
One-Year Outcome of Patients Undergoing Transcatheter Aortic Valve Replacement with Concomitant SignificantTricuspid Regurgitation

 , , ,
, , ,  , and
, and
Abstract

1. Introduction
2. Methods
2.1. Study Design
2.2. Patient Selection
2.3. TAVR Procedures
2.4. Statistical Analysis
3. Results
3.1. Hospital Results and 30-Day Outcome
3.2. One-Year Outcome
3.3. Functional and Echocardiographic Changes over Time
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| CI | confidence intervals |
| CT-scan | computed tomography scan |
| HR | hazard ratios |
| IQR | interquartile range |
| LV | left ventricle |
| LVEF | left ventricular ejection fraction |
| MR | mitral regurgitation |
| NYHA | New York Heart Association |
| PCI | percutaneous coronary intervention |
| PM | pacemaker |
| SD | standard deviation |
| STS | Society of Thoracic Surgeons |
| TAVR | transcatheter aortic valve replacement |
| TR | tricuspid regurgitation |
References
- Little, S.H.; Popma, J.J.; Kleiman, N.S.; Deeb, G.M.; Gleason, T.G.; Yakubov, S.J.; Checuti, S.; O’Hair, D.; Bajwa, T.; Mumtaz, M.; et al. Transcatheter aortic valve replacement in patients with severe mitral or tricuspid regurgitation at extreme risk for surgery. J. Thorac. Cardiovasc. Surg. 2018, 155, 1991–1999. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Binder, R.K.; Dvir, D.; Tan, J.; Freeman, M.; Thompson, C.R.; Cheung, A.; Wood, D.A.; Leipsic, J.; Webb, J.G.; et al. Prevalence and impact of preoperative moderate/severe tricuspid regurgitation on patients undergoing transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2015, 85, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Amat-Santos, I.J.; Castrodeza, J.; Nombela-Franco, L.; Muñoz-García, A.J.; Gutiérrez-Ibanes, E.; Hernández, J.M.d.l.T.; Córdoba-Soriano, J.G.; Jiménez-Quevedo, P.; Hernández-García, J.M.; González-Mansilla, A.; et al. Tricuspid but not Mitral Regurgitation Determines Mortality After TAVI in Patients with Nonsevere Mitral Regurgitation. Rev. Esp. Cardiol. (Engl. Ed.) 2018, 71, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.P.; Bartko, P.E.; Krickl, A.; Gatterer, C.; Donà, C.; Nitsche, C.; Koschutnik, M.; Spinka, G.; Siller-Matula, J.M.; Lang, I.M.; et al. Adaptive development of concomitant secondary mitral and tricuspid regurgitation after transcatheter aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1045–1053. [Google Scholar] [CrossRef]
- Khan, F.; Okuno, T.; Malebranche, D.; Lanz, J.; Praz, F.; Stortecky, S.; Windecker, S.; Pilgrim, T. Transcatheter Aortic Valve Replacement in Patients with Multivalvular Heart Disease. JACC Cardiovasc. Interv. 2020, 13, 1503–1514. [Google Scholar] [CrossRef]
