
Diagnosis and Management of Fetal Arrhythmias in the Current Era


Abstract
1. Introduction
2. Types of Fetal Arrhythmias
3. Extrasystoles
4. Tachyarrhythmias
- Atrioventricular re-entrant tachycardia (AVRT) involving the atrioventricular (AV) node for antegrade conduction and a fast retrograde-conducting accessory AV pathway;
- Permanent junctional reciprocating tachycardia (PJRT) with re-entry across a concealed slow retrograde-conducting accessory pathway;
- Ectopic atrial tachycardia (EAT) due to enhanced automaticity of atrial tissue;
- Atrial flutter (AF) due to a macro-re-entrant pathway within the atrial myocardium and associated with varying degrees of AV block (Figure 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Short VA SVT (60–70%) AVRT/ORT AVNRT | Long VA SVT EAT PJRT | Atrial Flutter (25–30%) | |
|---|---|---|---|
| “Faster and Later” | “Slower and Earlier” | “Variable AV Conduction” | |
| Typical GA at Diagnosis | >18 weeks GA | >12 weeks GA | >28 weeks GA |
| Usual Rates | 210–320 bpm | 170–220 bpm | Atrial rate 300–550 bpm Ventricular rate 180–240 bpm |
| Onset and Termination |
|
| 70% of fetuses with atrial flutter have accessory pathways and may have ORT postnatally |
| Atrioventricular (AV) Relationship |
|
| Variable degrees of AV block (primarily 2:1 or 3:1); fixed ventricular rate |
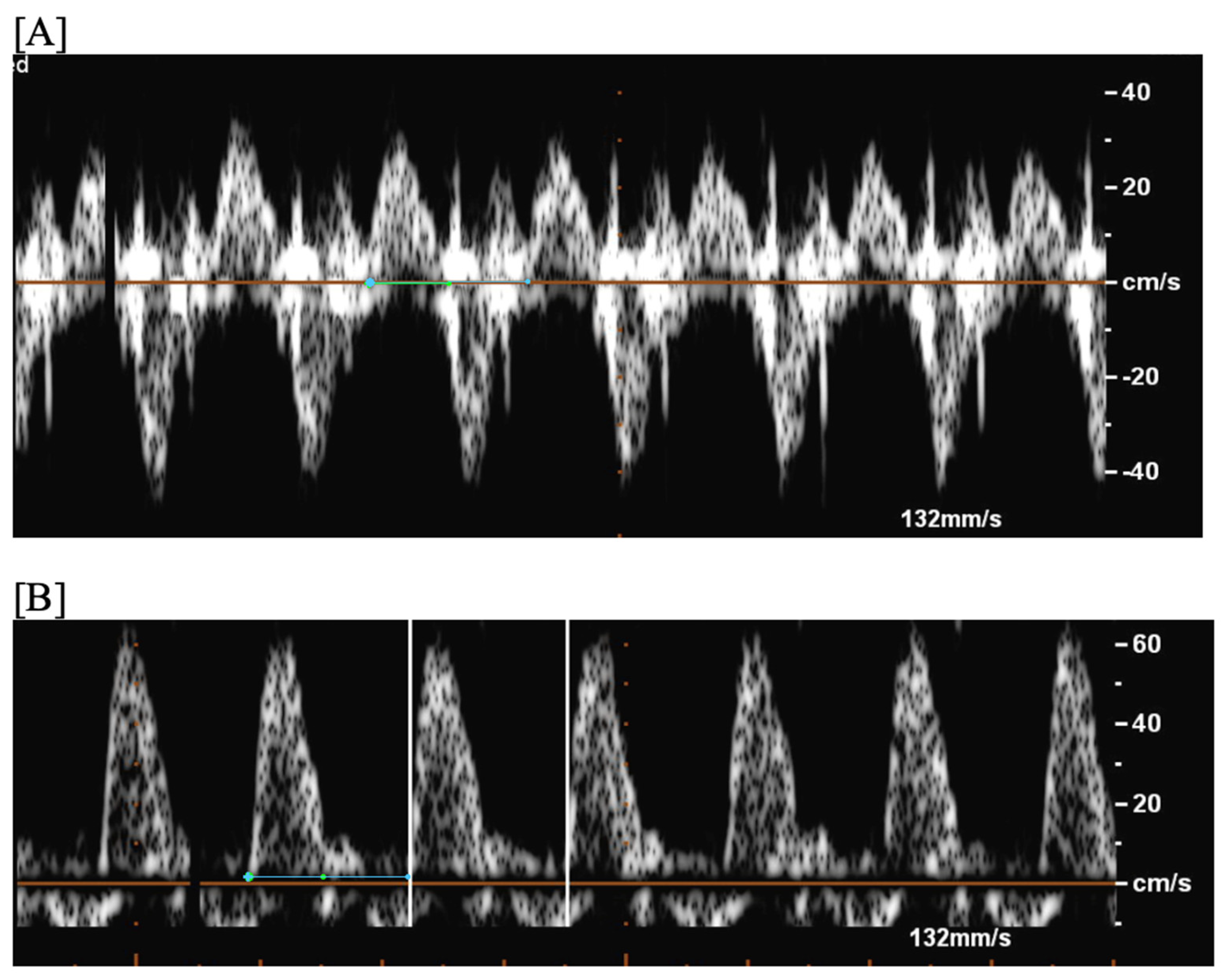
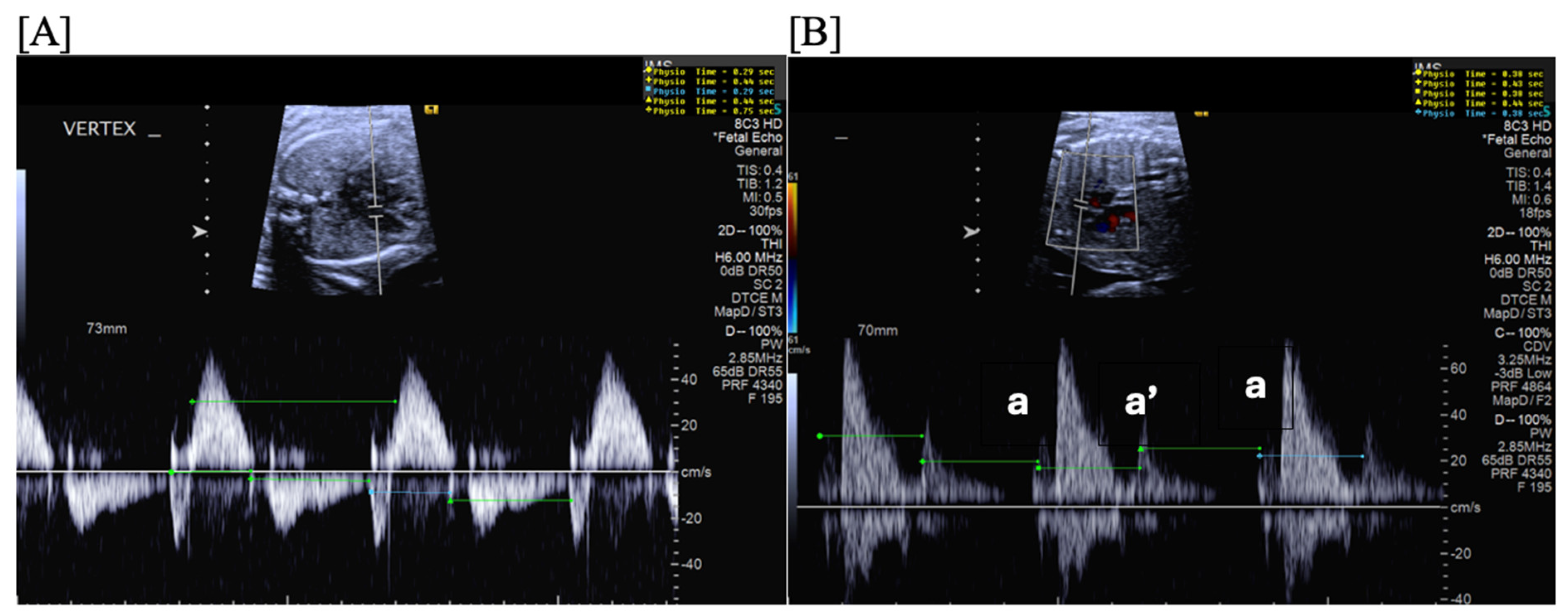
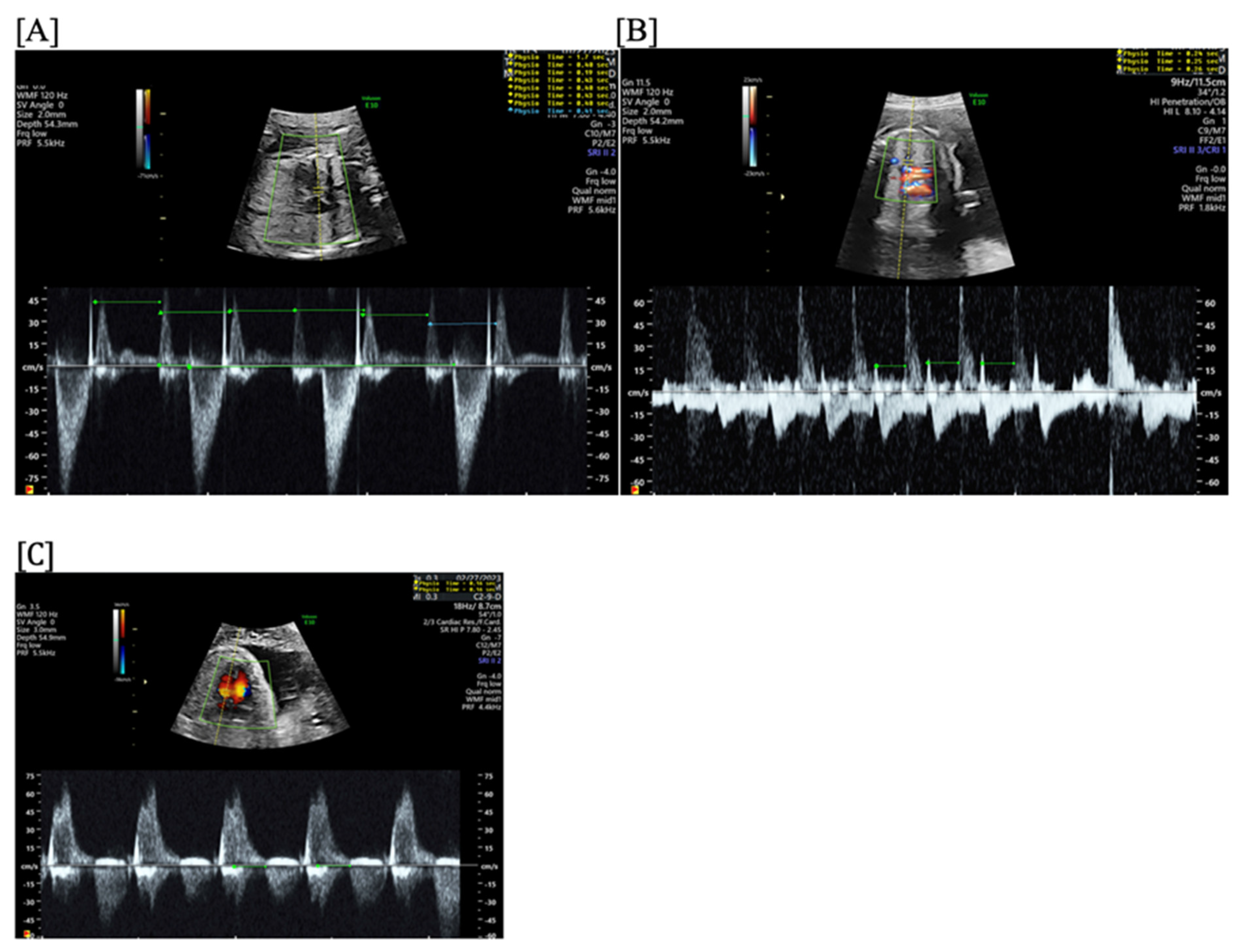
- Short VA SVT (Figure 3 and Figure 4) demonstrates a ventricular–atrial (VA) interval that is less than half of the ventricular–ventricular (VV) interval (VA:AV ratio < 1) and a sudden onset and termination of tachycardia; tachycardia usually terminates with a non-conducted atrial contraction. Short VA SVT includes AVRT (also known as orthodromic reciprocating tachycardia, ORT) and atrioventricular nodal reentrant tachycardia (AVNRT). Short VA SVT typically presents after 18 weeks of gestation.
- Long VA SVT (Figure 4) demonstrates a VA interval that is more than half of the VV interval (VA:AV ratio > 1). Long VA SVT includes EAT and PJRT. A distinguishing feature of EAT is tachycardia termination with ventricular contraction. Long VA SVT may occur as early as 12 weeks of gestation. Because long VA tachycardias have slower rates, they are less likely to cause hydrops.
5. Bradyarrhythmias
5.1. Long QT Syndrome and Other Channelopathies
5.2. Anti-Ro/SSA Mediated Heart Block
6. Diagnostic Tools
7. Multidisciplinary Collaboration and the Maternal-Fetal Dyad
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hornberger, L.K.; Sahn, D.J. Rhythm Abnormalities of the Fetus. Heart 2007, 93, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Wacker-Gussmann, A.; Strasburger, J.F.; Cuneo, B.F.; Wakai, R.T. Diagnosis and Treatment of Fetal Arrhythmia. Am. J. Perinatol. 2014, 31, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, J.F.; Cheulkar, B.; Wichman, H.J. Perinatal Arrhythmias: Diagnosis and Management. Clin. Perinatol. 2007, 34, 627–652. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, J.F.; Eckstein, G.; Butler, M.; Noffke, P.; Wacker-Gussmann, A. Fetal Arrhythmia Diagnosis and Pharmacologic Management. J. Clin. Pharmacol. 2022, 62 (Suppl. 1), S53–S66. [Google Scholar] [CrossRef] [PubMed]
- Veduta, A.; Panaitescu, A.M.; Ciobanu, A.M.; Neculcea, D.; Popescu, M.R.; Peltecu, G.; Cavoretto, P. Treatment of Fetal Arrhythmias. J. Clin. Med. 2021, 10, 2510. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice Bulletin No. 106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Obstet. Gynecol. 2009, 114, 192–202. [CrossRef] [PubMed]
- Pildner von Steinburg, S.; Boulesteix, A.-L.; Lederer, C.; Grunow, S.; Schiermeier, S.; Hatzmann, W.; Schneider, K.-T.M.; Daumer, M. What Is the “Normal” Fetal Heart Rate? PeerJ 2013, 1, e82. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.L.; Cuneo, B.F.; Etheridge, S.P.; Horigome, H.; Weng, H.-Y.; Benson, D.W. Fetal Heart Rate Predictors of Long QT Syndrome. Circulation 2012, 126, 2688–2695. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry-Waterman, N.; Dara, B.; Bucholz, E.; Londono Obregon, C.; Grenier, M.; Snyder, K.; Cuneo, B.F. Fetal Heart Rate < 3rd Percentile for Gestational Age Can Be a Marker of Inherited Arrhythmia Syndromes. J. Clin. Med. 2023, 12, 4464. [Google Scholar] [CrossRef]
- Batra, C.M. Fetal and Neonatal Thyrotoxicosis. Indian J. Endocrinol. Metab. 2013, 17, S50–S54. [Google Scholar] [CrossRef]
