
Trends in Medical and Device Therapies Following Incident Heart Failure in Denmark during 1996–2019: A Nationwide Register-Based Follow-Up Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Population and Data Sources
2.2. Study Variables
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Characteristics
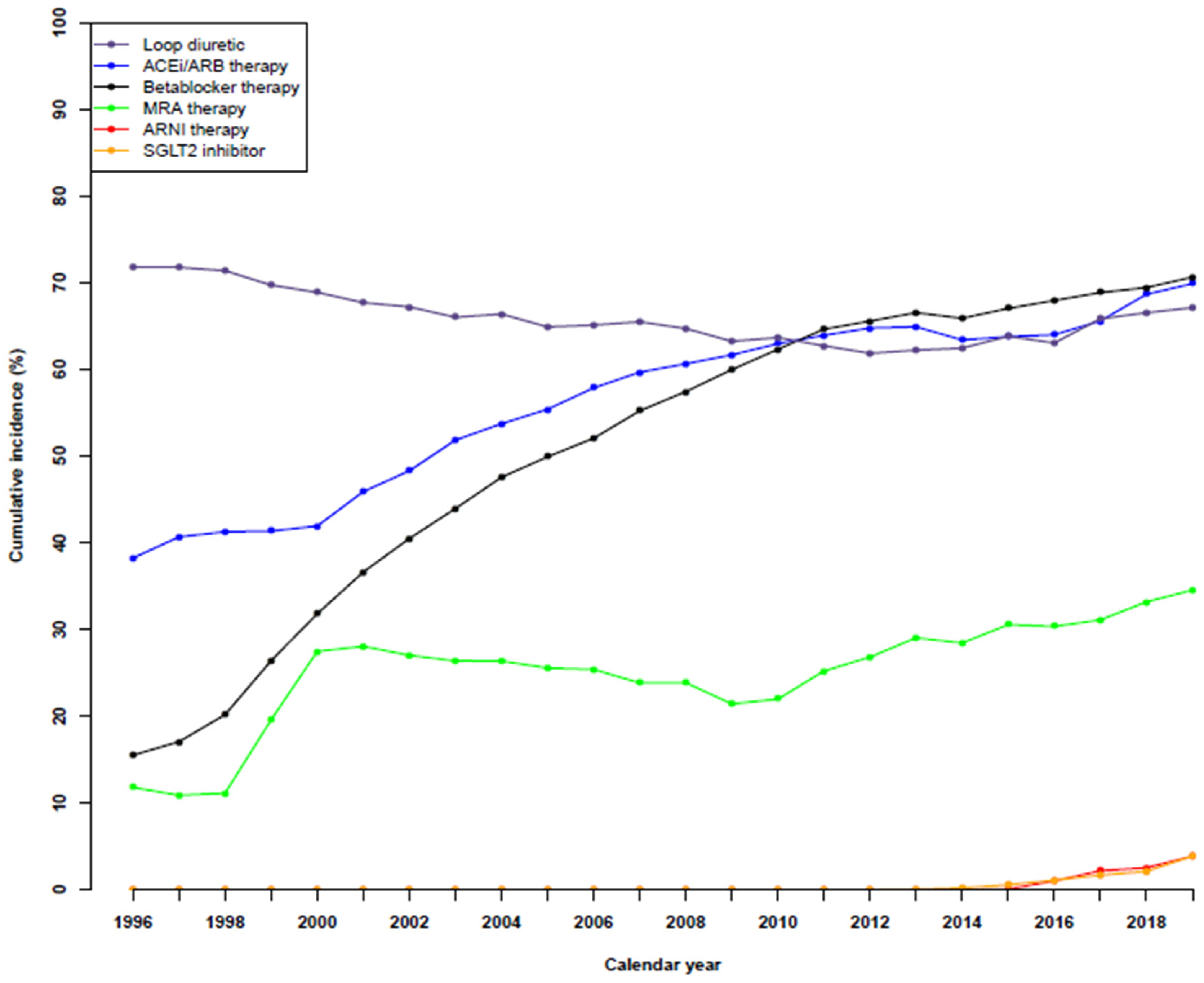
3.3. Temporal Trends in Guideline-Based HF Medical Therapies
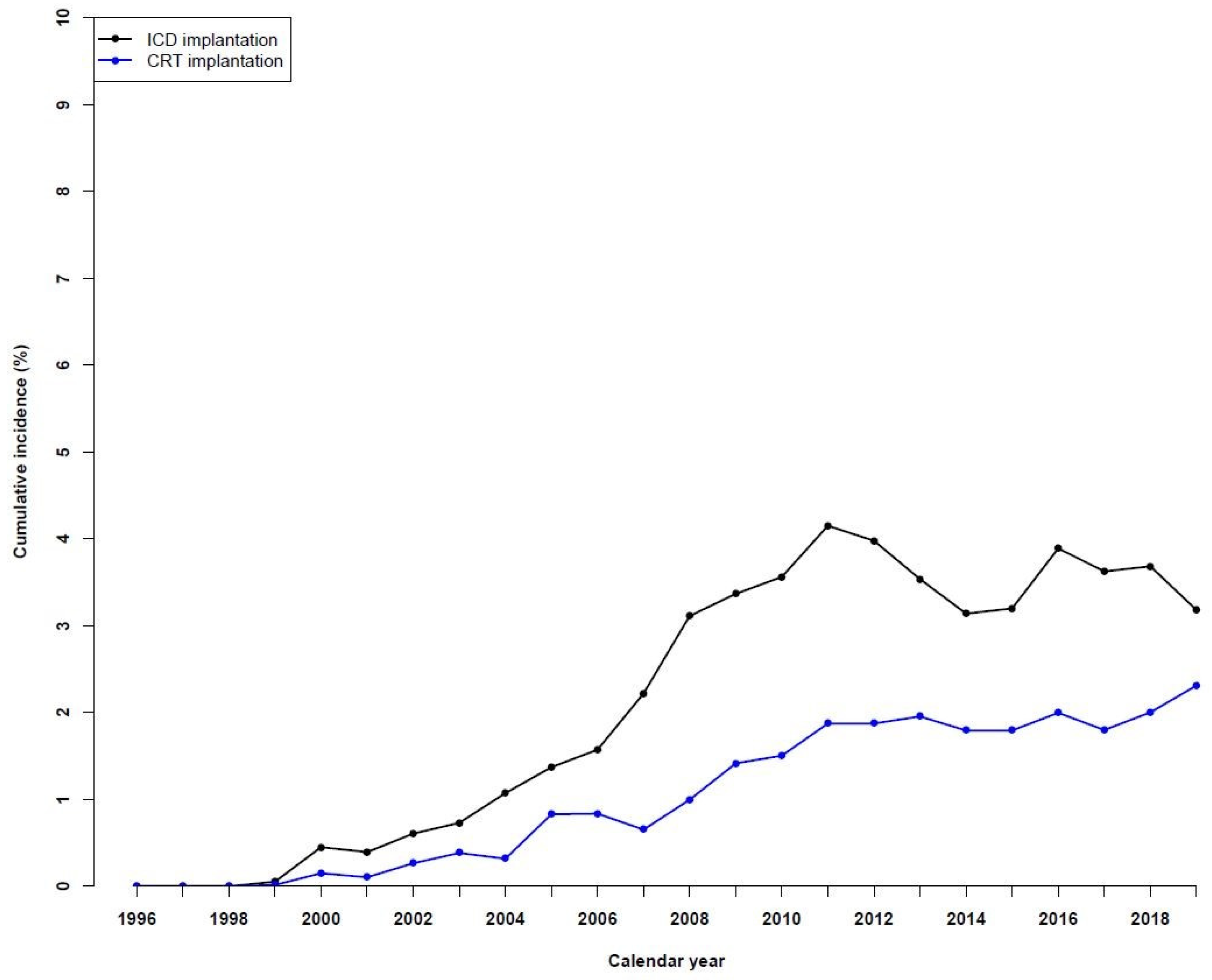
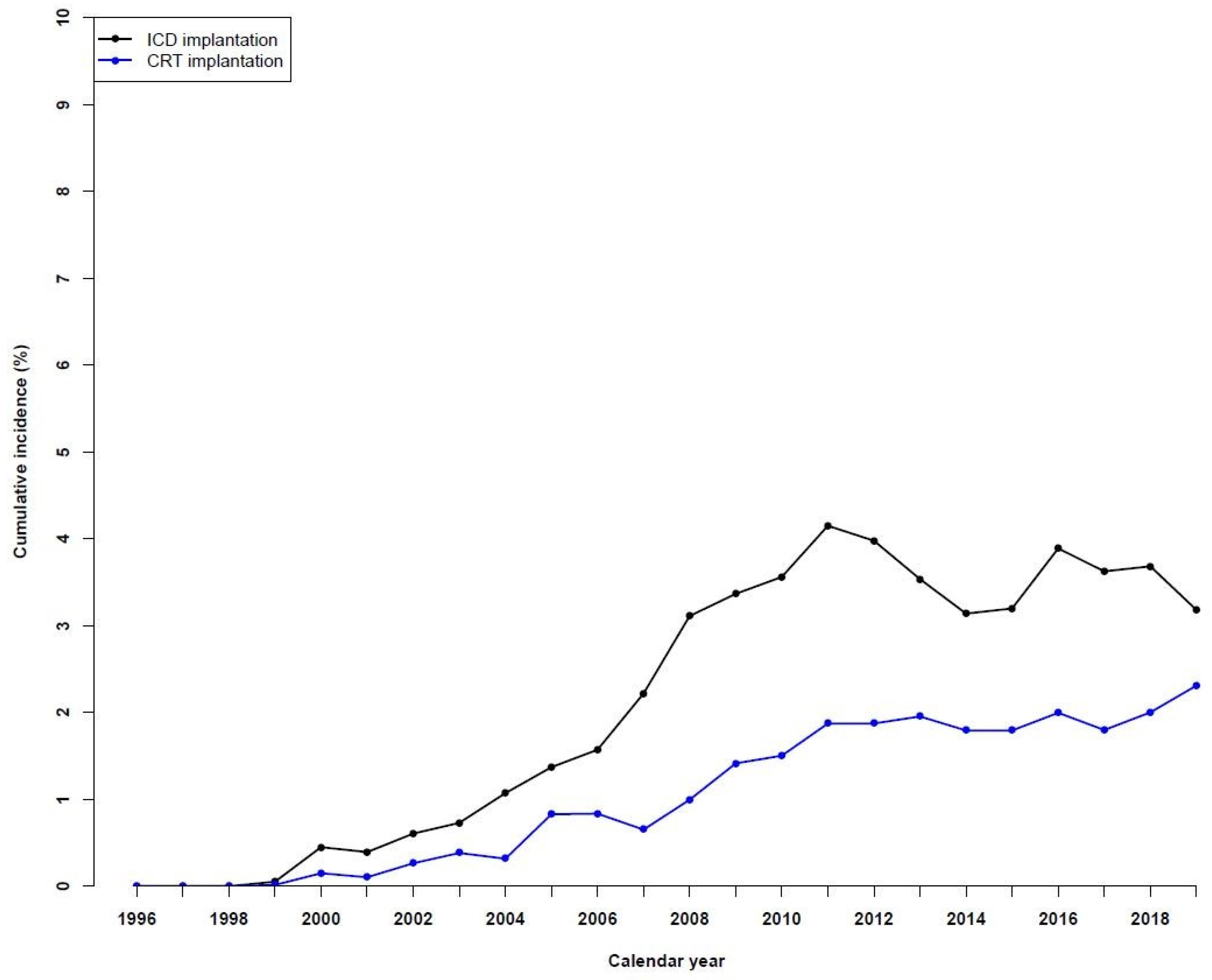
3.4. Temporal Trends in ICD and CRT Device Use
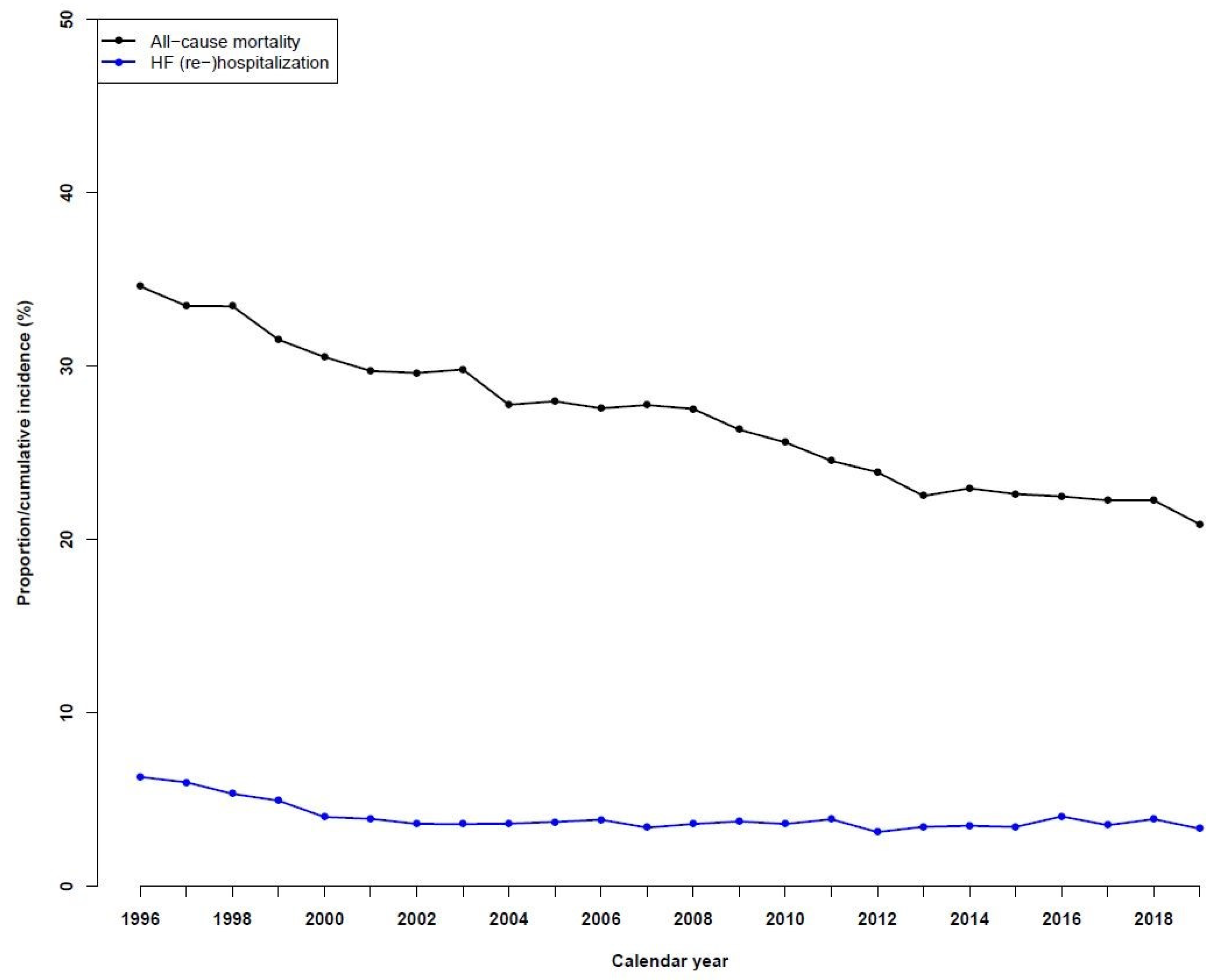
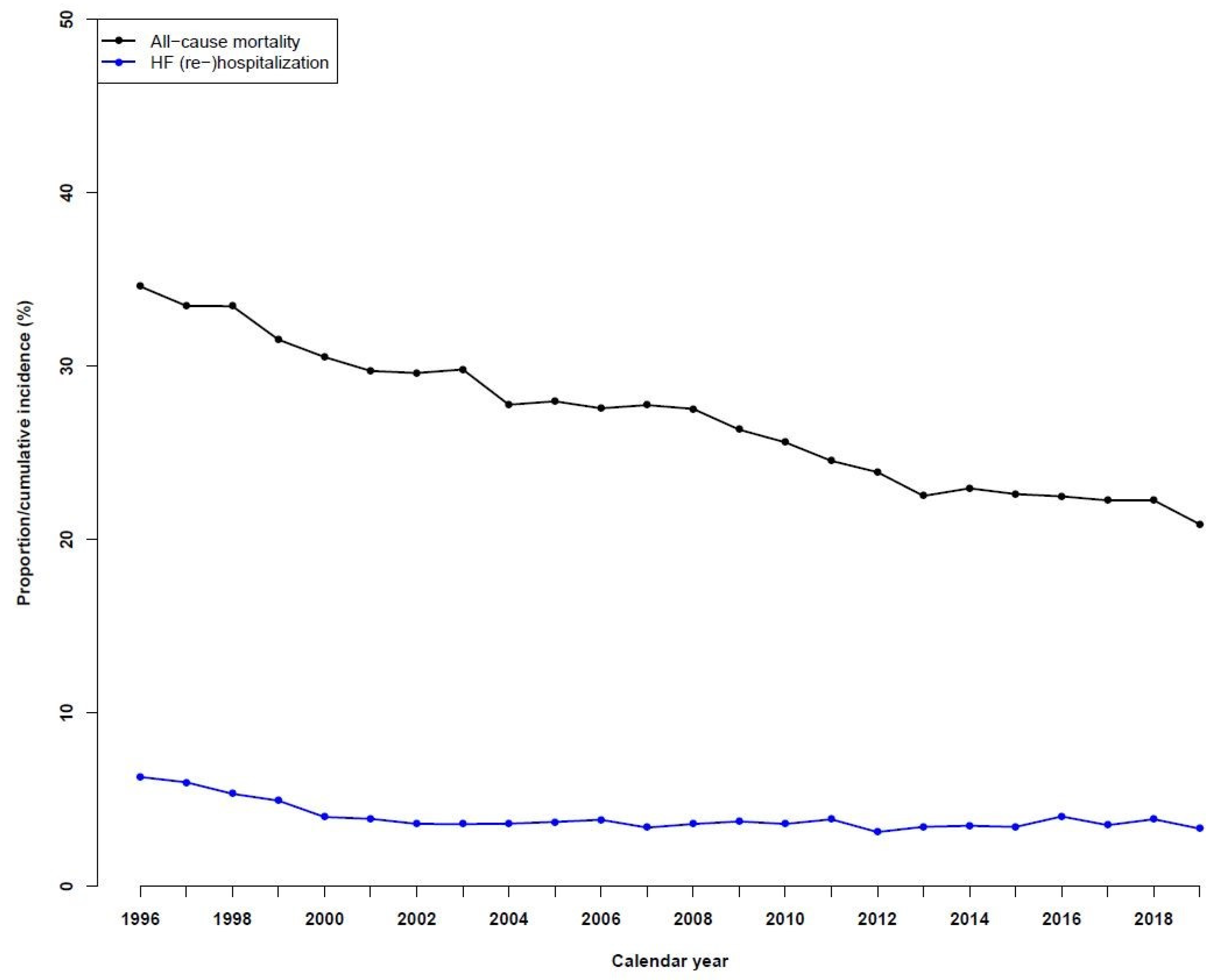
3.5. Temporal Trends in One-Year All-Cause Mortality and HF Rehospitalizations
3.6. Sensitivity Analysis in Patients Treated with a Beta-Blocker and an ACEi/ARB in Combination
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N. Engl. J. Med. 1987, 316, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): A randomised trial. Lancet 1999, 353, 9–13. [Google Scholar] [CrossRef]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N. Engl. J. Med. 1999, 341, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, C.; Cazeau, S.; Le Breton, H.; Ritter, P.; Mabo, P.; Gras, D.; Pavin, D.; Lazarus, A.; Daubert, J.-C. Acute hemodynamic effects of biventricular DDD pacing in patients with end-stage heart failure. J. Am. Coll. Cardiol. 