- Schubert, S.A.; Yarboro, L.T.; Madala, S.; Ayunipudi, K.; Kron, I.L.; Kern, J.A.; Ailawadi, G.; Stukenborg, G.J.; Ghanta, R.K. Natural history of coexistent mitral regurgitation after aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 1032–1039. [Google Scholar] [CrossRef]
- Rozenbaum, Z.; Granot, Y.; Steinvil, A.; Banai, S.; Finkelstein, A.; Ben-Gal, Y.; Ailawadi, G.; Stukenborg, G.J.; Ghanta, R.K. Aortic Stenosis with Severe Tricuspid Regurgitation: Comparative Study between Conservative Transcatheter Aortic Valve Replacement and Surgical Aortic Valve Replacement Combined With Tricuspid Repair. J. Am. Soc. Echocardiogr. 2018, 31, 1101–1108. [Google Scholar] [CrossRef]
- Cremer, P.C.; Wang, T.K.M.; Rodriguez, L.L.; Lindman, B.R.; Zhang, Y.; Zajarias, A.; Hahn, R.T.; Lerakis, S.; Malaisrie, S.C.; Douglas, P.S.; et al. PARTNER II Investigators. Incidence and Clinical Significance of Worsening Tricuspid Regurgitation Following Surgical or Transcatheter Aortic Valve Replacement: Analysis from the PARTNER IIA Trial. Circ. Cardiovasc. Interv. 2021, 14, e010437. [Google Scholar] [CrossRef]
- Sathananthan, J.; Murdoch, D.J.; Lindman, B.R.; Zajarias, A.; Jaber, W.A.; Cremer, P.; Wood, D.; Moss, R.; Cheung, A.; Ye, J.; et al. Implications of Concomitant Tricuspid Regurgitation in Patients Undergoing Transcatheter Aortic Valve Replacement for Degenerated Surgical Aortic Bioprosthesis: Insights from the PARTNER 2 Aortic Valve-in-Valve Registry. JACC Cardiovasc. Interv. 2018, 11, 1154–1160. [Google Scholar] [CrossRef]
- Purmah, Y.; Lei, L.Y.; Dykstra, S.; Mikami, Y.; Cornhill, A.; Satriano, A.; Seib, M.; Lydell, C.P. Right Ventricular Ejection Fraction for the Prediction of Major Adverse Cardiovascular and Heart Failure-Related Events: A Cardiac MRI Based Study of 7131 Patients with Known or Suspected Cardiovascular Disease. Circ. Cardiovasc. Imaging 2021, 14, e011337. [Google Scholar] [CrossRef]
- Myers, P.O.; Dayan, V.; Szeto, W.Y.; Thourani, V.H.; Malaisrie, S.C.; Moon, M.R.; Prager, R.L.; Ono, M.; Okita, Y.; Freemantle, N.; et al. Joint Surgical Associations (EACTS, LACES, ASCVTS, AATS, and STS) Position Statement Regarding the VARC-3 Definitions for Aortic Valve Clinical Research. Eur. J. Cardiothorac. Surg. 2022, 62, ezac110. [Google Scholar] [CrossRef] [PubMed]