- Bohîlțea, R.-E.; Mihai, B.-M.; Szini, E.; Șucaliuc, I.-A.; Badiu, C. Diagnosis and Management of Fetal and Neonatal Thyrotoxicosis. Medicina 2022, 59, 36. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Strasburger, J. Overview of Fetal Arrhythmias. Curr. Opin. Pediatr. 2008, 20, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, J.F. Fetal Arrhythmias. Prog. Pediatr. Cardiol. 2000, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, E.; Öhman, A. Fetal and Neonatal Arrhythmias. Clin. Perinatol. 2016, 43, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Larmay, H.J.; Strasburger, J.F. Differential Diagnosis and Management of the Fetus and Newborn with an Irregular or Abnormal Heart Rate. Pediatr. Clin. N. Am. 2004, 51, 1033–1050. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.L. Fetal Supraventricular Tachycardias: Diagnosis and Management. Semin. Perinatol. 2000, 24, 360–372. [Google Scholar] [CrossRef]
- Southall, D.P.; Richards, J.; Hardwick, R.A.; Shinebourne, E.A.; Gibbens, G.L.; Thelwall-Jones, H.; de Swiet, M.; Johnston, P.G. Prospective Study of Fetal Heart Rate and Rhythm Patterns. Arch. Dis. Child. 1980, 55, 506–511. [Google Scholar] [CrossRef]
- Cuneo, B.F. Treatment of Fetal Tachycardia. Heart Rhythm 2008, 5, 1216–1218. [Google Scholar] [CrossRef]
- Jaeggi, E.T.; Carvalho, J.S.; De Groot, E.; Api, O.; Clur, S.-A.B.; Rammeloo, L.; McCrindle, B.W.; Ryan, G.; Manlhiot, C.; Blom, N.A. Comparison of Transplacental Treatment of Fetal Supraventricular Tachyarrhythmias with Digoxin, Flecainide, and Sotalol: Results of a Nonrandomized Multicenter Study. Circulation 2011, 124, 1747–1754. [Google Scholar] [CrossRef]
- Simpson, J.M.; Sharland, G.K. Fetal Tachycardias: Management and Outcome of 127 Consecutive Cases. Heart 1998, 79, 576–581. [Google Scholar] [CrossRef]
- Boldt, T.; Eronen, M.; Andersson, S. Long-Term Outcome in Fetuses with Cardiac Arrhythmias. Obstet. Gynecol. 2003, 102, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Rasiah, S.V.; Ewer, A.K.; Miller, P.; Kilby, M.D. Prenatal Diagnosis, Management and Outcome of Fetal Dysrhythmia: A Tertiary Fetal Medicine Centre Experience over an Eight-Year Period. Fetal Diagn. Ther. 2011, 30, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.S. Fetal Dysrhythmias. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 58, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Krapp, M.; Kohl, T.; Simpson, J.M.; Sharland, G.K.; Katalinic, A.; Gembruch, U. Review of Diagnosis, Treatment, and Outcome of Fetal Atrial Flutter Compared with Supraventricular Tachycardia. Heart 2003, 89, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.A.; Williams, P.; Lu, Z.; Kavanaugh-McHugh, A.; Fish, F.A.; Killen, S.A.S. Fetuses of Mothers with Thyroid Disease May Be at Higher Risk of Developing Supraventricular Tachycardia. Am. J. Perinatol. 2015, 32, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Naheed, Z.J.; Strasburger, J.F.; Deal, B.J.; Benson, D.W.; Gidding, S.S. Fetal Tachycardia: Mechanisms and Predictors of Hydrops Fetalis. J. Am. Coll. Cardiol. 1996, 27, 1736–1740. [Google Scholar] [CrossRef] [PubMed]
- Fouron, J.-C.; Fournier, A.; Proulx, F.; Lamarche, J.; Bigras, J.L.; Boutin, C.; Brassard, M.; Gamache, S. Management of Fetal Tachyarrhythmia Based on Superior Vena Cava/Aorta Doppler Flow Recordings. Heart 2003, 89, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, E.; Fouron, J.C.; Fournier, A.; van Doesburg, N.; Drblik, S.P.; Proulx, F. Ventriculo-Atrial Time Interval Measured on M Mode Echocardiography: A Determining Element in Diagnosis, Treatment, and Prognosis of Fetal Supraventricular Tachycardia. Heart 1998, 79, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. Diagnosis and Treatment of Fetal Cardiac Disease: A Scientific Statement from the American Heart Association. Circulation 2014, 129, 2183–2242. [Google Scholar] [CrossRef]
- Seravalli, V.; Miller, J.L.; Block-Abraham, D.; Baschat, A.A. Ductus Venosus Doppler in the Assessment of Fetal Cardiovascular Health: An Updated Practical Approach. Acta Obstet. Gynecol. Scand. 2016, 95, 635–644. [Google Scholar] [CrossRef]
- Zoeller, B.B. Treatment of Fetal Supraventricular Tachycardia. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Holmes, S.; Hornberger, L.K.; Jaeggi, E.; Howley, L.; Moon-Grady, A.J.; Uzun, O.; Kaizer, A.; Gilicze, O.; Cuneo, B.F. Treatment, Not Delivery, of the Late Preterm and Term Fetus with Supraventricular Arrhythmia. Ultrasound Obstet. Gynecol. 2023, 62, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Strasburger, J.F.; Cuneo, B.F.; Michon, M.M.; Gotteiner, N.L.; Deal, B.J.; McGregor, S.N.; Oudijk, M.A.; Meijboom, E.J.; Feinkind, L.; Hussey, M.; et al. Amiodarone Therapy for Drug-Refractory Fetal Tachycardia. Circulation 2004, 109, 375–379. [Google Scholar] [CrossRef]
- Cuneo, B.; Drose, J.; Benson, D.W. Diagnosis and Management of Fetal Arrhythmias; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020; ISBN 1-975122-87-9. [Google Scholar]
