
Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom


Abstract
1. Background
2. Methods
2.1. Study Design
2.2. Within-Trial Analysis
2.3. Study Population
2.4. Study Perspective
2.5. Intervention and Comparator
2.6. Time Horizon
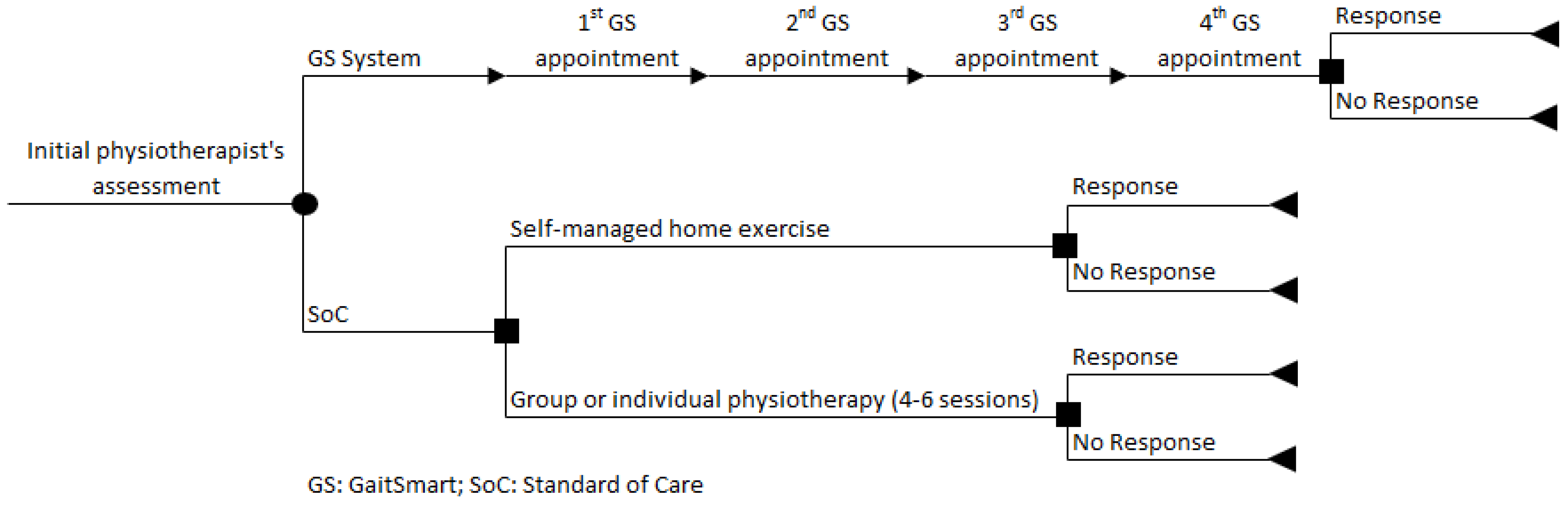
2.7. Decision Modelling
2.8. Model Input Parameters
2.8.1. Transition Probabilities
2.8.2. Costs
2.8.3. Health Outcomes—Clinical Effectiveness
