
Early Investigational and Experimental Therapeutics for the Treatment of Hypertriglyceridemia


Abstract
:1. Introduction
2. Apolipoprotein (APO) C-III Inhibitors
3. Omega-3 Fatty Acids (FA)
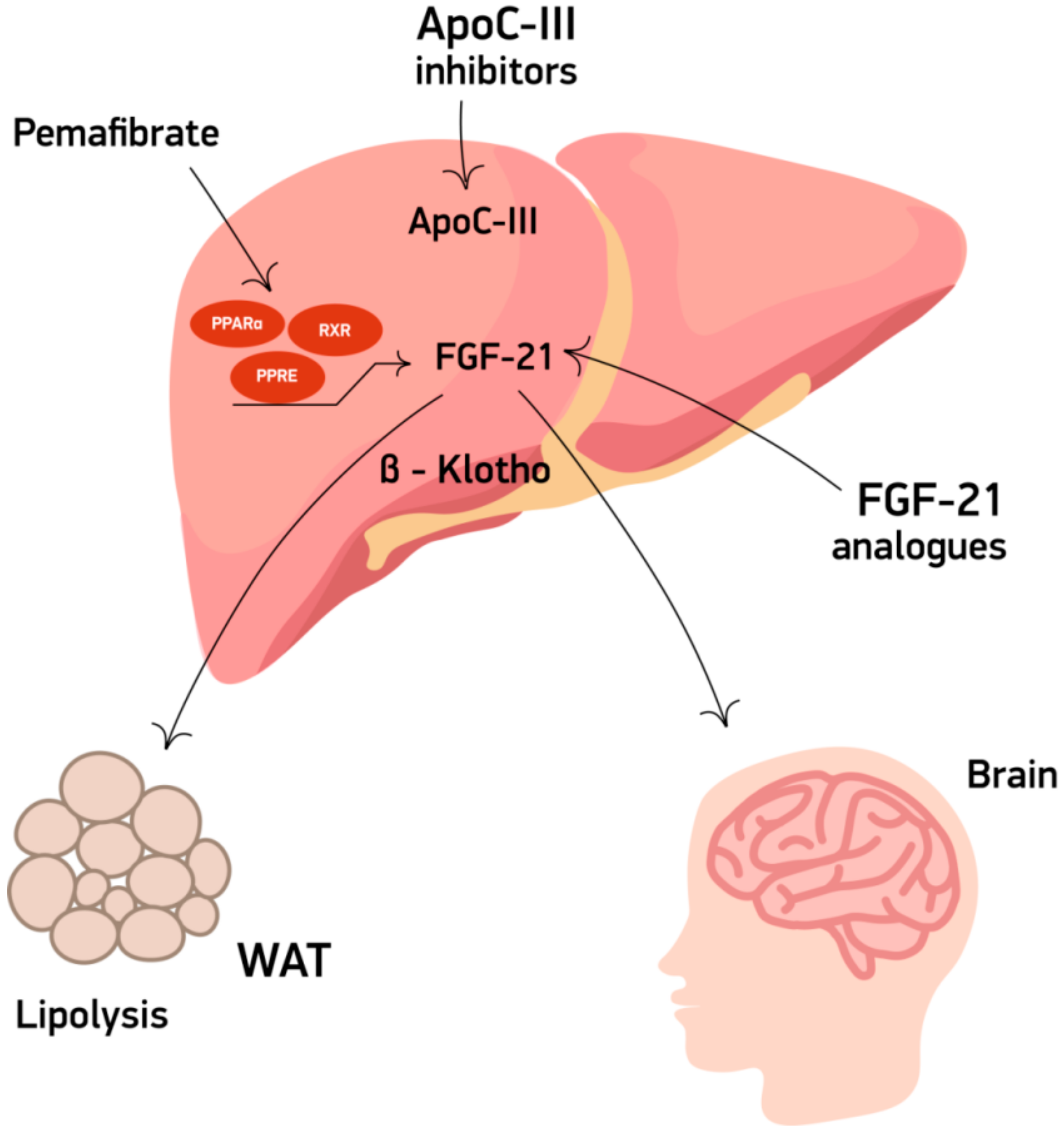
4. Fibroblast Growth Factor 21 (FGF21) Analogues
5. Pemafibrate
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nordestgaard, B.G.; Varbo, A. Triglycerides and cardiovascular disease. Lancet 2014, 384, 626–635. [Google Scholar]
- Guo, Y.Y.; Li, H.X.; Zhang, Y.; He, W.H. Hypertriglyceridemia-induced acute pancreatitis: Progress on disease mechanisms and treatment modalities. Discov. Med. 2019, 27, 101–109. [Google Scholar]
- Reiner, Z. Hypertriglyceridaemia and risk of coronary artery disease. Nat. Rev. Cardiol. 2017, 14, 401–411. [Google Scholar]
- Sacks, F.M.; Hermans, M.P.; Fioretto, P.; Valensi, P.; Davis, T.; Horton, E.; Wanner, C.; Al-Rubeaan, K.; Aronson, R.; Barzon, I.; et al. Association between plasma triglycerides and high-density lipoprotein cholesterol and microvascular kidney disease and retinopathy in type 2 diabetes mellitus: A global case-control study in 13 countries. Circulation 2014, 129, 999–1008. [Google Scholar]
- Miller, M.; Cannon, C.P.; Murphy, S.A.; Qin, J.; Ray, K.K.; Braunwald, E. Impact of triglyceride levels beyond low-density lipoprotein cholesterol after acute coronary syndrome in the PROVE IT-TIMI 22 trial. J. Am. Coll. Cardiol. 2008, 51, 724–730. [Google Scholar]
- Schwartz, G.G.; Abt, M.; Bao, W.; DeMicco, D.; Kallend, D.; Miller, M.; Mundl, H.; Olsson, A.G. Fasting triglycerides predict recurrent ischemic events in patients with acute coronary syndrome treated with statins. J. Am. Coll. Cardiol. 2015, 65, 2267–2275. [Google Scholar]
- Sarwar, N.; Danesh, J.; Eiriksdottir, G.; Sigurdsson, G.; Wareham, N.; Bingham, S.; Boekholdt, S.M.; Khaw, K.T.; Gudnason, V. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation 2007, 115, 450–458. [Google Scholar]