- Sridharan, S.; Sullivan, I.; Tomek, V.; Wolfenden, J.; Škovránek, J.; Yates, R.; Janoušek, J.; Dominguez, T.E.; Marek, J. Flecainide versus Digoxin for Fetal Supraventricular Tachycardia: Comparison of Two Drug Treatment Protocols. Heart Rhythm 2016, 13, 1913–1919. [Google Scholar] [CrossRef]
- Oudijk, M.A.; Michon, M.M.; Kleinman, C.S.; Kapusta, L.; Stoutenbeek, P.; Visser, G.H.; Meijboom, E.J. Sotalol in the Treatment of Fetal Dysrhythmias. Circulation 2000, 101, 2721–2726. [Google Scholar] [CrossRef]
- Shah, A.; Moon-Grady, A.; Bhogal, N.; Collins, K.K.; Tacy, T.; Brook, M.; Hornberger, L.K. Effectiveness of Sotalol as First-Line Therapy for Fetal Supraventricular Tachyarrhythmias. Am. J. Cardiol. 2012, 109, 1614–1618. [Google Scholar] [CrossRef] [PubMed]
- van der Heijden, L.B.; Oudijk, M.A.; Manten, G.T.R.; ter Heide, H.; Pistorius, L.; Freund, M.W. Sotalol as First-Line Treatment for Fetal Tachycardia and Neonatal Follow-Up. Ultrasound Obstet. Gynecol. 2013, 42, 285–293. [Google Scholar] [CrossRef]
- Oudijk, M.A.; Stoutenbeek, P.; Sreeram, N.; Visser, G.H.A.; Meijboom, E.J. Persistent Junctional Reciprocating Tachycardia in the Fetus. J. Matern.-Fetal Neonatal Med. 2003, 13, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Hill, G.D.; Kovach, J.R.; Saudek, D.E.; Singh, A.K.; Wehrheim, K.; Frommelt, M.A. Transplacental Treatment of Fetal Tachycardia: A Systematic Review and Meta-Analysis. Prenat. Diagn. 2017, 37, 1076–1083. [Google Scholar] [CrossRef]
- Alsaied, T.; Baskar, S.; Fares, M.; Alahdab, F.; Czosek, R.J.; Murad, M.H.; Prokop, L.J.; Divanovic, A.A. First-Line Antiarrhythmic Transplacental Treatment for Fetal Tachyarrhythmia: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2017, 6, e007164. [Google Scholar] [CrossRef]
- Jouannic, J.-M.; Delahaye, S.; Fermont, L.; Le Bidois, J.; Villain, E.; Dumez, Y.; Dommergues, M. Fetal Supraventricular Tachycardia: A Role for Amiodarone as Second-Line Therapy? Prenat. Diagn. 2003, 23, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Bartalena, L.; Bogazzi, F.; Braverman, L.E.; Martino, E. Effects of Amiodarone Administration during Pregnancy on Neonatal Thyroid Function and Subsequent Neurodevelopment. J. Endocrinol. Investig. 2001, 24, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Vanbesien, J.; Casteels, A.; Bougatef, A.; De Catte, L.; Foulon, W.; De Bock, S.; Smitz, J.; De Schepper, J. Transient Fetal Hypothyroidism Due to Direct Fetal Administration of Amiodarone for Drug Resistant Fetal Tachycardia. Am. J. Perinatol. 2001, 18, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Gembruch, U.; Hansmann, M.; Redel, D.A.; Bald, R. Intrauterine Therapy of Fetal Tachyarrhythmias: Intraperitoneal Administration of Antiarrhythmic Drugs to the Fetus in Fetal Tachyarrhythmias with Severe Hydrops Fetalis. J. Perinat. Med. 1988, 16, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Parilla, B.V.; Strasburger, J.F.; Socol, M.L. Fetal Supraventricular Tachycardia Complicated by Hydrops Fetalis: A Role for Direct Fetal Intramuscular Therapy. Am. J. Perinatol. 1996, 13, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Kohl, T.; Tercanli, S.; Kececioglu, D.; Holzgreve, W. Direct Fetal Administration of Adenosine for the Termination of Incessant Supraventricular Tachycardia. Obstet. Gynecol. 1995, 85, 873–874. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, B.F.; Strasburger, J.F.; Niksch, A.; Ovadia, M.; Wakai, R.T. An Expanded Phenotype of Maternal SSA/SSB Antibody-Associated Fetal Cardiac Disease. J. Matern.-Fetal Neonatal Med. 2009, 22, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.H.; Samai, C.; Gomez, K.; Kanaan, U. Maternal Antibody-Associated Fetal Second-Degree Heart Block and Atrial Flutter: Case Report and Review. Pediatr. Cardiol. 2013, 34, 2040–2043. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, T.; Maeno, Y.; Hamasaki, T.; Inamura, N.; Yasukochi, S.; Kawataki, M.; Horigome, H.; Yoda, H.; Taketazu, M.; Nii, M.; et al. Antenatal Therapy for Fetal Supraventricular Tachyarrhythmias: Multicenter Trial. J. Am. Coll. Cardiol. 2019, 74, 874–885. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Moon-Grady, A.J.; Sonesson, S.-E.; Levasseur, S.; Hornberger, L.; Donofrio, M.T.; Krishnan, A.; Szwast, A.; Howley, L.; Benson, D.W.; et al. Heart Sounds at Home: Feasibility of an Ambulatory Fetal Heart Rhythm Surveillance Program for Anti-SSA-Positive Pregnancies. J. Perinatol. 2017, 37, 226–230. [Google Scholar] [CrossRef]
- Strasburger, J.F. Predictability in Fetal Supraventricular Tachycardia Management. J. Am. Coll. Cardiol. 2019, 74, 886–888. [Google Scholar] [CrossRef] [PubMed]
- Bourget, P.; Pons, J.C.; Delouis, C.; Fermont, L.; Frydman, R. Flecainide Distribution, Transplacental Passage, and Accumulation in the Amniotic Fluid during the Third Trimester of Pregnancy. Ann. Pharmacother. 1994, 28, 1031–1034. [Google Scholar] [CrossRef] [PubMed]
