
Comparison of Fractional Flow Reserve with Resting Non-Hyperemic Indices in Patients with Coronary Artery Disease

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Toth, G.; Hamilos, M.; Pyxaras, S.; Mangiacapra, F.; Nelis, O.; De Vroey, F.; Di Serafino, L.; Muller, O.; Van Mieghem, C.; Wyffels, E.; et al. Evolving concepts of angiogram: Fractional flow reserve discordances in 4000 coronary stenoses. Eur. Heart J. 2014, 35, 2831–2838. [Google Scholar] [CrossRef] [PubMed]
- Kogame, N.; Ono, M.; Kawashima, H.; Tomaniak, M.; Hara, H.; Leipsic, J.; Andreini, D.; Collet, C.; Patel, M.R.; Tu, S.; et al. The Impact of Coronary Physiology on Contemporary Clinical Decision Making. JACC Cardiovasc. Interv. 2020, 13, 1617–1638. [Google Scholar] [CrossRef] [PubMed]
- Michail, M.; Thakur, U.; Mehta, O.; Ramzy, J.M.; Comella, A.; Ihdayhid, A.R.; Cameron, J.D.; Nicholls, S.J.; Hoole, S.P.; Brown, A.J. Non-hyperaemic pressure ratios to guide percutaneous coronary intervention. Open Heart 2020, 7, e001308. [Google Scholar] [CrossRef] [PubMed]
- Siudak, Z.; Bartus, S.; Hawranek, M.; Kusa, J.; Kleczynski, P.; Milewski, K.; Opolski, M.P.; Pawlowski, T.; Protasiewicz, M.; Smolka, G.; et al. Interventional cardiology in Poland in 2021. Annual summary report of the Association of Cardiovascular Interventions of the Polish Cardiac Society (AISN PTK) and Jagiellonian University Medical College. Adv. Interv. Cardiol. 2022, 18, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Maznyczka, A.M.; Matthews, C.J.; Blaxill, J.M.; Greenwood, J.P.; Mozid, A.M.; Rossington, J.A.; Veerasamy, M.; Wheatcroft, S.B.; Curzen, N.; Bulluck, H. Fractional Flow Reserve versus Angiography-Guided Management of Coronary Artery Disease: A Meta-Analysis of Contemporary Randomised Controlled Trials. J. Clin. Med. 2022, 11, 7092. [Google Scholar] [CrossRef]
- Hu, M.; Tan, J.; Yang, Y. Comparison of Six Different Percutaneous Coronary Intervention Guidance Modalities. J. Cardiovasc. Dev. Dis. 2022, 9, 343. [Google Scholar] [CrossRef]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef]
- Kleczynski, P.; Dziewierz, A.; Rzeszutko, L.; Dudek, D.; Legutko, J. Hyperemic versus non-hyperemic indexes for coronary physiology assessment in patients with severe aortic stenosis. Adv. Med. Sci. 2021, 66, 366–371. [Google Scholar] [CrossRef]
- Kleczynski, P.; Dziewierz, A.; Rzeszutko, L.; Dudek, D.; Legutko, J. Contrast medium Pd/Pa ratio in comparison to fractional flow reserve, quantitative flow ratio and instantaneous wave-free ratio for evaluation of intermediate coronary lesions. Adv. Interv. Cardiol. 2020, 16, 384–390. [Google Scholar] [CrossRef]