2.8.4. Assumptions
2.8.5. Sensitivity Analysis
3. Results
3.1. Cost-Effectiveness for the Base Case
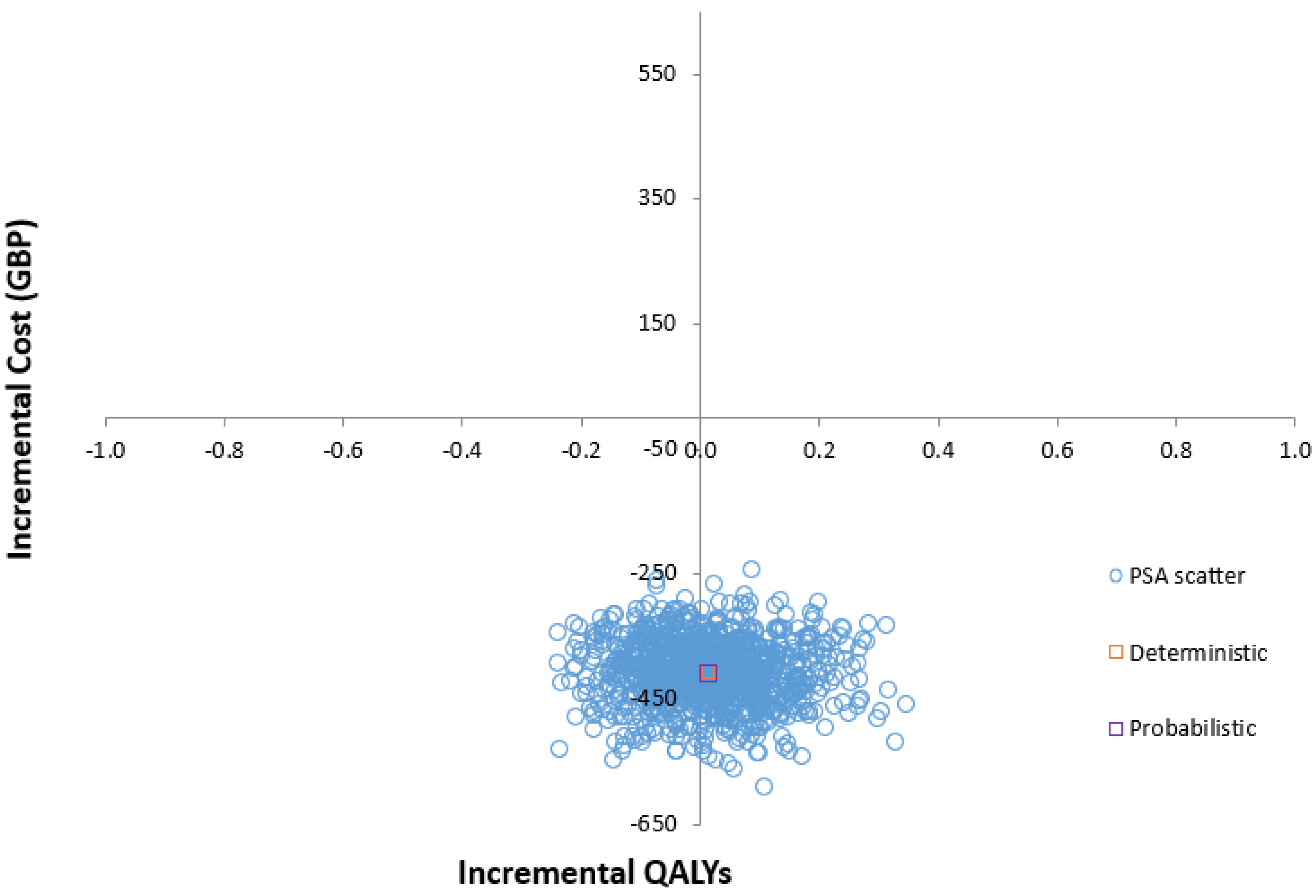
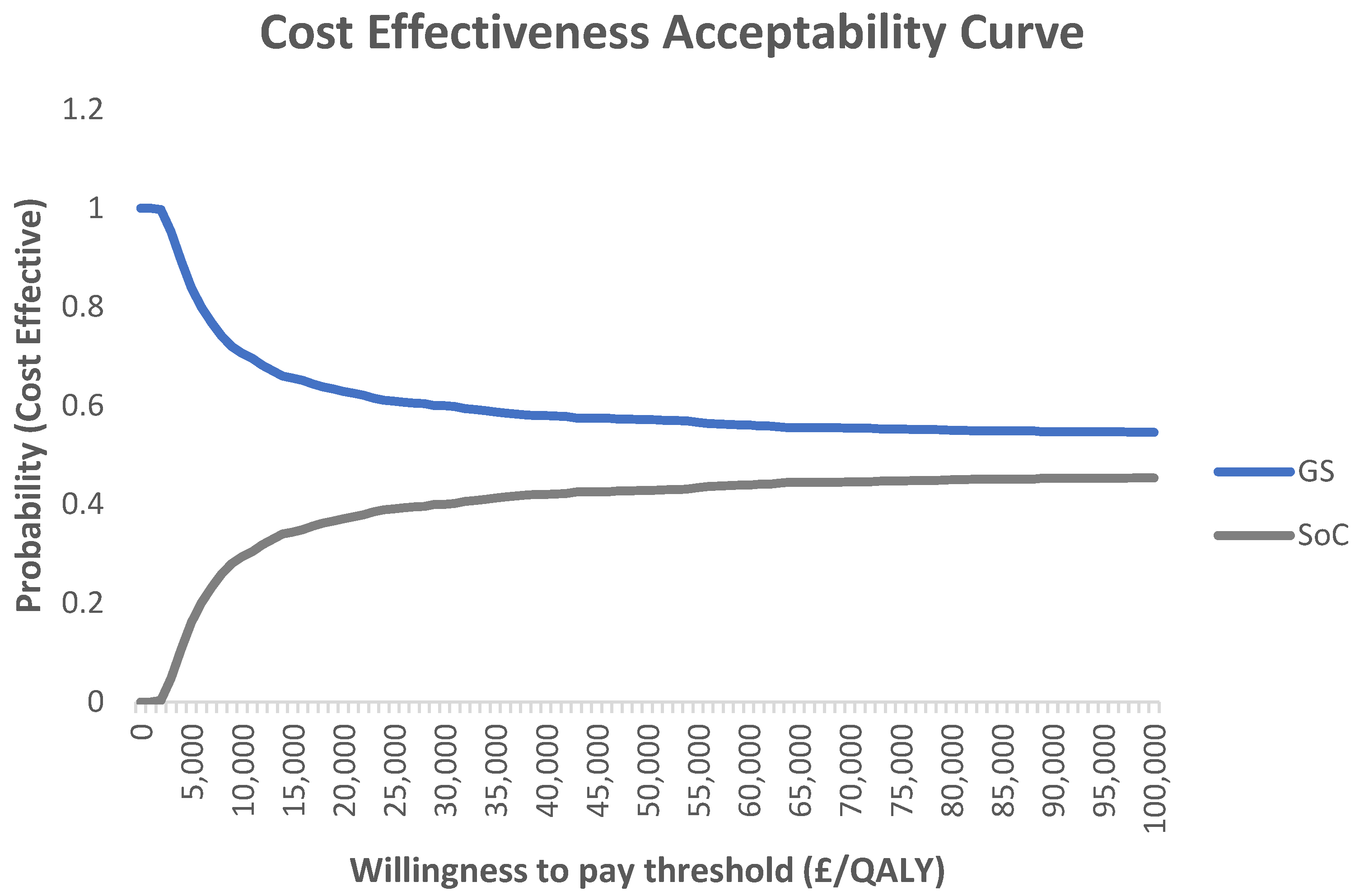
3.2. Probabilistic Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, W.; Nims, R.J.; Savadipour, A.; Zhang, Q.; Leddy, H.A.; Liu, F.; McNulty, A.L.; Chen, Y.; Guilak, F.; Liedtke, W.B. Inflammatory signaling sensitizes Piezo1 mechanotransduction in articular chondrocytes as a pathogenic feed-forward mechanism in osteoarthritis. Proc. Natl. Acad. Sci. USA 2021, 118, e2001611118. [Google Scholar] [CrossRef] [PubMed]
- Public Health England; Arthritis Research UK. Prevalence of Osteoarthritis in England and Local Authorities: Birmingham; Public Health England: London, UK; Arthritis Research UK: London, UK, 2014.