- Prasitlumkum, N.; Kittipibul, V.; Tokavanich, N.; Kewcharoen, J.; Rattanawong, P.; Angsubhakorn, N.; Mao, M.A.; Gillaspie, E.A.; Cheungpasitporn, W. Baseline significant tricuspid regurgitation is associated with higher mortality in transcatheter aortic valve replacement: Systemic review and meta-analysis. J. Cardiovasc. Med. (Hagerstown) 2019, 20, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Liu, X.; Yu, L.; Sun, Y.; Jaiswal, S.; Zhu, Q.; Chen, H.; He, Y.; Wang, L.; Ren, K.; et al. Impact of tricuspid regurgitation and right ventricular dysfunction on outcomes after transcatheter aortic valve replacement: A systematic review and meta-analysis. Clin. Cardiol. 2019, 42, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.A.; Rozenbaum, Z.; Ghantous, E.; Kramarz, J.; Biner, S.; Ghermezi, M.; Shimiaie, J.; Finkelstein, A.; Banai, S.; Aviram, G.; et al. Impact of Right Ventricular Dysfunction and Tricuspid Regurgitation on Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Am. Soc. Echocardiogr. 2017, 30, 36–46. [Google Scholar] [CrossRef]
- Omar, S.; Aneni, E.; Escolar, E.; Mihos, C.G.; Xydas, S.; LaPietra, A.; Beohar, N.; Arenas, I.A. Tricuspid regurgitation and in-hospital outcomes after transcatheter aortic valve replacement in high-risk patients. J. Thorac. Dis. 2020, 12, 2963–2970. [Google Scholar] [CrossRef]
- Takagi, H.; Hari, Y.; Kawai, N.; Ando, T.; ALICE (All-Literature Investigation of Cardiovascular Evidence) Group. Impact of concurrent tricuspid regurgitation on mortality after transcatheter aortic-valve implantation. Catheter. Cardiovasc. Interv. 2019, 93, 946–953. [Google Scholar] [CrossRef]
- Barvalia, M.; Tayal, R.; Cohen, M.; Amor, M.M.; Tcharnaia, L.; Chen, C.; Russo, M.; Haik, B. Impact of Tricuspid Valve Regurgitation on Early Outcomes after Transcatheter Aortic Valve Replacement. J. Heart Valve Dis. 2017, 26, 380–385. [Google Scholar]
- McCarthy, F.H.; Vemulapalli, S.; Li, Z.; Thourani, V.; Matsouaka, R.A.; Desai, N.D.; Kirtane, A.; Anwaruddin, S.; Williams, M.L.; Giri, J.; et al. Association of Tricuspid Regurgitation with Transcatheter Aortic Valve Replacement Outcomes: A Report from The Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Ann. Thorac. Surg. 2018, 105, 1121–1128. [Google Scholar] [CrossRef]
- Tomii, D.; Okuno, T.; Praz, F.; Heg, D.; Wild, M.G.; Lanz, J.; Stortecky, S.; Reineke, D.; Windecker, S.; Pilgrim, T. Potential Candidates for Transcatheter Tricuspid Valve Intervention after Transcatheter Aortic Valve Replacement: Predictors and Prognosis. JACC Cardiovasc. Interv. 2021, 14, 2246–2256. [Google Scholar] [CrossRef]
- Granot, Y.; Merdler, I.; Finkelstein, A.; Arbel, Y.; Banai, S.; Topilsky, Y.; Scwartz, L.A.; Segev, A.; Barbash, I.; Fefer, P.; et al. Prognostic implication of right ventricular dysfunction and tricuspid regurgitation following transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2021, 98, e758–e767. [Google Scholar] [CrossRef]