1998, 32, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Pharm, D.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Ulrichsen, S.P.; Pedersen, L.; Bøtker, H.E.; Sørensen, H.T. Thirty-year trends in heart failure hospitalization and mortality rates and the prognostic impact of co-morbidity: A Danish nationwide cohort study. Eur. J. Heart Fail. 2016, 18, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.B. The Danish Civil Registration System. Scand. J. Public Health 2011, 39 (Suppl. S7), 22–25. [Google Scholar] [CrossRef] [PubMed]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39 (Suppl. S7), 30–33. [Google Scholar] [CrossRef] [PubMed]
- Kildemoes, H.W.; Sørensen, H.T.; Hallas, J. The Danish National Prescription Registry. Scand. J. Public Health 2011, 39 (Suppl. S7), 38–41. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, S.K.; Christiansen, C.F.; Christensen, S.; Lash, T.L.; Sørensen, H.T. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med. Res. Methodol. 2011, 11, 83. [Google Scholar] [CrossRef] [PubMed]
- Madelaire, C.; Gustafsson, F.; Køber, L.; Torp-Pedersen, C.; Andersson, C.; Kristensen, S.L.; Gislason, G.; Schou, M. Identification of Patients with New-Onset Heart Failure and Reduced Ejection Fraction in Danish Administrative Registers. Clin. Epidemiol. 