
Multiresistant Kawasaki Disease in a Young Infant with Giant Aneurysms Growing Fast

 , , ,
, , ,
Abstract
1. Background
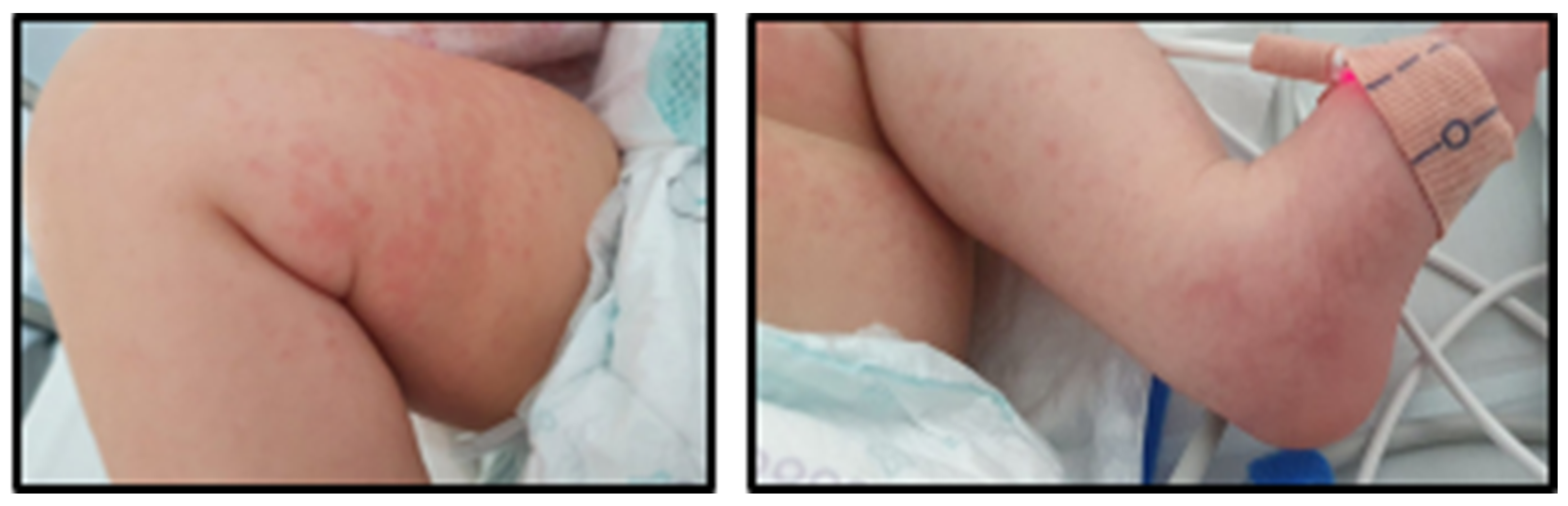
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACE | Angiotensin-converting enzyme |
| ADA2 | Adenosine deaminase 2 |
| AHA | American Heart Association |
| ANA | Antinuclear antibodies |
| ANCA | Anti-neutrophil cytoplasm antibody |
| aPTT | Activated partial thromboplastin time |
| ASA | Acetylsalicylic acid |
| ALT | Alanine transaminase |
| AST | Aspartate transaminase |
| CAA | Coronary artery aneurysm |
| CRP | C-reactive protein |
| CSF | Cerebrospinal fluid |
| DNA | Deoxyribonucleic acid |
| ESR | Erythrocyte sedimentation rate |
| IL-1 | Interleukin-1 |
| IL-6 | Interleukin-6 |
| INR | International normalized ratio |
| IVIg | Intravenous Immunoglobulin |
| KD | Kawasaki disease |
| LAD | Left anterior descending artery |
| LMCA | Left main coronary artery |
| MIS-C | Multisystem inflammatory syndrome in children |
| MPN | Methylprednisolone |
| MPNp | Methylprednisolone pulses |
| PCR | Polymerase chain reaction |
| PDN | Prednisolone |
| RCA | Right coronary artery |
| TNF | Tumor necrosis factor |
References
- Weiss, P.F. Pediatric Vasculitis. Pediatr. Clin. N. Am. 2012, 59, 407–423. [Google Scholar] [CrossRef] [PubMed]
- James, K.E.; Kalot, M.A.; Husainat, N.M.; Dua, A.B.; Byram, K.; Springer, J.M.; Lin, Y.C.; Turgunbaev, M.; Villa-Forte, A.; Gorelik, M.; et al. Kawasaki Disease: A Systematic Review and Meta-Analysis of Benefits and Harms of Common Treatments. ACR Open Rheumatol. 2021, 3, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Shulman, S.T.; Rowley, A.H. Kawasaki disease: Insights into pathogenesis and approaches to treatment. Nat. Rev. Rheumatol. 2015, 11, 475–482. [Google Scholar] [CrossRef]
- Sundel, R.P. Kawasaki disease. Rheum. Dis. Clin. N. Am. 2015, 41, 1738–1749. [Google Scholar] [CrossRef]
- Patil, S.; Shirodkar, S.; Pinto, R.; Dalvi, B. Giant coronary artery aneurysm with a thrombus secondary to Kawasaki disease. Ann. Pediatr. Cardiol. 2008, 1, 59–61. [Google Scholar] [CrossRef]
- Noval Rivas, M.; Arditi, M. Kawasaki disease: Pathophysiology and insights from mouse models. Nat. Rev. Rheumatol. 2020, 16, 391–405. [Google Scholar] [CrossRef]
- Thadchanamoorthy, V.; Dayasiri, K. Refractory Kawasaki Disease Presenting with Erythema at Bacille Calmette-Guérin Inoculation Site: A Paediatric Case Report. Cureus 2020, 12, e10928. [Google Scholar] [CrossRef]