- Worku, B.; Valovska, M.T.; Elmously, A.; Kampaktsis, P.; Castillo, C.; Wong, S.C.; Salemi, A. Predictors of Persistent Tricuspid Regurgitation After Transcatheter Aortic Valve Replacement in Patients with Baseline Tricuspid Regurgitation. Innovations 2018, 13, 190–199. [Google Scholar] [PubMed]
- Yoshida, J.; Ikenaga, H.; Hayashi, A.; Yamaguchi, S.; Nagaura, T.; Rader, F.; Siegel, R.J.; Makkar, R.R.; Shiota, T. Predictors and Outcomes of Persistent Tricuspid Regurgitation After Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2019, 124, 772–780. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Overall (n = 345) | TAVR-Low-Grade TR (n = 297) | TAVR-Significant TR (n = 48) | p-Value | |
|---|---|---|---|---|
| Age (years) | 82.6 ± 5.8 | 82.4 ± 5.7 | 83.8 ± 6.2 | 0.109 |
| Female gender | 168 (48.7) | 141 (47.5) | 27 (56.3) | 0.279 |
| Body mass index (kg/m2) | 26.5 ± 4.8 | 26.8 ± 4.8 | 24.6 ± 4.0 | 0.003 |
| Hypertension | 270 (78.3) | 233 (78.5) | 37 (77.1) | 0.851 |
| Diabetes | 100 (29.0) | 85 (28.6) | 15 (31.3) | 0.733 |
| Chronic kidney failure | 15 (4.3) | 14 (4.7) | 1 (2.1) | 0.704 |
| Dialysis | 11 (3.2) | 10 (3.4) | 1 (2.1) | 1.000 |
| COPD | 48 (13.9) | 42 (14.1) | 6 (12.5) | 1.000 |
| Cerebrovascular accident | 34 (9.9) | 28 (9.4) | 6 (12.5) | 0.446 |
| Peripheral artery disease | 106 (30.7) | 89 (30.0) | 17 (35.4) | 0.500 |
| NYHA III–IV | 245 (71.0) | 207 (69.7) | 38 (79.2) | 0.230 |
| NYHA class | 0.644 | |||
| I | 25 (7.3) | 23 (7.7) | 2 (4.2) | - |
| II | 75 (21.7) | 67 (22.6) | 8 (16.7) | - |
| III | 195 (56.5) | 164 (55.2) | 31 (64.6) | - |
| IV | 50 (14.5) | 43 (14.5) | 7 (14.6) | - |
| Coronary artery disease | 221 (64.0) | 193 (65.0) | 28 (58.3) | 0.418 |
| Myocardial infarction | 53 (15.4) | 42 (14.1) | 11 (22.9) | 0.131 |
| Previous PCI | 118 (34.2) | 104 (35.0) | 14 (29.2) | 0.513 |
| Atrial fibrillation | 102 (29.6) | 76 (25.6) | 26 (54.2) | <0.001 |
| Previous cardiac surgery | 49 (14.2) | 36 (12.1) | 13 (27.1) | 0.012 |
| Previous pacemaker | 43 (12.5) | 31 (10.4) | 12 (25.0) | 0.009 |
| Log. EuroSCORE-I (%) | 11.25 (IQR: 6.6–18.3) | 10.3 (IQR: 6.2–16.9) | 16.6 (IQR: 11.7–28.9) | <0.001 |
| EuroSCORE-II (%) | 3.4 (IQR: 2.1–6.2) | 3.2 (IQR: 1.9–5.7) | 5.6 (IQR: 3.7–8.1) | <0.001 |
| STS-score (%) | 4.3 (IQR: 2.6–7.2) | 4.1 (IQR: 2.5–7.1) | 5.4 (IQR: 3.4–8.5) | 0.011 |
| Echocardiographic data | ||||
| LVEF (%) | 59.0 (IQR: 45.0–62.0) | 60.0 (IQR: 47.0–62.0) | 55.0 (IQR: 38.0–60.0) | 0.064 |
| Aortic peak gradient (mmHg) | 70.0 (IQR: 56.0–84.0) | 70.0 (IQR: 59.0–85.0) | 66.0 (IQR: 45.0–81.0) | 0.159 |
| Aortic mean gradient (mmHg) | 43.0 (IQR: 36.0–53.0) | 43.0 (IQR: 37.0–53.0) | 42.0 (IQR: 28.0–52.0) | 0.279 |