2020, 12, 589–594. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Zahir, D.; Bonde, A.; Madelaire, C.; Malmborg, M.; Butt, J.H.; Fosbol, E.; Gislason, G.; Torp-Pedersen, C.; Andersson, C.; Rossignol, P.; et al. Temporal trends in initiation of mineralocorticoid receptor antagonists and risk of subsequent withdrawal in patients with heart failure: A nationwide study in Denmark from 2003–2017. Eur. J. Heart Fail. 2021, 24, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.L.; Goode, K.; Cleland, J.G.F. The prevalence and incidence of left bundle branch block in ambulant patients with chronic heart failure. Eur. J. Heart Fail. 2008, 10, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.G.F.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.S.L.; Wells, G.A.; Talajic, M.; Arnold, M.O.; Sheldon, R.; Connolly, S.; Hohnloser, S.H.; Nichol, G.; Birnie, D.H.; Sapp, J.L.; et al. Cardiac-Resynchronization Therapy for Mild-to-Moderate Heart Failure. N. Engl. J. Med. 2010, 363, 2385–2395. [Google Scholar] [CrossRef] [PubMed]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.A.M., III; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| 1996 | 1997 | 1998 | 1999 | 2000 | 2001 | 2002 | 2003 | |
| Variable | n = 12,209 | n = 11,736 | n = 12,555 | n = 13,277 | n = 14,655 | n = 14,478 | n = 14,344 | n = 13,559 |
