
Endurance Training Exercise Dose in Coronary Artery Disease Rehabilitation


Abstract
1. Introduction
2. Exercise Prescription
3. Lessons from the STRRIDE Study: The Importance of Exercise Dose
4. Exercise Dose Response for the Secondary Prevention of CAD
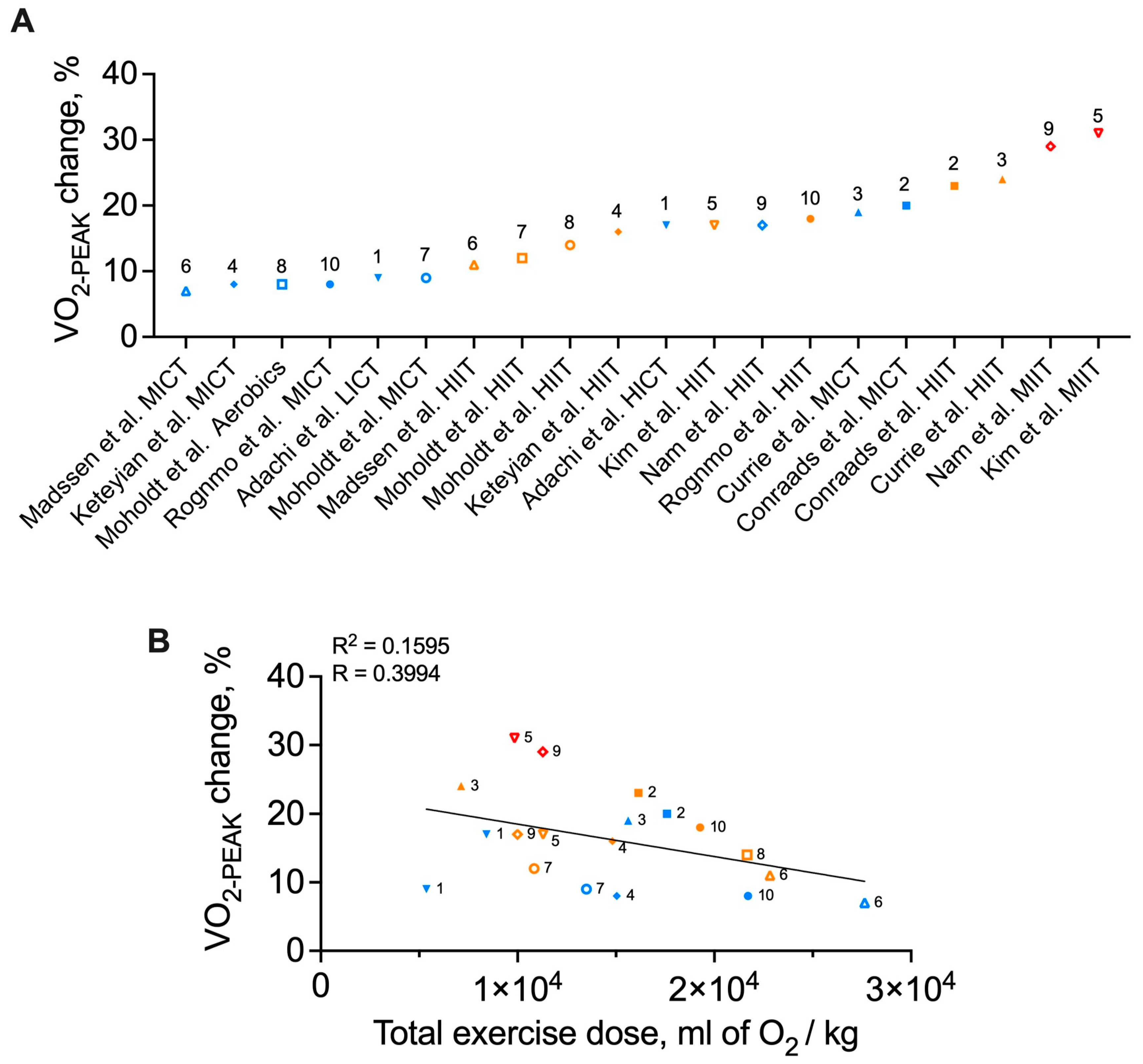
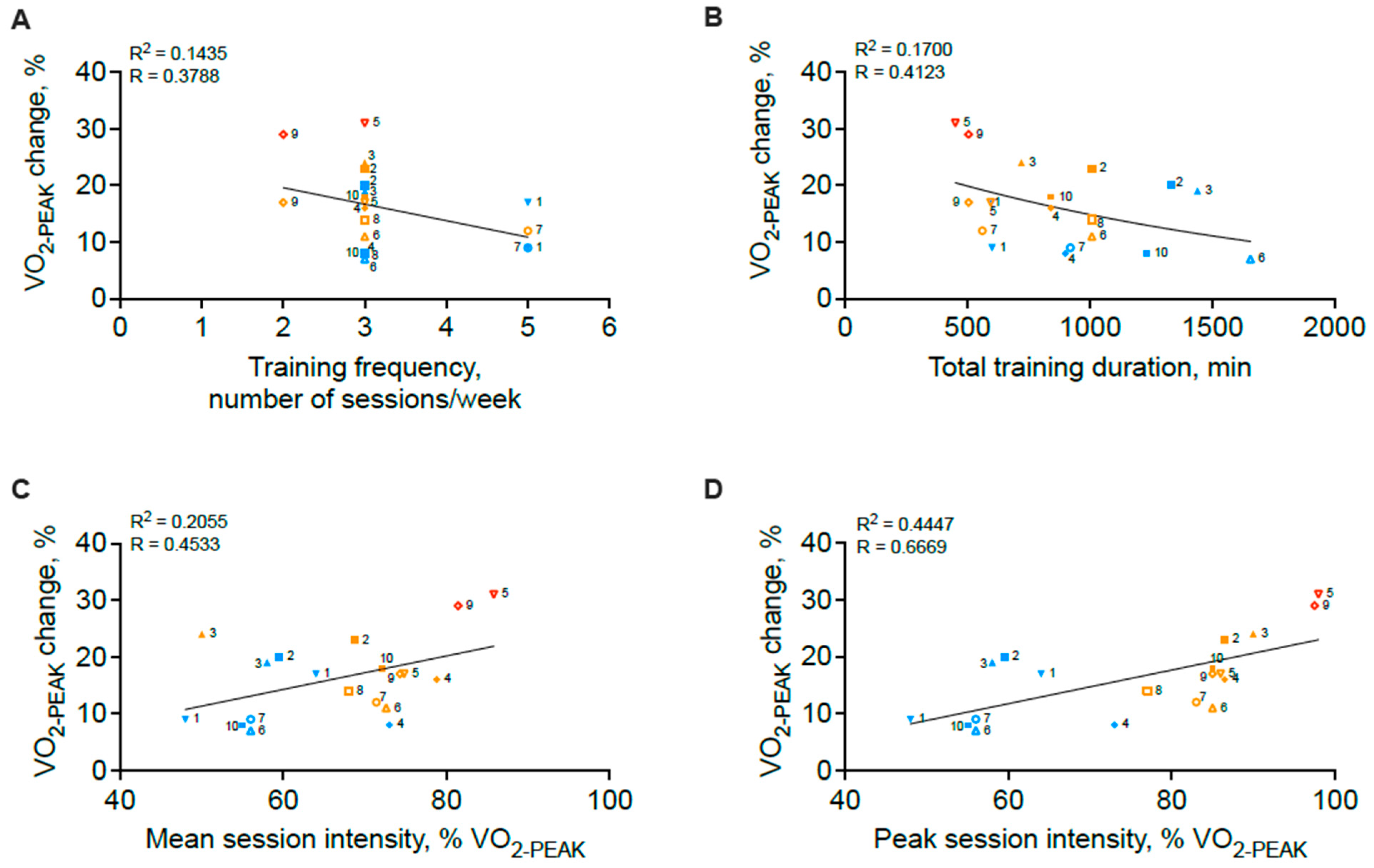
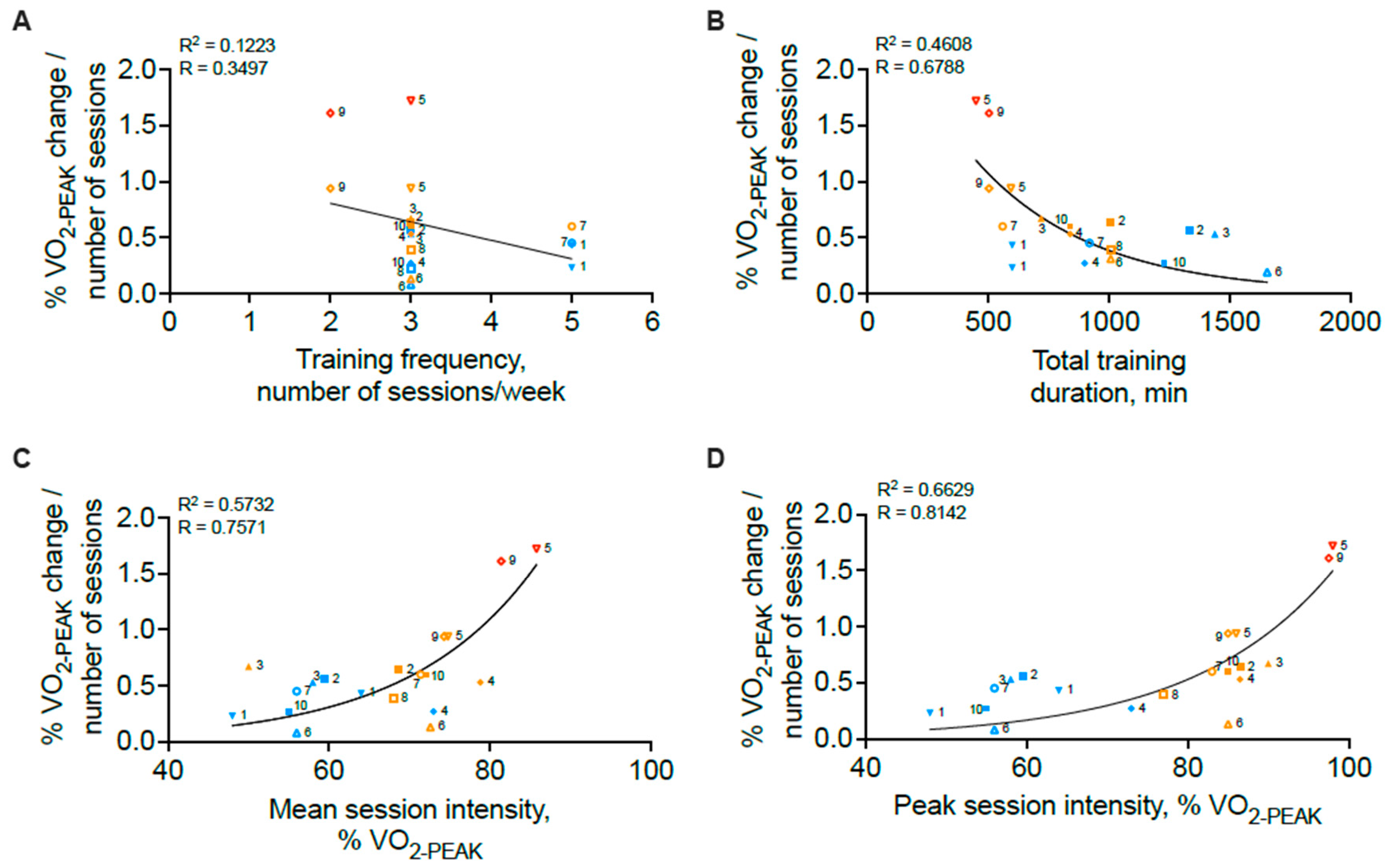
4.1. Exercise Dose and Cardiorespiratory Fitness
4.2. Beyond : Cardiac Risk Factors and Quality of Life
5. Methodological Limitations to Consider
6. Future Directions
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 18 October 2024).
