
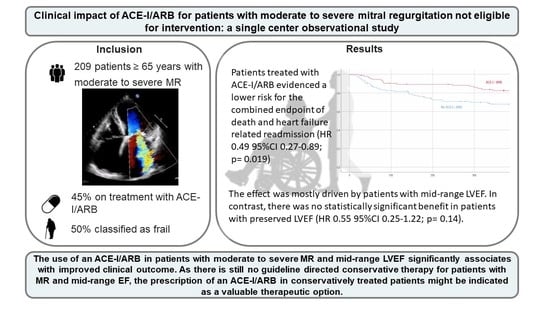
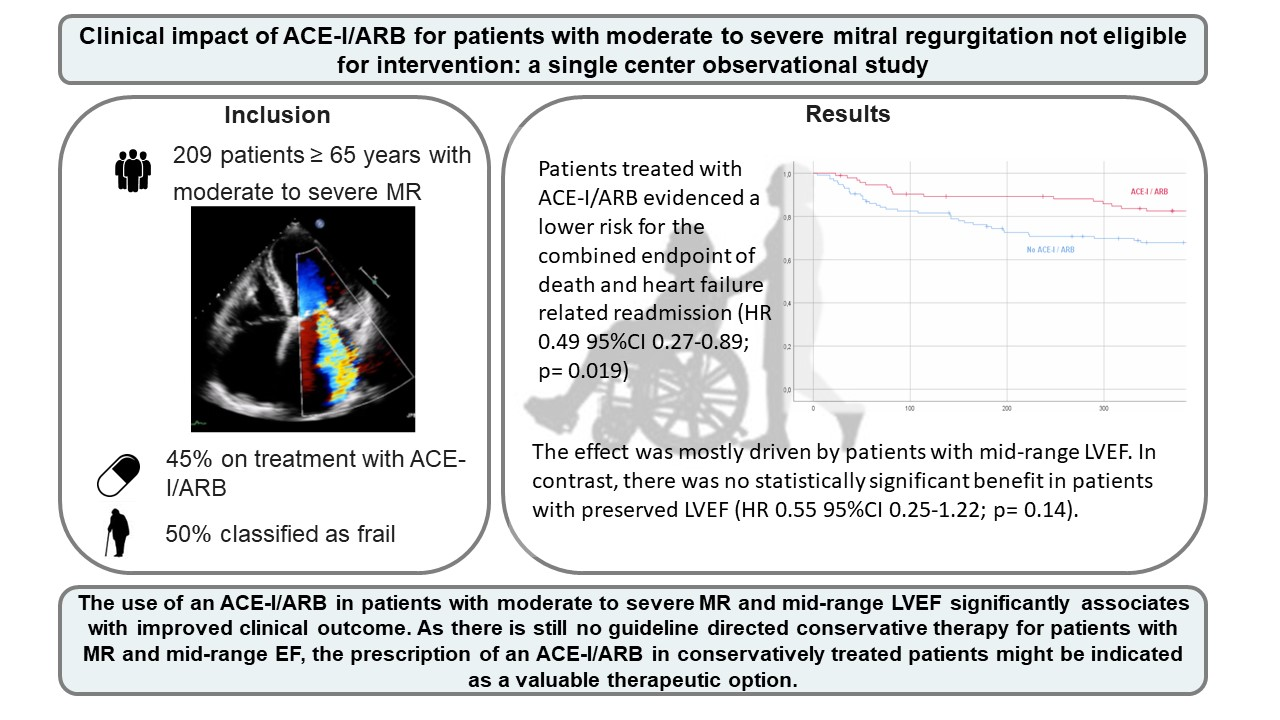
Clinical Impact of ACE-I/ARB for Conservatively Treated Patients with Moderate to Severe Mitral Regurgitation: A Single Center Observational Study
 , , , ,
, , , , 
Abstract
1. Introduction
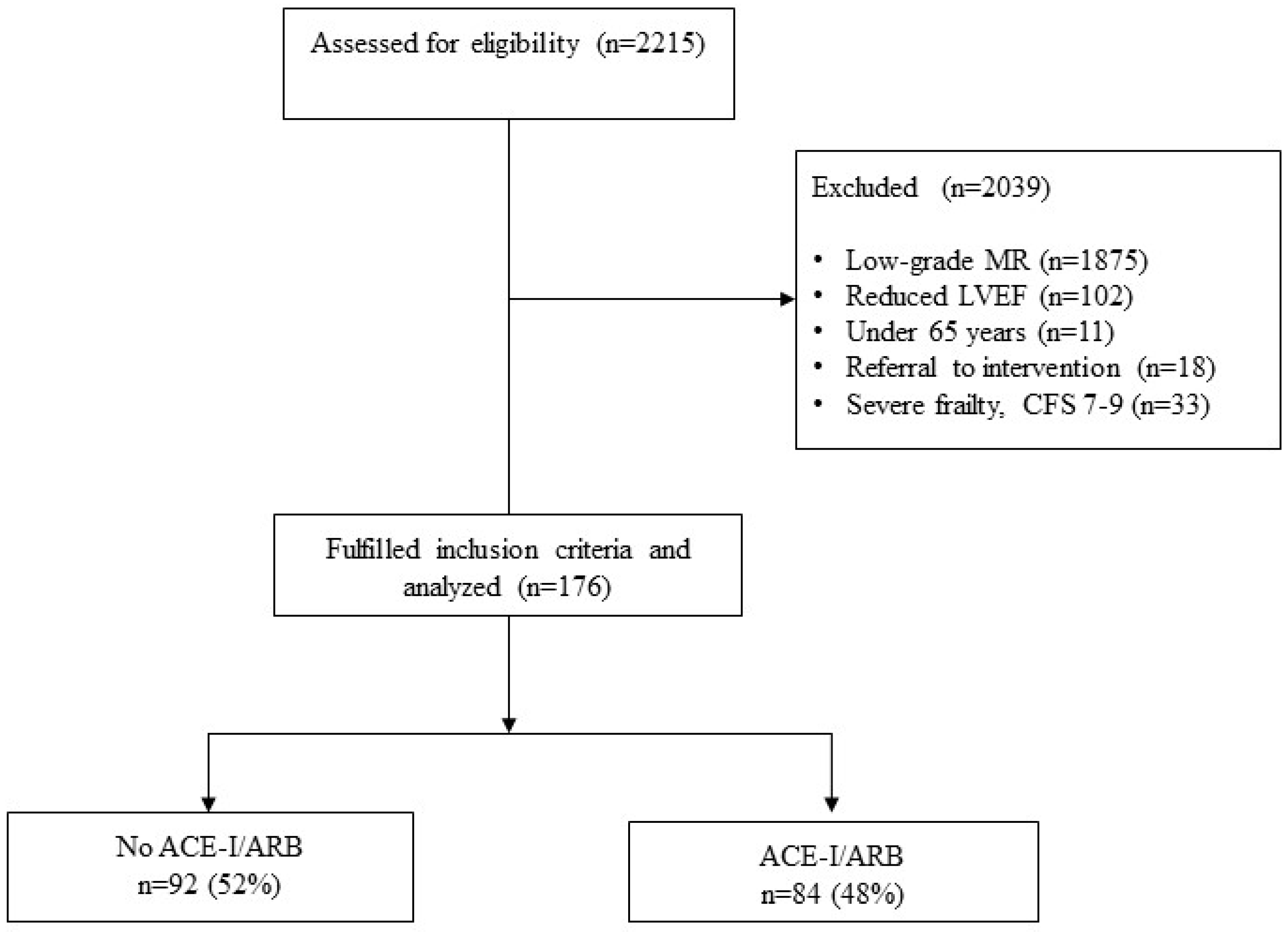
2. Materials and Methods
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dziadzko, V.; Clavel, M.-A.; Dziadzko, M.; Medina-Inojosa, J.R.; Michelena, H.; Maalouf, J.; Nkomo, V.; Thapa, P.; Enriquez-Sarano, P.M. Outcome and Undertreatment of Mitral Regurgitation: A Community Cohort Study. Lancet 2018, 391, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease: Developed by the Task Force for the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- d’Arcy, J.L.; Coffey, S.; Loudon, M.A.; Kennedy, A.; Pearson-Stuttard, J.; Birks, J.; Frangou, E.; Farmer, A.J.; Mant, D.; Wilson, J.; et al. Large-Scale Community Echocardiographic Screening Reveals a Major Burden of Undiagnosed Valvular Heart Disease in Older People: The OxVALVE Population Cohort Study. Eur. Heart J. 2016, 37, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Freed, L.A.; Levy, D.; Levine, R.A.; Larson, M.G.; Evans, J.C.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and Clinical Outcome of Mitral-Valve Prolapse. N. Engl. J. Med. 1999, 341, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Sarano, M.; Avierinos, J.-F.; Messika-Zeitoun, D.; Detaint, D.; Capps, M.; Nkomo, V.; Scott, C.; Schaff, H.V.; Tajik, A.J. Quantitative Determinants of the Outcome of Asymptomatic Mitral Regurgitation. N. Engl. J. Med. 2005, 352, 875–883. [Google Scholar] [CrossRef]
- O’Gara, P.T.; Mack, M.J. Secondary Mitral Regurgitation. N. Engl. J. Med. 2020, 383, 1458–1467. [Google Scholar] [CrossRef]
- Coffey, S.; Cairns, B.J.; Iung, B. The Modern Epidemiology of Heart Valve Disease. Heart Br. Card. Soc. 2016, 102, 75–85. [Google Scholar] [CrossRef]