| Age, median [Q1, Q3] | 77 [69, 84] | 77 [69, 84] | 77 [69, 84] | 77 [68, 84] | 77 [68, 84] | 77 [68, 84] | 77 [68, 84] | 77 [67, 84] |
| Male sex, n% | 6284 (51.5) | 6037 (51.4) | 6456 (51.4) | 6914 (52.1) | 7593 (51.8) | 7367 (50.9) | 7413 (51.7) | 7170 (52.9) |
| In-patient, n% | 9847 (80.7) | 9440 (80.4) | 9893 (78.8) | 10,030 (75.5) | 10,888 (74.3) | 10,474 (72.3) | 10,136 (70.7) | 9244 (68.2) |
| Hypertension, n% | 3083 (25.3) | 3486 (29.7) | 4269 (34.0) | 4857 (36.6) | 5882 (40.1) | 6302 (43.5) | 6803 (47.4) | 6808 (50.2) |
| Diabetes, n% | 1528 (12.5) | 1503 (12.8) | 1660 (13.2) | 1728 (13.0) | 1972 (13.5) | 1948 (13.5) | 2087 (14.5) | 1936 (14.3) |
| COPD, n% | 1749 (14.3) | 1752 (14.9) | 1872 (14.9) | 2160 (16.3) | 2339 (16.0) | 2444 (16.9) | 2452 (17.1) | 2267 (16.7) |
| Previous MI, n% | 1955 (16.0) | 1925 (16.4) | 1999 (15.9) | 2154 (16.2) | 2429 (16.6) | 2401 (16.6) | 2583 (18.0) | 2463 (18.2) |
| IHD, n% | 3437 (28.2) | 3374 (28.7) | 3685 (29.4) | 3937 (29.7) | 4400 (30.0) | 4433 (30.6) | 4664 (32.5) | 4518 (33.3) |
| Previous ICD, n% | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 9 (0.1) | 22 (0.2) | 21 (0.1) | 52 (0.4) |
| CKD, n% | 218 (1.8) | 249 (2.1) | 297 (2.4) | 320 (2.4) | 410 (2.8) | 435 (3.0) | 536 (3.7) | 525 (3.9) |