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics-2022 Update: A Report from the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur. Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients with Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2023, 148, e9–e119. [Google Scholar] [CrossRef] [PubMed]
- Herold, F.; Muller, P.; Gronwald, T.; Muller, N.G. Dose-Response Matters!—A Perspective on the Exercise Prescription in Exercise-Cognition Research. Front. Psychol. 2019, 10, 2338. [Google Scholar] [CrossRef] [PubMed]
- Wasfy, M.M.; Baggish, A.L. Exercise Dose in Clinical Practice. Circulation 2016, 133, 2297–2313. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008; Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef]
- Brown, T.M.; Pack, Q.R.; Aberegg, E.; Brewer, L.C.; Ford, Y.R.; Forman, D.E.; Gathright, E.C.; Khadanga, S.; Ozemek, C.; Thomas, R.J.; et al. Core Components of Cardiac Rehabilitation Programs: 2024 Update: A Scientific Statement from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2024, 150, e328–e347. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corra, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.E.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [PubMed]
- Verdicchio, C.; Freene, N.; Hollings, M.; Maiorana, A.; Briffa, T.; Gallagher, R.; Hendriks, J.M.; Abell, B.; Brown, A.; Colquhoun, D.; et al. A Clinical Guide for Assessment and Prescription of Exercise and Physical Activity in Cardiac Rehabilitation. A CSANZ Position Statement. Heart Lung Circ. 2023, 32, 1035–1048. [Google Scholar] [CrossRef]
- Kraus, W.E.; Torgan, C.E.; Duscha, B.D.; Norris, J.; Brown, S.A.; Cobb, F.R.; Bales, C.W.; Annex, B.H.; Samsa, G.P.; Houmard, J.A.; et al. Studies of a targeted risk reduction intervention through defined exercise (STRRIDE). Med. Sci. Sports Exerc. 2001, 33, 1774–1784. [Google Scholar] [CrossRef]
- Krauss, R.M. Is the size of low-density lipoprotein particles related to the risk of coronary heart disease? JAMA 2002, 287, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Duscha, B.D.; Slentz, C.A.; Johnson, J.L.; Houmard, J.A.; Bensimhon, D.R.; Knetzger, K.J.; Kraus, W.E. Effects of exercise training amount and intensity on peak oxygen consumption in middle-age men and women at risk for cardiovascular disease. Chest 2005, 128, 2788–2793. [Google Scholar] [CrossRef] [PubMed]
- Slentz, C.A.; Duscha, B.D.; Johnson, J.L.; Ketchum, K.; Aiken, L.B.; Samsa, G.P.; Houmard, J.A.; Bales, C.W.; Kraus, W.E. Effects of the amount of exercise on body weight, body composition, and measures of central obesity: STRRIDE--a randomized controlled study. Arch. Intern. Med. 2004, 164, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Houmard, J.A.; Tanner, C.J.; Slentz, C.A.; Duscha, B.D.; McCartney, J.S.; Kraus, W.E. Effect of the volume and intensity of exercise training on insulin sensitivity. J. Appl. Physiol. 2004, 96, 101–106. [Google Scholar] [CrossRef]
- Slentz, C.A.; Aiken, L.B.; Houmard, J.A.; Bales, C.W.; Johnson, J.L.; Tanner, C.J.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise, and visceral fat. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2005, 99, 1613–1618. [Google Scholar] [CrossRef]