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zühlke, L.; Prendergast, B.D. Global Epidemiology of Valvular Heart Disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef]
- Pibarot, P.; Delgado, V.; Bax, J.J. MITRA-FR vs. COAPT: Lessons from Two Trials with Diametrically Opposed Results. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 620–624. [Google Scholar] [CrossRef]
- Bartko, P.E.; Hülsmann, M.; Hung, J.; Pavo, N.; Levine, R.A.; Pibarot, P.; Vahanian, A.; Stone, G.W.; Goliasch, G. Secondary Valve Regurgitation in Patients with Heart Failure with Preserved Ejection Fraction, Heart Failure with Mid-Range Ejection Fraction, and Heart Failure with Reduced Ejection Fraction. Eur. Heart J. 2020, 41, 2799–2810. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Delgado, V.; Murray, S.; Hayes, S.; De Bonis, M.; Rosenhek, R.; Haude, M.; Hindricks, G.; Lazure, P.; Bax, J.; et al. P5811Real-Life Management of Mitral Regurgitations. Lesson from a European Survey. Eur. Heart J. 2017, 38. [Google Scholar] [CrossRef]
- Mirabel, M.; Iung, B.; Baron, G.; Messika-Zeitoun, D.; Détaint, D.; Vanoverschelde, J.-L.; Butchart, E.G.; Ravaud, P.; Vahanian, A. What Are the Characteristics of Patients with Severe, Symptomatic, Mitral Regurgitation Who Are Denied Surgery? Eur. Heart J. 2007, 28, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Iung, B.; Lancellotti, P.; Lansac, E.; Rodriguez Muñoz, D.; et al. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC) With the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Buzzatti, N.; Van Hemelrijck, M.; Denti, P.; Ruggeri, S.; Schiavi, D.; Scarfò, I.S.; Reser, D.; Taramasso, M.; Weber, A.; La Canna, G.; et al. Transcatheter or Surgical Repair for Degenerative Mitral Regurgitation in Elderly Patients: A Propensity-Weighted Analysis. J. Thorac. Cardiovasc. Surg. 2019, 158, 86–94.e1. [Google Scholar] [CrossRef]
- Harris, K.M.; Pastorius, C.A.; Duval, S.; Harwood, E.; Henry, T.D.; Carabello, B.A.; Hirsch, A.T. Practice Variation among Cardiovascular Physicians in Management of Patients with Mitral Regurgitation. Am. J. Cardiol. 2009, 103, 255–261. [Google Scholar] [CrossRef]