- Berry, C.; van ’t Veer, M.; Witt, N.; Kala, P.; Bocek, O.; Pyxaras, S.A.; McClure, J.D.; Fearon, W.F.; Barbato, E.; Tonino, P.A.; et al. VERIFY (VERification of Instantaneous Wave-Free Ratio and Fractional Flow Reserve for the Assessment of Coronary Artery Stenosis Severity in EverydaY Practice): A multicenter study in consecutive patients. J. Am. Coll. Cardiol. 2013, 61, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Gotberg, M.; Frobert, O. Instantaneous Wave-free Ratio versus Fractional Flow Reserve. N. Engl. J. Med. 2017, 377, 1596–1597. [Google Scholar] [CrossRef] [PubMed]
- Svanerud, J.; Ahn, J.M.; Jeremias, A.; van ’t Veer, M.; Gore, A.; Maehara, A.; Crowley, A.; Pijls, N.H.J.; De Bruyne, B.; Johnson, N.P.; et al. Validation of a novel non-hyperaemic index of coronary artery stenosis severity: The Resting Full-cycle Ratio (VALIDATE RFR) study. EuroIntervention 2018, 14, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Muroya, T.; Kawano, H.; Hata, S.; Shinboku, H.; Sonoda, K.; Kusumoto, S.; Eto, R.; Otsuka, K.; Maemura, K. Relationship between resting full-cycle ratio and fractional flow reserve in assessments of coronary stenosis severity. Catheter. Cardiovasc. Interv. 2020, 96, E432–E438. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Dohi, T.; Chikata, Y.; Fukase, T.; Takeuchi, M.; Takahashi, N.; Endo, H.; Nishiyama, H.; Doi, S.; Okai, I.; et al. Predictors of discordance between fractional flow reserve and resting full-cycle ratio in patients with coronary artery disease: Evidence from clinical practice. J. Cardiol. 2021, 77, 313–319. [Google Scholar] [CrossRef]
- Lee, J.M.; Shin, E.S.; Nam, C.W.; Doh, J.H.; Hwang, D.; Park, J.; Kim, K.J.; Zhang, J.; Koo, B.K. Discrepancy between fractional flow reserve and instantaneous wave-free ratio: Clinical and angiographic characteristics. Int. J. Cardiol. 2017, 245, 63–68. [Google Scholar] [CrossRef]
- Benenati, S.; De Maria, G.L.; Scarsini, R.; Porto, I.; Banning, A.P. Invasive "in the cath-lab" assessment of myocardial ischemia in patients with coronary artery disease: When does the gold standard not apply? Cardiovasc. Revasc. Med. 2018, 19, 362–372. [Google Scholar] [CrossRef]
- Legutko, J.; Kleczynski, P.; Dziewierz, A.; Rzeszutko, L.; Dudek, D. Adenosine intracoronary bolus dose escalation versus intravenous infusion to induce maximum coronary hyperemia for fractional flow reserve assessment. Kardiol. Pol. 2019, 77, 610–617. [Google Scholar] [CrossRef]
- Derimay, F.; Johnson, N.P.; Zimmermann, F.M.; Adjedj, J.; Witt, N.; Hennigan, B.; Koo, B.K.; Barbato, E.; Esposito, G.; Trimarco, B.; et al. Predictive factors of discordance between the instantaneous wave-free ratio and fractional flow reserve. Catheter. Cardiovasc. Interv. 2019, 94, 356–363. [Google Scholar] [CrossRef]
