
A Propensity Score Analysis of Early and Long-Term Outcomes of Retrograde Arterial Perfusion for Endoscopic and Minimally Invasive Heart Valve Surgery in Both Young and Elderly Patients

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Surgical Technique
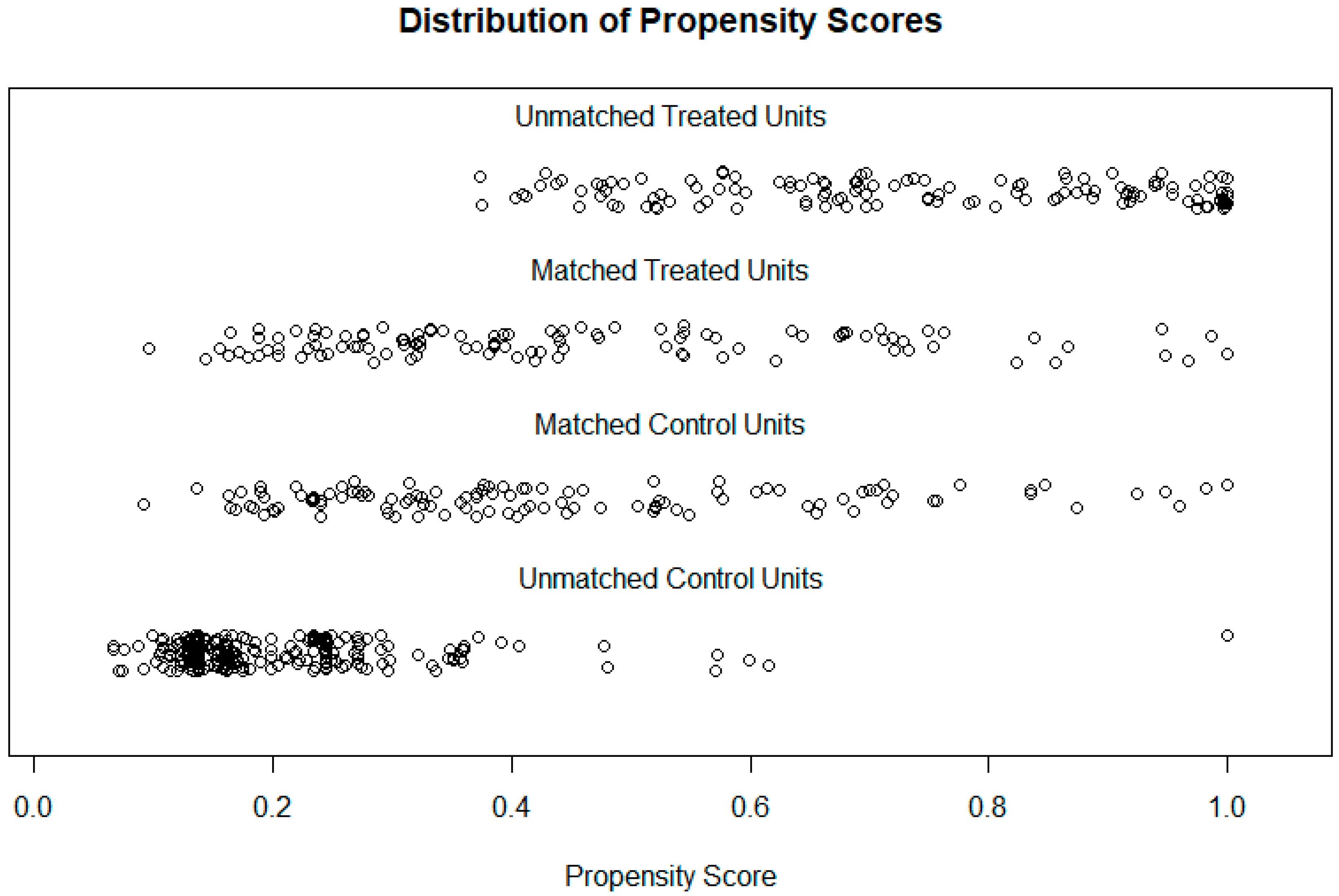
4. Data Analysis
5. Results
5.1. Patient Characteristics and Operative Data
5.2. Risk-Adjusted In-Hospital Outcomes
5.3. Primary Endpoint: Post-Operative Complications
5.4. Secondary Endpoint: Survival Rates
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soltesz, E.G.; Cohn, L.H. Minimally invasive valve surgery. Cardiol. Rev. 2007, 15, 109–115. Available online: https://journals.lww.com/cardiologyinreview/Fulltext/2007/05000/Minimally_Invasive_Valve_Surgery.1.aspx (accessed on 16 August 2021). [CrossRef] [PubMed][Green Version]
- Cheng, D.C.; Martin, J.; Lal, A.; Diegeler, A.; Folliguet, T.A.; Nifong, L.W.; Perier, P.; Raanani, E.; Smith, J.M.; Seeburger, J.; et al. Minimally invasive versus conventional open mitral valve surgery: A meta-analysis and systematic review. Innovations 2011, 6, 84–103. Available online: https://journals.sagepub.com/doi/10.1097/IMI.0b013e3182167feb?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub++0pubmed (accessed on 16 August 2021). [CrossRef] [PubMed]
- Glower, D.D.; Landolfo, K.P.; Clements, F.; Debruijn, N.P.; Stafford-Smith, M.; Smith, P.K.; Duhaylongsod, F. Mitral valve operation via Port Access versus median sternotomy. Eur. J. Cardio-Thorac. Surg. 1998, 14, S143–S147. Available online: https://academic.oup.com/ejcts/article/14/Supplement_1/S143/408260 (accessed on 16 December 2021). [CrossRef]
- Chitwood, J.; Wixon, C.L.; Elbeery, J.R.; Moran, J.F.; Chapman, W.H.H.; Lust, R.M. Video-assisted minimally invasive mitral valve surgery. J. Thorac. Cardiovasc. Surg. 1997, 114, 773–782. [Google Scholar] [CrossRef]
- Felger, J.E.; Chitwood, W.R.; Nifong, L.W.; Holbert, D. Evolution of mitral valve surgery: Toward a totally endoscopic approach. Ann. Thorac. Surg. 2001, 72, 1203–1209. [Google Scholar] [CrossRef]
- Grossi, E.A.; Loulmet, D.F.; Schwartz, C.F.; Ursomanno, P.; Zias, E.A.; Dellis, S.L.; Galloway, A.C. Evolution of operative techniques and perfusion strategies for minimally invasive mitral valve repair. J. Thorac. Cardiovasc. Surg. 2012, 143, S68–S70. Available online: http://www.jtcvs.org/article/S0022522312000128/fulltext (accessed on 16 August 2021). [CrossRef]
- Grossi, E.A.; Galloway, A.C.; LaPietra, A.; Ribakove, G.H.; Ursomanno, P.; Delianides, J.; Culliford, A.T.; Bizekis, C.; Esposito, R.A.; Baumann, F.G.; et al. Minimally invasive mitral valve surgery: A 6-year experience with 714 patients. Ann. Thorac. Surg. 2002, 74, 660–664. Available online: http://www.annalsthoracicsurgery.org/article/S0003497502037542/fulltext (accessed on 16 August 2021). [CrossRef]