| Aortic valve area (cm2) | 0.70 (IQR: 0.60–0.86) | 0.72 (IQR: 0.60–0.89) | 0.64 (IQR: 0.51–0.70) | 0.002 |
| LV mass (g) | 216.0 (IQR: 170.0–254.0) | 217.0 (IQR: 167.0–250.0) | 208.0 (IQR: 174.0–267.0) | 0.658 |
| Indexed LV mass (g/m2) | 121.0 (IQR: 102.0–142.0) | 120.0 (IQR: 100.5–241.0) | 129.0 (IQR: 117.0–151.0) | 0.060 |
| Impaired RV function (RVEF < 40%) | 19 (5.5) | 9 (3.0) | 10 (20.8) | <0.001 |
| Pulmonary hypertension (PASP ≥ 50 mmHg) | 46 (13.3) | 27 (9.1) | 19 (39.6) | <0.001 |
| Overall (n = 345) | TAVR-Low-Grade TR (n = 297) | TAVR-Significant TR (n = 48) | p-Value | |
|---|---|---|---|---|
| Mean TAVR valve size (mm) | 27.7 ± 2.9 | 27.7 ± 3.0 | 27.1 ± 2.3 | 0.219 |
| LOTUS valve | 17 (4.9) | 15 (5.1) | 2 (4.2) | - |
| Edwards SAPIEN | 2 (0.6) | 1 (0.3) | 1 (2.1) | - |
| Edwards SAPIEN-XT | 6 (1.7) | 6 (2.0) | 0 | - |
| Edwards SAPIEN-3 | 75 (21.7) | 63 (21.2) | 12 (25.0) | - |
| Edwards SAPIEN-3 ULTRA | 3 (0.9) | 2 (0.7) | 1 (2.1) | - |
| Medtronic CoreValve | 70 (20.3) | 57 (19.2) | 13 (27.1) | - |
| Medtronic CoreValve Evolut PRO | 2 (0.6) | 1 (0.3) | 1 (2.1) | - |
| Medtronic CoreValve Evolut R | 141 (40.9) | 127 (42.8) | 14 (29.3) | - |
| St. Jude Medical PORTICO | 4 (1.2) | 3 (1.0) | 1 (2.1) | - |
| Boston Scientific ACURATE | 25 (7.2) | 22 (7.4) | 3 (6.3) | - |
Vascular access: - Transfemoral - Transaortic - Trans-subclavian - Trans-carotid | 304 (88.1) 36 (10.4) 3 (0.9) 2 (0.6) | 262 (88.2) 30 (10.1) 3 (1.0) 2 (0.7) | 42 (87.5) 6 (12.5) 0 0 | 0.914 |
| Use of vascular closure device | 265 (76.8) | 227 (76.4) | 38 (79.2) | 0.309 |
| Use of embolic protection device | 13 (3.8) | 10 (3.4) | 3 (6.3) | 0.403 |
| Balloon diameter for BAV (n = 338) (mm) | 21.6 ± 2.2 | 21.6 ± 2.2 | 21.4 ± 2.3 | 0.655 |
| Contrast (mL) | 285.3 ± 132.1 | 288.0 ± 134.7 | 268.4 ± 114.2 | 0.423 |
| Procedural time (min) | 104.4 ± 46.3 | 104.8 ± 47.0 | 102.4 ± 41.3 | 0.709 |
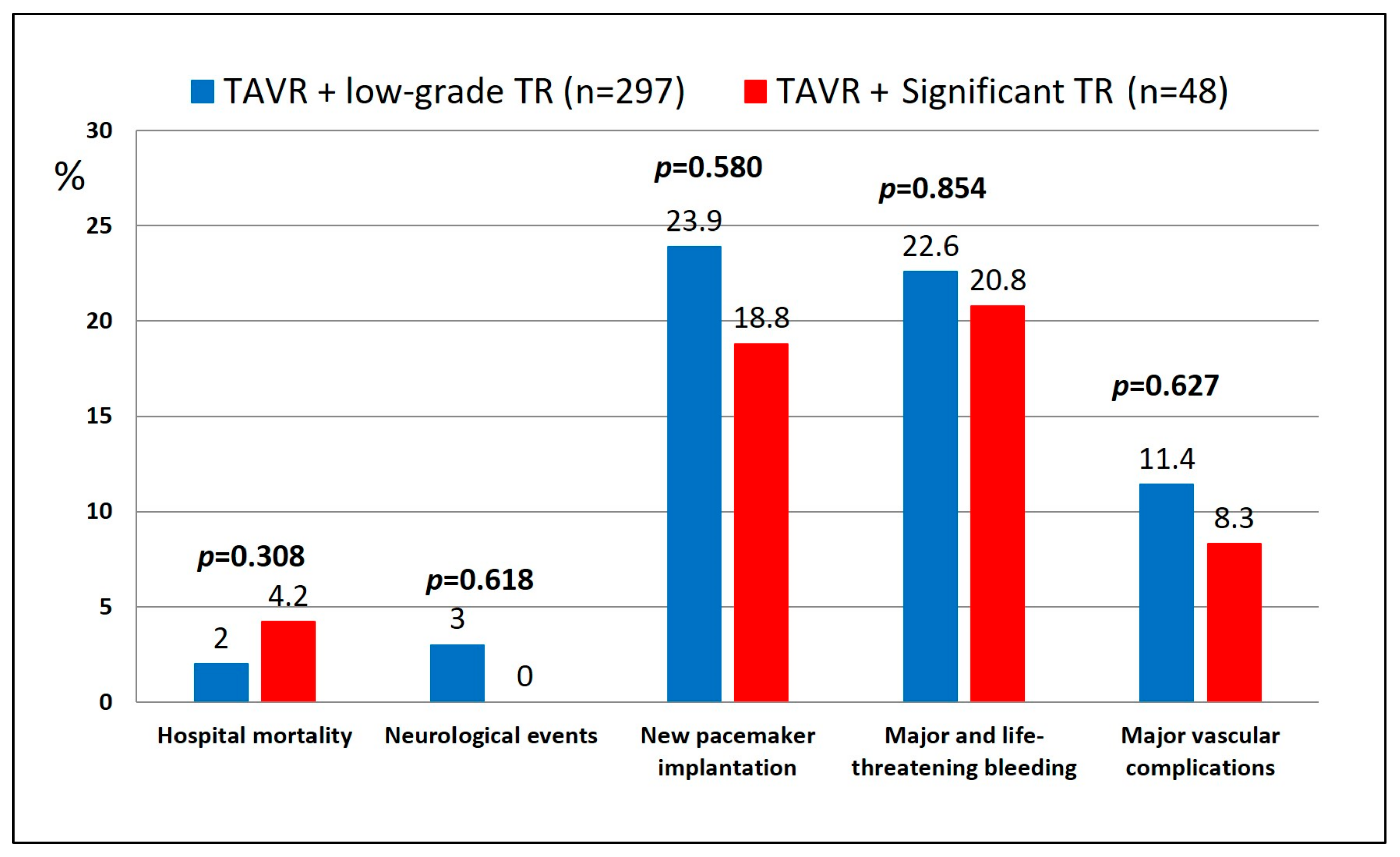
| 30-Day Outcomes | Overall (n = 345) | TAVR-Low-Grade TR (n = 297) | TAVR-Significant TR (n = 48) | p-Value |
|---|---|---|---|---|
| Valve dislocation/embolisation | 5 (1.4) | 4 (1.3) | 1 (2.1) | 0.529 |
| Major vascular complications | 38 (11.0) | 34 (11.4) | 4 (8.3) | 0.627 |
| Major and life-threatening bleeding | 77 (22.3) | 67 (22.6) | 10 (20.8) | 0.854 |
| Median red blood transfusions (bags) | 0 (IQR: 0.0–2.0) | 0 (IQR:0.0–2.0) | 0 (IQR: 0.0–1.0) | 0.555 |
| New PCI (coronary occlusion) | 1 (0.3) | 1 (0.3) | 0 | 1.000 |
| New pacemaker implantation | 80 (23.2) | 71 (23.9) | 9 (18.8) | 0.580 |
| Acute kidney injury | 15 (4.3) | 13 (4.4) | 2 (4.2) | 1.000 |