- Slentz, C.A.; Houmard, J.A.; Johnson, J.L.; Bateman, L.A.; Tanner, C.J.; McCartney, J.S.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2007, 103, 432–442. [Google Scholar] [CrossRef]
- Adachi, H.; Koike, A.; Obayashi, T.; Umezawa, S.; Aonuma, K.; Inada, M.; Korenaga, M.; Niwa, A.; Marumo, F.; Hiroe, M. Does appropriate endurance exercise training improve cardiac function in patients with prior myocardial infarction? Eur. Heart J. 1996, 17, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Conraads, V.M.; Pattyn, N.; De Maeyer, C.; Beckers, P.J.; Coeckelberghs, E.; Cornelissen, V.A.; Denollet, J.; Frederix, G.; Goetschalckx, K.; Hoymans, V.Y.; et al. Aerobic interval training and continuous training equally improve aerobic exercise capacity in patients with coronary artery disease: The SAINTEX-CAD study. Int. J. Cardiol. 2015, 179, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Currie, K.D.; Dubberley, J.B.; McKelvie, R.S.; MacDonald, M.J. Low-volume, high-intensity interval training in patients with CAD. Med. Sci. Sports Exerc. 2013, 45, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Keteyian, S.J.; Hibner, B.A.; Bronsteen, K.; Kerrigan, D.; Aldred, H.A.; Reasons, L.M.; Saval, M.A.; Brawner, C.A.; Schairer, J.R.; Thompson, T.M.; et al. Greater improvement in cardiorespiratory fitness using higher-intensity interval training in the standard cardiac rehabilitation setting. J. Cardiopulm. Rehabil. Prev. 2014, 34, 98–105. [Google Scholar] [CrossRef]
- Kim, C.; Choi, H.E. The Effect and Safety of Aerobic Interval Training According to Exercise Intensity in Acute Coronary Syndrome. J. Cardiopulm. Rehabil. Prev. 2020, 40, 178–182. [Google Scholar] [CrossRef]
- Madssen, E.; Moholdt, T.; Videm, V.; Wisloff, U.; Hegbom, K.; Wiseth, R. Coronary atheroma regression and plaque characteristics assessed by grayscale and radiofrequency intravascular ultrasound after aerobic exercise. Am. J. Cardiol. 2014, 114, 1504–1511. [Google Scholar] [CrossRef] [PubMed]
- Moholdt, T.T.; Amundsen, B.H.; Rustad, L.A.; Wahba, A.; Lovo, K.T.; Gullikstad, L.R.; Bye, A.; Skogvoll, E.; Wisloff, U.; Slordahl, S.A. Aerobic interval training versus continuous moderate exercise after coronary artery bypass surgery: A randomized study of cardiovascular effects and quality of life. Am. Heart J. 2009, 158, 1031–1037. [Google Scholar] [CrossRef] [PubMed]
- Moholdt, T.; Aamot, I.L.; Granoien, I.; Gjerde, L.; Myklebust, G.; Walderhaug, L.; Brattbakk, L.; Hole, T.; Graven, T.; Stolen, T.O.; et al. Aerobic interval training increases peak oxygen uptake more than usual care exercise training in myocardial infarction patients: A randomized controlled study. Clin. Rehabil. 2012, 26, 33–44. [Google Scholar] [CrossRef]
- Nam, H.; Jeon, H.E.; Kim, W.H.; Joa, K.L.; Lee, H. Effect of maximal-intensity and high-intensity interval training on exercise capacity and quality of life in patients with acute myocardial infarction: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2024, 60, 104–112. [Google Scholar] [CrossRef]
