
Intraoperative Hemoadsorption in Heart Transplant Surgery: A 5-Year Experience

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Study Design
2.2. Ethics Statement
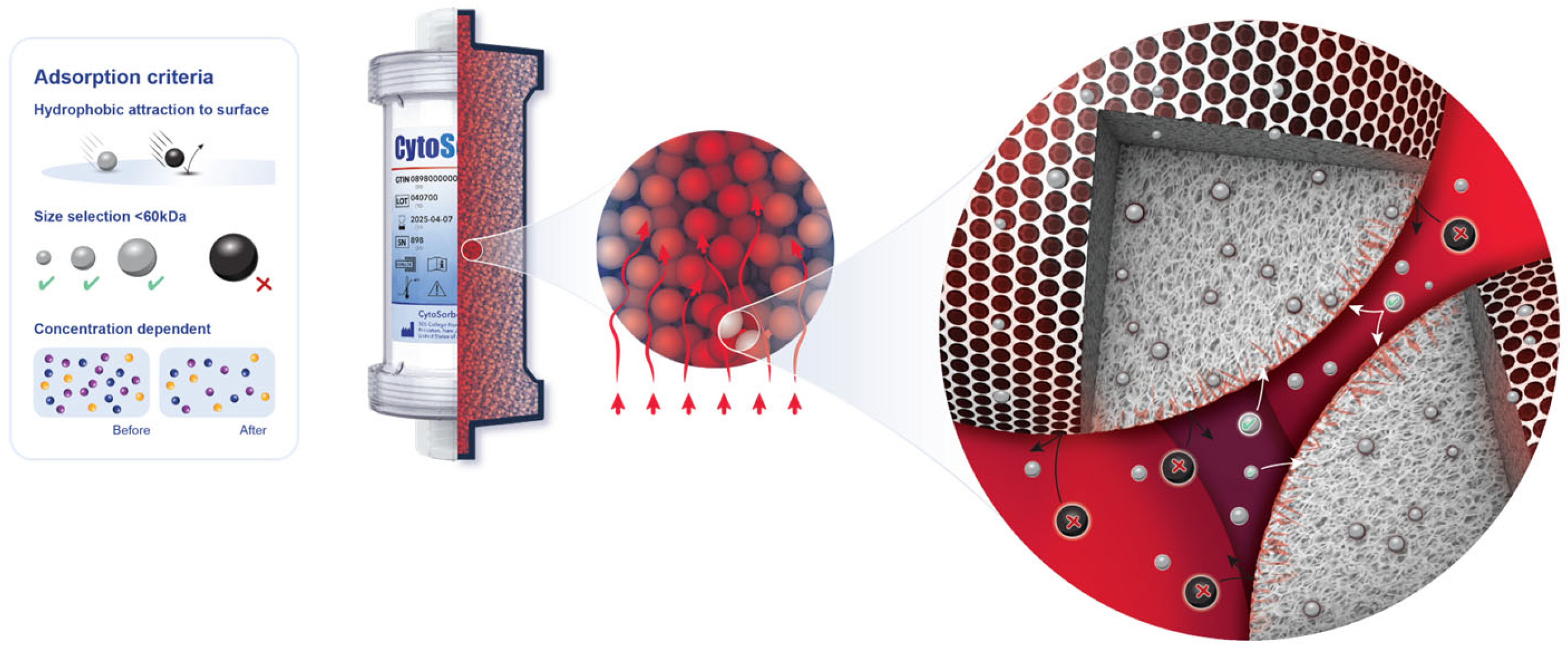
2.3. Device Information
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Patient Cohort and Operative Details
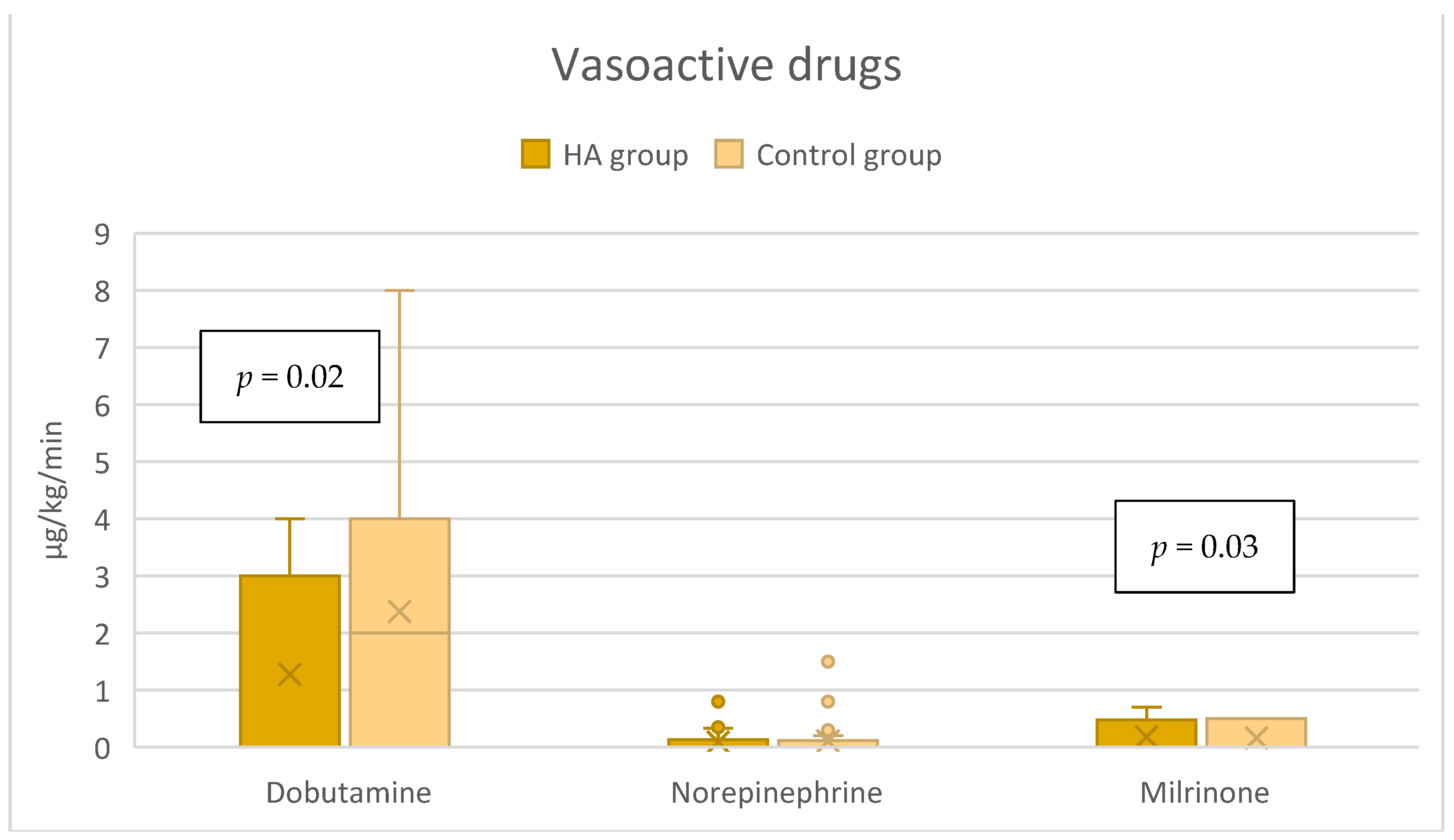
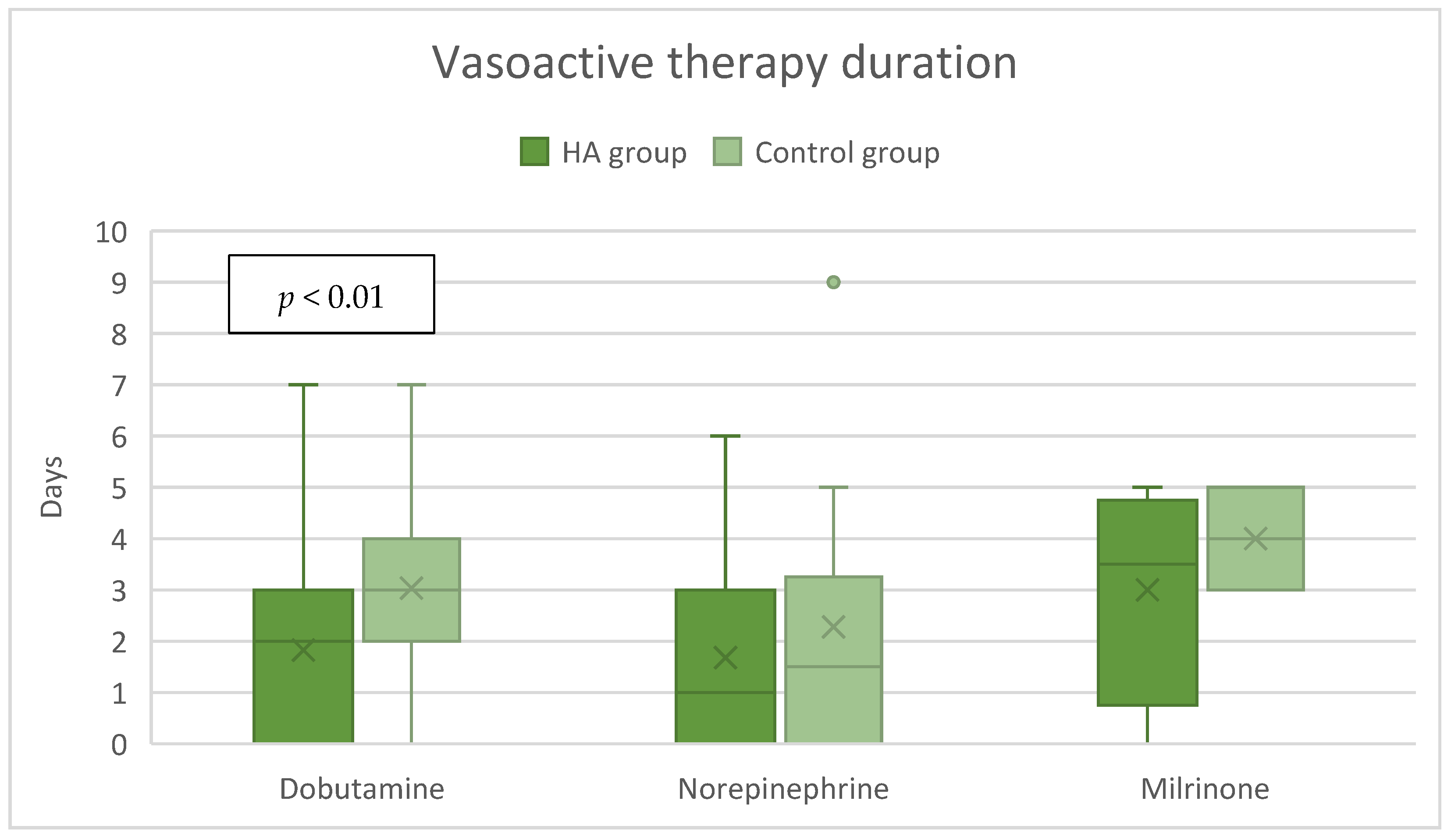
3.2. Hemodynamic Stability
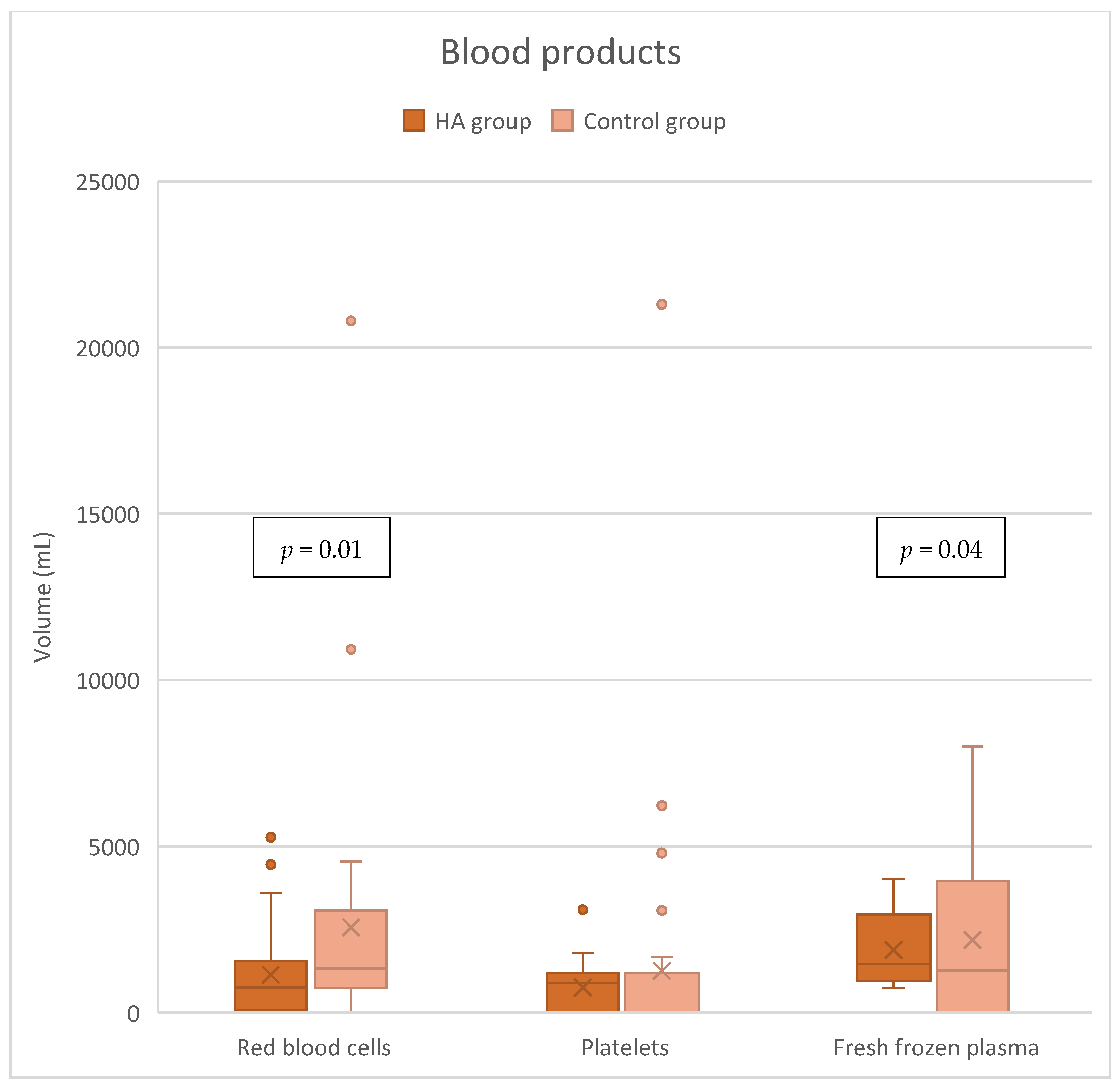
3.3. Blood Product Requirements
3.4. Acute Kidney Injury Requiring Hemodialysis
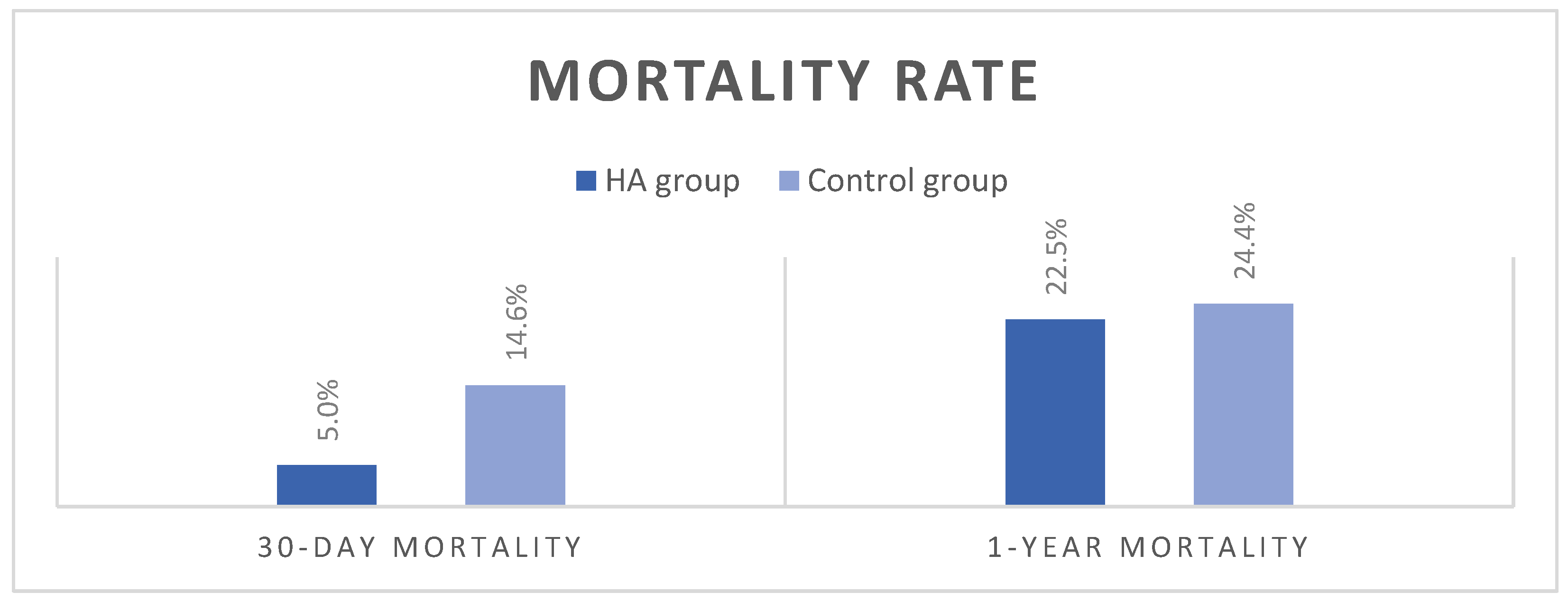
3.5. Mortality and Other Postoperative Clinical Outcomes
3.6. Regression Analysis (Table S2)
4. Discussion
4.1. Hemodynamic Stability
4.2. Secondary and Other Outcomes
4.3. Blood Product Consumption
4.4. Clinical Implications and Future Directions
