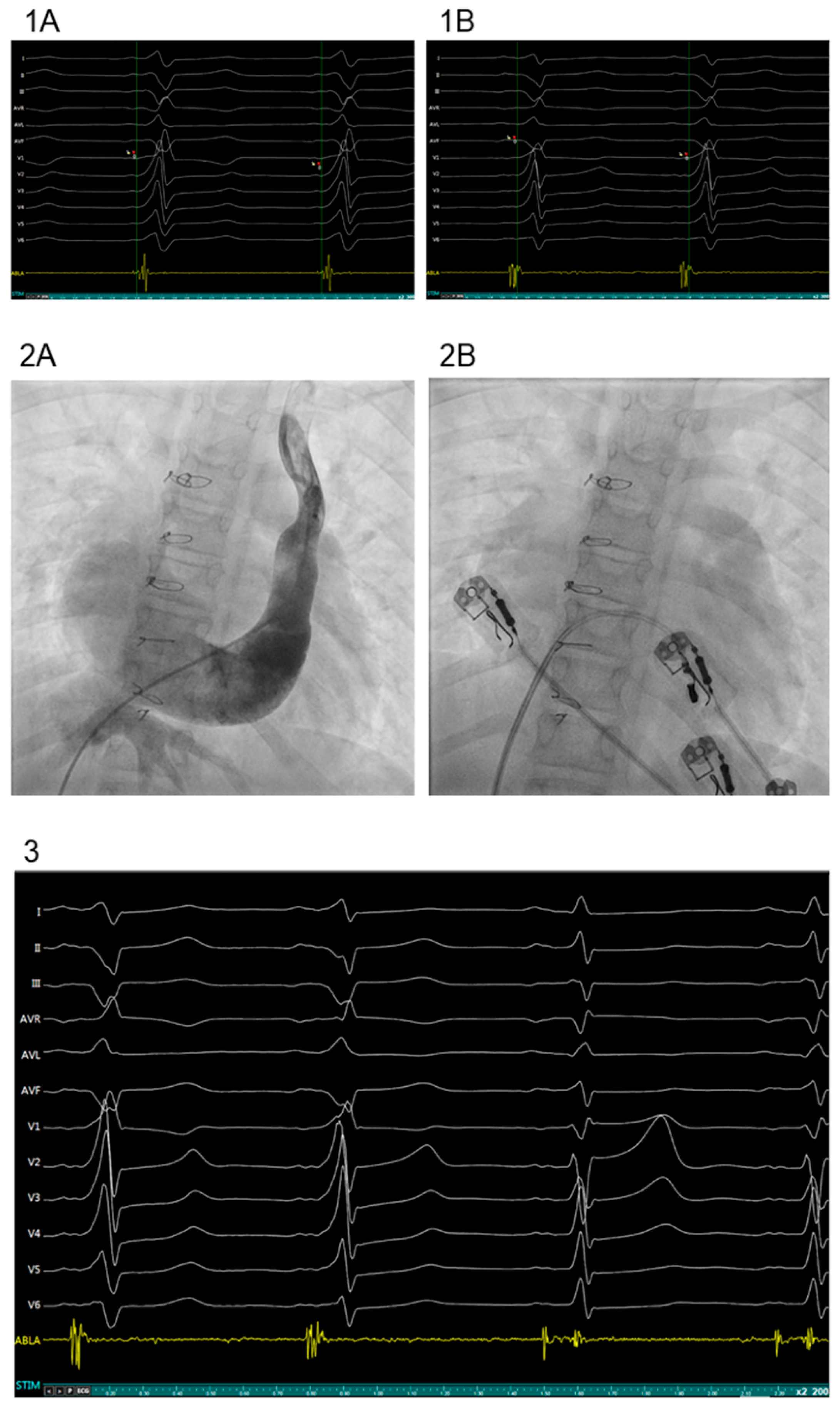
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nagasawa, H.; Kuwabara, N.; Goto, H.; Omoya, K.; Yamamoto, T.; Terazawa, A.; Kohno, Y.; Kuwahara, T. Incidence of Persistent Left Superior Vena Cava in the Normal Population and in Patients with Congenital Heart Diseases Detected Using Echocardiography. Pediatr. Cardiol. 2018, 39, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Uhm, J.S.; Choi, J.I.; Baek, Y.S.; Yu, H.T.; Yang, P.S.; Kim, Y.G.; Oh, S.K.; Park, H.S.; Lee, K.N.; Kim, T.H.; et al. Electrophysiological features and radiofrequency catheter ablation of supraventricular tachycardia in patients with persistent left superior vena cava. Heart Rhythm. 2018, 15, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Azizova, A.; Onder, O.; Arslan, S.; Ardali, S.; Hazirolan, T. Persistent left superior vena cava: Clinical importance and differential diagnoses. Insights Imaging 2020, 11, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Al Fagih, A.; Al Zahrani, G.; Al Hebaishi, Y.; Dagriri, K.; Al Ghamdi, S.A. Coronary sinus diverticulum as a cause of resistant posteroseptal pathway ablation. J. Saudi Heart Assoc. 2011, 23, 41–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.; Park, H.S.; Kim, J.; Kim, J.S.; Park, J.S.; Kim, K.H.; Bae, M.H.; Lee, S.H.; Lee, Y.S.; Han, S.; et al. Supraventricular tachyarrhythmias in patients with a persistent left superior vena cava. Europace 2018, 20, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.; Chandra, S.; Naik, N.; Juneja, R. Radiofrequency catheter ablation of atrioventricular nodal reentrant tachycardia associated with anomalous drainage of both superior vena cava into coronary sinus. Indian Pacing Electrophysiol. J. 2009, 9, 278. [Google Scholar] [PubMed]
