
Impact of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Cohorts
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
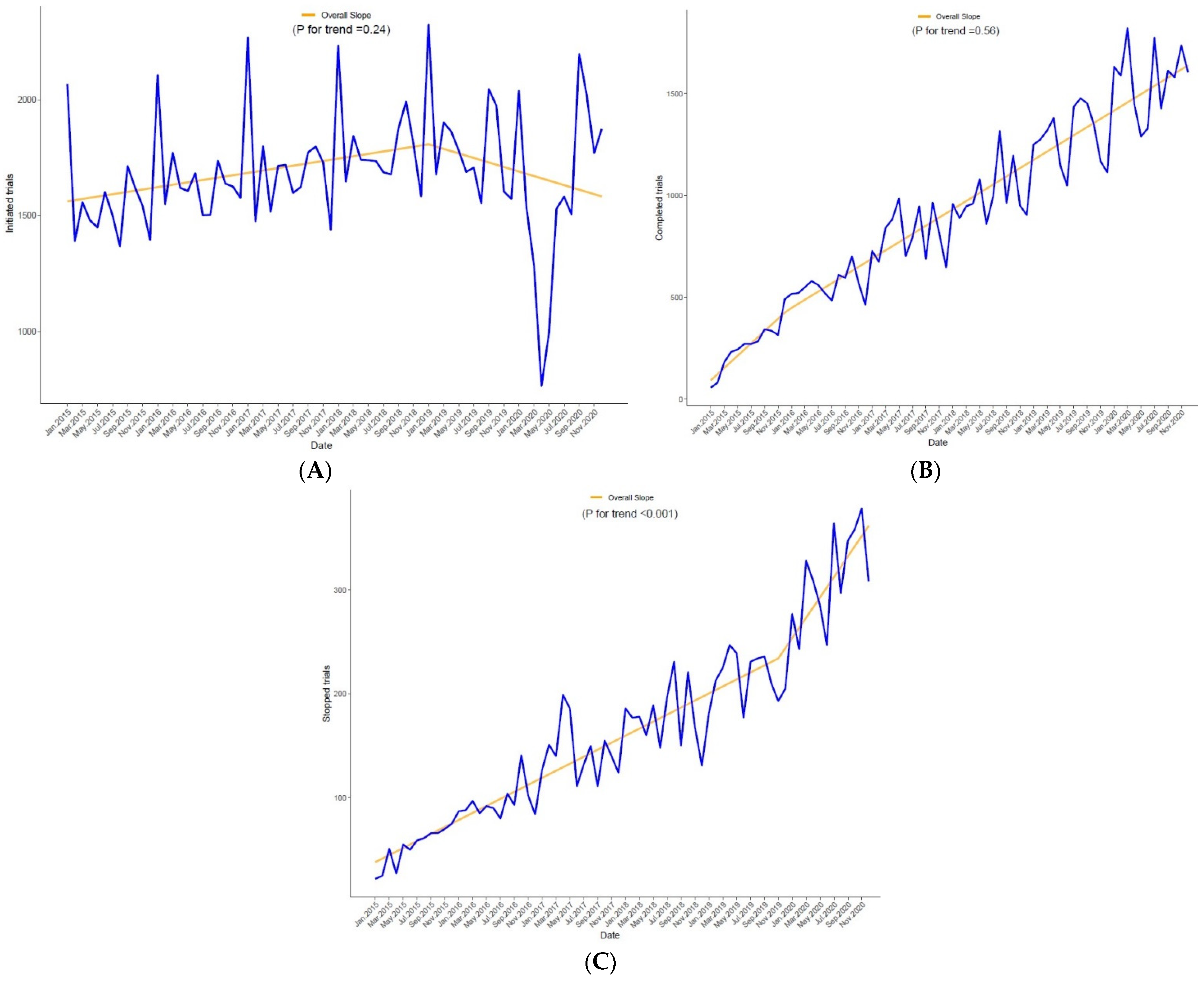
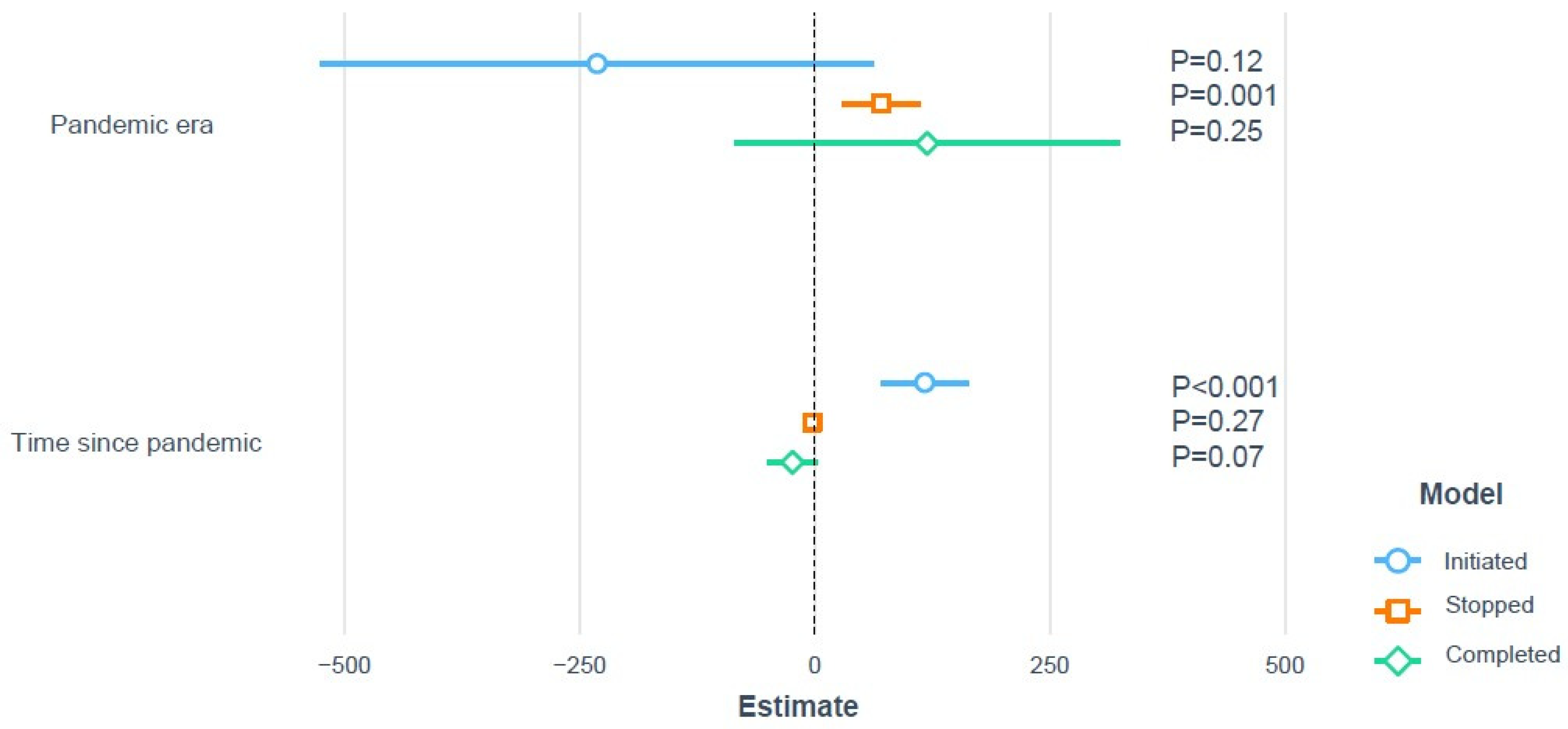