- Seligman, H.; Nijjer, S.S.; van de Hoef, T.P.; de Waard, G.A.; Mejia-Renteria, H.; Echavarria-Pinto, M.; Shun-Shin, M.J.; Howard, J.P.; Cook, C.M.; Warisawa, T.; et al. Phasic flow patterns of right versus left coronary arteries in patients undergoing clinical physiological assessment. EuroIntervention 2022, 17, 1260–1270. [Google Scholar] [CrossRef]
- Nijjer, S.S.; de Waard, G.A.; Sen, S.; van de Hoef, T.P.; Petraco, R.; Echavarria-Pinto, M.; van Lavieren, M.A.; Meuwissen, M.; Danad, I.; Knaapen, P.; et al. Coronary pressure and flow relationships in humans: Phasic analysis of normal and pathological vessels and the implications for stenosis assessment: A report from the Iberian-Dutch-English (IDEAL) collaborators. Eur. Heart J. 2016, 37, 2069–2080. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Johnson, N.P.; Berry, C.; De Bruyne, B.; Gould, K.L.; Jeremias, A.; Oldroyd, K.G.; Pijls, N.H.J.; Fearon, W.F.; Investigators, C.S. The Influence of Lesion Location on the Diagnostic Accuracy of Adenosine-Free Coronary Pressure Wire Measurements. JACC Cardiovasc. Interv. 2016, 9, 2390–2399. [Google Scholar] [CrossRef] [PubMed]
- Hennigan, B.; Oldroyd, K.G.; Berry, C.; Johnson, N.; McClure, J.; McCartney, P.; McEntegart, M.B.; Eteiba, H.; Petrie, M.C.; Rocchiccioli, P.; et al. Discordance Between Resting and Hyperemic Indices of Coronary Stenosis Severity: The VERIFY 2 Study (A Comparative Study of Resting Coronary Pressure Gradient, Instantaneous Wave-Free Ratio and Fractional Flow Reserve in an Unselected Population Referred for Invasive Angiography). Circ. Cardiovasc. Interv. 2016, 9, e004016. [Google Scholar] [CrossRef]
- Onishi, K.; Watanabe, H.; Kakehi, K.; Ikeda, T.; Takase, T.; Yamaji, K.; Ueno, M.; Kobuke, K.; Nakazawa, G.; Miyazaki, S.; et al. Determinants and prognostic implications of instantaneous wave-free ratio in patients with mild to intermediate coronary stenosis: Comparison with those of fractional flow reserve. PLoS ONE 2020, 15, e0237275. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, H.; Chikamori, T.; Tanaka, N.; Usui, Y.; Takazawa, K.; Yamashina, A. Application of pressure-derived myocardial fractional flow reserve in assessing the functional severity of coronary artery stenosis in patients with diabetes mellitus. Circ. J. 2004, 68, 993–998. [Google Scholar] [CrossRef]
- Reith, S.; Battermann, S.; Hellmich, M.; Marx, N.; Burgmaier, M. Impact of type 2 diabetes mellitus and glucose control on fractional flow reserve measurements in intermediate grade coronary lesions. Clin. Res. Cardiol. 2014, 103, 191–201. [Google Scholar] [CrossRef]