- Hopson, J.R.; Buxton, A.E.; Rinkenberger, R.L.; Nademanee, K.; Heilman, J.M.; Kienzle, M.G. Safety and Utility of Flecainide Acetate in the Routine Care of Patients with Supraventricular Tachyarrhythmias: Results of a Multicenter Trial. The Flecainide Supraventricular Tachycardia Study Group. Am. J. Cardiol. 1996, 77, 72A–82A. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, E.T.; Alexander, M.E.; Bezzerides, V.J.; Drogosz, M.; Economy, K.E.; Friedman, K.G.; Pickard, S.S.; Tworetzky, W.; Mah, D.Y. Low Mortality in Fetal Supraventricular Tachycardia: Outcomes in a 30-Year Single-Institution Experience. J. Cardiovasc. Electrophysiol. 2020, 31, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Moodley, S.; Sanatani, S.; Potts, J.E.; Sandor, G.G.S. Postnatal Outcome in Patients with Fetal Tachycardia. Pediatr. Cardiol. 2013, 34, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Hinkle, K.A.; Peyvandi, S.; Stiver, C.; Killen, S.A.S.; Weng, H.Y.; Etheridge, S.P.; Puchalski, M.D. Postnatal Outcomes of Fetal Supraventricular Tachycardia: A Multicenter Study. Pediatr. Cardiol. 2017, 38, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Till, J.; Wren, C. Atrial Flutter in the Fetus and Young Infant: An Association with Accessory Connections. Br. Heart J. 1992, 67, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Tunca Sahin, G.; Lewis, M.; Uzun, O. Association of Fetal Atrial Flutter with Neonatal Atrioventricular Re-Entry Tachycardia Involving Accessory Pathway: A Link to Be Remembered. Pediatr. Cardiol. 2021, 42, 849–856. [Google Scholar] [CrossRef] [PubMed]
- van Engelen, A.D.; Weijtens, O.; Brenner, J.I.; Kleinman, C.S.; Copel, J.A.; Stoutenbeek, P.; Meijboom, E.J. Management Outcome and Follow-up of Fetal Tachycardia. J. Am. Coll. Cardiol. 1994, 24, 1371–1375. [Google Scholar] [CrossRef]
- Zaidi, S.J.; Siddiqui, S.; Cuneo, B.F.; Strasburger, J.F.; McDuffie, R.; Wakai, R.T. Prenatal Diagnosis and Management of Junctional Ectopic Tachycardia. Heart Rhythm Case Rep. 2017, 3, 503–508. [Google Scholar] [CrossRef]
- Dubin, A.M.; Cuneo, B.F.; Strasburger, J.F.; Wakai, R.T.; Van Hare, G.F.; Rosenthal, D.N. Congenital Junctional Ectopic Tachycardia and Congenital Complete Atrioventricular Block: A Shared Etiology? Heart Rhythm 2005, 2, 313–315. [Google Scholar] [CrossRef] [PubMed]
- Winbo, A.; Fosdal, I.; Lindh, M.; Diamant, U.-B.; Persson, J.; Wettrell, G.; Rydberg, A. Third Trimester Fetal Heart Rate Predicts Phenotype and Mutation Burden in the Type 1 Long QT Syndrome. Circ. Arrhythmia Electrophysiol. 2015, 8, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, B.F. The Beginnings of Long QT Syndrome. Curr. Opin. Cardiol. 2015, 30, 112–117. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Strasburger, J.F. We Only Find What We Look for: Fetal Heart Rate and the Diagnosis of Long-QT Syndrome. Circ. Arrhythmia Electrophysiol. 2015, 8, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Wacker-Gussmann, A.; Eckstein, G.K.; Strasburger, J.F. Preventing and Treating Torsades de Pointes in the Mother, Fetus and Newborn in the Highest Risk Pregnancies with Inherited Arrhythmia Syndromes. J. Clin. Med. 2023, 12, 3379. [Google Scholar] [CrossRef] [PubMed]
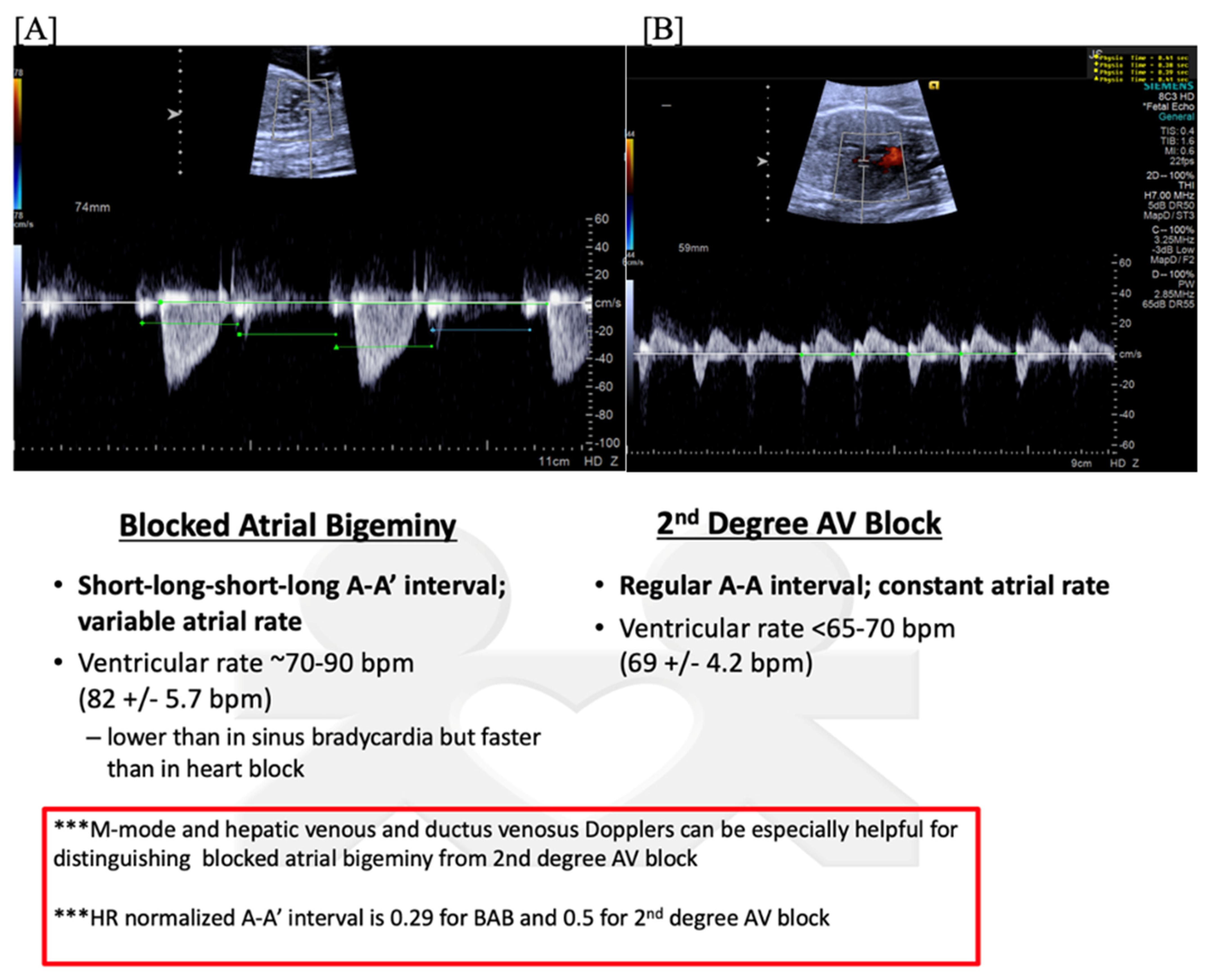
- Sonesson, S.-E.; Eliasson, H.; Conner, P.; Wahren-Herlenius, M. Doppler Echocardiographic Isovolumetric Time Intervals in Diagnosis of Fetal Blocked Atrial Bigeminy and 2:1 Atrioventricular Block. Ultrasound Obstet. Gynecol. 2014, 44, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, D.L.; Strasburger, J.F.; Gotteiner, N.L.; Cuneo, B.; Wakai, R.T. Magnetophysiologic and Echocardiographic Comparison of Blocked Atrial Bigeminy and 2:1 Atrioventricular Block in the Fetus. Heart Rhythm 2013, 10, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Jaeggi, E.T.; Friedberg, M.K. Diagnosis and Management of Fetal Bradyarrhythmias. Pacing Clin. Electrophysiol. 2008, 31 (Suppl. S1), S50–S53. [Google Scholar] [CrossRef] [PubMed]
- Kikano, S.D.; Killen, S.A.S. Transient Fetal Atrioventricular Block: A Series of Four Cases and Approach to Management. J. Cardiovasc. Electrophysiol. 2022, 33, 2228–2232. [Google Scholar] [CrossRef]
- Strand, S.; Strasburger, J.F.; Lutter, W.J.; Wakai, R.T. Repolarization Predictors of Fetal Long QT Syndrome. Heart Rhythm O2 2020, 1, 200–205. [Google Scholar] [CrossRef]
- Crotti, L.; Tester, D.J.; White, W.M.; Bartos, D.C.; Insolia, R.; Besana, A.; Kunic, J.D.; Will, M.L.; Velasco, E.J.; Bair, J.J.; et al. Long QT Syndrome-Associated Mutations in Intrauterine Fetal Death. JAMA 2013, 309, 1473–1482. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.J. Stillbirths, Sudden Infant Deaths, and Long-QT Syndrome: Puzzle or Mosaic, the Pieces of the Jigsaw Are Being Fitted Together. Circulation 2004, 109, 2930–2932. [Google Scholar] [CrossRef] [PubMed]