| Stroke, n% | 1395 (11.4) | 1323 (11.3) | 1459 (11.6) | 1496 (11.3) | 1666 (11.4) | 1678 (11.6) | 1685 (11.7) | 1614 (11.9) |
| PAD, n% | 1008 (8.3) | 906 (7.7) | 1052 (8.4) | 1072 (8.1) | 1273 (8.7) | 1202 (8.3) | 1278 (8.9) | 1164 (8.6) |
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | |
| Variable | n = 13,247 | n = 12,544 | n = 11,958 | n = 11,803 | n = 11,439 | n = 11,166 | n = 11,371 | n = 11,154 |
| Age, median [Q1, Q3] | 77 [67, 84] | 77 [66, 84] | 76 [66, 84] | 76 [65, 84] | 76 [65, 84] | 76 [66, 84] | 76 [65, 84] | 75 [65, 84] |
| Male sex, n% | 7021 (53.0) | 6777 (54.0) | 6562 (54.9) | 6496 (55.0) | 6395 (55.9) | 6258 (56.0) | 6429 (56.5) | 6403 (57.4) |
| In-patient, n% | 8840 (66.7) | 8129 (64.8) | 7331 (61.3) | 7251 (61.4) | 6945 (60.7) | 6376 (57.1) | 6247 (54.9) | 5938 (53.2) |
| Hypertension, n% | 6955 (52.5) | 7028 (56.0) | 6833 (57.1) | 6952 (58.9) | 7066 (61.8) | 7146 (64.0) | 7254 (63.8) | 7250 (65.0) |
| Diabetes, n% | 2018 (15.2) | 2034 (16.2) | 1930 (16.1) | 1948 (16.5) | 2031 (17.8) | 2052 (18.4) | 2216 (19.5) | 2179 (19.5) |
| COPD, n% | 2275 (17.2) | 2119 (16.9) | 2084 (17.4) | 2014 (17.1) | 1977 (17.3) | 1958 (17.5) | 2043 (18.0) | 2074 (18.6) |
| Previous MI, n% | 2587 (19.5) | 2455 (19.6) | 2411 (20.2) | 2378 (20.1) | 2282 (19.9) | 2262 (20.3) | 2434 (21.4) | 2372 (21.3) |