- Greco, E.; Mestres, C.A.; Cartañá, R.; Pomar, J.L. Video-Assisted Cardioscopy for Removal of Primary Left Ventricular Myxoma. Eur. J. Cardio-Thorac. Surg. 1999, 16, 677–678. [Google Scholar] [CrossRef]
- Belluschi, I.; Lapenna, E.; Blasio, A.; del Forno, B.; Giacomini, A.; Ruggeri, S.; Schiavi, D.; Castiglioni, A.; Alfieri, O.; de Bonis, M. Excellent Long-Term Results with Minimally Invasive Edge-to-Edge Repair in Myxomatous Degenerative Mitral Valve Regurgitation. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 28–34. [Google Scholar] [CrossRef]
- Grant, S.W.; Hickey, G.L.; Modi, P.; Hunter, S.; Akowuah, E.; Zacharias, J. Propensity-Matched Analysis of Minimally Invasive Approach versus Sternotomy for Mitral Valve Surgery. Heart 2019, 105, 783–789. [Google Scholar] [CrossRef]
- Glauber, M.; Miceli, A.; Canarutto, D.; Lio, A.; Murzi, M.; Gilmanov, D.; Ferrarini, M.; Farneti, P.A.; Quaini, E.L.; Solinas, M. Early and Long-Term Outcomes of Minimally Invasive Mitral Valve Surgery through Right Minithoracotomy: A 10-Year Experience in 1604 Patients. J. Cardiothorac. Surg. 2015, 10, 181. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, J.; Greco, E. The Treatment of Mitral Valve Disease—The Only Thing Constant Is Change. Biomedicines 2021, 9, 126. [Google Scholar] [CrossRef] [PubMed]
- Kastengren, M.; Svenarud, P.; Ahlsson, A.; Dalén, M. Minimally Invasive Mitral Valve Surgery Is Associated with a Low Rate of Complications. J. Intern. Med. 2019, 286, 614–626. [Google Scholar] [CrossRef] [PubMed]
- Murzi, M.; Cerillo, A.G.; Miceli, A.; Bevilacqua, S.; Kallushi, E.; Farneti, P.; Solinas, M.; Glauber, M. Antegrade and Retrograde Arterial Perfusion Strategy in Minimally Invasive Mitral-Valve Surgery: A Propensity Score Analysis on 1280 Patients. Eur. J. Cardio-Thorac. Surg. 2013, 43, e167–e172. [Google Scholar] [CrossRef]
- Gammie, J.S.; Zhao, Y.; Peterson, E.D.; O’Brien, S.M.; Rankin, J.S.; Griffith, B.P. Less-Invasive Mitral Valve Operations: Trends and Outcomes From The Society of Thoracic Surgeons Adult Cardiac Surgery Database. Ann. Thorac. Surg. 2010, 90, 1401–1410.e1. Available online: http://www.annalsthoracicsurgery.org/article/S000349751001218X/fulltext (accessed on 16 October 2021). [CrossRef]
- Modi, P.; Chitwood, W.R., Jr. Retrograde femoral arterial perfusion and stroke risk during minimally invasive mitral valve surgery: Is there cause for concern? Ann. Cardiothorac. Surg. 2013, 2, E1. [Google Scholar]