- Rognmo, O.; Hetland, E.; Helgerud, J.; Hoff, J.; Slordahl, S.A. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Kavanagh, T.; Mertens, D.J.; Hamm, L.F.; Beyene, J.; Kennedy, J.; Corey, P.; Shephard, R.J. Peak Oxygen Intake and Cardiac Mortality in Women Referred for Cardiac Rehabilitation. J. Am. Coll. Cardiol. 2003, 42, 2139–2143. [Google Scholar] [CrossRef]
- Kavanagh, T.; Mertens, D.J.; Hamm, L.F.; Beyene, J.; Kennedy, J.; Corey, P.; Shephard, R.J. Prediction of long-term prognosis in 12 169 men referred for cardiac rehabilitation. Circulation 2002, 106, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Rognmo, O.; Moholdt, T.; Bakken, H.; Hole, T.; Molstad, P.; Myhr, N.E.; Grimsmo, J.; Wisloff, U. Cardiovascular risk of high- versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 2012, 126, 1436–1440. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Ahn, D.; Yu, J.; Liou, K.; Keech, A. High-Intensity Interval Training for Patients with Cardiovascular Disease—Is It Safe? A Systematic Review. J. Am. Heart Assoc. 2018, 7, e009305. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, F.D.; Whelton, P.K. High Blood Pressure and Cardiovascular Disease. Hypertension 2020, 75, 285–292. [Google Scholar] [CrossRef]
- Hansen, D.; Bonne, K.; Alders, T.; Hermans, A.; Copermans, K.; Swinnen, H.; Maris, V.; Jansegers, T.; Mathijs, W.; Haenen, L.; et al. Exercise training intensity determination in cardiovascular rehabilitation: Should the guidelines be reconsidered? Eur. J. Prev. Cardiol. 2019, 26, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Milani, J.; Milani, M.; Verboven, K.; Cipriano, G., Jr.; Hansen, D. Exercise intensity prescription in cardiovascular rehabilitation: Bridging the gap between best evidence and clinical practice. Front. Cardiovasc. Med. 2024, 11, 1380639. [Google Scholar] [CrossRef] [PubMed]
- Pattyn, N.; Beulque, R.; Cornelissen, V. Aerobic Interval vs. Continuous Training in Patients with Coronary Artery Disease or Heart Failure: An Updated Systematic Review and Meta-Analysis with a Focus on Secondary Outcomes. Sports Med. 2018, 48, 1189–1205. [Google Scholar] [CrossRef]
- Uddin, J.; Zwisler, A.D.; Lewinter, C.; Moniruzzaman, M.; Lund, K.; Tang, L.H.; Taylor, R.S. Predictors of exercise capacity following exercise-based rehabilitation in patients with coronary heart disease and heart failure: A meta-regression analysis. Eur. J. Prev. Cardiol. 2016, 23, 683–693. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Yan, X.; Cai, X.; Li, J. Effects of High-Intensity Interval Training on Aerobic Capacity in Cardiac Patients: A Systematic Review with Meta-Analysis. Biomed Res. Int. 2017, 2017, 5420840. [Google Scholar] [CrossRef]
- Liou, K.; Ho, S.; Fildes, J.; Ooi, S.Y. High Intensity Interval versus Moderate Intensity Continuous Training in Patients with Coronary Artery Disease: A Meta-analysis of Physiological and Clinical Parameters. Heart Lung Circ. 2016, 25, 166–174. [Google Scholar] [CrossRef]
- Elliott, A.D.; Rajopadhyaya, K.; Bentley, D.J.; Beltrame, J.F.; Aromataris, E.C. Interval training versus continuous exercise in patients with coronary artery disease: A meta-analysis. Heart Lung Circ. 2015, 24, 149–157. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| (Study #)/Author/Reference | Inclusion Criteria | Exercise Intervention | Study Population | Frequency and Duration | Key Findings | Training Effect/Dose Effect |