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart. J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Goldfarb, S.; Hayes, D., Jr.; Kucheryavaya, A.Y.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; Stehlik, J.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth Adult Heart Transplantation Report-2018; Focus Theme: Multiorgan Transplantation. J. Heart Lung Transplant. 2018, 37, 1155–1168. [Google Scholar] [CrossRef] [PubMed]
- Matejic-Spasic, M.; Lindstedt, S.; Lebreton, G.; Dzemali, O.; Suwalski, P.; Folliguet, T.; Geidel, S.; Klautz, R.J.M.; Baufreton, C.; Livi, U.; et al. The role of hemoadsorption in cardiac surgery—A systematic review. BMC Cardiovasc. Disord. 2024, 24, 258. [Google Scholar] [CrossRef]
- Naruka, V.; Salmasi, M.Y.; Arjomandi Rad, A.; Marczin, N.; Lazopoulos, G.; Moscarelli, M.; Casula, R.; Athanasiou, T. Use of Cytokine Filters During Cardiopulmonary Bypass: Systematic Review and Meta-Analysis. Heart Lung Circ. 2022, 31, 1493–1503. [Google Scholar] [CrossRef]
- Squiccimarro, E.; Stasi, A.; Lorusso, R.; Paparella, D. Narrative review of the systemic inflammatory reaction to cardiac surgery and cardiopulmonary bypass. Artif. Organs 2022, 46, 568–577. [Google Scholar] [CrossRef]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic syndrome following cardiothoracic surgery-review of pathophysiology and update of treatment options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef] [PubMed]
- Kalisnik, J.M.; Leiler, S.; Mamdooh, H.; Zibert, J.; Bertsch, T.; Vogt, F.A.; Bagaev, E.; Fittkau, M.; Fischlein, T. Single-Centre Retrospective Evaluation of Intraoperative Hemoadsorption in Left-Sided Acute Infective Endocarditis. J. Clin. Med. 2022, 11, 3954. [Google Scholar] [CrossRef]
- Haidari, Z.; Leiler, S.; Mamdooh, H.; Fittkau, M.; Boss, K.; Tyczynski, B.; Thielmann, M.; Bagaev, E.; El Gabry, M.; Wendt, D.; et al. Effect of