- Crooke, G.A.; Schwartz, C.F.; Ribakove, G.H.; Ursomanno, P.; Gogoladze, G.; Culliford, A.T.; Galloway, A.C.; Grossi, E.A. Retrograde Arterial Perfusion, Not Incision Location, Significantly Increases the Risk of Stroke in Reoperative Mitral Valve Procedures. Ann. Thorac. Surg. 2010, 89, 723–730. Available online: http://www.annalsthoracicsurgery.org/article/S0003497509023935/fulltext (accessed on 16 September 2021). [CrossRef]
- Moodley, S.; Schoenhagen, P.; Gillinov, A.M.; Mihaljevic, T.; Flamm, S.D.; Griffin, B.P.; Desai, M.Y. Preoperative multidetector computed tomograpy angiography for planning of minimally invasive robotic mitral valve surgery: Impact on decision making. J. Thorac. Cardiovasc. Surg. 2013, 146, 262–268.e1. Available online: http://www.jtcvs.org/article/S0022522312007313/fulltext (accessed on 16 December 2021). [CrossRef][Green Version]
- Holzhey, D.M.; Seeburger, J.; Misfeld, M.; Borger, M.A.; Mohr, F.W. Learning minimally invasive mitral valve surgery: A cumulative sum sequential probability analysis of 3895 operations from a single high-volume center. Circulation 2013, 128, 483–491. Available online: https://pubmed.ncbi.nlm.nih.gov/23804253/ (accessed on 16 September 2021). [CrossRef]
- Tabata, M.; Cohn, L.H. Minimally invasive mitral valve repair with and without robotic technology in the elderly. Am. J. Geriatr. Cardiol. 2006, 15, 306–310. Available online: https://pubmed.ncbi.nlm.nih.gov/16957450/ (accessed on 16 September 2021). [CrossRef]
- Grossi, E.A.; Galloway, A.C.; Ribakove, G.H.; Buttenheim, P.M.; Esposito, R.; Baumann, F.G.; Colvin, S.B. Minimally invasive port access surgery reduces operative morbidity for valve replacement in the elderly. Heart Surg. Forum 1999, 2, 212–215. Available online: https://europepmc.org/article/med/11276477 (accessed on 16 August 2021). [PubMed]
- Schneider, F.; Onnasch, J.F.; Falk, V.; Walther, T.; Autschbach, R.; Mohr, F.W. Cerebral microemboli during minimally invasive and conventional mitral valve operations. Ann. Thorac. Surg. 2000, 70, 1094–1097. Available online: https://pubmed.ncbi.nlm.nih.gov/11016385/ (accessed on 16 August 2021). [CrossRef]


{kind=link}
| Variable | Elderly Patients Age ≥ 70 (n = 241) | Adult Patients Age < 70 (n = 355) | p-Value |
|---|---|---|---|
| Age | 76.0 [72, 79] | 58 [47, 65] | p < 0.001 |
| Female | 105 (43.6%) | 116 (32.7%) | p = 0.009 |
| BMI (Body Mass Index) | 26.2 [23.3, 29.2] | 26.5 [23.5, 29.5] | p = 0.41 |
| DM (Diabetes Mellitus) | 25 (10.3%) | 21 (5.9%) | p = 0.065 |
| HTN | 148 (61.4%) | 132 (37.8%) | p < 0.001 |
| Peripheral vascular disease | 13 (5.4%) | 13 (3.7%) | p = 0.42 |
| COPD | 33 (13.7%) | 50 (14.1%) | p = 0.97 |