- Swain, S.; Sarmanova, A.; Mallen, C.; Kuo, C.; Coupland, C.; Doherty, M.; Zhang, W. Trends in incidence and prevalence of osteoarthritis in the United Kingdom: Findings from the Clinical Practice Research Datalink (CPRD). Osteoarthr. Cartil. 2020, 28, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Gupte, C.; Akhtar, K.; Smith, P.; Cobb, J. The Global Economic Cost of Osteoarthritis: How the UK Compares. Arthritis 2012, 2012, 698709. [Google Scholar] [CrossRef] [PubMed]
- Abraham, L.; Halsby, K.; Stein, N.; Wrona, B.; Emir, B.; Stevenson, H. An Observational Retrospective Matched Cohort Study of Healthcare Resource Utilisation and Costs in UK Patients with Moderate to Severe Osteoarthritis Pain. Rheumatol. Ther. 2022, 9, 851–874. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Care Excellence. Osteoarthritis in over 16 s: Diagnosis and Management | Guidance. Available online: https://www.nice.org.uk/guidance/ng226 (accessed on 17 February 2024).
- Ethgen, O.; Bruyerè, O.; Richy, F.; Dardennes, C.; Reginster, J. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J. Bone Jt. Surg. Am. 2004, 86, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.; Sledge, C. Total hip and total knee replacement (1). N. Engl. J. Med. 1990, 323, 725–731. [Google Scholar] [CrossRef]
- Daigle, M.; Weinstein, A.; Katz, J.; Losina, E. The cost-effectiveness of total joint arthroplasty: A systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 2012, 26, 649–658. [Google Scholar] [CrossRef]
- Dakin, H.; Gray, A.; Fitzpatrick, R.; MacLennan, G.; Murray, D. Rationing of total knee replacement: A cost-effectiveness analysis on a large trial data set. BMJ Open 2012, 2, e000332. [Google Scholar] [CrossRef]
- Brittain, R.; Howard, P.; Lawrence, S.; Stonadge, J.; Wilkinson, M.; Wilton, T. NJR Statistical Analysis, Support and Associated Services National Joint Registry|19th Annual Report. Available online: https://www.njrcentre.org.uk/njr-annual-report-2022/ (accessed on 1 April 2024).
- Culliford, D.; Maskell, J.; Judge, A.; Cooper, C.; Prieto-Alhambra, D.; Arden, N. Future projections of total hip and knee arthroplasty in the UK: Results from the UK Clinical Practice Research Datalink. Osteoarthr. Cartil. 2015, 23, 594–600. [Google Scholar] [CrossRef]
- Heath, E.; Ackerman, I.; Cashman, K.; Lorimer, M.; Graves, S.; Harris, I. Patient-reported outcomes after hip and knee arthroplasty: Results from a large national registry. Bone Jt. Open 2021, 2, 422–432. [Google Scholar] [CrossRef]
- Dash, S.; Palo, N.; Arora, G.; Chandel, S.; Kumar, M. Effects of preoperative walking ability and patient’s surgical education on quality of life and functional outcomes after total knee arthroplasty. Rev. Bras. Ortop. 2017, 52, 435. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.B.; Chesworth, B.; Davis, A.; Mahomed, N.; Charron, K. Comparing patient outcomes after THA and TKA: Is there a difference? Clin. Orthop. Relat. Res. 2010, 468, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Konnyu, K.J.; Thoma, L.M.; Cao, W.; Aaron, R.K.; Panagiotou, O.A.; Bhuma, M.R.; Adam, G.P.; Balk, E.M.; Pinto, D. Rehabilitation for total knee arthroplasty: A systematic review. Am. J. Phys. Med. Rehabil. 2023, 102, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Zanghelini, F.; Xydopoulos, G.; Fordham, R.; Rodgers, G.; Khanal, S. Early economic evaluation of the digital gait analysis system for fall prevention–Preliminary analysis of the GaitSmart system. Aging Med. 2024, 7, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Fatoye, F.; Yeowell, G.; Wright, J.; Gebrye, T. Clinical and cost-effectiveness of physiotherapy interventions following total knee replacement: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2021, 141, 1761–1778. [Google Scholar] [CrossRef]
- Larsen, K.; Hansen, T.B.; Thomsen, P.B.; Christiansen, T.; Søballe, K. Cost-effectiveness of accelerated perioperative care and rehabilitation after total hip and knee arthroplasty. J. Bone Jt. Surg. 2009, 91, 761–772. [Google Scholar] [CrossRef]
- Pritchard, M.G.; Murphy, J.; Cheng, L.; Janarthanan, R.; Judge, A.; Leal, J. Enhanced recovery following hip and knee arthroplasty: A systematic review of cost-effectiveness evidence. BMJ Open 2020, 10, e032204. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Augustovski, F.; de Bekker-Grob, E.; Briggs, A.; Carswell, C.; Caulley, L.; Chaiyakunapruk, N.; Greenberg, D.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) Statement: Updated Reporting Guidance for Health Economic Evaluations. Value Health 2022, 25, 3–9. [Google Scholar] [CrossRef]
- National Institute for Health Care Excellence. Joint Replacement (Primary): Hip, Knee and Shoulder|Quality Standards—206. Available online: https://www.nice.org.uk/guidance/qs206 (accessed on 21 February 2024).