intraoperative haemoadsorption therapy on cardiac surgery for active infective endocarditis with confirmed Staphylococcus aureus bacteraemia. Interdiscip. Cardiovasc. Thorac. Surg. 2023, 36, ivad010. [Google Scholar] [CrossRef]
- Saller, T.; Hagl, C.; Woitsch, S.; Li, Y.; Niedermayer, S.; Born, F.; Luehr, M.; Kammerer, T.; Pichlmaier, M.; Scheiermann, P.; et al. Haemadsorption improves intraoperative haemodynamics and metabolic changes during aortic surgery with hypothermic circulatory arrest. Eur. J. Cardiothorac. Surg. 2019, 56, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Doukas, P.; Hellfritsch, G.; Wendt, D.; Magliani, M.; Barbati, M.E.; Jalaie, H.; Jacobs, M.J.; Gombert, A. Intraoperative Hemoadsorption (Cytosorb) during Open Thoracoabdominal Aortic Repair: A Pilot Randomized Controlled Trial. J. Clin. Med. 2023, 12, 546. [Google Scholar] [CrossRef]
- Schmoeckel, M.; Thielmann, M.; Hassan, K.; Geidel, S.; Schmitto, J.; Meyer, A.L.; Vitanova, K.; Liebold, A.; Marczin, N.; Bernardi, M.H.; et al. Intraoperative haemoadsorption for antithrombotic drug removal during cardiac surgery: Initial report of the international safe and timely antithrombotic removal (STAR) registry. J. Thromb. Thrombolysis 2024, 57, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Hassan, K.; Geidel, S.; Zamvar, V.; Tanaka, K.; Knezevic-Woods, Z.; Wendt, D.; Deliargyris, E.N.; Storey, R.F.; Schmoeckel, M. Intraoperative ticagrelor removal via hemoadsorption during on-pump coronary artery bypass grafting. JTCVS Open 2023, 15, 190–196. [Google Scholar] [CrossRef] [PubMed]
- CytoSorbents. CytoSorb 300 mL Device. Instructions for Use; CytoSorbents Inc.: Princeton, NJ, USA, 2021; Available online: https://www.biocon.com/docs/prescribing_information/ccd/CytoSorb_DeviceInstructionsForUse.pdf (accessed on 2 May 2023).