| Neurological events | 9 (2.6) | 9 (3.0) | 0 | 0.618 |
| New onset of atrial fibrillation | 32 (12.7) | 20 (9.3) | 12 (32.4) | <0.001 |
| ICU stay (days) | 1.0 (IQR: 1.0–3.0) | 1.0 (IQR: 1.0–2.0) | 1.5 (IQR: 1.0–3.0) | 0.436 |
| Hospital stay (days) | 6.0 (IQR: 4.0–8.0) | 6.0 (IQR: 4.0–8.0) | 6.0 (IQR: 4.0–8.0) | 0.659 |
| NYHA III–IV | 12 (3.5) | 8 (2.7) | 4 (8.3) | 0.069 |
In-hospital mortality - Multiple organ failure - Myocardial infarction - Cardiac tamponade - Cardiogenic shock - Haemoptysis for gastric cancer | 8 (2.3) 2 (0.6) 1 (0.3) 2 (0.6) 2 (0.6) 1 (0.3) | 6 (2.0) 0 1 (0.3) 2 (0.7) 2 (0.7) 1 (0.3) | 2 (4.2) 2 (4.2) 0 0 0 0 | 0.308 |
30-day mortality (including in hospital) - Multiple organ failure - Myocardial infarction - Cardiac tamponade - Cardiogenic shock - Sudden death - Respiratory failure - Aortic root rupture - Haemoptysis for gastric cancer | 15 (4.3) 3 (0.9) 2 (0.6) 2 (0.6) 4 (1.2) 1 (0.3) 1 (0.3) 1 (0.3) 1 (0.3) | 12 (4.0) 0 2 (0.7) 2 (0.7) 4 (1.4) 1 (0.3) 1 (0.3) 1 (0.3) 1 (0.3) | 3 (6.3) 3 (6.3) 0 0 0 0 0 0 0 | 0.070 |
| Re-hospitalisation for heart failure | 40 (11.6) | 33 (11.1) | 7 (14.6) | 0.470 |
| 1-year outcomes | Overall (n = 337) | TAVR-low-grade TR (n = 291) | TAVR-Significant TR (n = 46) | p-value |
| New PCI | 2 (0.6) | 2 (0.7) | 0 | 0.734 |
| New pacemaker implantation | 2 (0.6) | 2 (0.7) | 0 | 1.000 |
| Re-hospitalisation for heart failure | 57 (16.9) | 48 (16.5) | 9 (19.6) | 0.713 |
| NYHA Class | 0.331 | |||
| NYHA Class I | 91 (27.0) | 79 (27.1) | 12 (26.1) | - |
| NYHA Class II | 143 (42.4) | 124 (42.6) | 19 (41.3) | - |
| NYHA Class III | 9 (2.7) | 6 (2.1) | 3 (6.5) | - |
| NYHA Class IV | 1 (0.3) | 1 (0.3) | 0 | - |
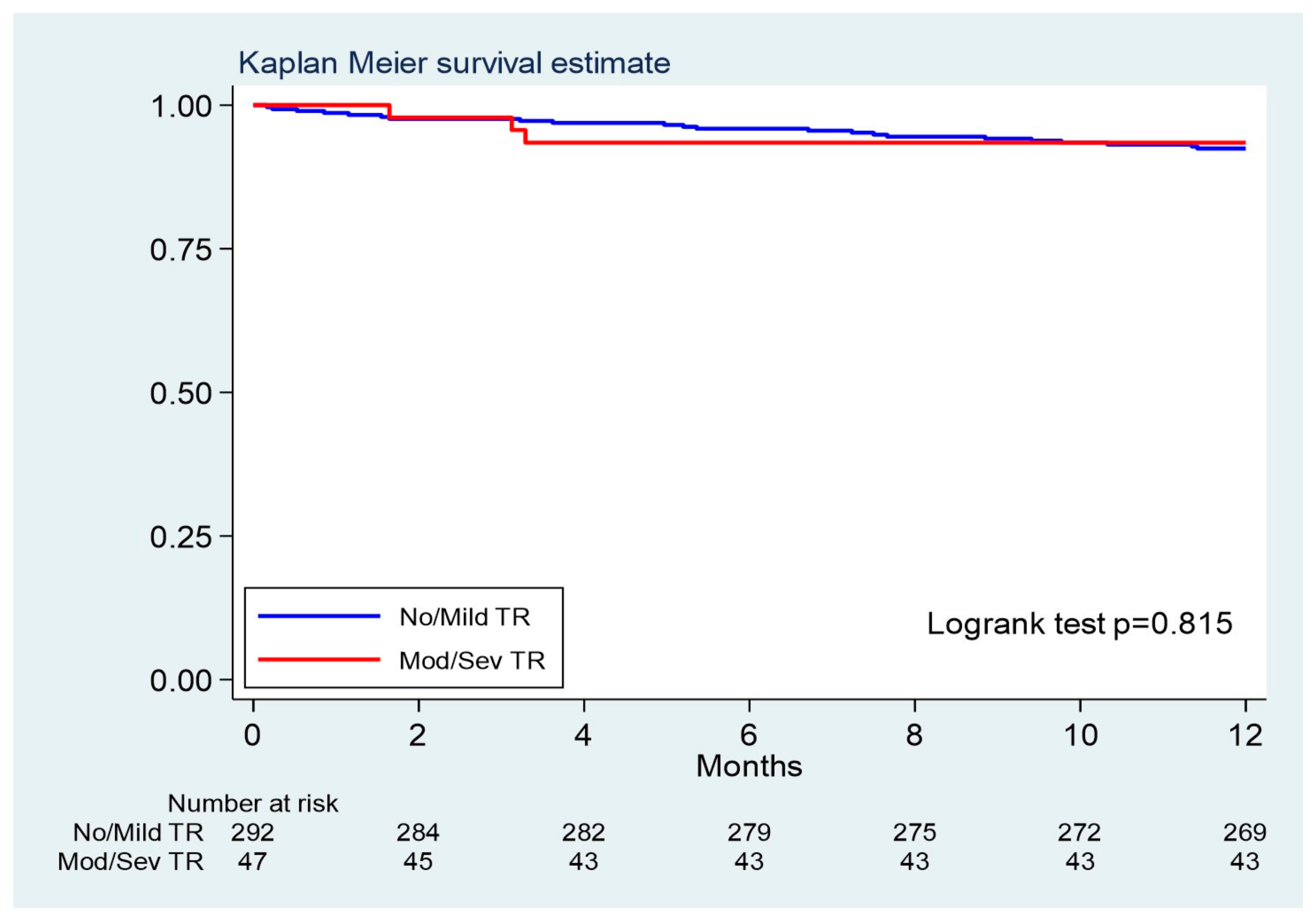
1-year mortality * Number of deaths Rate per 100 person year (95% CI) - Malignancy - Sepsis - Multiple organ failure - Myocardial infarction - Cardiogenic shock - Pulmonary embolism - Pneumonia - Cardiac arrest - Haemorrhagic stroke - Respiratory failure - Aortic root rupture - Sudden death - Unknown | 26 (7.7) 8.1 (5.5–11.8) 5 (1.5) 3 (0.9) 2 (0.6) 2 (0.6) 2 (0.6) 2 (0.6) 2 (0.6) 1 (0.3) 1 (0.3) 1 (0.3) 1 (0.3) 1 (0.3) 3 (0.9) | 22 (7.6) 7.9 (5.2–12.0) 5 (1.7) 3 (1.0) 0 2 (0.7) 2 (0.7) 2 (0.7) 1 (0.4) 0 1 (0.3) 1 (0.3) 1 (0.3) 1 (0.3) 3 (1.0) | 4 (8.7) 9.1 (3.4–24.3) 0 0 2 (4.3) 0 0 0 1 (2.2) 1 (2.2) 0 0 0 0 0 | 0.815 ** |
| Change over Time | Post Hoc Comparisons | Difference Between TR Time Profiles | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Preoperative (n = 345) | Discharge (n = 337) | 30 Days (n = 330) | 1-Year Follow-Up (n = 311) | Overall p-Value # | Discharge vs. Preoperative | 30 Days vs. Discharge | 1 Year vs. 30 Days | * p for Interaction | |