- Garrido-García, L.M.; Morán-Villaseñor, E.; Yamazaki-Nakashimada, M.A.; Cravioto, P.; Galván, F. Giant coronary artery aneurysms complicating Kawasaki disease in Mexican children. Cardiol. Young 2018, 28, 386–390. [Google Scholar] [CrossRef] [PubMed]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- Abraham, D.; Kalyanasundaram, S.; Krishnamurthy, K. Refractory Kawasaki Disease—A Challenge for the Pediatrician. SN Compr. Clin. Med. 2021, 3, 855–860. [Google Scholar] [CrossRef]
- Gambacorta, A.; Buonsenso, D.; De Rosa, G.; Lazzareschi, I.; Gatto, A.; Brancato, F.; Pata, D.; Valentini, P. Resolution of Giant Coronary Aneurisms in a Child with Refractory Kawasaki Disease Treated with Anakinra. Front. Pediatr. 2020, 8, 195. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.; Nagaraju, L.; Gorelik, M. Complete Regression of Giant Aneurysms in an Infant with Delayed Diagnosis and Refractory Kawasaki Disease via Combination Anticytokine Therapy: Case Report and Review of Similar Cases. Case Rep. Rheumatol. 2020, 2020, 6249013. [Google Scholar] [CrossRef] [PubMed]
- Walser, M.; Hermann, M.; Hufnagel, M.; Haas, N.A.; Fischer, M.; Dalla-Pozza, R.; Jakob, A. Anakinra And Etanercept Combination Treatment in a Child with Severe, Nonresponsive Kawasaki Disease. Pediatr. Infect. Dis. J. 2020, 39, e310–e313. [Google Scholar] [CrossRef] [PubMed]
- Saneeymehri, S.; Baker, K.; So, T.Y. Overview of pharmacological treatment options for pediatric patients with refractory kawasaki disease. J. Pediatr. Pharmacol. Ther. 2015, 20, 163–177. [Google Scholar] [CrossRef] [PubMed]
- Buda, P.; Friedman-Gruszczyńska, J.; Książyk, J. Anti-inflammatory Treatment of Kawasaki Disease: Comparison of Current Guidelines and Perspectives. Front. Med. 2021, 8, 738850. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Liu, L.; Huang, X.; Tian, J. Insights Into Coronary Artery Lesions in Kawasaki Disease. Front. Pediatr. 2020, 8, 493. [Google Scholar] [CrossRef] [PubMed]
- Wood, K.P.; Lee, G.S.; Li, J.S.; Barker, P.C.A.; Van Mater, H.; Chamberlain, R.C. Coronary Artery Aneurysm Rupture in Kawasaki Disease and SARS-CoV-2 Infection. CASE 2024, 8, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Peña-Juárez, A.; Medina-Andrade, M.A.; Olivares, I.E.R.; Colín-Ortíz, J.L.; Yamazaki-Nakashimada, M.A.; Garrido-Garcia, L.M. Multiresistant Kawasaki Disease Complicated with Facial Nerve Palsy, Bilateral Giant Coronary Artery Aneurysms, and Stenosis of the Right Coronary Artery in an Infant. J. Clin. Rheumatol. 