| CKD (chronic kidney disease) | 4 (1.7%) | 2 (0.6%) | 0.37 |
| Previous stroke: TIA (Transient Ischaemic Attack) CVA (cerebrovascular accident) | 27 (11.2%) 9 (3.7%) | 16 (4.5%) 12 (3.4%) | p = 0.008 |
| Pre-op AF | 55 (22.8%) | 27 (7.6%) | p < 0.001 |
| Urgent operation | 16 (6.6%) | 37 (10.4%) | p = 0.15 |
| NYHA class III/IV | 129 (57.5%) | 151 (46.5%) | p = 0.011 |
| Ejection fraction < 30% | 6 (2.5%) | 10 (2.8%) | p > 0.99 |
| Logistic Euro Score | 7.01 [4.25, 12.25] | 2.4 [1.51, 4.38] | p < 0.001 |
| Variable | Elderly Patients >= 70 | Adult Patients < 70 | p Value |
|---|---|---|---|
| CPB time (mins) | 146 [127, 172] | 152 [131, 185] | p = 0.036 |
| Aortic clamp time | 96 [75, 111] | 103 [82, 127] | p < 0.001 |
| Mitral valve procedure +/− Tricuspid valve procedure +/− other | 177 (73.4%) | 291 (82%) | p = 0.017 |
| Other cardiac procedure +/− valve | 0 (0%) | 23 (6.5%) | |
| Aortic valve procedure | 64 (26.6%) | 61 (17.2%) | p = 0.006 |
| AF ablation | 56 (23.2%) | 40 (11.3%) | p < 0.001 |
| Conversion to sternotomy | 8 (3.3%) | 16 (4.5%) | p = 0.61 |
| Variable | Elderly Patients Age ≥ 70 (n = 112) | Adult Patients Age < 70 (n = 112) | p-Value |
|---|---|---|---|
| Age | 75.0 [71, 79] | 64.0 [55, 68] | p < 0.001 |
| Female | 69 (38.4%) | 57 (49.1%) | p = 0.14 |
| BMI | 26.4 [23.6, 29.2] | 26.4 [23.2, 29.8] | p = 0.85 |
| DM | 6 (5.4%) | 6 (5.4%) | p > 0.99 |
| HTN | 57 (50.9%) | 57 (50.9%) | p > 0.99 |
| Peripheral vascular disease | 3 (2.7%) | 8 (7.1%) | p = 0.22 |
| COPD | 14 (12.5%) | 12 (10.7%) | p = 0.83 |
| CKD | 1 (0.9%) | 2 (1.8%) | p > 0.99 |
| Previous stroke: TIA CVA | 9 (8.0%) 3 (2.7%) | 8 (7.1%) 5 (4.5%) | p = 0.75 |
| Pre-op AF | 17 (15.2%) | 17 (15.2%) | p > 0.99 |
| Urgent operation | 5 (4.5%) | 11 (9.8%) | p = 0.19 |
| NYHA class III/IV | 55 (49.1%) | 52 (46.4%) | p = 0.79 |
| Ejection fraction < 30% | 1 (0.9%) | 7 (6.2%) | p = 0.07 |
| Logistic Euro Score | 4.83 [3.51, 7.46] | 4.70 [3.19, 7.17] | p = 0.36 |
| Variable | Elderly Patients Age ≥ 70 (n = 112) | Adult Patients Age < 70 (n = 112) | p-Value |
|---|---|---|---|
| Stroke: transient permanent | 1 (0.9%) 2 (1.8%) | 3 (2.7%) 2 (1.8%) | p = 0.60 |
| MI | 0 | 0 | p > 0.99 |
| New post-operative AF | 6 (5.4%) | 2 (1.8%) | p = 0.66 |
| Renal failure | 4 (3.6%) | 0 | p = 0.12 |
| Re-operation (any purpose) | 4 (3.6%) | 4 (3.6%) | p > 0.99 |
| Pulmonary complications | 16 (14.3%) | 11 (9.8%) | p = 0.41 |
| ICU LOS (days) | 1.0 [1.0, 1.0] | 1.0 [1.0, 1.0] | p = 0.77 |
| Inotropes | 30 (26.8%) | 34 (30.4%) | p = 0.66 |
| GI complications | 4 (3.6%) | 2 (1.8%) | p = 0.68 |
| Required blood transfusion | 7 (7.1%) | 6 (6.2%) | p = 0.87 |