| LVEF (%) | 53.4 ± 12.6 | 54.2 ± 11.5 | 55.2 ± 10.6 | 55.6 ± 9.7 | <0.001 | 0.090 | 0.004 | 0.467 | 0.482 |
| Aortic peak gradient (mmHg) | 71.4 ± 23.5 | 15.6 ± 7.4 | 16.2 ± 8.7 | 16.5 ± 11.2 | <0.001 | <0.001 | 0.231 | 0.724 | 0.836 |
| Aortic mean gradient (mmHg) | 44.7 ± 15.4 | 8.4 ± 4.1 | 8.8 ± 4.9 | 9.2 ± 7.0 | <0.001 | <0.001 | 0.154 | 0.421 | 0.925 |
| Aortic orifice area (cm2) | 0.7 ± 0.2 | N.A. | N.A. | N.A. | |||||
| LV mass (g) | 216.7 ± 72.3 | 210.4 ± 63.0 | 204.5 ± 67.6 | 195.0 ± 61.5 | 0.008 | 0.133 | 0.264 | 0.200 | 0.389 |
| Indexed LV mass (g/m2) | 123.8 ± 34.5 | 122.8 ± 42.5 | 115.8 ± 35.3 | 110.7 ± 31.4 | <0.001 | 0.678 | 0.011 | 0.181 | 0.392 |
| LVEDD (mm) | 47.0 ± 8.0 | 46.8 ± 7.9 | 47.8 ± 8.3 | 46.6 ± 7.8 | 0.352 | 0.719 | 0.097 | 0.118 | 0.435 |
| LVESD (mm) | 33.8 ± 14.9 | 32.5 ± 15.2 | 32.1 ± 7.6 | 31.7 ± 8.0 | 0.046 | 0.023 | 0.672 | 0.521 | 0.176 |
| Impaired RV function (RVEF < 40%) | 19 (5.5) | 17 (5.0) | 6 (1.8) | 3 (0.9) | 0.082 | 0.744 | 0.078 | 0.342 | 0.407 |
| Pulmonary hypertension (PASP ≥ 50 mmHg) | 46 (13.3) | 25 (7.4) | 15 (4.5) | 6 (1.9) | <0.001 | 0.002 | 0.545 | 0.085 | 0.398 |
| Significant tricuspid regurgitation | 48 (13.9) | 48 (14.2) | 38 (11.5) | 29 (9.3) | 0.055 | 0.818 | 0.102 | 0.284 | 0.509 |
| NYHA III–IV | 245 (71.0) | - | 12 (4.2) | 10 (3.2) | <0.001 | - | - | 0.962 | 0.564 |
| Change over Time | Post Hoc Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|
| Pre-Operative | Discharge | 30 Days | 1 Year Follow-Up | Overall p-Value | Discharge vs. Preoperative | Overall p-Value | Discharge vs. Preoperative | |
Significant Tricuspid regurgitation - Low-grade (0–1+) - Significant (2–4+) | 0 (0%) 48 (100%) | 16 (5%) 33 (69%) | 13 (5%) 25 (56%) | 10 (4%) 30 (45%) | 0.573 0.027 | 0.573 0.027 | ||
LVEF (%) - Low-grade TR group - Significant TR group | 53.9 ± 12.5 50.3 ± 11.9 | 54.4 ± 11.3 51.9 ± 12.7 | 55.5 ± 10.4 52.7 ± 11.8 | 55.7 ± 9.6 54.2 ± 11.2 | 0.005 0.040 | 0.235 0.080 | 0.005 0.040 | 0.235 0.080 |
Aortic peak gradient (mmHg) - Low-grade TR group - Significant TR group | 71.8 ± 22.7 68.8 ± 28.2 | 15.5 ± 7.2 16.1 ± 8.7 | 16.2 ± 8.2 16.4 ± 11.7 | 16.4 ± 10.7 17.3 ± 14.9 | <0.001 <0.001 | <0.001 <0.001 | <0.001 <0.001 | <0.001 <0.001 |
Aortic mean gradient (mmHg) - Low-grade TR group - Significant TR group | 44.8 ± 14.7 43.9 ± 19.0 | 8.5 ± 4.0 8.2 ± 4.7 | 8.8 ± 4.6 9.1 ± 6.7 | 9.1 ± 6.8 9.4 ± 8.4 | <0.001 <90.001 | <0.001 <0.001 | <0.001 <90.001 | <0.001 <0.001 |
LV mass (g) - Low-grade TR group - Significant TR group | 214 ± 66 231 ± 102 | 209 ± 61 220 ± 80 | 200 ± 63 241 ± 95 | 192 ± 57 206 ± 80 | 0.011 0.267 | 0.256 0.357 | 0.011 0.267 | 0.256 0.357 |