| IHD, n% | 4697 (35.5) | 4439 (35.4) | 4336 (36.3) | 4212 (35.7) | 4112 (35.9) | 4113 (36.8) | 4291 (37.7) | 4230 (37.9) |
| Previous ICD, n% | 53 (0.4) | 61 (0.5) | 66 (0.6) | 101 (0.9) | 115 (1.0) | 96 (0.9) | 129 (1.1) | 112 (1.0) |
| CKD, n% | 546 (4.1) | 558 (4.4) | 564 (4.7) | 591 (5.0) | 625 (5.5) | 669 (6.0) | 685 (6.0) | 708 (6.3) |
| Stroke, n% | 1621 (12.2) | 1583 (12.6) | 1490 (12.5) | 1491 (12.6) | 1474 (12.9) | 1434 (12.8) | 1501 (13.2) | 1431 (12.8) |
| PAD, n% | 1225 (9.2) | 1214 (9.7) | 1134 (9.5) | 1083 (9.2) | 1059 (9.3) | 1106 (9.9) | 1161 (10.2) | 1180 (10.6) |
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |
| Variable | n = 11,310 | n = 11,507 | n = 11,370 | n = 11,816 | n = 11,515 | n = 11,169 | n = 10,287 | n = 11,251 |
| Age, median [Q1, Q3] | 75 [65, 84] | 75 [65, 83] | 75 [66, 83] | 75 [66, 84] | 75 [66, 83] | 75 [66, 84] | 75 [66, 83] | 75 [65, 83] |
| Male sex, n% | 6612 (58.5) | 6780 (58.9) | 6647 (58.5) | 6930 (58.6) | 6745 (58.6) | 6587 (59.0) | 6236 (60.6) | 6725 (59.8) |
| In-patient, n% | 5643 (49.9) | 5495 (47.8) | 5409 (47.6) | 5570 (47.1) | 5487 (47.7) | 5032 (45.1) | 4541 (44.1) | 5589 (49.7) |
| Hypertension, n% | 7445 (65.8) | 7640 (66.4) | 7630 (67.1) | 7855 (66.5) | 7665 (66.6) | 7525 (67.4) | 6715 (65.3) | 7462 (66.3) |
| Diabetes, n% | 2296 (20.3) | 2387 (20.7) | 2309 (20.3) | 2484 (21.0) | 2410 (20.9) | 2368 (21.2) | 2082 (20.2) | 2370 (21.1) |