- Ye, X.; Kong, W.; Zafar, M.I.; Chen, L.L. Serum triglycerides as a risk factor for cardiovascular diseases in type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Cardiovasc. Diabetol. 2019, 18, 48. [Google Scholar]
- Raposeiras-Roubin, S.; Rosselló, X.; Oliva, B.; Fernández-Friera, L.; Mendiguren, J.M.; Andrés, V.; Bueno, H.; Sanz, J.; Martínez de Vega, V.; Abu-Assi, E.; et al. Triglycerides and Residual Atherosclerotic Risk. J. Am. Coll. Cardiol. 2021, 77, 3031–3041. [Google Scholar]
- Gan, S.I.; Edwards, A.L.; Symonds, C.J.; Beck, P.L. Hypertriglyceridemia-induced pancreatitis: A case-based review. World J. Gastroenterol. 2006, 12, 7197–7202. [Google Scholar]
- Miller, M.; Stone, N.J.; Ballantyne, C.; Bittner, V.; Criqui, M.H.; Ginsberg, H.N.; Goldberg, A.C.; Howard, W.J.; Jacobson, M.S.; Kris-Etherton, P.M.; et al. Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2011, 123, 2292–2333. [Google Scholar]
- Nicholls, S.J.; Brandrup-Wognsen, G.; Palmer, M.; Barter, P.J. Meta-analysis of comparative efficacy of increasing dose of Atorvastatin versus Rosuvastatin versus Simvastatin on lowering levels of atherogenic lipids (from VOYAGER). Am. J. Cardiol. 2010, 105, 69–76. [Google Scholar]
- Rizos, E.C.; Ntzani, E.E.; Bika, E.; Kostapanos, M.S.; Elisaf, M.S. Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: A systematic review and meta-analysis. JAMA 2012, 308, 1024–1033. [Google Scholar]
- Florentin, M.; Kostapanos, M.S.; Anagnostis, P.; Liamis, G. Recent developments in pharmacotherapy for hypertriglyceridemia: What’s the current state of the art? Expert Opin. Pharm. 2020, 21, 107–120. [Google Scholar]
- Khan, T.Z.; Schatz, U.; Bornstein, S.R.; Barbir, M. Hypertriglyceridaemia: Contemporary management of a neglected cardiovascular risk factor. Glob. Cardiol. Sci. Pract. 2021, 2021, e202119. [Google Scholar]
- Simha, V. Management of hypertriglyceridemia. BMJ 2020, 371, m3109. [Google Scholar]
- Taskinen, M.R.; Packard, C.J.; Boren, J. Emerging Evidence that ApoC-III Inhibitors Provide Novel Options to Reduce the Residual CVD. Curr. Atheroscler. Rep. 2019, 21, 27. [Google Scholar]