- Tester, D.J.; Wong, L.C.H.; Chanana, P.; Jaye, A.; Evans, J.M.; FitzPatrick, D.R.; Evans, M.J.; Fleming, P.; Jeffrey, I.; Cohen, M.C.; et al. Cardiac Genetic Predisposition in Sudden Infant Death Syndrome. J. Am. Coll. Cardiol. 2018, 71, 1217–1227. [Google Scholar] [CrossRef]
- Clur, S.-A.B.; Vink, A.S.; Etheridge, S.P.; Robles de Medina, P.G.; Rydberg, A.; Ackerman, M.J.; Wilde, A.A.; Blom, N.A.; Benson, D.W.; Herberg, U.; et al. Left Ventricular Isovolumetric Relaxation Time Is Prolonged in Fetal Long-QT Syndrome. Circ. Arrhythmia Electrophysiol. 2018, 11, e005797. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.N.; Wakai, R.T.; Zhang, J.; Simpson, P.; Strasburger, J.F. Late-Coupled Premature Ventricular Contractions Predict Mortality in Fetuses Evaluated by Fetal Magnetocardiography. JACC Clin. Electrophysiol. 2023, 9, 1601–1603. [Google Scholar] [CrossRef] [PubMed]
- Strand, S.; Strasburger, J.F.; Cuneo, B.F.; Wakai, R.T. Complex and Novel Arrhythmias Precede Stillbirth in Fetuses with De Novo Long QT Syndrome. Circ. Arrhythmia Electrophysiol. 2020, 13, e008082. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Tsuji, Y.; Makita, N. Inherited Bradyarrhythmia: A Diverse Genetic Background. J. Arrhythmia 2016, 32, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Boczek, N.J.; Gomez-Hurtado, N.; Ye, D.; Calvert, M.L.; Tester, D.J.; Kryshtal, D.; Hwang, H.S.; Johnson, C.N.; Chazin, W.J.; Loporcaro, C.G.; et al. Spectrum and Prevalence of CALM1-, CALM2-, and CALM3-Encoded Calmodulin Variants in Long QT Syndrome and Functional Characterization of a Novel Long QT Syndrome-Associated Calmodulin Missense Variant, E141G. Circ. Cardiovasc. Genet. 2016, 9, 136–146. [Google Scholar] [CrossRef]
- Batra, A.S.; Silka, M.J.; Borquez, A.; Cuneo, B.; Dechert, B.; Jaeggi, E.; Kannankeril, P.J.; Tabulov, C.; Tisdale, J.E.; Wolfe, D.; et al. Pharmacological Management of Cardiac Arrhythmias in the Fetal and Neonatal Periods: A Scientific Statement From the American Heart Association: Endorsed by the Pediatric & Congenital Electrophysiology Society (PACES). Circulation 2024, 149, e937–e952. [Google Scholar] [CrossRef]
- Zidere, V.; Vigneswaran, T.V.; Dumitrascu-Biris, I.; Regan, W.; Simpson, J.M.; Homfray, T. Presentation and Genetic Confirmation of Long QT Syndrome in the Fetus. Heart Rhythm Case Rep. 2022, 8, 674–678. [Google Scholar] [CrossRef]
- Putra, M.; Lee, Y.M.; Bucholz, E.; Ross, E.L.; Galan, H.; Behrendt, N.; Micke, K.; Chow, F.S.; Zaretsky, M.V.; Cuneo, B.F. Successful Management of Fetal Torsades de Pointes and Long QT Syndrome by a Cardio-Obstetrical Team. JACC Case Rep. 2023, 27, 102110. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, B.; Bhan, R.; Trad, C.; Cohen, R.; Saxena, A.; Buyon, J.; Izmirly, P. Autoimmune-Mediated Congenital Heart Block. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 64, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Hiebert, R.; Copel, J.; Craft, J.; Friedman, D.; Katholi, M.; Lee, L.A.; Provost, T.T.; Reichlin, M.; Rider, L.; et al. Autoimmune-Associated Congenital Heart Block: Demographics, Mortality, Morbidity and Recurrence Rates Obtained from a National Neonatal Lupus Registry. J. Am. Coll. Cardiol. 1998, 31, 1658–1666. [Google Scholar] [CrossRef] [PubMed]
- Brucato, A.; Franceschini, F.; Buyon, J.P. Neonatal Lupus: Long-Term Outcomes of Mothers and Children and Recurrence Rate. Clin. Exp. Rheumatol. 1997, 15, 467–473. [Google Scholar] [PubMed]
- Cuneo, B.F.; Bitant, S.; Strasburger, J.F.; Kaizer, A.M.; Wakai, R.T. Assessment of Atrioventricular Conduction by Echocardiography and Magnetocardiography in Normal and Anti-Ro/SSA-Antibody-Positive Pregnancies. Ultrasound Obstet. Gynecol. 2019, 54, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Julkunen, H.; Eronen, M. Long-Term Outcome of Mothers of Children with Isolated Heart Block in Finland. Arthritis Rheum. 2001, 44, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, H.; Sonesson, S.-E.; Sharland, G.; Granath, F.; Simpson, J.M.; Carvalho, J.S.; Jicinska, H.; Tomek, V.; Dangel, J.; Zielinsky, P.; et al. Isolated Atrioventricular Block in the Fetus: A Retrospective, Multinational, Multicenter Study of 175 Patients. Circulation 2011, 124, 1919–1926. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.M.; Saxena, A.; Kim, M.Y.; Wang, D.; Sahl, S.K.; Llanos, C.; Friedman, D.; Buyon, J.P. Maternal and Fetal Factors Associated with Mortality and Morbidity in a Multi-Racial/Ethnic Registry of Anti-SSA/Ro-Associated Cardiac Neonatal Lupus. Circulation 2011, 124, 1927–1935. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M.; Chan, E.K.L.; Ho, L.A.; Rose, K.M.; Parks, C.G.; Cohn, R.D.; Jusko, T.A.; Walker, N.J.; Germolec, D.R.; Whitt, I.Z.; et al. Prevalence and Sociodemographic Correlates of Antinuclear Antibodies in the United States. Arthritis Rheum. 2012, 64, 2319–2327. [Google Scholar] [CrossRef]