| Extubation > 12 h | 10 (8.9%) | 14 (12.5%) | p = 0.52 |
| Duration of hospitalisation (days) | 7 [5, 9] | 6 [5, 8] | p = 0.38 |
| Discharge destination (home) | 105 (93.8%) | 107 (95.5%) | p = 0.42 |
| Reintervention | 1 (0.9%) | 3 (2.7%) | p = 0.60 |
| Variable | Elderly Patients Age ≥ 70 | Adult Patients Age < 70 | p-Value | The Relative Risk of Death for Elderly Patients over Adult (CI) |
|---|---|---|---|---|
| Mortality | 4 (3.6%) | 1 (0.9%) | p = 0.37 | 4.0 [0.45, 35.2] |
| One year survival | 104/110 (94.5%) | 99/101 (98.0%) | p = 0.28 | 2.8 [0.57, 13.3] |
| 3 years survival | 76/88 (86.4%) | 85/90 (94.4%) | p = 0.078 | 1.7 [0.58, 5.0] |
| Time Period (Postop) | Mean Restricted Survival in Years (95% Confidence Interval) | Difference in RMST | |
|---|---|---|---|
| Elderly (Age ≥ 70) | Adult (Age < 70) | ||
| 1 year | 0.96 [0.92, 0.99] | 0.98 [0.96, 1.00] | 0.02 [−0.07, 0.02] |
| 3 years | 2.78 [2.65, 2.91] | 2.90 [2.81, 2.99] | 0.12 [−0.27, 0.04] |
| 5 years | 4.46 [4.21, 4.71] | 4.75 [4.57, 4.93] | 0.29 [−0.60, 0.02] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elhassan, H.; Abdelbar, A.; Taylor, R.; Laskawski, G.; Saravanan, P.; Knowles, A.; Zacharias, J. A Propensity Score Analysis of Early and Long-Term Outcomes of Retrograde Arterial Perfusion for Endoscopic and Minimally Invasive Heart Valve Surgery in Both Young and Elderly Patients. J. Cardiovasc. Dev. Dis. 2022, 9, 44. https://doi.org/10.3390/jcdd9020044
Elhassan H, Abdelbar A, Taylor R, Laskawski G, Saravanan P, Knowles A, Zacharias J. A Propensity Score Analysis of Early and Long-Term Outcomes of Retrograde Arterial Perfusion for Endoscopic and Minimally Invasive Heart Valve Surgery in Both Young and Elderly Patients. Journal of Cardiovascular Development and Disease. 2022; 9(2):44. https://doi.org/10.3390/jcdd9020044
Chicago/Turabian StyleElhassan, Hind, Abdelrahman Abdelbar, Rebecca Taylor, Grzegorz Laskawski, Palanikumar Saravanan, Andrew Knowles, and Joseph Zacharias. 2022. "A Propensity Score Analysis of Early and Long-Term Outcomes of Retrograde Arterial Perfusion for Endoscopic and Minimally Invasive Heart Valve Surgery in Both Young and Elderly Patients" Journal of Cardiovascular Development and Disease 9, no. 2: 44. https://doi.org/10.3390/jcdd9020044
APA StyleElhassan, H., Abdelbar, A., Taylor, R., Laskawski, G., Saravanan, P., Knowles, A., & Zacharias, J. (2022). A Propensity Score Analysis of Early and Long-Term Outcomes of Retrograde Arterial Perfusion for Endoscopic and Minimally Invasive Heart Valve Surgery in Both Young and Elderly Patients. Journal of Cardiovascular Development and Disease, 9(2), 44. https://doi.org/10.3390/jcdd9020044