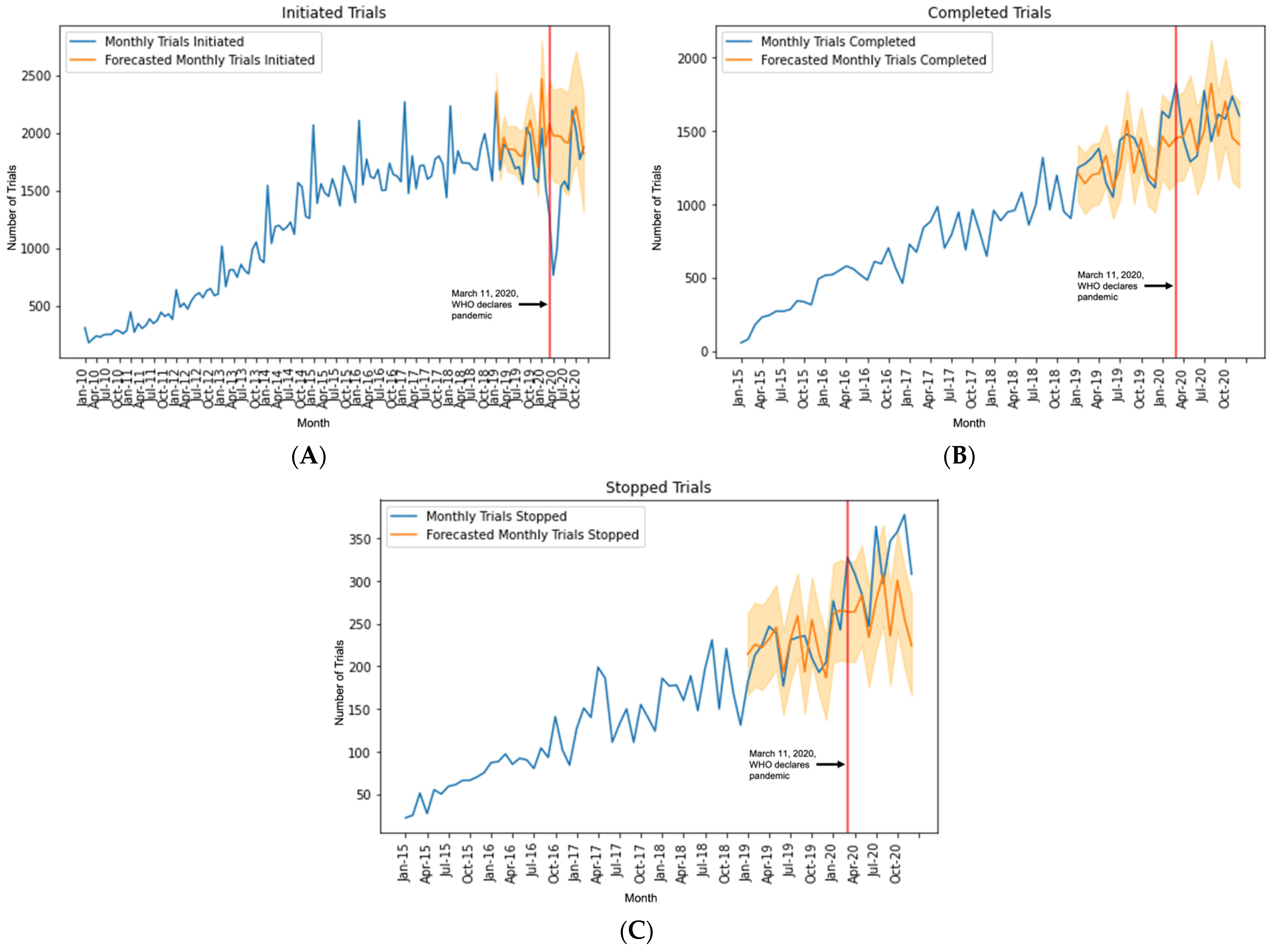
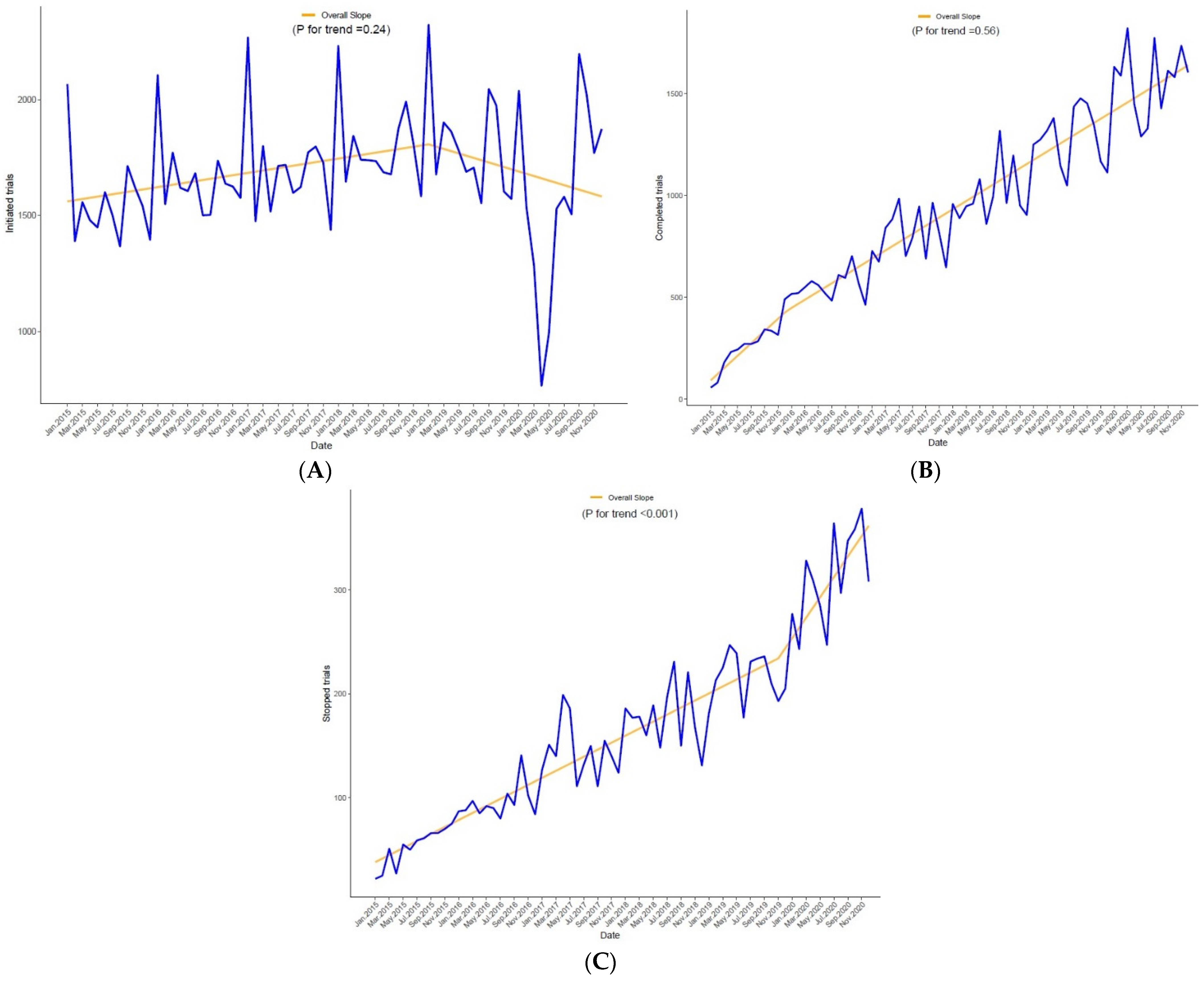
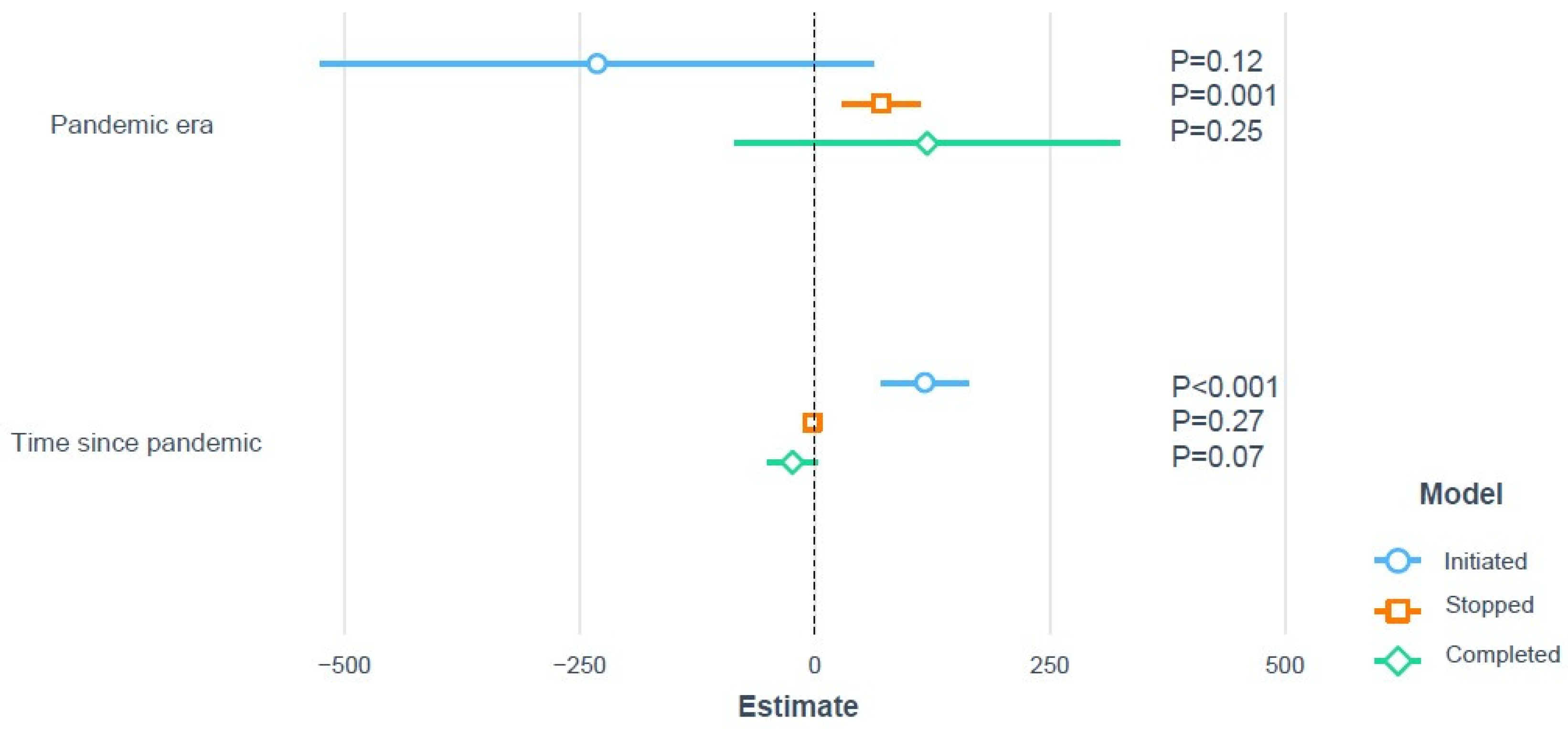