- Hurskainen, M.; Ainasoja, O.; Lemstrom, K.B. Failing Heart Transplants and Rejection-A Cellular Perspective. J. Cardiovasc. Dev. Dis. 2021, 8, 180. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Kovacs, E.; Racz, K.; Soltesz, A.; Szigeti, S.; Kiss, N.; Csikos, G.; Koritsanszky, K.B.; Berzsenyi, V.; Trembickij, G.; et al. Impact of intraoperative cytokine adsorption on outcome of patients undergoing orthotopic heart transplantation-an observational study. Clin. Transplant. 2018, 32, e13211. [Google Scholar] [CrossRef]
- Garcia-Villegas, R.; Arni, S. Hemoadsorption in Organ Preservation and Transplantation: A Narrative Review. Life 2023, 14, 65. [Google Scholar] [CrossRef] [PubMed]
- Garau, I.; Marz, A.; Sehner, S.; Reuter, D.A.; Reichenspurner, H.; Zollner, C.; Kubitz, J.C. Hemadsorption during cardiopulmonary bypass reduces interleukin 8 and tumor necrosis factor alpha serum levels in cardiac surgery: A randomized controlled trial. Minerva Anestesiol. 2019, 85, 715–723. [Google Scholar] [CrossRef]
- Diab, M.; Lehmann, T.; Bothe, W.; Akhyari, P.; Platzer, S.; Wendt, D.; Deppe, A.C.; Strauch, J.; Hagel, S.; Gunther, A.; et al. Cytokine Hemoadsorption During Cardiac Surgery Versus Standard Surgical Care for Infective Endocarditis (REMOVE): Results From a Multicenter Randomized Controlled Trial. Circulation 2022, 145, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Matejic-Spasic, M.; Hassan, K.; Thielmann, M.; Geidel, S.; Storey, R.F.; Schmoeckel, M.; Adamson, H.; Deliargyris, E.N.; Wendt, D. Management of perioperative bleeding risk in patients on antithrombotic medications undergoing cardiac surgery-a systematic review. J. Thorac. Dis. 2022, 14, 3030–3044. [Google Scholar] [CrossRef]
- Grafe, C.; Liebchen, U.; Greimel, A.; Maciuga, N.; Bruegel, M.; Irlbeck, M.; Weidhase, L.; Zoller, M.; Paal, M.; Scharf, C. The effect of cytosorb(R) application on kidney recovery in critically ill patients with severe rhabdomyolysis: A propensity score matching analysis. Ren. Fail. 2023, 45, 2259231. [Google Scholar] [CrossRef]
- Greimel, A.; Habler, K.; Grafe, C.; Maciuga, N.; Brozat, C.I.; Vogeser, M.; Zoller, M.; Happich, F.L.; Liebchen, U.; Frank, S.; et al. Extracorporeal adsorption of protective and toxic bile acids and bilirubin in patients with cholestatic liver dysfunction: A prospective study. Ann. Intensive Care 2023, 13, 110. [Google Scholar] [CrossRef]
- Jansen, A.; Waalders, N.J.B.; van Lier, D.P.T.; Kox, M.; Pickkers, P. CytoSorb hemoperfusion markedly attenuates circulating cytokine concentrations during systemic inflammation in humans in vivo. Crit. Care 2023, 27, 117. [Google Scholar] [CrossRef]
- Nemeth, E.; Soltesz, A.; Kovacs, E.; Szakal-Toth, Z.; Tamaska, E.; Katona, H.; Racz, K.; Csikos, G.; Berzsenyi, V.; Fabry, S.; et al. Use of intraoperative haemoadsorption in patients undergoing heart transplantation: A proof-of-concept randomized trial. ESC Heart Fail. 2024, 11, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Leber, B.; Liebchen, U.; Rohrhofer, L.; Weber, J.; Klaus, T.; Scheier, J.; Sucher, R.; Stiegler, P. Pharmacokinetics of immunosuppressive agents during hemoperfusion in a sheep model. Front. Med. 2023, 10, 1258661. [Google Scholar] [CrossRef]
- Datt, V.; Wadhhwa, R.; Sharma, V.; Virmani, S.; Minhas, H.S.; Malik, S. Vasoplegic syndrome after cardiovascular surgery: A review of pathophysiology and outcome-oriented therapeutic management. J. Card. Surg. 2021, 36, 3749–3760. [Google Scholar] [CrossRef] [PubMed]
- Ltaief, Z.; Ben-Hamouda, N.; Rancati, V.; Gunga, Z.; Marcucci, C.; Kirsch, M.; Liaudet, L. Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care. J. Clin. Med. 2022, 11, 6407. [Google Scholar] [CrossRef]
- Huette, P.; Moussa, M.D.; Beyls, C.; Guinot, P.G.; Guilbart, M.; Besserve, P.; Bouhlal, M.; Mounjid, S.; Dupont, H.; Mahjoub, Y.; et al. Association between acute kidney injury and norepinephrine use following cardiac surgery: A retrospective propensity score-weighted analysis. Ann. Intensive Care 2022, 12, 61. [Google Scholar] [CrossRef]