|---|---|---|---|---|---|---|
| (1) Adachi et al. 1996 [19] | Post-MI | Walking UC: no structured physical activity LICT: 15 min/session at 80% of VT1 HICT: 15 min/session at HR of 40% ∆ HR—VT1 HR | Duration between MI and training onset = 48 ± 8 days n = 29 UC: 62 ± 9 y, 75% male LICT:63 ± 7 y, 91% male HICT:51 ± 11 y, 90% male | 2x/day 5x/wk 2 mo | ∆UC = ↑ 10% (p = 0.09) LICT = ↑ 9% (p = 0.20) HICT = ↑ 14% (p = 0.03) Additional Findings:
| Yes/yes Training effect only with HICT |
| (2) Conraads et al. 2015 [20] | Post-MI, post-PCI, or post-CABG | Cycling MICT: 47 min/session including 5 min warm-up, 37 min at 70–75% HRPEAK, 5 min cool-downHIIT: 38 min/session including 10 min of warm-up, 4 × 4 min at 90–95% HRPEAK interspersed by 3 min at 50–70% HRPEAK, 3 min cool-down | Duration between acute event and training onset = 4–12 wk n = 200 MICT: 59.9 ± 9.2 y, 89% male HIIT: 57.0 ± 8.8 y, 91% male | 3x/wk 12 wk | ∆MICT = 20.3% (p < 0.001) HIIT = 22.7% (p < 0.001) Additional Findings:
| Yes/no |
| (3) Currie et al. 2013 [21] | Post-MI, post-PCI, or post-CABG | Cycling MICT: 30–50 min/session at 58% of PPO HIIT: 20 min/session consisting of 10 × 1 min at 80–104% of PPO interspersed with 1 min at 10% of PPO HIIT = ½ training load of MICT | Patients referred to CR n = 22 MICT: 68 ± 8 y, 91% male HIIT: 62 ± 11 y, 91% male | 3x/wk 12 wk | ∆MICT = 19% (p ≤ 0.001) HIIT = 24% (p ≤ 0.001) Additional Findings:
| Yes/yes |
| (4) Keteyian et al. 2014 [22] | Post-MI, post-PCI, or post-CABG; EF > 40% | Treadmill MICT: 40 min/session, including 5 min warm-up, 30 min at 60–80% HRR, 5 min cool-downHIIT: 40 min/session consisting of 5 min warm-up, 3 min at 60–70% HRR, 4 × 4 min at 80–90% HRR interspersed by 3 min at 60–70% HRR, 4 min cool-down | Patients enrolled in CR Duration between MI or PCI and training onset >3 wk Duration between CABG and training onset >4 wk n = 28 MICT: 58 ± 9 y, 92% male HIIT: 60 ± 7 y, 73% male | 3x/wk 10 wk | ∆MICT = 8% (p ≤ 0.05) HIIT = 16% (p ≤ 0.05) Additional Findings:
| Yes/yes |
| (5) Kim & Choi 2020 [23] | Post-ACS | Walking HIIT: 50 min/session consisting of 10 min warm-up at 50–70% HRR, 3 × 8 min at 85% HRR interspersed by 3 min at 40% HRR, 10 min cool-down at 50–70% HRR MIIT: 45 min/session including 10 min warm-up at 50–70% HRR, 4 × 4 min at 95–100% HRR interspersed by 3 min at 60% HRR, 10 min cool-down at 50–70% HRR | Duration between ACS and training onset > 3 wk n = 47 HIIT: 62.8 ± 11.9 y, 67% male MIIT: 60.0 ± 11.0 y, 78% male | 3x/wk 6 wk | ∆HIIT = 17% (p < 0.05) MIIT = 31% (p < 0.05) Additional Findings:
| Yes/yes |
| (6) Madssen et al. 2014 [24] | Post-angina pectoris or non-ST elevation ACS following stent implantation | Walking/running MICT: 46 min/session at 70% HRPEAK HIIT: 41 min/session consisting of 10 min warm-up, 4 × 4 min at 85–95% HRPEAK interspersed with 3 min at 70% HRPEAK MICT and HIIT = isocaloric | n = 36 MICT: 60.5 (56.5–63.5) y, 71% male HIIT: 55.5 (50.0–60.5) y, 93% male | 3x/wk 12 wk | ∆MICT = 7% (p < 0.05) HIIT = 11% (p < 0.05) Additional Findings:
| Yes/yes |
| (7) Moholdt et al. 2009 [25] | Post-CABG | Treadmill walking MICT: 46 min/session at 70% HRPEAK HIIT: 41 min/session consisting of 8 min warm-up, 4 × 4 min at 90% HRPEAK interspersed with 3 min at 70% HRPEAK, 5 min cool-downHIIT and MICT = isocaloric | Duration between CABG and training onset = 4–16 wks n = 59 MICT: 62.0 ± 7.6 y, 77% male HIIT: 60.2 ± 6.9 y, 86% male | 5x/wk 4 wk | ∆MICT = 9% (p < 0.001) HIIT = 12% (p < 0.001) Additional Findings:
| Yes/no |
| (8) Moholdt et al. 2012 [26] | Post-MI | Aerobic: 60 min consisting of 10 min warm-up, 35 min of aerobic exercise (walking, jogging, lunges, squats) following music, 10 min cool-downHIIT:38 min of treadmill consisting of 8 min warm-up, 4 × 4 min at 85% HRPEAK interspersed with 3 min at 70% HRPEAK, 5 min cool-down | Duration between MI and training onset = 2–12 wk n = 107 Aerobics: 57.7 ± 9.3 y, 83% male HIIT: 56.7 ± 10.4 y, 83% male | 3x/wk 12 wk | ∆Aerobics = 7.5% (p < 0.001) HIIT = 14% (p < 0.001) Additional Findings:
| Yes/yes |
| (9) Nam et al. 2024 [27] | Post-MI | Treadmill UC:instructed to exercise at an RPE of 11–13 with no restrictions placed on exercise activitiesHIIIT: 50 min consisting of 10 min at 40% , 4 × 4 min at 85% interspersed with 3 min at 60% , 10 min cool-down at 40% MIIT: 50 min consisting of 10 min at 40% , 4 × 4 min at 95–100% interspersed with 3 min at 60% , 10 min cool-down at 40% | Duration between MI and training onset = 1–2 wk n = 106 UC: 56.7 ± 9.5 y, 88% male HIIT: 58.7 ± 12.4 y, 86% male MIIT: 56.1 ± 10.5 y, 90% male | 2x/wk 9 wk | ∆UC = 5% (p < 0.05) HIIT = 17% (p < 0.05) MIIT = 30% (p < 0.05) Additional Findings:
| Yes/yes |
| (10) Rognmo et al. 2004 [28] | Post-MI, post-PCI, or post-CABG | Uphill treadmill walking MICT: 41 min at 50–60% HIIT: 33 min consisting of 5 min warm-up at 50–60% , 4 × 4 min at 80–90% VO2PEAK interspersed by 3 min at 50–60% , 3 min cool-down at 50–60% MICT and HIIT = same workload | Duration between MI and training onset >3 mo; duration between PCI/CABG and training onset > 12 mo n = 21 MICT: 61.2 ± 7.3 y, 89% male HIIT: 62.9 ± 11.2 y, 75% male | 3x/wk 10 wk | ∆MICT = 7.9% (p < 0.05) HIIT = 17.9% (p < 0.05) Additional Findings:
| Yes/yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neyroud, D.; Baggish, A.L. Endurance Training Exercise Dose in Coronary Artery Disease Rehabilitation. J. Cardiovasc. Dev. Dis. 2025, 12, 134. https://doi.org/10.3390/jcdd12040134
Neyroud D, Baggish AL. Endurance Training Exercise Dose in Coronary Artery Disease Rehabilitation. Journal of Cardiovascular Development and Disease. 2025; 12(4):134. https://doi.org/10.3390/jcdd12040134
Chicago/Turabian StyleNeyroud, Daria, and Aaron L. Baggish. 2025. "Endurance Training Exercise Dose in Coronary Artery Disease Rehabilitation" Journal of Cardiovascular Development and Disease 12, no. 4: 134. https://doi.org/10.3390/jcdd12040134
APA StyleNeyroud, D., & Baggish, A. L. (2025). Endurance Training Exercise Dose in Coronary Artery Disease Rehabilitation. Journal of Cardiovascular Development and Disease, 12(4), 134. https://doi.org/10.3390/jcdd12040134