- Miyazawa, H.; Morishima, I.; Kanzaki, Y.; Kamiya, Y. Cryoablation for atrioventricular nodal re-entrant tachycardia associated with persistent left superior vena cava. Indian Pacing Electrophysiol. J. 2021, 21, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Okishige, K.; Fisher, J.D.; Goseki, Y.; Azegami, K.; Satoh, T.; Ohira, H.; Yamashita, K.; Satake, S. Radiofrequency catheter ablation for AV nodal reentrant tachycardia associated with persistent left superior vena cava. Pacing Clin. Electrophysiol. 1997, 20, 2213–2218. [Google Scholar] [CrossRef] [PubMed]
- Kursaklioglu, H.; Kose, S.; Barcin, C.; Iyisoy, A.; Isik, E.; Demirtas, E. Radiofrequency catheter ablation of a left lateral accessory pathway in a patient with persistent left superior vena cava. Heart Dis. 2002, 4, 162–165. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruzalegui, J.; Cesar, S.; Campuzano, O.; Fiol, V.; Brugada, J.; Sarquella-Brugada, G. Pediatric Left Posteroseptal Accessory Pathway Ablation from Giant Coronary Sinus with Persistent Left Superior Cava. J. Cardiovasc. Dev. Dis. 2022, 9, 109. https://doi.org/10.3390/jcdd9040109
Cruzalegui J, Cesar S, Campuzano O, Fiol V, Brugada J, Sarquella-Brugada G. Pediatric Left Posteroseptal Accessory Pathway Ablation from Giant Coronary Sinus with Persistent Left Superior Cava. Journal of Cardiovascular Development and Disease. 2022; 9(4):109. https://doi.org/10.3390/jcdd9040109
Chicago/Turabian StyleCruzalegui, José, Sergi Cesar, Oscar Campuzano, Victoria Fiol, Josep Brugada, and Georgia Sarquella-Brugada. 2022. "Pediatric Left Posteroseptal Accessory Pathway Ablation from Giant Coronary Sinus with Persistent Left Superior Cava" Journal of Cardiovascular Development and Disease 9, no. 4: 109. https://doi.org/10.3390/jcdd9040109
APA StyleCruzalegui, J., Cesar, S., Campuzano, O., Fiol, V., Brugada, J., & Sarquella-Brugada, G. (2022). Pediatric Left Posteroseptal Accessory Pathway Ablation from Giant Coronary Sinus with Persistent Left Superior Cava. Journal of Cardiovascular Development and Disease, 9(4), 109. https://doi.org/10.3390/jcdd9040109