- Rivero, F.; Antuna, P.; Garcia-Guimaraes, M.; Jimenez, C.; Cuesta, J.; Bastante, T.; Alfonso, F. Correlation between fractional flow reserve and instantaneous wave-free ratio with morphometric assessment by optical coherence tomography in diabetic patients. Int. J. Cardiovasc. Imaging 2020, 36, 1193–1201. [Google Scholar] [CrossRef]
- DEFINE-FLAIR Trial Investigators; Lee, J.M.; Choi, K.H.; Koo, B.K.; Dehbi, H.M.; Doh, J.H.; Nam, C.W.; Shin, E.S.; Cook, C.M.; Al-Lamee, R.; et al. Comparison of Major Adverse Cardiac Events Between Instantaneous Wave-Free Ratio and Fractional Flow Reserve-Guided Strategy in Patients With or Without Type 2 Diabetes: A Secondary Analysis of a Randomized Clinical Trial. JAMA Cardiol. 2019, 4, 857–864. [Google Scholar] [CrossRef]
- Dziewierz, A.; Zdzierak, B.; Malinowski, K.P.; Siudak, Z.; Zasada, W.; Tokarek, T.; Zabojszcz, M.; Dolecka-Slusarczyk, M.; Dudek, D.; Bartus, S.; et al. Diabetes Mellitus Is Still a Strong Predictor of Periprocedural Outcomes of Primary Percutaneous Coronary Interventions in Patients Presenting with ST-Segment Elevation Myocardial Infarction (from the ORPKI Polish National Registry). J. Clin. Med. 2022, 11, 6284. [Google Scholar] [CrossRef]
- Tebaldi, M.; Biscaglia, S.; Fineschi, M.; Manari, A.; Menozzi, M.; Secco, G.G.; Di Lorenzo, E.; D’Ascenzo, F.; Fabbian, F.; Tumscitz, C.; et al. Fractional Flow Reserve Evaluation and Chronic Kidney Disease: Analysis From a Multicenter Italian Registry (the FREAK Study). Catheter. Cardiovasc. Interv. 2016, 88, 555–562. [Google Scholar] [CrossRef]
- Dziewierz, A.; Rzeszutko, L.; Dudek, D.; Legutko, J.; Kleczynski, P. Impact of diabetes mellitus on the diagnostic performance of fractional flow reserve in patients with severe aortic stenosis. Kardiol. Pol. 2022, 80, 1217–1223. [Google Scholar] [CrossRef] [PubMed]
- Zelis, J.M.; Tonino, P.A.L.; Johnson, N.P. Why Can Fractional Flow Reserve Decrease After Transcatheter Aortic Valve Implantation? J. Am. Heart. Assoc. 2020, 9, e04905. [Google Scholar] [CrossRef]
- Pintea Bentea, G.; Berdaoui, B.; Samyn, S.; Morissens, M.; Rodriguez, J.C. Reliability of Fractional Flow Reserve and Instantaneous Wave-Free Ratio in Assessing Intermediate Coronary Stenosis in Patients with Atrial Fibrillation. Am. J. Cardiol. 2022, 162, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Choi, K.H.; Park, J.; Hwang, D.; Rhee, T.M.; Kim, J.; Park, J.; Kim, H.Y.; Jung, H.W.; Cho, Y.K.; et al. Physiological and Clinical Assessment of Resting Physiological Indexes. Circulation 2019, 139, 889–900. [Google Scholar] [CrossRef]