- Strauss, C.E.; Duval, S.; Pastorius, D.; Harris, K.M. Pharmacotherapy in the Treatment of Mitral Regurgitation: A Systematic Review. J. Heart Valve Dis. 2012, 21, 275–285. [Google Scholar]
- Sampaio, R.O.; Grinberg, M.; Leite, J.J.; Tarasoutchi, F.; Chalela, W.A.; Izaki, M.; Spina, G.S.; Rossi, E.G.; Mady, C. Effect of Enalapril on Left Ventricular Diameters and Exercise Capacity in Asymptomatic or Mildly Symptomatic Patients with Regurgitation Secondary to Mitral Valve Prolapse or Rheumatic Heart Disease. Am. J. Cardiol. 2005, 96, 117–121. [Google Scholar] [CrossRef]
- Wong, G.C.; Marcotte, F.; Rudski, L.G. Impact of Chronic Lisinopril Therapy on Left Atrial Volume versus Dimension in Chronic Organic Mitral Regurgitation. Can. J. Cardiol. 2006, 22, 125–129. [Google Scholar] [CrossRef]
- Marcotte, F.; Honos, G.N.; Walling, A.D.; Beauvais, D.; Blais, M.J.; Daoust, C.; Lisbona, A.; McCans, J.L. Effect of Angiotensin-Converting Enzyme Inhibitor Therapy in Mitral Regurgitation with Normal Left Ventricular Function. Can. J. Cardiol. 1997, 13, 479–485. [Google Scholar] [PubMed]
- Harris, K.M.; Aeppli, D.M.; Carey, C.F. Effects of Angiotensin-Converting Enzyme Inhibition on Mitral Regurgitation Severity, Left Ventricular Size, and Functional Capacity. Am. Heart J. 2005, 150, 1106. [Google Scholar] [CrossRef] [PubMed]
- Malev, E.; Kim, G.; Vasina, L.; Omelchenko, M.; Zemtsovsky, E. P100Angiotensin II Receptor Blockers in Modulation of Transforming Growth Factor-b Cardiac Effects in Mitral Valve Prolapse. Cardiovasc. Res. 2014, 103, S17. [Google Scholar] [CrossRef]
- Sekuri, C.; Utuk, O.; Bayturan, O.; Bilge, A.; Kurhan, Z.; Tavli, T. Effect of Losartan on Exercise Tolerance and Echocardiographic Parameters in Patients with Mitral Regurgitation. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2008, 9, 107–111. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| No ACE-I/ARB n = 92 | ACE-I/ARB n = 84 | p-Value | ||