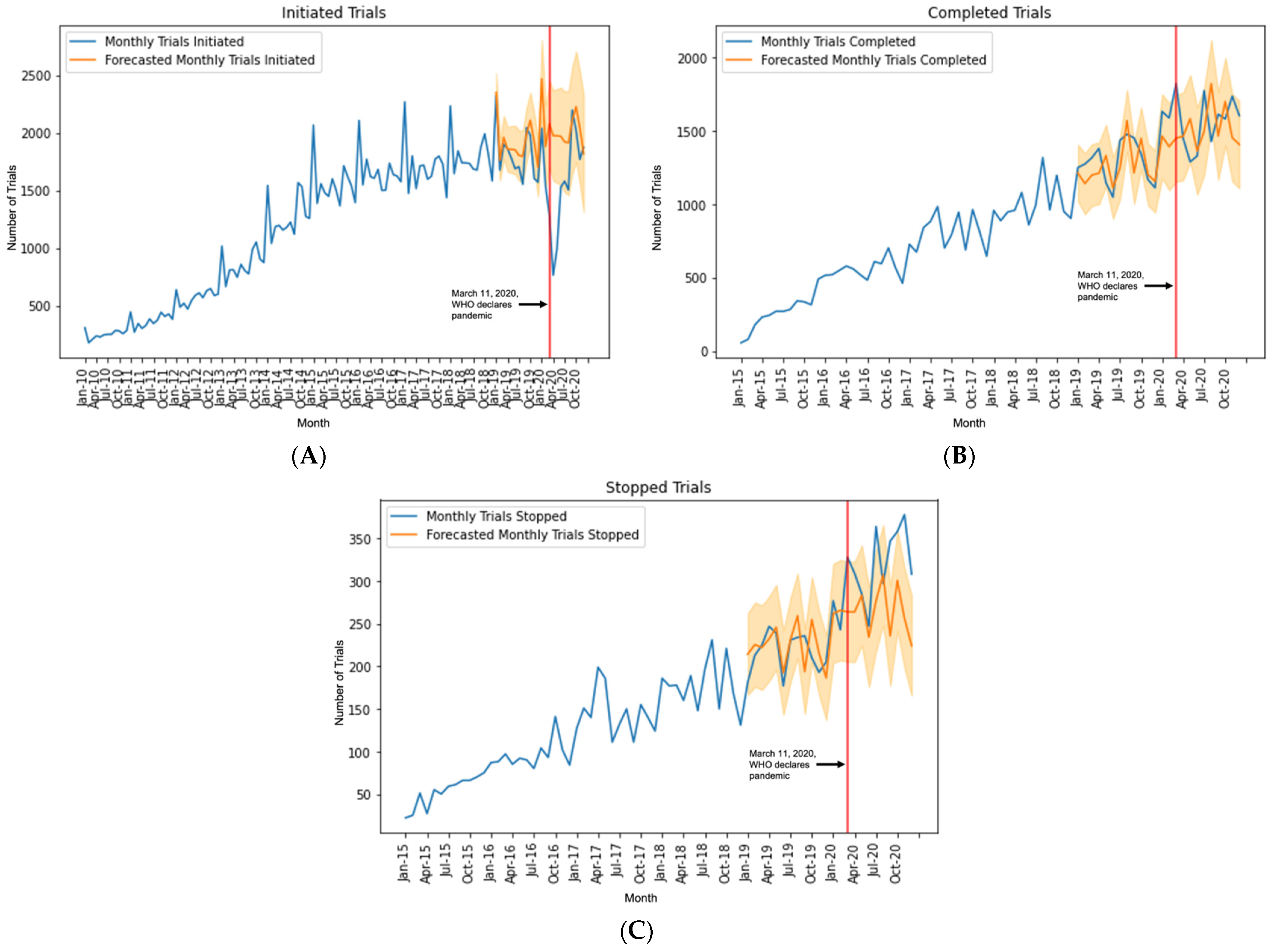
Trends over Time and Pandemic Effect
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johns Hopkins University Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 8 January 2021).