- Ramms, B.; Gordts, P. Apolipoprotein C-III in triglyceride-rich lipoprotein metabolism. Curr. Opin. Lipidol. 2018, 29, 171–179. [Google Scholar]
- Taskinen, M.R.; Boren, J. Why Is Apolipoprotein CIII Emerging as a Novel Therapeutic Target to Reduce the Burden of Cardiovascular Disease? Curr. Atheroscler. Rep. 2016, 18, 59. [Google Scholar]
- Kawakami, A.; Aikawa, M.; Libby, P.; Alcaide, P.; Luscinskas, F.W.; Sacks, F.M. Apolipoprotein CIII in apolipoprotein B lipoproteins enhances the adhesion of human monocytic cells to endothelial cells. Circulation 2006, 113, 691–700. [Google Scholar]
- Jorgensen, A.B.; Frikke-Schmidt, R.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. Loss-of-function mutations in APOC3 and risk of ischemic vascular disease. N. Engl. J. Med. 2014, 371, 32–41. [Google Scholar]
- Laina, A.; Gatsiou, A.; Georgiopoulos, G.; Stamatelopoulos, K.; Stellos, K. RNA Therapeutics in Cardiovascular Precision Medicine. Front. Physiol. 2018, 9, 953. [Google Scholar]
- Yang, X.; Lee, S.R.; Choi, Y.S.; Alexander, V.J.; Digenio, A.; Yang, Q.; Miller, Y.I.; Witztum, J.L.; Tsimikas, S. Reduction in lipoprotein-associated apoC-III levels following volanesorsen therapy: Phase 2 randomized trial results. J. Lipid Res. 2016, 57, 706–713. [Google Scholar]
- Schwabe, R.S.C.; Sullivan, D.; Baker, J.; Clifton, P.; Hamilton, J.; Given, B.; Martin, J.S.; Melquist, S.; Watts, G.F.; Goldberg, I.; et al. RNA interference targeting apolipoprotein C-III with ARO-APOC3 in healthy volunteers mimics lipid and lipoprotein findings seen in subjects with inherited apolipoprotein C-III deficiency. Eur. Heart J. 2020, 41, ehaa946-3330. [Google Scholar]
- Study of ARO-APOC3 in Healthy Volunteers, Hypertriglyceridemic Patients and Patients with Familial Chylomicronemia Syndrome (FCS). Available online: https://www.clinicaltrials.gov/ct2/show/NCT03783377 (accessed on 28 July 2021).
- Study to Evaluate ARO-APOC3 in Adults with Severe Hypertriglyceridemia. Available online: https://clinicaltrials.gov/ct2/show/NCT04720534?recrs=ab&cond=hypertriglyceridemia&draw=2 (accessed on 28 July 2021).