- Kaizer, A.M.; Lindblade, C.; Clancy, R.; Tebo, A.E.; Drewes, B.; Masson, M.; Chang, M.; Fraser, N.; Buyon, J.P.; Cuneo, B.F. Reducing the Burden of Surveillance in Pregnant Women with No History of Fetal Atrioventricular Block Using the Negative Predictive Value of Anti-Ro/SSA Antibody Titers. Am. J. Obstet. Gynecol. 2022, 227, e1–e761. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Izmirly, P.M.; Ramos-Casals, M.; Buyon, J.P.; Khamashta, M.A. The Clinical Spectrum of Autoimmune Congenital Heart Block. Nat. Rev. Rheumatol. 2015, 11, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Spence, D.; Hornberger, L.; Hamilton, R.; Silverman, E.D. Increased Risk of Complete Congenital Heart Block in Infants Born to Women with Hypothyroidism and Anti-Ro and/or Anti-La Antibodies. J. Rheumatol. 2006, 33, 167–170. [Google Scholar] [PubMed]
- Jaeggi, E.T.; Silverman, E.D.; Laskin, C.; Kingdom, J.; Golding, F.; Weber, R. Prolongation of the Atrioventricular Conduction in Fetuses Exposed to Maternal Anti-Ro/SSA and Anti-La/SSB Antibodies Did Not Predict Progressive Heart Block. A Prospective Observational Study on the Effects of Maternal Antibodies on 165 Fetuses. J. Am. Coll. Cardiol. 2011, 57, 1487–1492. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Ambrose, S.E.; Tworetzky, W. Detection and Successful Treatment of Emergent Anti-SSA-Mediated Fetal Atrioventricular Block. Am. J. Obstet. Gynecol. 2016, 215, 527–528. [Google Scholar] [CrossRef] [PubMed]
- Mawad, W.; Hornberger, L.; Cuneo, B.; Raboisson, M.-J.; Moon-Grady, A.J.; Lougheed, J.; Diab, K.; Parkman, J.; Silverman, E.; Jaeggi, E. Outcome of Antibody-Mediated Fetal Heart Disease With Standardized Anti-Inflammatory Transplacental Treatment. J. Am. Heart Assoc. 2022, 11, e023000. [Google Scholar] [CrossRef]
- Trucco, S.M.; Jaeggi, E.; Cuneo, B.; Moon-Grady, A.J.; Silverman, E.; Silverman, N.; Hornberger, L.K. Use of Intravenous Gamma Globulin and Corticosteroids in the Treatment of Maternal Autoantibody-Mediated Cardiomyopathy. J. Am. Coll. Cardiol. 2011, 57, 715–723. [Google Scholar] [CrossRef]
- Sunderji, S.; Peyvandi, S.; Jaeggi, E.; Szwast, A.; Ryan, G.; Tessier, F.; Siddiqui, S.; Cuneo, B.; Sheth, S.; Treadwell, M.; et al. NAFTNet Retrospective Report on the Treatment of Anti-Ro/SSA Mediated Fetal Heart Block with Dexamethasone. J. Matern.-Fetal Neonatal Med. 2022, 35, 9263–9270. [Google Scholar] [CrossRef]
- Jain, S.; Spadafora, R.; Maxwell, S.; Botas, C.; Nawaytou, H.; von Scheven, E.; Crouch, E.E. A Case of Neonatal Lupus Presenting with Myocardial Dysfunction in the Absence of Congenital Heart Block (CHB): Clinical Management and Brief Literature Review of Neonatal Cardiac Lupus. Pediatr. Cardiol. 2023, 44, 736–739. [Google Scholar] [CrossRef]
- Kelly, E.N.; Sananes, R.; Chiu-Man, C.; Silverman, E.D.; Jaeggi, E. Prenatal Anti-Ro Antibody Exposure, Congenital Complete Atrioventricular Heart Block, and High-Dose Steroid Therapy: Impact on Neurocognitive Outcome in School-Age Children. Arthritis Rheumatol. 2014, 66, 2290–2296. [Google Scholar] [CrossRef]
- Pruetz, J.D.; Miller, J.C.; Loeb, G.E.; Silka, M.J.; Bar-Cohen, Y.; Chmait, R.H. Prenatal Diagnosis and Management of Congenital Complete Heart Block. Birth Defects Res. 2019, 111, 380–388. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Lee, M.; Roberson, D.; Niksch, A.; Ovadia, M.; Parilla, B.V.; Benson, D.W. A Management Strategy for Fetal Immune-Mediated Atrioventricular Block. J. Matern.-Fetal Neonatal Med. 2010, 23, 1400–1405. [Google Scholar] [CrossRef]
- Strasburger, J.F.; Wacker-Gussmann, A. Congenital Heart Block in Subsequent Pregnancies of SSA/Ro-Positive Mothers. J. Am. Coll. Cardiol. 2020, 76, 303–305. [Google Scholar] [CrossRef]
- Izmirly, P.; Kim, M.; Friedman, D.M.; Costedoat-Chalumeau, N.; Clancy, R.; Copel, J.A.; Phoon, C.K.L.; Cuneo, B.F.; Cohen, R.E.; Robins, K.; et al. Hydroxychloroquine to Prevent Recurrent Congenital Heart Block in Fetuses of Anti-SSA/Ro-Positive Mothers. J. Am. Coll. Cardiol. 2020, 76, 292–302. [Google Scholar] [CrossRef]
- Kaplinski, M.; Cuneo, B.F. Novel Approaches to the Surveillance and Management of Fetuses at Risk for Anti-Ro/SSA Mediated Atrioventricular Block. Semin. Perinatol. 2022, 46, 151585. [Google Scholar] [CrossRef] [PubMed]