- Chan, C.H.-S.; Tan, E.-K. Safeguarding Non-COVID-19 Research: Looking Up from Ground Zero. Arch. Med. Res. 2020, 51, 731–732. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Califf, R.M.; Harrington, R.A.; Granger, C.B.; McMurray, J.J.V.; Patel, M.R.; Bhatt, D.L.; Windecker, S.; Hernandez, A.F.; Gibson, C.M.; et al. Randomized Trials Versus Common Sense and Clinical Observation. J. Am. Coll. Cardiol. 2020, 76, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Bagiella, E.; Bhatt, D.L.; Gaudino, M. The Consequences of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials. J. Am. Coll. Cardiol. 2020, 76, 342–345. [Google Scholar] [CrossRef]
- Varshney, A.S.; Wang, D.E.; Bhatt, A.S.; Blood, A.; Sharkawi, M.A.; Siddiqi, H.K.; Vaduganathan, M.; Monteleone, P.P.; Patel, M.R.; Jones, W.S.; et al. Characteristics of clinical trials evaluating cardiovascular therapies for Coronavirus Disease 2019 Registered on ClinicalTrials.gov: A cross sectional analysis. Am. Heart J. 2021, 232, 105–115. [Google Scholar] [CrossRef]
- Zarin, D.A.; Tse, T.; Williams, R.J.; Califf, R.M.; Ide, N.C. The ClinicalTrials.gov results database--update and key issues. N. Engl. J. Med. 2011, 364, 852–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKinney, W. Data Structures for Statistical Computing in Python. In Proceedings of the 9th Python in Science Conference (SciPy 2010), Austin, TX, USA, 28 June–3 July 2010; pp. 56–61. [Google Scholar]
- Gaudino, M.; Chikwe, J.; Hameed, I.; Robinson, N.B.; Fremes, S.E.; Ruel, M. Response of Cardiac Surgery Units to COVID-19: An Internationally-Based Quantitative Survey. Circulation 2020, 142, 300–302. [Google Scholar] [CrossRef]
- Upadhaya, S.; Yu, J.X.; Oliva, C.; Hooton, M.; Hodge, J.; Hubbard-Lucey, V.M. Impact of COVID-19 on oncology clinical trials. Nat. Rev. Drug Discov. 2020, 19, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.E.; Farner, A.M.; Unger, J.M. Association of the COVID-19 Outbreak With Patient Willingness to Enroll in Cancer Clinical Trials. JAMA Oncol. 2021, 7, 131–132. [Google Scholar] [CrossRef]
- van Dorn, A. COVID-19 and readjusting clinical trials. Lancet 2020, 396, 523–524. [Google Scholar] [CrossRef]
- Sathian, B.; Asim, M.; Banerjee, I.; Pizarro, A.B.; Roy, B.; van Teijlingen, E.R.; do Nascimento, I.J.B.; Alhamad, H.K. Impact of COVID-19 on clinical trials and clinical research: A systematic review. Nepal. J. Epidemiol. 2020, 10, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, S.; Greene, S.J.; Khatana, S.A.M.; Nathan, A.S.; Solomon, S.D.; Bhatt, D.L. The Landscape of Cardiovascular Clinical Trials in the United States Initiated Before and During COVID-19. JAHA 2020, 9, e018274. [Google Scholar] [CrossRef]
- Vignot, S.; Martin, M.; Albin, N.; Schurtz, C.; Chapel, E. Facilitating access to new therapeutic options through clinical trials: The vision of a regulator to reconcile innovation and safety. Ann. Oncol. 2019, 30, 1694–1696. [Google Scholar] [CrossRef] [Green Version]
- Lamont, E.B.; Diamond, S.S.; Katriel, R.G.; Ensign, L.L.; Liu, J.; Rusli, E.; Alexander, G.C. Trends in Oncology Clinical Trials Launched Before and During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2036353. [Google Scholar] [CrossRef]
- McDermott, M.M.; Newman, A.B. Preserving Clinical Trial Integrity During the Coronavirus Pandemic. JAMA 2020, 323, 2135–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrd, J.B.; Bello, N.; Meyer, M.N. Pandemic Pandemonium: Pausing Clinical Research During the COVID-19 Outbreak. Circulation 2020, 141, 2045–2047. [Google Scholar] [CrossRef]
- Center for Biologics Evaluation and Research. FDA Guidance on Conduct of Clinical Trials of Medical Products During the COVID-19 Public Health Emergency. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/fda-guidance-conduct-clinical-trials-medical-products-during-covid-19-public-health-emergency (accessed on 29 January 2021).
- Czarska-Thorley, D. Implications of Coronavirus Disease (COVID-19) on Methodological Aspects Ongoing Clinical Trials. Available online: https://www.ema.europa.eu/en/implications-coronavirus-disease-covid-19-methodological-aspects-ongoing-clinical-trials (accessed on 4 March 2021).