- Nobre Menezes, M.; Francisco, A.R.G.; Carrilho Ferreira, P.; Jorge, C.; Torres, D.; Cardoso, P.; Duarte, J.A.; Marques da Costa, J.; Infante de Oliveira, E.; Pinto, F.J.; et al. Comparative analysis of fractional flow reserve and instantaneous wave-free ratio: Results of a five-year registry. Rev. Port. Cardiol. 2018, 37, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Rhee, T.M.; Choi, K.H.; Park, J.; Hwang, D.; Kim, J.; Park, J.; Kim, H.Y.; Jung, H.W.; Cho, Y.K.; et al. Clinical Outcome of Lesions With Discordant Results Among Different Invasive Physiologic Indices—Resting Distal Coronary to Aortic Pressure Ratio, Resting Full-Cycle Ratio, Diastolic Pressure Ratio, Instantaneous Wave-Free Ratio, and Fractional Flow Reserve. Circ. J. 2019, 83, 2210–2221. [Google Scholar] [CrossRef] [PubMed]
- Higashioka, D.; Shiono, Y.; Emori, H.; Khalifa, A.K.M.; Takahata, M.; Wada, T.; Fujita, S.; Kashiwagi, M.; Shimamura, K.; Kuroi, A.; et al. Prevalence of myocardial perfusion scintigraphy derived ischemia in coronary lesions with discordant fractional flow reserve and non-hyperemic pressure ratios. Int. J. Cardiol. 2022, 357, 20–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Value; n = 279 Patients | ||
|---|---|---|
| Age, years | mean (SD) | 67.55 (10.52) |
| Female | N (%) | 70 (25%) |
| Height, cm | median (IQR) | 170.00 (11.00) |
| Weight, kg | median (IQR) | 84.00 (21.88) |
| Body mass index, kg/m2 | median (IQR) | 28.40 (6.67) |
| eGFR, mL/min/1.73 m2 | mean (SD) | 76.80 (25.86) |
| LVEF, % | median (IQR) | 52.00 (20.00) |
| Arterial hypertension | N (%) | 242 (87%) |
| Diabetes mellitus | N (%) | 112 (40%) |
| Diabetes mellitus-treatment | diet, N (%) oral medications, N (%) insulin, N (%) | 6 (2%) 63 (23%) 44 (16%) |
| Atrial fibrillation | N (%) | 55 (20%) |
| Previous MI | N (%) | 134 (48%) |
| Previous PCI | N (%) | 141 (51%) |
| Previous CABG | N (%) | 14 (5%) |
| Peripheral vascular disease | N (%) | 42 (15%) |
| COPD | N (%) | 18 (6%) |
| Stroke/TIA | N (%) | 27 (10%) |
| Current smoker | N (%) | 144 (52%) |
| Dyslipidemia | N (%) | 218 (78%) |
| Number of assessed vessels - per patient | 1 (%) 2 (%) 3 (%) 4 (%) | 169 (61%) 85 (30%) 22 (8%) 3 (1%) |
| value, n = 417 vessels | ||
| Assessed vessels-location | LAD (%) non-LAD (%) Dg (%) Cx (%) Mg (%) RCA (%) | 249 (60%) 168 (40%) 17 (4%) 81 (19%) 20 (5%) 50 (12%) |
| LAD | non-LAD | p-Value | ||||
|---|---|---|---|---|---|---|
| Cx | Mg | Dg | RCA | |||
| FFR, median (Q1–Q3) | 0.78 (0.74–0.84) | 0.86 (0.79–0.91) | <0.0001 | |||
| 0.87 (0.8–0.92) | 0.88 (0.80–0.91) | 0.76 (0.72–0.82) | 0.86 (0.82–0.91) | <0.0001 * | ||