|---|---|---|---|---|
| Age—yrs | 82 (8) | 81 (7) | 0.38 | |
| Male sex | 34% (31) | 35% (29) | 0.91 | |
| Coronary artery disease | 21% (19) | 24% (20) | 0.61 | |
| Diabetes mellitus | 18% (17) | 20% (17) | 0.77 | |
| Atrial fibrillation | 70% (64) | 62% (52) | 0.28 | |
| Extracardiac Arteriopathy | 37% (34) | 26% (22) | 0.13 | |
| Chronic lung disease | 14% (13) | 12% (10) | 0.66 | |
| CCS class 4 angina | 5% (5) | 4% (3) | 0.55 | |
| NYHA | I | 59% (54) | 50% (42) | 0.56 |
| II | 11% (10) | 15% (13) | ||
| III | 20% (18) | 19% (16) | ||
| IV | 11% (10) | 15% (13) | ||
| Renal insufficiency | Normal (>85 mL/min) | 26% (24) | 20% (17) | 0.47 |
| Moderately impaired (50–85 mL/min) | 55% (51) | 55% (46) | ||
| Severely impaired (<50 mL/min) | 18% (17) | 25% (21) | ||
| Dementia | 14% (13) | 5% (4) | 0.034 | |
| EuroScoreII (%) | 7 (8) | 6 (7) | 0.49 | |
| Polypharmacy ≥ 5 prescriptions | 74% (68) | 93% (78) | <0.001 | |
| Oral anticoagulation | 64% (58) | 62% (52) | 0.80 | |
| Beta blocker | 65% (60) | 64% (54) | 0.90 | |
| Heart rate at admission | 82 (22) | 79 (23) | 0.40 | |
| Heart rate at discharge | 73 (9) | 71 (10) | 0.13 | |
| Frailty | 43% (40) | 38% (32) | 0.47 | |
| Reason for admission | Heart failure | 40% (37) | 39% (33) | 0.69 |
| Gastroenterology | 16% (15) | 11% (9) | ||
| Other cardiac | 18% (17) | 17% (14) | ||
| Infection | 12% (11) | 14% (12) | ||
| Other | 13% (12) | 19% (16) |
| No ACE-I/ARB n = 92 | ACE-I/ARB n = 84 | p-Value | ||
|---|---|---|---|---|
| Mitral regurgitation | Moderate | 72% (66) | 68% (57) | 0.57 |
| Severe | 28% (26) | 32% (27) | ||
| Vena contracta—mm | 6 (1) | 6 (2) | 0.062 | |
| PISA | 8 (4) | 8 (3) | 0.74 | |
| LVEDD—mm | 48 (8) | 48 (9) | 0.95 | |
| Left Atrium—cm2 | 29 (8) | 29 (11) | 0.88 | |
| LVEF | Mildly reduced | 33% (30) | 35% (29) | 0.79 |
| Preserved | 67% (62) | 65% (55) | ||