| COPD, n% | 1988 (17.6) | 2046 (17.8) | 2121 (18.7) | 2120 (17.9) | 2151 (18.7) | 2103 (18.8) | 1909 (18.6) | 2029 (18.0) |
| Previous MI, n% | 2380 (21.0) | 2256 (19.6) | 2237 (19.7) | 2293 (19.4) | 2144 (18.6) | 1977 (17.7) | 1807 (17.6) | 1808 (16.1) |
| IHD, n% | 4249 (37.6) | 4143 (36.0) | 4065 (35.8) | 4125 (34.9) | 3892 (33.8) | 3623 (32.4) | 3213 (31.2) | 3272 (29.1) |
| Previous ICD, n% | 154 (1.4) | 144 (1.3) | 161 (1.4) | 156 (1.3) | 157 (1.4) | 155 (1.4) | 134 (1.3) | 212 (1.9) |
| CKD, n% | 818 (7.2) | 828 (7.2) | 881 (7.7) | 941 (8.0) | 908 (7.9) | 915 (8.2) | 863 (8.4) | 859 (7.6) |
| Stroke, n% | 1522 (13.5) | 1391 (12.1) | 1375 (12.1) | 1496 (12.7) | 1438 (12.5) | 1349 (12.1) | 1167 (11.3) | 1182 (10.5) |
| PAD, n% | 1132 (10.0) | 1204 (10.5) | 1193 (10.5) | 1258 (10.6) | 1181 (10.3) | 1137 (10.2) | 1007 (9.8) | 1016 (9.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ettrup-Christensen, A.; Butt, J.H.; Andersen, M.P.; Sessa, M.; Polcwiartek, C.; Fosbøl, E.L.; Rørth, R.; Kristensen, S.L.; Torp-Pedersen, C.; Køber, L.; et al. Trends in Medical and Device Therapies Following Incident Heart Failure in Denmark during 1996–2019: A Nationwide Register-Based Follow-Up Study. J. Cardiovasc. Dev. Dis. 2023, 10, 362. https://doi.org/10.3390/jcdd10090362