- Venema, C.S.; Erasmus, M.E.; Mariani, M.; Voors, A.A.; Damman, K. Post-transplant inotrope score is associated with clinical outcomes after adult heart transplantation. Clin. Transplant. 2021, 35, e14347. [Google Scholar] [CrossRef]
- Chan, J.L.; Kobashigawa, J.A.; Aintablian, T.L.; Li, Y.; Perry, P.A.; Patel, J.K.; Kittleson, M.M.; Czer, L.S.; Zarrini, P.; Velleca, A.; et al. Vasoplegia after heart transplantation: Outcomes at 1 year. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 212–217. [Google Scholar] [CrossRef]
- Batchelor, R.J.; Wong, N.; Liu, D.H.; Chua, C.; William, J.; Tee, S.L.; Sata, Y.; Bergin, P.; Hare, J.; Leet, A.; et al. Vasoplegia Following Orthotopic Heart Transplantation: Prevalence, Predictors and Clinical Outcomes. J. Card. Fail. 2022, 28, 617–626. [Google Scholar] [CrossRef]
- Kumar, N.; Fitzsimons, M.G.; Iyer, M.H.; Essandoh, M.; Kumar, J.E.; Dalia, A.A.; Osho, A.; Sawyer, T.R.; Bardia, A. Vasoplegic syndrome during heart transplantation: A systematic review and meta-analysis. J. Heart Lung Transplant. 2024, 43, 931–943. [Google Scholar] [CrossRef]
- Jernryd, V.; Metzsch, C.; Andersson, B.; Nilsson, J. The influence of ischemia and reperfusion time on outcome in heart transplantation. Clin. Transplant. 2020, 34, e13840. [Google Scholar] [CrossRef] [PubMed]
- Jernryd, V.; Stehlik, J.; Metzsch, C.; Lund, L.H.; Gustav Smith, J.; Andersson, B.; Perez, R.; Nilsson, J. Donor age and ischemic time in heart transplantation—Implications for organ preservation. J. Heart Lung Transplant. 2025, 44, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Curcio, A.; Noma, T.; Naga Prasad, S.V.; Wolf, M.J.; Lemaire, A.; Perrino, C.; Mao, L.; Rockman, H.A. Competitive displacement of phosphoinositide 3-kinase from beta-adrenergic receptor kinase-1 improves postinfarction adverse myocardial remodeling. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H1754–H1760. [Google Scholar] [CrossRef] [PubMed]
- Indolfi, C.; Gasparri, C.; Vicinanza, C.; De Serio, D.; Boncompagni, D.; Mongiardo, A.; Spaccarotella, C.; Agosti, V.; Torella, D.; Curcio, A. Mitogen-activated protein kinases activation in T lymphocytes of patients with acute coronary syndromes. Basic Res. Cardiol. 2011, 106, 667–679. [Google Scholar] [CrossRef]
- Toy, P.; Gajic, O.; Bacchetti, P.; Looney, M.R.; Gropper, M.A.; Hubmayr, R.; Lowell, C.A.; Norris, P.J.; Murphy, E.L.; Weiskopf, R.B.; et al. Transfusion-related acute lung injury: Incidence and risk factors. Blood 2012, 119, 1757–1767. [Google Scholar] [CrossRef]
- Kim, H.J.; Ko, D.-H. Transfusion-transmitted infections. Blood Res. 2024, 59, 14. [Google Scholar] [CrossRef]
- Bhaskar, B.; Dulhunty, J.; Mullany, D.V.; Fraser, J.F. Impact of blood product transfusion on short and long-term survival after cardiac surgery: More evidence. Ann. Thorac. Surg. 2012, 94, 460–467. [Google Scholar] [CrossRef]
- Siniarski, A.; Gasecka, A.; Borovac, J.A.; Papakonstantinou, P.E.; Bongiovanni, D.; Ehrlinder, H.; Giustozzi, M.; Guerreiro, R.A.; Parker, W.A.E. Blood Coagulation Disorders in Heart Failure: From Basic Science to Clinical Perspectives. J. Card. Fail. 2023, 29, 517–526. [Google Scholar] [CrossRef]
- Holmen, A.; Corderfeldt, A.; Lannemyr, L.; Dellgren, G.; Hansson, E.C. Whole Blood Adsorber During CPB and Need for Vasoactive Treatment After Valve Surgery in Acute Endocarditis: A Randomized Controlled Study. J. Cardiothorac. Vasc. Anesth. 2022, 36, 3015–3020. [Google Scholar] [CrossRef]
- Carvalho, W.D.N.; Alves Maria, G.D.S.; Goncalves, K.C.; Miranda, A.L.; Moreira, M. Health-Related Quality of Life of Heart Transplant Recipients Living in a Developing Country. Transplant. Proc. 2021, 53, 358–363. [Google Scholar] [CrossRef]
- Saemann, L.; Hoorn, F.; Georgevici, A.I.; Pohl, S.; Korkmaz-Icoz, S.; Veres, G.; Guo, Y.; Karck, M.; Simm, A.; Wenzel, F.; et al. Cytokine Adsorber Use during DCD Heart Perfusion Counteracts Coronary Microvascular Dysfunction. Antioxidants 2022, 11, 2280. [Google Scholar] [CrossRef] [PubMed]