| Aortic stenosis | Absent | 74% (68) | 83% (70) | 0.06 |
| Mild | 5% (5) | 8% (7) | ||
| Moderate | 11% (10) | 7% (6) | ||
| Severe | 10% (9) | 1% (1) | ||
| Univariate Model-1 | Multivariable Model-2 | Multivariable Model-3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | p-Value | aHR | 95%CI | p-Value | aHR | 95%CI | p-Value | |
| No ACE-I/ARB | Reference | Reference | Reference | ||||||
| ACE-I/ARB | 0.52 | 0.27–0.99 | 0.046 | 0.52 | 0.27–0.99 | 0.049 | 0.51 | 0.26–1.01 | 0.053 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uzel, R.; Bruno, R.R.; Jung, C.; Lang, C.; Hoi, H.; Grünbart, M.; Datz, C.; Hoppichler, F.; Wernly, B. Clinical Impact of ACE-I/ARB for Conservatively Treated Patients with Moderate to Severe Mitral Regurgitation: A Single Center Observational Study. J. Cardiovasc. Dev. Dis. 2023, 10, 177. https://doi.org/10.3390/jcdd10040177
Uzel R, Bruno RR, Jung C, Lang C, Hoi H, Grünbart M, Datz C, Hoppichler F, Wernly B. Clinical Impact of ACE-I/ARB for Conservatively Treated Patients with Moderate to Severe Mitral Regurgitation: A Single Center Observational Study. Journal of Cardiovascular Development and Disease. 2023; 10(4):177. https://doi.org/10.3390/jcdd10040177
Chicago/Turabian StyleUzel, Robert, Raphael R. Bruno, Christian Jung, Christian Lang, Hannes Hoi, Martin Grünbart, Christian Datz, Friedrich Hoppichler, and Bernhard Wernly. 2023. "Clinical Impact of ACE-I/ARB for Conservatively Treated Patients with Moderate to Severe Mitral Regurgitation: A Single Center Observational Study" Journal of Cardiovascular Development and Disease 10, no. 4: 177. https://doi.org/10.3390/jcdd10040177
APA StyleUzel, R., Bruno, R. R., Jung, C., Lang, C., Hoi, H., Grünbart, M., Datz, C., Hoppichler, F., & Wernly, B. (2023). Clinical Impact of ACE-I/ARB for Conservatively Treated Patients with Moderate to Severe Mitral Regurgitation: A Single Center Observational Study. Journal of Cardiovascular Development and Disease, 10(4), 177. https://doi.org/10.3390/jcdd10040177