2021, 27, S351–S354. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Zhang, Y.Y.; Yu, H.G. Clinical Manifestations of Kawasaki Disease Shock Syndrome. Clin. Pediatr. 2018, 57, 428–435. [Google Scholar] [CrossRef]
- Gamez-Gonzalez, L.B.; Moribe-Quintero, I.; Cisneros-Castolo, M.; Varela-Ortiz, J.; Muñoz-Ramírez, M.; Garrido-García, M.; Yamazaki-Nakashimada, M. Kawasaki disease shock syndrome: Unique and severe subtype of Kawasaki disease. Pediatr. Int. 2018, 60, 781–790. [Google Scholar] [CrossRef]
- Yalta, K.; Yalta, T.; Yetkin, E.; Ozturk, C. Late coronary aneurysm formation after Kawasaki disease: A review of mechanistic and clinical aspects. Korean Circ. J. 2021, 51, 837. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.C.; Liu, H.M.; Lin, M.T.; Chen, C.A.; Chiu, S.N.; Lu, C.W.; Chang, L.Y.; Wang, J.K.; Wu, M.H. Outcomes of Kawasaki disease children with spontaneous defervescence within 10 days. Front. Pediatr. 2019, 7, 158. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; He, X.; Zhang, L.; Wang, Z.; Wang, Y.; Lin, H.; Yuan, J.; Xie, X.; Qin, Y.; Huang, P. A Retrospective Cohort Study of Intravenous Immunoglobulin Therapy in the Acute Phase of Kawasaki Disease: The Earlier, the Better? Cardiovasc. Ther. 2021, 2021, 6660407. [Google Scholar] [CrossRef] [PubMed]
- Scherler, L.; Haas, N.A.; Tengler, A.; Pattathu, J.; Mandilaras, G.; Jakob, A. Acute phase of Kawasaki disease: A review of national guideline recommendations. Eur. J. Pediatr. 2022, 181, 2563–2573. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Qiu, H.; Wen, Z.; Shi, H.; Yu, H.; Li, J.; Zhang, Q.; Wang, J.; Rong, X.; Wu, R.; et al. Albumin level and progression of coronary artery lesions in Kawasaki disease: A retrospective cohort study. Front. Pediatr. 2022, 10, 947059. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Sugimura, T.; Akagi, T.; Sato, N.; Hashino, K.; Maeno, Y.; Kazue, T.; Eto, G.; Yamakawa, R. Long-term Consequences of Kawasaki Disease. Circulation 1996, 94, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M.; Shulman, S.T. Kawasaki disease: A comprehensive review of treatment options. J. Clin. Pharm. Ther. 2015, 40, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Blonz, G.; Lacroix, S.; Benbrik, N.; Warin-Fresse, K.; Masseau, A.; Trewick, D.; Hamidou, M.; Stephan, J.L.; Néel, A. Severe Late-Onset Kawasaki Disease Successfully Treated with Anakinra. J. Clin. Rheumatol. 