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Gaba, P.; Bhatt, D.L. The COVID-19 pandemic: A catalyst to improve clinical trials. Nat. Rev. Cardiol. 2020, 17, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Kadakia, K.; Patel, B.; Shah, A. Advancing digital health: FDA innovation during COVID-19. Npj Digit. Med. 2020, 3, 161. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mattar, C.; Zorumski, C.F.; Stevens, A.; Schweiger, J.; Nicol, G.E.; Miller, J.P.; Yang, L.; Yingling, M.; Avidan, M.S.; et al. Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients With Symptomatic COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 2292–2300. [Google Scholar] [CrossRef]
- Fu, Z.; Jiang, M.; Wang, K.; Li, J. Minimizing the impact of the COVID-19 epidemic on oncology clinical trials: A retrospective study of Beijing Cancer Hospital. J. Med. Internet. Res. 2021, 23, e26799. [Google Scholar] [CrossRef]
- Cummings, S.R. Clinical Trials Without Clinical Sites. JAMA Intern. Med. 2021, 181, 680–684. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 161,377) | PRE a (n = 59,478) | PAN (n = 101,899) | p-Value | SMD |
|---|---|---|---|---|---|
| Sponsor Class | - | - | - | <0.001 | 0.17 |
| • Federal | 8376 (5.2) | 2658 (4.5) | 5718 (5.6) | - | - |
| • Individual | 162 (0.1) | 83 (0.1) | 79 (0.1) | - | - |
| • Industry | 35,669 (22.1) | 15,797 (26.6) | 19,872 (19.5) | - | - |
| • Other | 117,170 (72.6) | 40,940 (68.8) | 76,230 (74.8) | - | - |
| Study Phase b | - | - | - | <0.001 | 0.02 |
| • Phase 1 and/or 2 | 49,421 (30.6) | 17,917 (30.1) | 31,504 (30.9) | - | - |
| • Phase 3 and/or 4 | 26,364 (16.3) | 9982 (16.8) | 16,382 (16.1) | - | - |
| • Not Applicable | 85,592 (53.0) | 31,579 (53.1) | 54,013 (53.0) | - | - |
| Intervention Type | - | - | - | <0.001 | 0.14 |
| • Device | 19,212 (11.9) | 7012 (11.8) | 12,200 (12.0) | - | - |
| • Diagnostic | 1976 (1.2) | 350 (0.6) | 1626 (1.6) | - | - |
| • Drug | 53,618 (33.2) | 20,682 (34.8) | 32,936 (32.3) | - | - |
| • Other | 74,082 (45.9) | 27,619 (46.4) | 46,463 (45.6) | - | - |
| • Procedure | 11,108 (6.9) | 3530 (5.9) | 7578 (7.4) | - | - |
| • Radiation | 1381 (0.9) | 285 (0.5) | 1096 (1.1) | - | - |
| Healthy Volunteers | - | - | - | <0.001 | 0.28 |
| • Accepted | 42,301 (26.2) | 18,589 (31.3) | 23,712 (23.3) | - | - |
| • Not Accepted | 119,076 (73.8) | 40,889 (68.7) | 78,187 (76.7) | - | - |
| Age group included | - | - | - | <0.001 | 0.04 |
| • Adults and Older Adults | 134,532 (83.4) | 49,742 (83.6) | 84,790 (83.2) | - | - |
| • Children Only | 10,029 (6.2) | 3913 (6.6) | 6116 (6.0) | - | - |
| • Children, Adults, and Older Adults | 16,816 (10.4) | 5823 (9.8) | 10,993 (10.8) | - | - |
| Continent | - | -- | - | <0.001 | 0.17 |
| • Africa | 5031 (3.1) | 1731 (2.9) | 3300 (3.2) | - | - |
| • Antarctica | 1 (0.0) | 0 (0.0) | 1 (0.0) | - | - |
| • Asia | 30,894 (19.1) | 9325 (15.7) | 21,569 (21.2) | - | - |
| • Europe | 34,409 (21.3) | 13,619 (22.9) | 20,790 (20.4) | - | - |
| • Multiple | 12,373 (7.7) | 4133 (6.9) | 8240 (8.1) | - | - |
| • North America | 59,701 (37.0) | 22,812 (38.4) | 36,889 (36.2) | - | - |
| • Oceania | 871 (0.5) | 332 (0.6) | 539 (0.5) | - | - |
| • South America | 3306 (2.0) | 1319 (2.2) | 1987 (1.9) | - | - |
| • Unknown | 14,791 (9.2) | 6207 (10.4) | 8584 (8.4) | - | - |
| Start Year | - | - | - | <0.001 | 1.19 |
| • Before 2015 | 39,968 (24.8) | 25,095 (42.2) | 14,873 (14.6) | - | - |