- A First in Human Study of STT-5058, an Antibody That Binds ApoC3. Available online: https://clinicaltrials.gov/ct2/show/NCT04419688?recrs=ab&cond=hypertriglyceridemia&draw=2&rank=8 (accessed on 28 July 2021).
- Esan, O.; Wierzbicki, A.S. Volanesorsen in the Treatment of Familial Chylomicronemia Syndrome or Hypertriglyceridaemia: Design, Development and Place in Therapy. Drug Des. Devel. Ther. 2020, 14, 2623–2636. [Google Scholar]
- Bradberry, J.C.; Hilleman, D.E. Overview of omega-3 Fatty Acid therapies. Pharm. Ther. 2013, 38, 681–691. [Google Scholar]
- Rhainds, D.; Brodeur, M.R.; Tardif, J.C. Investigational drugs in development for hypertriglyceridemia: A coming-of-age story. Expert Opin. Investig. Drugs 2019, 28, 1059–1079. [Google Scholar]
- Kromhout, D.; Giltay, E.J.; Geleijnse, J.M. n-3 fatty acids and cardiovascular events after myocardial infarction. N. Engl. J. Med. 2010, 363, 2015–2026. [Google Scholar]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1540–1550. [Google Scholar]
- Aung, T.; Halsey, J.; Kromhout, D.; Gerstein, H.C.; Marchioli, R.; Tavazzi, L.; Geleijnse, J.M.; Rauch, B.; Ness, A.; Galan, P.; et al. Associations of Omega-3 Fatty Acid Supplement Use with Cardiovascular Disease Risks: Meta-Analysis of 10 Trials Involving 77917 Individuals. JAMA Cardiol. 2018, 3, 225–234. [Google Scholar]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle Jr, R.T.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar]
- Vijayaraghavan, K.; Szerlip, H.M.; Ballantyne, C.M.; Bays, H.E.; Philip, S.; Doyle Jr, R.T.; Juliano, R.A.; Granowitz, C. Icosapent ethyl reduces atherogenic markers in high-risk statin-treated patients with stage 3 chronic kidney disease and high triglycerides. Postgrad. Med. 2019, 131, 390–396. [Google Scholar]
- Miller, M.; Ballantyne, C.M.; Bays, H.E.; Granowitz, C.; Doyle, R.T., Jr.; Juliano, R.A.; Philip, S. Effects of Icosapent Ethyl (Eicosapentaenoic Acid Ethyl Ester) on Atherogenic Lipid/Lipoprotein, Apolipoprotein, and Inflammatory Parameters in Patients with Elevated High-Sensitivity C-Reactive Protein (from the ANCHOR Study). Am. J. Cardiol. 2019, 124, 696–701. [Google Scholar]
- Wulff, A.B.; Nordestgaard, B.G.; Tybjaerg-Hansen, A. APOC3 Loss-of-Function Mutations, Remnant Cholesterol, Low-Density Lipoprotein Cholesterol, and Cardiovascular Risk: Mediation- and Meta-Analyses of 137 895 Individuals. Arter. Thromb. Vasc. Biol. 2018, 38, 660–668. [Google Scholar]
- Digenio, A.; Dunbar, R.L.; Alexander, V.J.; Hompesch, M.; Morrow, L.; Lee, R.G.; Graham, M.J.; Hughes, S.G.; Yu, R.; Singleton, W.; et al. Antisense-Mediated Lowering of Plasma Apolipoprotein C-III by Volanesorsen Improves Dyslipidemia and Insulin Sensitivity in Type 2 Diabetes. Diabetes Care 2016, 39, 1408–1415. [Google Scholar]
- Tillman, E.J.; Rolph, T. FGF21: An Emerging Therapeutic Target for Non-Alcoholic Steatohepatitis and Related Metabolic Diseases. Front. Endocrinol. 2020, 11, 601290. [Google Scholar]