Ettrup-Christensen A, Butt JH, Andersen MP, Sessa M, Polcwiartek C, Fosbøl EL, Rørth R, Kristensen SL, Torp-Pedersen C, Køber L, et al. Trends in Medical and Device Therapies Following Incident Heart Failure in Denmark during 1996–2019: A Nationwide Register-Based Follow-Up Study. Journal of Cardiovascular Development and Disease. 2023; 10(9):362. https://doi.org/10.3390/jcdd10090362
Chicago/Turabian StyleEttrup-Christensen, Asbjørn, Jawad H. Butt, Mikkel Porsborg Andersen, Maurizio Sessa, Christoffer Polcwiartek, Emil L. Fosbøl, Rasmus Rørth, Søren L. Kristensen, Christian Torp-Pedersen, Lars Køber, and et al. 2023. "Trends in Medical and Device Therapies Following Incident Heart Failure in Denmark during 1996–2019: A Nationwide Register-Based Follow-Up Study" Journal of Cardiovascular Development and Disease 10, no. 9: 362. https://doi.org/10.3390/jcdd10090362
APA StyleEttrup-Christensen, A., Butt, J. H., Andersen, M. P., Sessa, M., Polcwiartek, C., Fosbøl, E. L., Rørth, R., Kristensen, S. L., Torp-Pedersen, C., Køber, L., Schou, M., Tayal, B., Søgaard, P., & Kragholm, K. (2023). Trends in Medical and Device Therapies Following Incident Heart Failure in Denmark during 1996–2019: A Nationwide Register-Based Follow-Up Study. Journal of Cardiovascular Development and Disease, 10(9), 362. https://doi.org/10.3390/jcdd10090362