| • 2015 | 18,684 (11.6) | 10,835 (18.2) | 7849 (7.7) | - | - |
| • 2016 | 19,917 (12.3) | 9514 (16.0) | 10,403 (10.2) | - | - |
| • 2017 | 20,453 (12.7) | 7427 (12.5) | 13,026 (12.8) | - | - |
| • 2018 | 21,561 (13.4) | 4802 (8.1) | 16,759 (16.4) | - | - |
| • 2019 | 21,693 (13.4) | 1776 (3.0) | 19,917 (19.5) | - | - |
| • 2020 | 19,101 (11.8) | 29 (0.0) | 19,072 (18.7) | - | - |
| Month | Observed Trials (n°) | Forecasted Trials (n°) | 95% Confidence Interval | Difference (%) |
|---|---|---|---|---|
| Initiated Trials | ||||
| March 2020 | 1285 | 2079 | 1704–2454 | −38.2% |
| April 2020 | 765 | 1976 | 1585–2368 | −61.3% |
| May 2020 | 996 | 1974 | 1566–2382 | −49.5% |
| June 2020 | 1530 | 1970 | 1547–2394 | −22.3% |
| July 2020 | 1581 | 1922 | 1484–2361 | −17.7% |
| August 2020 | 1505 | 1913 | 1460–2366 | −21.3% |
| September 2020 | 2198 | 2111 | 1644–2578 | +4.1% |
| October 2020 | 2022 | 2227 | 1747–2708 | −9.2% |
| November 2020 | 1770 | 2042 | 1549–2536 | −13.3% |
| December 2020 | 1874 | 1818 | 1312–2325 | +3.1% |
| Completed Trials | ||||
| March 2020 | 1822 | 1451 | 1153–1749 | +25.6% |
| April 2020 | 1449 | 1462 | 1164–1761 | −0.9% |
| May 2020 | 1289 | 1583 | 1285–1882 | −18.6% |
| June 2020 | 1329 | 1362 | 1064–1661 | −2.4% |
| July 2020 | 1774 | 1498 | 1200–1797 | +18.4% |
| August 2020 | 1427 | 1821 | 1523–2120 | −21.6% |
| September 2020 | 1613 | 1465 | 1167–1764 | −10.1% |
| October 2020 | 1581 | 1700 | 1402–1999 | −7.1% |
| November 2020 | 1736 | 1453 | 1155–1752 | +19.5% |
| December 2020 | 1604 | 1407 | 1109–1706 | +14% |
| Stopped Trials | ||||
| March 2020 | 328 | 264 | 205–323 | +24.2 |
| April 2020 | 309 | 264 | 205–323 | +17.0 |
| May 2020 | 285 | 283 | 224–342 | +0.7 |
| June 2020 | 247 | 234 | 176–293 | +5.6 |
| July 2020 | 364 | 277 | 218–336 | +31.4 |
| August 2020 | 297 | 307 | 248–366 | −3.3 |
| September 2020 | 347 | 236 | 177–295 | +47.0 |
| October 2020 | 358 | 301 | 242–359 | +18.9 |
| November 2020 | 378 | 256 | 198–315 | +47.7 |
| December 2020 | 308 | 224 | 166–283 | +37.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Audisio, K.; Lia, H.; Robinson, N.B.; Rahouma, M.; Soletti, G.; Cancelli, G.; Perezgrovas Olaria, R.; Chadow, D.; Tam, D.Y.; Vervoort, D.; et al. Impact of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials. J. Cardiovasc. Dev. Dis. 2022, 9, 19. https://doi.org/10.3390/jcdd9010019
Audisio K, Lia H, Robinson NB, Rahouma M, Soletti G, Cancelli G, Perezgrovas Olaria R, Chadow D, Tam DY, Vervoort D, et al. Impact of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials. Journal of Cardiovascular Development and Disease. 2022; 9(1):19. https://doi.org/10.3390/jcdd9010019
Chicago/Turabian StyleAudisio, Katia, Hillary Lia, Newell Bryce Robinson, Mohamed Rahouma, Giovanni Soletti, Gianmarco Cancelli, Roberto Perezgrovas Olaria, David Chadow, Derrick Y. Tam, Dominique Vervoort, and et al. 2022. "Impact of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials" Journal of Cardiovascular Development and Disease 9, no. 1: 19. https://doi.org/10.3390/jcdd9010019
APA StyleAudisio, K., Lia, H., Robinson, N. B., Rahouma, M., Soletti, G., Cancelli, G., Perezgrovas Olaria, R., Chadow, D., Tam, D. Y., Vervoort, D., Farkouh, M. E., Bhatt, D. L., Fremes, S. E., & Gaudino, M. (2022). Impact of the COVID-19 Pandemic on Non-COVID-19 Clinical Trials. Journal of Cardiovascular Development and Disease, 9(1), 19. https://doi.org/10.3390/jcdd9010019