- Lee, S.; Choi, J.; Mohanty, J.; Sousa, L.P.; Tome, F.; Pardon, E.; Steyaert, J.; Lemmon, M.A.; Lax, I.; Schlessinger, J. Structures of beta-klotho reveal a ‘zip code’-like mechanism for endocrine FGF signalling. Nature 2018, 553, 501–505. [Google Scholar]
- Ornitz, D.M.; Itoh, N. The Fibroblast Growth Factor signaling pathway. Wiley Interdiscip. Rev. Dev. Biol. 2015, 4, 215–266. [Google Scholar]
- Kurosu, H.; Choi, M.; Ogawa, Y.; Dickson, A.S.; Goetz, R.; Eliseenkova, A.V.; Mohammadi, M.; Rosenblatt, K.P.; Kliewer, S.A.; Kuro-o, M. Tissue-specific expression of betaKlotho and fibroblast growth factor (FGF) receptor isoforms determines metabolic activity of FGF19 and FGF21. J. Biol. Chem. 2007, 282, 26687–26695. [Google Scholar]
- Keinicke, H.; Sun, G.; Mentzel, C.M.; Fredholm, M.; John, L.M.; Andersen, B.; Raun, K.; Kjaergaard, M. FGF21 regulates hepatic metabolic pathways to improve steatosis and inflammation. Endocr. Connect. 2020, 9, 755–768. [Google Scholar]
- Yu, Y.; He, J.; Li, S.; Song, L.; Guo, X.; Yao, W.; Zou, D.; Gao, X.; Liu, Y.; Bai, F.; et al. Fibroblast growth factor 21 (FGF21) inhibits macrophage-mediated inflammation by activating Nrf2 and suppressing the NF-kappaB signaling pathway. Int. Immunopharmacol. 2016, 38, 144–152. [Google Scholar]
- Cui, A.; Li, J.; Ji, S.; Ma, F.; Wang, G.; Xue, Y.; Liu, Z.; Gao, J.; Han, J.; Tai, P.; et al. The Effects of B1344, a Novel Fibroblast Growth Factor 21 Analog, on Nonalcoholic Steatohepatitis in Nonhuman Primates. Diabetes 2020, 69, 1611–1623. [Google Scholar]
- Andrew Pierce, P.; Moti Rosenstock, P.; Maya Margalit, M.; Hank Mansbach, M. BIO89-100, a novel glycoPEGylated FGF21 Analog, Demonstrates Triglyceride Reduction and Broad Metabolic Effects in Spontaneously Diabetic Obese Cynomolgus Monkeys. J. Clin. Lipidiology 2020, 14, 584–585. [Google Scholar]
- Fruchart, J.C.; Santos, R.D.; Aguilar-Salinas, C.; Aikawa, M.; Al Rasadi, K.; Amarenco, P.; Barter, P.J.; Ceska, R.; Corsini, A.; Després, J.-P. The selective peroxisome proliferator-activated receptor alpha modulator (SPPARMalpha) paradigm: Conceptual framework and therapeutic potential: A consensus statement from the International Atherosclerosis Society (IAS) and the Residual Risk Reduction Initiative (R3i) Foundation. Cardiovasc. Diabetol. 2019, 18, 71. [Google Scholar]
- Pradhan, A.D.; Paynter, N.P.; Everett, B.M.; Glynn, R.J.; Amarenco, P.; Elam, M.; Ginsberg, H.; Hiatt, W.R.; Ishibashi, S.; Koenig, W.; et al. Rationale and design of the Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT) study. Am. Heart J. 2018, 206, 80–93. [Google Scholar]

{kind=link}
| Agent | Trial Design | Primary Endpoint | Secondary Endpoint | Inclusion Criteria | Number of Participants |
|---|---|---|---|---|---|
| ARO-APOC3 (siRNA against apoC-III) | Double-blind, placebo-controlled, phase IIb study | Percent change in fasting TG at week 24 | Percent change in TG levels at week 48 as well as percent changes in apoC-III, HDL-C, non-HDL-C, LDL-C, and apoB at week 48, safety evaluation | Hypertriglyceridemia, i.e., TG > 500 mg/dL | 300 |