Indexed LV mass (g/m2) - Low-grade TR group - Significant TR group | 122 ± 33 135 ± 43 | 122 ± 43 127 ± 40 | 114 ± 34 130 ± 44 | 108 ± 30 123 ± 35 | <0.001 0.299 | 0.899 0.182 | <0.001 0.299 | 0.899 0.182 |
LVEDD (mm) - Low-grade TR group - Significant TR group | 47.0 ± 7.7 46.9 ± 9.9 | 46.7 ± 7.9 47.3 ± 8.0 | 48.0 ± 7.9 46.2 ± 10.4 | 46.3 ± 7.0 48.0 ± 11.3 | 0.109 0.847 | 0.564 0.691 | 0.109 0.847 | 0.564 0.691 |
LVESD (mm) - Low-grade TR group - Significant TR group | 33.5 ± 15.3 35.5 ± 12.2 | 32.5 ± 15.8 32.3 ± 10.1 | 31.9 ± 7.2 33.6 ± 9.7 | 31.1 ± 6.8 34.5 ± 12.1 | 0.101 0.056 | 0.115 0.012 | 0.101 0.056 | 0.115 0.012 |
Impaired RV function (RVEF < 40%) - Low-grade TR group - Significant TR group | 9 (3.1%) 10 (21.3%) | 7 (2.5%) 10 (23.3%) | 1 (0.5%) 5 (15.1%) | 0 (0%) 3 (10.3%) | 0.209 0.295 | 0.557 0.649 | 0.209 0.295 | 0.557 0.649 |
Pulmonary hypertension (PASP ≥ 50 mmHg) - Low-grade TR group - Significant TR group | 27 (9.3%) 19 (40.4%) | 14 (4.9%) 11 (24.4%) | 9 (4.5%) 6 (18.2%) | 5 (3.0%) 1 (3.4%) | 0.009 0.004 | 0.018 0.061 | 0.009 0.004 | 0.018 0.061 |
NYHA III-IV - Low-grade TR group - Significant TR group | 207 (70%) 38 (79%) | NA NA | 8 (3%) 4 (10%) | 7 (3%) 3 (9%) | <0.001 <0.001 | NA NA | <0.001 <0.001 | NA NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrari, E.; Pozzoli, A.; Klersy, C.; Caporali, E.; Demertzis, S.; Pedrazzini, G. One-Year Outcome of Patients Undergoing Transcatheter Aortic Valve Replacement with Concomitant SignificantTricuspid Regurgitation. J. Cardiovasc. Dev. Dis. 2025, 12, 184. https://doi.org/10.3390/jcdd12050184
Ferrari E, Pozzoli A, Klersy C, Caporali E, Demertzis S, Pedrazzini G. One-Year Outcome of Patients Undergoing Transcatheter Aortic Valve Replacement with Concomitant SignificantTricuspid Regurgitation. Journal of Cardiovascular Development and Disease. 2025; 12(5):184. https://doi.org/10.3390/jcdd12050184
Chicago/Turabian StyleFerrari, Enrico, Alberto Pozzoli, Catherine Klersy, Elena Caporali, Stefanos Demertzis, and Giovanni Pedrazzini. 2025. "One-Year Outcome of Patients Undergoing Transcatheter Aortic Valve Replacement with Concomitant SignificantTricuspid Regurgitation" Journal of Cardiovascular Development and Disease 12, no. 5: 184. https://doi.org/10.3390/jcdd12050184
APA StyleFerrari, E., Pozzoli, A., Klersy, C., Caporali, E., Demertzis, S., & Pedrazzini, G. (2025). One-Year Outcome of Patients Undergoing Transcatheter Aortic Valve Replacement with Concomitant SignificantTricuspid Regurgitation. Journal of Cardiovascular Development and Disease, 12(5), 184. https://doi.org/10.3390/jcdd12050184