- Society for Maternal-Fetal Medicine (SMFM); Silver, R.; Craigo, S.; Porter, F.; Osmundson, S.S.; Kuller, J.A.; Norton, M.E. Society for Maternal-Fetal Medicine Consult Series #64: Systemic Lupus Erythematosus in Pregnancy. Am. J. Obstet. Gynecol. 2023, 228, B41–B60. [Google Scholar] [CrossRef] [PubMed]
- Moak, J.P.; Barron, K.S.; Hougen, T.J.; Wiles, H.B.; Balaji, S.; Sreeram, N.; Cohen, M.H.; Nordenberg, A.; Van Hare, G.F.; Friedman, R.A.; et al. Congenital Heart Block: Development of Late-Onset Cardiomyopathy, a Previously Underappreciated Sequela. J. Am. Coll. Cardiol. 2001, 37, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, R.J.; Strasburger, J.F.; Garson, A.; Smith, R.T.; Deter, R.L.; Engelhardt, H.T. Fetal Ventricular Pacing for Hydrops Secondary to Complete Atrioventricular Block. J. Am. Coll. Cardiol. 1986, 8, 1434–1436. [Google Scholar] [CrossRef] [PubMed]
- Bar-Cohen, Y.; Loeb, G.E.; Pruetz, J.D.; Silka, M.J.; Guerra, C.; Vest, A.N.; Zhou, L.; Chmait, R.H. Preclinical Testing and Optimization of a Novel Fetal Micropacemaker. Heart Rhythm 2015, 12, 1683–1690. [Google Scholar] [CrossRef]
- Kohl, T.; Strümper, D.; Witteler, R.; Merschhoff, G.; Alexiene, R.; Callenbeck, C.; Asfour, B.; Reckers, J.; Aryee, S.; Vahlhaus, C.; et al. Fetoscopic Direct Fetal Cardiac Access in Sheep: An Important Experimental Milestone along the Route to Human Fetal Cardiac Intervention. Circulation 2000, 102, 1602–1604. [Google Scholar] [CrossRef]
- Choi, Y.-H.; Stamm, C.; Hammer, P.E.; Kwaku, K.F.; Marler, J.J.; Friehs, I.; Jones, M.; Rader, C.M.; Roy, N.; Eddy, M.-T.; et al. Cardiac Conduction through Engineered Tissue. Am. J. Pathol. 2006, 169, 72–85. [Google Scholar] [CrossRef]
- Berul, C.I.; Dasgupta, S.; LeGras, M.D.; Peer, S.M.; Alsoufi, B.; Sherwin, E.D.; Desai, M.; Yerebakan, C.; Johnsrude, C. Tiny Pacemakers for Tiny Babies. Heart Rhythm 2023, 20, 766–769. [Google Scholar] [CrossRef] [PubMed]
- Howley, L.W.; Eyerly-Webb, S.A.; Killen, S.A.S.; Paul, E.; Krishnan, A.; Gropler, M.R.F.; Drewes, B.; Dion, E.; Lund, A.; Buyon, J.P.; et al. Variation in Prenatal Surveillance and Management of Anti-SSA/Ro Autoantibody Positive Pregnancies. J. Matern.-Fetal Neonatal Med. 2024, 37, 2323623. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Ridder, A.; Smith, V.; Thilaganathan, B.; Bhide, A. Feasibility of Antenatal Ambulatory Fetal Electrocardiography: A Systematic Review. J. Matern.-Fetal Neonatal Med. 2023, 36, 2204390. [Google Scholar] [CrossRef] [PubMed]
- Wacker-Gussmann, A.; Plankl, C.; Sewald, M.; Schneider, K.-T.M.; Oberhoffer, R.; Lobmaier, S.M. Fetal Cardiac Time Intervals in Healthy Pregnancies—An Observational Study by Fetal ECG (Monica Healthcare System). J. Perinat. Med. 2018, 46, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, B.F.; Sonesson, S.-E.; Levasseur, S.; Moon-Grady, A.J.; Krishnan, A.; Donofrio, M.T.; Raboisson, M.-J.; Hornberger, L.K.; Van Eerden, P.; Sinkovskaya, E.; et al. Home Monitoring for Fetal Heart Rhythm During Anti-Ro Pregnancies. J. Am. Coll. Cardiol. 2018, 72, 1940–1951. [Google Scholar] [CrossRef] [PubMed]
- Sethi, N.; Funamoto, K.; Ingbar, C.; Mass, P.; Moak, J.; Wakai, R.; Strasburger, J.; Donofrio, M.; Khandoker, A.; Kimura, Y.; et al. Noninvasive Fetal Electrocardiography in the Diagnosis of Long QT Syndrome: A Case Series. Fetal Diagn. Ther. 2020, 47, 711–716. [Google Scholar] [CrossRef]
- Roshanitabrizi, P.; Krishnan, A.; Ingbar, C.; Salvador, T.; Zhang, A.; Donofrio, M.T.; Govindan, R. Frequency-Based Maternal Electrocardiogram Attenuation for Fetal Electrocardiogram Analysis. Ann. Biomed. Eng. 2022, 50, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Huang, X.; Wei, C.; Yu, J.; Yu, X.; Dong, C.; Chen, J.; Chen, R.; Wu, X.; Yu, Z.; et al. An Intelligent Quantification System for Fetal Heart Rhythm Assessment: A Multicenter Prospective Study. Heart Rhythm 2024, 21, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Day, T.G.; Kainz, B.; Hajnal, J.; Razavi, R.; Simpson, J.M. Artificial Intelligence, Fetal Echocardiography, and Congenital Heart Disease. Prenat. Diagn. 2021, 41, 733–742. [Google Scholar] [CrossRef]
- Sharma, K.; Masood, S. Deep Learning-Based Non-Invasive Fetal Cardiac Arrhythmia Detection; Springer: Berlin/Heidelberg, Germany, 2021; pp. 511–523. [Google Scholar]
- de Vries, I.R.; van Laar, J.O.E.H.; van der Hout-van der Jagt, M.B.; Clur, S.-A.B.; Vullings, R. Fetal Electrocardiography and Artificial Intelligence for Prenatal Detection of Congenital Heart Disease. Acta Obstet. Gynecol. Scand. 2023, 102, 1511–1520. [Google Scholar] [CrossRef]