| ARO-APOC3 (siRNA against apoC-III) | Phase I trial of healthy individuals evaluating the safety, tolerability, pharmacokinetics, and pharmacodynamics of single and multiple doses of ARO-APOC3given s.c | Number of participants with adverse events related to the drug up to day 113 | Reduction in apoC-III levels up to day 113 and several pharmacokinetic parameters (time to maximum plasma concentration and terminal elimination half time up to 48 h after the injection) | Patients with hypertriglyceridemia (TG > 300 mg/dL) and patients with a diagnosis of FCS | 112 |
| STT-5058 (monoclonal antibody against apoC-III) | Phase I double-blind, randomized, placebo-controlled trial. Consists of 4 parts. Part 1: 6 ascending i.v doses in healthy individuals with TG > 150 mg/dL. Part 2: 4 ascending i.v doses in individuals with TG > 150 mg/dL. Part 3: a single cohort of subjects with TG > 200 mg/dL who will receive 3 of the same doses at 2 week intervals. Part 4: 2 single s.c doses | Safety and tolerability of STT-5058 at week 10 from administration | Good health, BMI between 18 and 35 kg/m2, fasting TG between 150 and 400 mg/dL for part 3, LDL-C between 70 and 160 mg/dL | 104 | |
| NST-1024 (omega-3 FA) | Phase I trial evaluating the safety, tolerability, and pharmacokinetics | Any reported adverse event within 4 weeks | Healthy individuals with elevated TG (>150 mg/dL) | 96 | |
| MAT9001 (omega-3 FA) | Randomized, double blind, placebo-controlled, phase III trial | Safety and efficacy of MAT9001 in lowering TG levels in individuals with severe hypertriglyceridemia | Individuals with fasting TG ≥ 500 mg/dL and <2000 mg/dL while following therapeutic lifestyle changes and a BMI > 20 kg/m2 | 300 | |
| BIO89-100 (FGF21 analogue) (44) | Phase II, randomized, double-blind, placebo-controlled trial | Percentage change in TG levels at week 8 | Alterations in VLDL-C, LDL-C, non-HDL-C, HDL-C, apoB-100, remnant lipoprotein cholesterol, high-sensitivity C-reactive protein, fasting adiponectin | Individuals with severe hypertriglyceridemia (TG > 500 and <2000 mg/dL) | 90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parthymos, I.; Kostapanos, M.S.; Liamis, G.; Florentin, M. Early Investigational and Experimental Therapeutics for the Treatment of Hypertriglyceridemia. J. Cardiovasc. Dev. Dis. 2022, 9, 42. https://doi.org/10.3390/jcdd9020042
Parthymos I, Kostapanos MS, Liamis G, Florentin M. Early Investigational and Experimental Therapeutics for the Treatment of Hypertriglyceridemia. Journal of Cardiovascular Development and Disease. 2022; 9(2):42. https://doi.org/10.3390/jcdd9020042
Chicago/Turabian StyleParthymos, Ioannis, Michael S. Kostapanos, George Liamis, and Matilda Florentin. 2022. "Early Investigational and Experimental Therapeutics for the Treatment of Hypertriglyceridemia" Journal of Cardiovascular Development and Disease 9, no. 2: 42. https://doi.org/10.3390/jcdd9020042
APA StyleParthymos, I., Kostapanos, M. S., Liamis, G., & Florentin, M. (2022). Early Investigational and Experimental Therapeutics for the Treatment of Hypertriglyceridemia. Journal of Cardiovascular Development and Disease, 9(2), 42. https://doi.org/10.3390/jcdd9020042