- Merlo, A.; Bensimhon, H.F.; Chang, P.P.; Yu, Z.; Watkins, R.; Li, Q.; Byku, M. Use of mechanical circulatory support and survival for heart and heart-kidney transplant recipients in the new allocation system. JHLT Open 2024, 4, 100071. [Google Scholar] [CrossRef] [PubMed]
- Soltesz, A.; Molnar, Z.A.; Szakal-Toth, Z.; Tamaska, E.; Katona, H.; Fabry, S.; Csikos, G.; Berzsenyi, V.; Tamas, C.; Edes, I.F.; et al. Influence of Venoarterial Extracorporeal Membrane Oxygenation Integrated Hemoadsorption on the Early Reversal of Multiorgan and Microcirculatory Dysfunction and Outcome of Refractory Cardiogenic Shock. J. Clin. Med. 2022, 11, 6517. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | HA Group | Control Group | p-Value |
|---|---|---|---|
| Patients, n (%) | 40 (49.4) | 41 (50.6) | 1.00 |
| Sex—female, n (%) | 14 (35.0) | 6 (14.6) | 0.04 |
| Age, years | 58 [49–62] | 57 [48–61] | 0.67 |
| BMI, kg/m2 | 26 [23–30] | 27 [23–30] | 0.87 |
| Patients on high urgency list, n (%) | 20 (50.0) | 21 (51.2) | 1.00 |
INTERMACS, n (%)
| 0 (0) 2 (5.4) 11 (29.7) 3 (8.1) 2 (5.4) 7 (18.9) 12 (32.4) | n/a 3 (10.0) 9 (30.0) 1 (3.3) n/a 7 (23.3) 10 (33.3) | 0.83 |
| Patients requiring MCS, n (%)
| 3 (7.5) 2 (5) 1 (2.5) | 1 (2.4) 1 (2.4) 0 (0) | 0.36 |
NYHA class, n (%)
| 0 (0) 3 (7.5) 19 (47.5) 18 (45.0) | 0 (0) 10 (24.4) 18 (43.9) 13 (31.7) | 0.11 |
| Reoperation, n (%) | 8 (20.0) | 13 (31.7) | 0.31 |
| Donor age, years | 46.5 [34–50] | 47 [41–55] | 0.08 |
| Heart ischemia time, min | 174 [107–207] | 127 [81–169] | 0.01 |
| Surgery time, min | 250 [222–300] | 295 [250–360] | 0.01 |
| CPB time, min | 130 [118–148] | 130.5 [113–171] | 0.73 |
| VIS (intraoperative) | 7.25 [4–15] | 5 [3–10] | 0.28 |
| 0 h | 6 h | 12 h | 24 h | ||
|---|---|---|---|---|---|
| Lactate (mmol/L) | HA group | 1.9 [1.3–3.9] | 4.1 [3.0–5.9] | 3.1 [2.4–4.6] | 1.9 [1.6–2.5] |
| Control group | 2.1 [1.5–3.7] | 3.09 [2.2–5.9] | 3.08 [2.5–3.8] | 1.84 [1.4–2.4] | |
| p-value | 0.6 | 0.2 | 0.8 | 0.4 |
| Variables | HA Group | Control Group | p-Value |
|---|---|---|---|
AKI incidence, n (%)
| 12 (30.0) 8 (20.0) | 21 (51.2) 10 (24.4) | 0.68 0.80 |
| VIS (at 6-h post-op) | 5 [3–19] | 5 [3–14] | 0.75 |
First biopsy, n (%)
| 24 (68.6) 8 (22.8) 3 (8.6) | 34 (100.0) - - | <0.001 |
Second biopsy, n (%)
| 25 (80.6) 6 (19.4) | 29 (93.5) 2 (6.5) | 0.26 |
| Duration of mechanical ventilation, h | 22 [14–27] | 28 [19–38] | 0.01 |
Length of stay, days
| 5 [4–6] 24 [18–26] | 5 [4–6] 22 [19–25] | 0.80 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sliskovic, N.; Sestan, G.; Gjorgjievska, S.; Baric, D.; Unic, D.; Varvodic, J.; Kusurin, M.; Susnjar, D.; Singer, S.; Rudez, I. Intraoperative Hemoadsorption in Heart Transplant Surgery: A 5-Year Experience. J. Cardiovasc. Dev. Dis. 2025, 12, 119. https://doi.org/10.3390/jcdd12040119
Sliskovic N, Sestan G, Gjorgjievska S, Baric D, Unic D, Varvodic J, Kusurin M, Susnjar D, Singer S, Rudez I. Intraoperative Hemoadsorption in Heart Transplant Surgery: A 5-Year Experience. Journal of Cardiovascular Development and Disease. 2025; 12(4):119. https://doi.org/10.3390/jcdd12040119
Chicago/Turabian StyleSliskovic, Nikola, Gloria Sestan, Savica Gjorgjievska, Davor Baric, Daniel Unic, Josip Varvodic, Marko Kusurin, Dubravka Susnjar, Sarah Singer, and Igor Rudez. 2025. "Intraoperative Hemoadsorption in Heart Transplant Surgery: A 5-Year Experience" Journal of Cardiovascular Development and Disease 12, no. 4: 119. https://doi.org/10.3390/jcdd12040119
APA StyleSliskovic, N., Sestan, G., Gjorgjievska, S., Baric, D., Unic, D., Varvodic, J., Kusurin, M., Susnjar, D., Singer, S., & Rudez, I. (2025). Intraoperative Hemoadsorption in Heart Transplant Surgery: A 5-Year Experience. Journal of Cardiovascular Development and Disease, 12(4), 119. https://doi.org/10.3390/jcdd12040119