- Fouron, J.C.; Proulx, F.; Miró, J.; Gosselin, J. Doppler and M-Mode Ultrasonography to Time Fetal Atrial and Ventricular Contractions. Obstet. Gynecol. 2000, 96, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Fouron, J.-C. Fetal Arrhythmias: The Saint-Justine Hospital Experience. Prenat. Diagn. 2004, 24, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.S.; Prefumo, F.; Ciardelli, V.; Sairam, S.; Bhide, A.; Shinebourne, E.A. Evaluation of Fetal Arrhythmias from Simultaneous Pulsed Wave Doppler in Pulmonary Artery and Vein. Heart 2007, 93, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Howley, L.W.; Schuchardt, E.; Park, D.; Gilbert, L.; Gruenwald, J.; Cuneo, B.F. Simultaneous Recording of Pulsed-Wave Doppler Signals in Innominate Vein and Transverse Aortic Arch: New Technique to Evaluate Atrioventricular Conduction and Fetal Heart Rhythm. Ultrasound Obstet. Gynecol. 2018, 52, 544–545. [Google Scholar] [CrossRef] [PubMed]
- Detterich, J.A.; Pruetz, J.; Sklansky, M.S. Color M-Mode Sonography for Evaluation of Fetal Arrhythmias. J. Ultrasound Med. 2012, 31, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.M. Fetal Arrhythmias. Ultrasound Obstet. Gynecol. 2006, 27, 599–606. [Google Scholar] [CrossRef]
- Wacker-Gussmann, A.; Strasburger, J.F.; Wakai, R.T. Contribution of Fetal Magnetocardiography to Diagnosis, Risk Assessment, and Treatment of Fetal Arrhythmia. J. Am. Heart Assoc. 2022, 11, e025224. [Google Scholar] [CrossRef]
- Strasburger, J.F.; Cheulkar, B.; Wakai, R.T. Magnetocardiography for Fetal Arrhythmias. Heart Rhythm 2008, 5, 1073–1076. [Google Scholar] [CrossRef]
- Stinstra, J.; Golbach, E.; van Leeuwen, P.; Lange, S.; Menendez, T.; Moshage, W.; Schleussner, E.; Kaehler, C.; Horigome, H.; Shigemitsu, S.; et al. Multicentre Study of Fetal Cardiac Time Intervals Using Magnetocardiography. BJOG 2002, 109, 1235–1243. [Google Scholar] [CrossRef]
- Strasburger, J.F.; Wakai, R.T. Fetal Cardiac Arrhythmia Detection and in Utero Therapy. Nat. Rev. Cardiol. 2010, 7, 277–290. [Google Scholar] [CrossRef]
- Strand, S.; Lutter, W.; Strasburger, J.F.; Shah, V.; Baffa, O.; Wakai, R.T. Low-Cost Fetal Magnetocardiography: A Comparison of Superconducting Quantum Interference Device and Optically Pumped Magnetometers. J. Am. Heart Assoc. 2019, 8, e013436. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Kapa, S.; Saarel, E.V.; Dubin, A.M.; Gorenek, B.; Hameed, A.B.; Lara de Melo, S.; Leal, M.A.; Mondésert, B.; Pacheco, L.D.; et al. 2023 HRS Expert Consensus Statement on the Management of Arrhythmias during Pregnancy. Heart Rhythm 2023, 20, e175–e264. [Google Scholar] [CrossRef] [PubMed]




| Digoxin | Sotalol | Flecainide | Amiodarone | |
|---|---|---|---|---|
| Standard Doses (Transplacental) | Loading dose: 375–500 mcg q8 h × 3 doses OR 500 mcg q12 h × 4 doses Maintenance dose: 250–500 mcg bid Goal drug levels: 1.5–2.5 ng/mL Intramuscular digoxin | 240–480 mg daily (120–160 mg bid or tid) Starting dose with hydrops: 160 mg bid | 300 mg daily (100 mg q8 h or 150 mg bid) Goal drug levels: 0.2–1 mcg/mL If using a combination of digoxin and flecainide, decrease digoxin dose by 50% | Loading dose: 600 mg q6–8 h (1800–2400 mg/day) × 2–5 days Maintenance dose: 200–600 mg/day Goal drug levels: 0.7–2.8 mcg/mL If using digoxin or flecainide in combination with amiodarone, decrease doses of digoxin (by 50%) and flecainide. Intraperitoneal amiodarone |
| EKG Effects | Sinus bradycardia First- and second-degree AV block, including nocturnal Wenckebach (Mobitz type I second-degree AV block) | QRS widening (intraventricular conduction delay/bundle branch block) QTc prolongation First-degree AV block | QRS widening QTc prolongation First-degree AV block | QRS widening QTc prolongation Wide P waves Sinus bradycardia First-degree AV block |
| Side Effects | nausea, vomiting, fatigue, blurred vision | nausea, fatigue, dizziness, hypotension | headache, dizziness, visual disturbances (double vision) | nausea, visual disturbances, photosensitivity, rash, gait/coordination/movement problems, peripheral neuropathy/paresthesia thrombocytopenia, maternal/fetal thyroid dysfunction, liver dysfunction |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Killen, S.A.S.; Strasburger, J.F. Diagnosis and Management of Fetal Arrhythmias in the Current Era. J. Cardiovasc. Dev. Dis. 2024, 11, 163. https://doi.org/10.3390/jcdd11060163
Killen SAS, Strasburger JF. Diagnosis and Management of Fetal Arrhythmias in the Current Era. Journal of Cardiovascular Development and Disease. 2024; 11(6):163. https://doi.org/10.3390/jcdd11060163
Chicago/Turabian StyleKillen, Stacy A. S., and Janette F. Strasburger. 2024. "Diagnosis and Management of Fetal Arrhythmias in the Current Era" Journal of Cardiovascular Development and Disease 11, no. 6: 163. https://doi.org/10.3390/jcdd11060163
APA StyleKillen, S. A. S., & Strasburger, J. F. (2024). Diagnosis and Management of Fetal Arrhythmias in the Current Era. Journal of Cardiovascular Development and Disease, 11(6), 163. https://doi.org/10.3390/jcdd11060163