2020, 26, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Manubens, J.; Gelman, A.; Franch, N.; Teodoro, S.; Palacios, J.R.; Rudi, N.; Rivera, J.; Antón, J. A child with resistant Kawasaki disease successfully treated with anakinra: A case report. BMC Pediatr. 2017, 17, 102. [Google Scholar] [CrossRef]
- Ferrara, G.; Giani, T.; Caparello, M.C.; Farella, C.; Gamalero, L.; Cimaz, R. Anakinra for Treatment-Resistant Kawasaki Disease: Evidence from a Literature Review. Pediatr. Drugs 2020, 22, 645–652. [Google Scholar] [CrossRef]
- Youn, Y.; Kim, J.; Hong, Y.M.; Sohn, S. Infliximab as the first retreatment in patients with Kawasaki disease resistant to initial intravenous immunoglobulin. Pediatr. Infect. Dis. J. 2016, 35, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Boudiaf, H. Super Giant Coronary Aneurysm in an Algerian Boy with Kawasaki Disease. Int. J. Pediatr. Res. 2016, 2, 021. [Google Scholar] [CrossRef]
- Lee, J.; Kim, G.B.; Kwon, B.S.; Bae, E.J.; Noh, C., II. Two cases of super-giant coronary aneurysms after Kawasaki disease. Korean Circ. J. 2014, 44, 54. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.-Y.; Zhang, M.; Ko, S.; Chen, F. An Update on Cardiovascular Risk Factors after Kawasaki Disease. Front. Cardiovasc. Med. 2021, 8, 671198. [Google Scholar] [CrossRef] [PubMed]
- Newburger, J.W.; Takahashi, M.; Gerber, M.A.; Gewitz, M.H.; Tani, L.Y.; Burns, J.C.; Shulman, S.T.; Bolger, A.F.; Ferrieri, P.; Baltimore, R.S.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004, 110, 2747–2771. [Google Scholar] [CrossRef] [PubMed]
- Suganuma, E.; Niimura, F.; Matsuda, S.; Ukawa, T.; Nakamura, H.; Sekine, K.; Kato, M.; Aiba, Y.; Koga, Y.; Hayashi, K.; et al. Losartan attenuates the coronary perivasculitis through its local and systemic anti-inflammatory properties in a murine model of Kawasaki disease. Pediatr. Res. 2017, 81, 593–600. [Google Scholar] [CrossRef]
- Fukazawa, R.; Kobayashi, J.; Ayusawa, M.; Hamada, H.; Miura, M.; Mitani, Y.; Tsuda, E.; Nakajima, H.; Matsuura, H.; Ikeda, K.; et al. JCS/JSCS 2020 Guideline on Diagnosis and Management of Cardiovascular Sequelae in Kawasaki Disease. Circ. J. 2020, 84, 1348–1407. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Infectiology Unit | Cardiology Unit | Follow-Up (Months after Discharge) | ||||||