| FFR ≤ 0.80, N (%) | 149 (59.8%) | 51 (30.4%) | <0.0001 | |||
| 21 (25.9%) | 5 (25.0%) | 13 (76.5%) | 12 (24.0%) | <0.0001 * | ||
| iFR/RFR, median (Q1–Q3) | 0.89 (0.84–0.92) | 0.94 (0.88–0.97) | <0.0001 | |||
| 0.95 (0.89–0.98) | 0.93 (0.90–0.98) | 0.87 (0.81–0.91) | 0.95 (0.91–0.97) | <0.0001 * | ||
| iFR/RFR ≤ 0.89, N (%) | 145 (58.2%) | 49 (29.2%) | <0.0001 | |||
| 23 (28.4%) | 4 (20%) | 11 (64.7%) | 11 (22%) | <0.0001 ** | ||
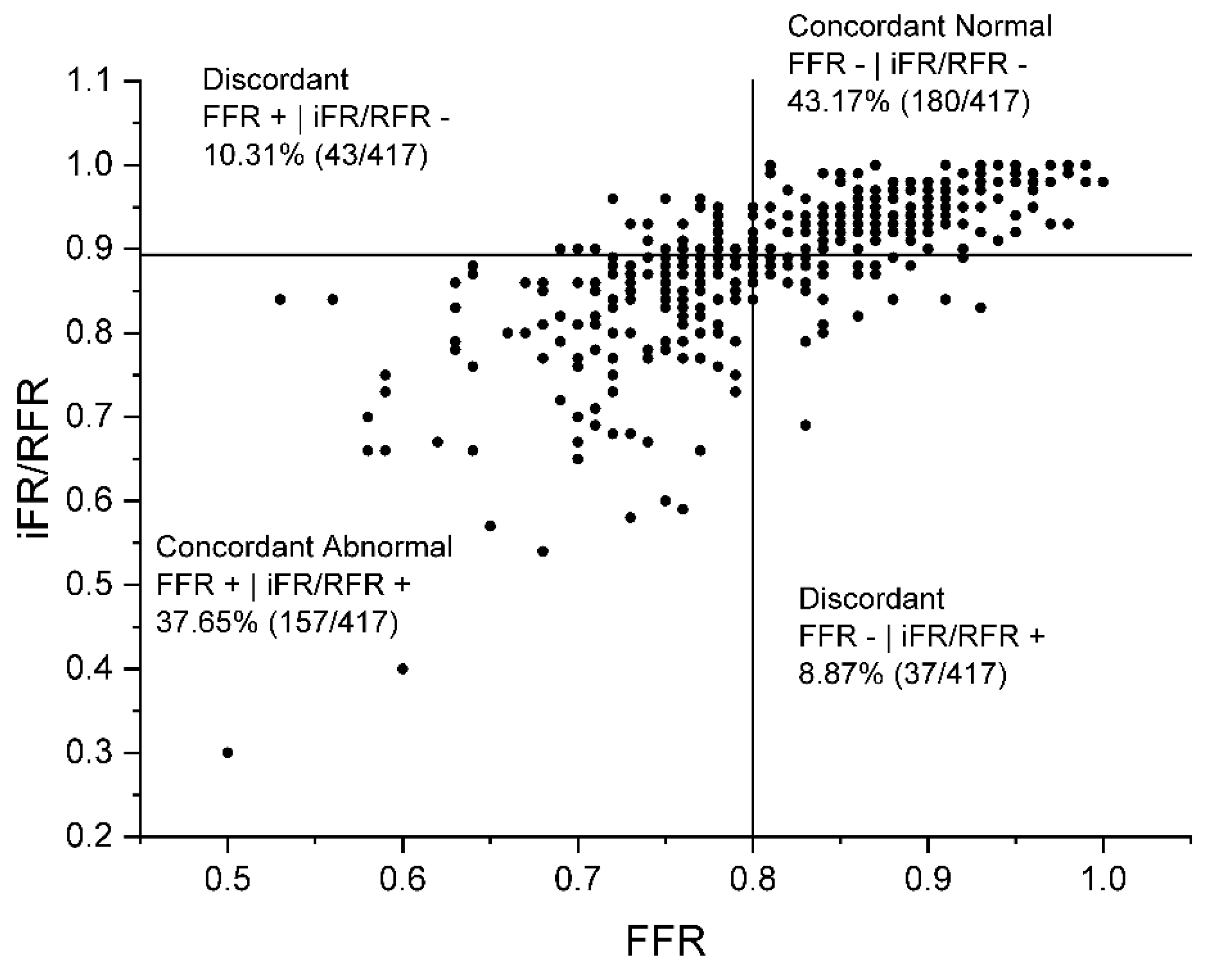
| FFR- | iFR/RFR- n = 180 (43.2%) | FFR- | iFR/RFR + n = 37 (8.9%) | FFR+ | iFR/RFR- n = 43 (10.3%) | FFR+ | iFR/RFR+ n = 157 (37.6%) | p-Value | |
|---|---|---|---|---|---|
| Age, years mean (SD) | 67.73 (9.37) | 68.68 (12.00) | 64.35 (9.96) * | 68.13 (10.74) | 0.16 |
| Female, N (%) | 60 (33.3%) * | 10 (27.0%) | 6 (14.0%) | 30 (19.1%) | 0.007 |
| Height, cm median (IQR) | 170 (11) | 171 (13.25) | 172 (11) | 170 (11) | 0.62 |
| Weight, kg median (IQR) | 84 (23) | 85 (16.25) | 89 (20) | 82 (23) | 0.75 |
| Body mass index, kg/m2 median (IQR) | 28.39 (7.56) | 28.38 (5.21) | 29.04 (5.89) | 28.44 (6.68) | 0.87 |
| eGFR, mL/min/1.73 m2 mean (SD) | 77.31 (26.67) ** | 69.35 (26.84) ** | 88.74 (26.81) * | 77.13 (25.59) | 0.010 |
| HbA1c, % median (IQR) | 6.5 (2.7) | 7.2 (4.4) | 8 (4.08) | 6.9 (2.3) | 0.97 |
| LVEF, % median (IQR) | 55 (20) | 49.5 (13) | 54 (15) | 51 (21.5) | 0.34 |
| Arterial hypertension, N (%) | 159 (88.3%) | 33 (89.2%) | 33 (76.7%) * | 144 (91.7%) | 0.042 |
| Diabetes mellitus, N (%) | 63 (35.0%) | 14 (37.8%) | 21 (48.8%) | 74 (47.1%) | 0.10 |
| Diabetes mellitus treatment - diet, N (%) - oral medications, N (%) - insulin, N (%) | 3 (1.7%) 40 (22.2%) 22 (12.2%) | ** 1 (2.7%) 3 (8.1%) 10 (27.0%) | 0 (0.0%) 18 (41.9%) 3 (7.0%) | 5 (3.2%) 38 (24.2%) 31 (19.7%) | 0.013 |
| Atrial fibrillation, N (%) | 39 (21.7%) | 12 (32.4%) | 9 (20.9%) | 27 (17.2%) | 0.23 |
| Previous MI, N (%) | 82 (45.6%) | 20 (54.1%) | 19 (44.2%) | 80 (51.0%) | 0.62 |
| Previous PCI, N (%) | 82 (45.6%) | 22 (59.5%) | 19 (44.2%) | 89 (56.7%) | 0.11 |
| Previous CABG, N (%) | 12 (6.7%) | 1 (2.7%) | 1 (2.3%) | 5 (3.2%) | 0.55 |
| Peripheral vascular disease, N (%) | 20 (11.1%) * | 5 (13.5%) | 4 (9.3%) | 37 (23.6%) | 0.008 |
| COPD, N (%) | 12 (6.7%) | 7 (18.9%) | 2 (4.7%) | 11 (7.0%) | 0.16 |
| Stroke/TIA, N (%) | 18 (10.0%) | 3 (8.1%) | 3 (7.0%) | 12 (7.6%) | 0.88 |
| Current smoker, N (%) | 90 (50.0%) | 18 (48.6%) | 23 (53.5%) | 92 (58.6%) | 0.41 |
| Dyslipidemia, N (%) | 144 (80.0%) | 29 (78.4%) | 36 (83.7%) | 114 (72.6%) | 0.50 |
| Assessed vessels - number 1, N (%) 2, N (%) 3, N (%) 4, N (%) | *** 59 (32.8%) 88 (48.9%) 30 (16.7%) 3 (1.7%) | * 14 (37.8%) 13 (35.1%) 4 (10.8%) 6 (16.2%) | 21 (48.8%) 13 (30.2%) 9 (20.9%) 0 (0.0%) | 75 (47.8%) 56 (35.7%) 23 (14.6%) 3 (1.9%) | <0.0001 |
| Assessed vessels - location LAD, N (%) non-LAD, N (%) - Cx, N (%) - Mg, N (%) - Dg, N (%) - RCA, N (%) | *, ** 77 (42.8%) 103 (57.2%) 54 (30.0%) 14 (7.8%) 2 (1.1%) 33 (18.3%) | 23 (62.2%) 14 (37.8%) 6 (16.2%) 1 (2.7%) 2 (5.4%) 5 (13.5%) | 27 (62.8%) 16 (37.2%) 4 (9.3%) 2 (4.7%) 4 (9.3%) 6 (14.0%) | 122 (77.7%) 35 (22.3%) 17 (10.8%) 3 (1.9%) 9 (5.7%) 6 (3.8%) | <0.0001 |
| Univariate Analysis OR (95% Confidence Interval) | p-Value | Multivariate Analysis OR (95% Confidence Interval) | p-Value | |
|---|---|---|---|---|
| Predictors of FFR+ | iFR/RFR− | ||||
| Age (per 1 year) | 0.96 (0.93–0.99) | 0.029 | 0.96 (0.93–0.99) | 0.024 |
| LVEF (per 1%) | 1.01 (0.98–1.04) | 0.30 | 1.02 (0.98-1.04) | 0.22 |
| Predictors of FFR− | iFR/RFR+ | ||||
| DM treatment (insulin vs. others) | 4.64 (1.39–15.48) | 0.013 | 4.61 (1.38–15.40) | 0.013 |
| eGFR (per 1 mL/min/1.73 m2) | 0.98 (0.97–0.99) | 0.046 | 0.99 (0.97–1.02) | 0.69 |
| Predictors of overall FFR and iFR/RFR discordance | ||||
| Age (per 1 year) | 0.99 (0.96–1.01) | 0.22 | 0.98 (0.95–1.01) | 0.06 |
| LVEF (per 1%) | 1.01 (0.99–1.03) | 0.28 | 1.01 (0.99–1.03) | 0.15 |
| Atrial fibrillation | 1.46 (0.83–2.56) | 0.20 | 1.90 (1.02–3.51) | 0.040 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zdzierak, B.; Zasada, W.; Krawczyk-Ożóg, A.; Rakowski, T.; Bartuś, S.; Surdacki, A.; Dziewierz, A. Comparison of Fractional Flow Reserve with Resting Non-Hyperemic Indices in Patients with Coronary Artery Disease. J. Cardiovasc. Dev. Dis. 2023, 10, 34. https://doi.org/10.3390/jcdd10020034
Zdzierak B, Zasada W, Krawczyk-Ożóg A, Rakowski T, Bartuś S, Surdacki A, Dziewierz A. Comparison of Fractional Flow Reserve with Resting Non-Hyperemic Indices in Patients with Coronary Artery Disease. Journal of Cardiovascular Development and Disease. 2023; 10(2):34. https://doi.org/10.3390/jcdd10020034
Chicago/Turabian StyleZdzierak, Barbara, Wojciech Zasada, Agata Krawczyk-Ożóg, Tomasz Rakowski, Stanisław Bartuś, Andrzej Surdacki, and Artur Dziewierz. 2023. "Comparison of Fractional Flow Reserve with Resting Non-Hyperemic Indices in Patients with Coronary Artery Disease" Journal of Cardiovascular Development and Disease 10, no. 2: 34. https://doi.org/10.3390/jcdd10020034
APA StyleZdzierak, B., Zasada, W., Krawczyk-Ożóg, A., Rakowski, T., Bartuś, S., Surdacki, A., & Dziewierz, A. (2023). Comparison of Fractional Flow Reserve with Resting Non-Hyperemic Indices in Patients with Coronary Artery Disease. Journal of Cardiovascular Development and Disease, 10(2), 34. https://doi.org/10.3390/jcdd10020034