|---|---|---|---|---|---|---|---|---|
| D16 | D19 | D29 | D36 | D69 | 1 Month | 4 Months * | 17 Months | |
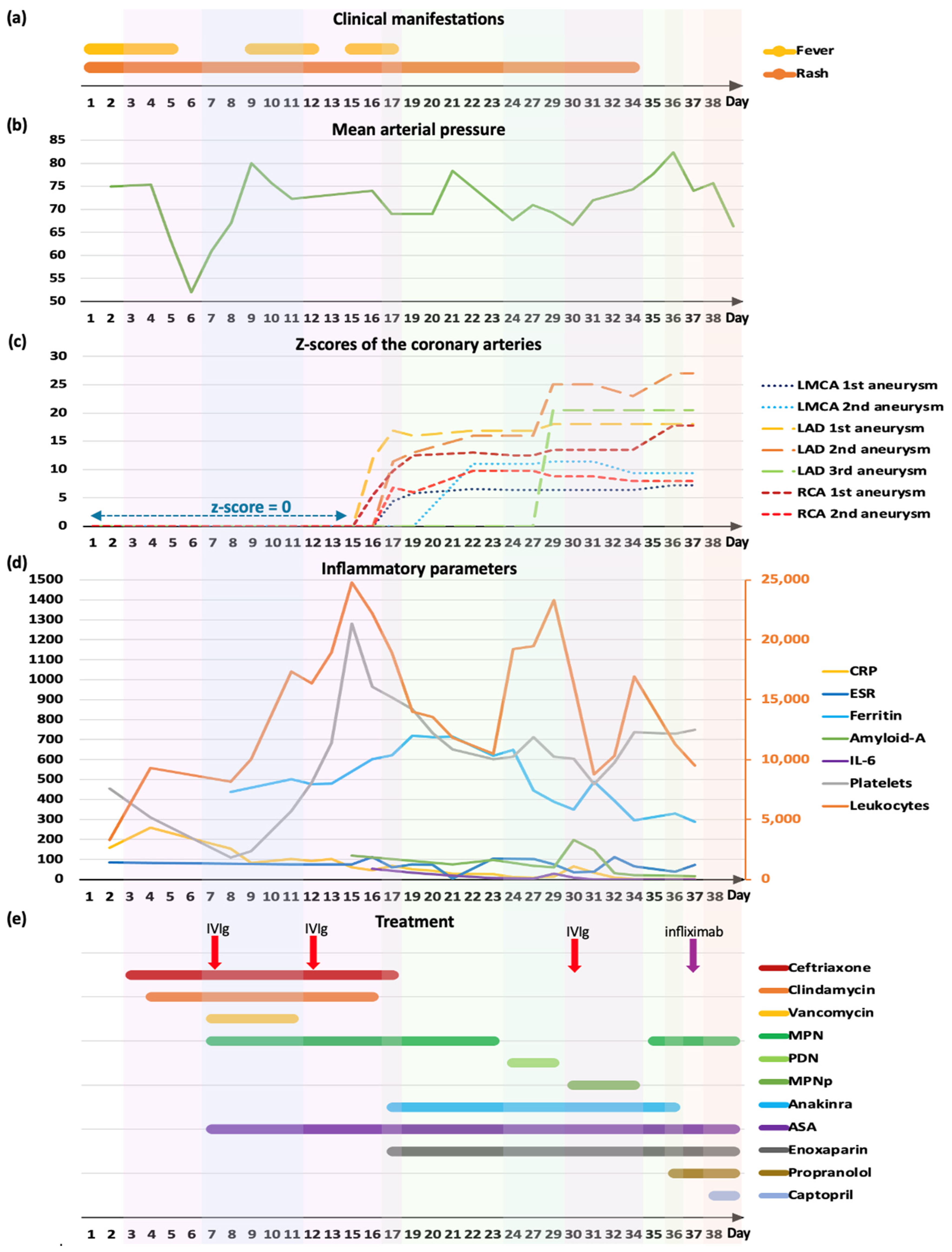
| LMCA | Ø | 1st 4 mm (z-score +5.8) | 1st 4.2 mm (z-score +6.4) | 1st 4.5 mm (z-score +7.2) | 1st 4 mm (z-score +5.8) | Ø | Ø | Ø |
| Ø | 2nd 6 mm (z-score +11.4) | 2nd 5.3 mm (z-score +9.4) | 2nd 5.5 mm (z-score +10) | |||||
| LAD | 1st 4.2 mm (z-score +12) | 1st 5 mm (z-score +16) | 1st 5.5 mm (z-score +18) | 1st 5.5 mm (z-score +18) | 1st 5.5 mm (z-score +18) | 1st 5.4 mm (z-score +17.8) | 2 aneurysms max diameter 4.5 mm (z-score +13.7) | 1st 3.6 mm (z-score +9.6) |
| Ø | 2nd 4.4 mm (z-score +13) | 2nd 7 mm (z-score +25) | 2nd 7.5 mm (z-score +27) | 2nd 6.8 mm (z-score +24) | 2nd 6.6 mm (z-score +23) | Ø | ||
| Ø | Ø | 3rd 6 mm (z-score +20.5) | 3rd 6 mm (z-score +20.5) | Ø | Ø | Ø | Ø | |
| RCA | 1st 3.1 mm (z-score +5.5) | 1st 5.2 mm (z-score +12.5) | 1st 5.5 mm (z-score +13.5) | 1st 6.8 mm (z-score +17.8) | 1st 7 mm (z-score +18.5) | 5.4 mm (z-score +13) | Max diameter 3.4 mm (z-score +6.5) | 1st 3.5 mm (z-score +6.8) |
| Ø | 2nd 3.2 mm (z-score +6) | 2nd 4.1 mm (z-score +8.8) | 2nd 3.9 mm (z-score +8) | Ø | Ø | Ø | Ø | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amorim-Figueiredo, R.; Pereira Lemos, A.; Rito, T.; Conde, M.; Brito, M.J.; Pinto, F. Multiresistant Kawasaki Disease in a Young Infant with Giant Aneurysms Growing Fast. J. Cardiovasc. Dev. Dis. 2024, 11, 149. https://doi.org/10.3390/jcdd11050149
Amorim-Figueiredo R, Pereira Lemos A, Rito T, Conde M, Brito MJ, Pinto F. Multiresistant Kawasaki Disease in a Young Infant with Giant Aneurysms Growing Fast. Journal of Cardiovascular Development and Disease. 2024; 11(5):149. https://doi.org/10.3390/jcdd11050149
Chicago/Turabian StyleAmorim-Figueiredo, Rosa, Ana Pereira Lemos, Tiago Rito, Marta Conde, Maria João Brito, and Fátima Pinto. 2024. "Multiresistant Kawasaki Disease in a Young Infant with Giant Aneurysms Growing Fast" Journal of Cardiovascular Development and Disease 11, no. 5: 149. https://doi.org/10.3390/jcdd11050149
APA StyleAmorim-Figueiredo, R., Pereira Lemos, A., Rito, T., Conde, M., Brito, M. J., & Pinto, F. (2024). Multiresistant Kawasaki Disease in a Young Infant with Giant Aneurysms Growing Fast. Journal of Cardiovascular Development and Disease, 11(5), 149. https://doi.org/10.3390/jcdd11050149