- Abellan Van Kan, G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- Curtis, L.A.; Burns, A. Unit Costs of Health and Social Care 2020|PSSRU. 2020. Available online: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2020/ (accessed on 1 February 2021).
- McNamara, I.; Whitehouse, C.E.; Ward, N.; Hodgins, D.; Whalley, R. Sensor Data-Driven Personalised Hip and Knee Replacement Rehabilitation Compared to Standard of Care, Pilot Randomized Trial. Br. J. Healthc. Med. Res. 2023, 10, 54–71. [Google Scholar] [CrossRef]
- National Institute for Health Care Excellence. NICE Health Technology Evaluations: The Manual|Guidance. Available online: https://www.nice.org.uk/process/pmg36/chapter/introduction-to-health-technology-evaluation (accessed on 21 February 2024).
- Bolz, K.M.D.; Crawford, R.W.; Donnelly, B.; Whitehouse, S.L.; Graves, N. The cost-effectiveness of routine follow-up after primary total hip arthroplasty. J. Arthroplast. 2010, 25, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Fusco, F.; Campbell, H.; Barker, K. Rehabilitation after resurfacing hip arthroplasty: Cost-utility analysis alongside a randomized controlled trial. Clin. Rehabil. 2019, 33, 1003–1014. [Google Scholar] [CrossRef] [PubMed]
- Fusco, F.; Turchetti, G. Telerehabilitation after total knee replacement in Italy: Cost-effectiveness and cost-utility analysis of a mixed telerehabilitation-standard rehabilitation programme compared with usual care. BMJ Open 2016, 6, e009964. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.K. Interpretation of cost-effectiveness analyses. J. Gen. Intern. Med. 1998, 13, 716. [Google Scholar] [CrossRef] [PubMed]
- Sanders, G.D.; Maciejewski, M.L.; Basu, A. Overview of cost-effectiveness analysis. JAMA 2019, 321, 1400–1401. [Google Scholar] [CrossRef]
- Hunter, D.J.; March, L.; Chew, M. Osteoarthritis in 2020 and beyond: A Lancet Commission. Lancet 2020, 396, 1711–1712. [Google Scholar] [CrossRef]
- Hiligsmann, M.; Cooper, C.; Arden, N.; Boers, M.; Branco, J.C.; Brandi, M.L.; Bruyère, O.; Guillemin, F.; Hochberg, M.C.; Hunter, D.J. Health economics in the field of osteoarthritis: An expert’s consensus paper from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). In Seminars in Arthritis and Rheumatism; Elsevier: Amsterdam, The Netherlands, 2013; pp. 303–313. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Parameter | Deterministic Value | Probabilistic Value | Distribution | Source | |
|---|---|---|---|---|---|
| Transition Probabilities | Self-Managed Rehabilitation (SMR-SoC) | 0.200 | 0.208 | Beta | Expert Opinion |
| Self-Managed Rehabilitation (SMR-Int) | 0.000 | 0.000 | Beta | Expert Opinion | |
| SMR Response Probability | 0.400 | 0.394 | Beta | Expert Opinion | |
| SMR No Response Probability | 0.600 | 0.606 | Beta | Expert Opinion | |
| Costs (GBP) | Physiotherapy Cost | 10.333 | 11.126 | Gamma | [18] |
| Follow-Up Cost | 0.000 | 0.000 | Gamma | [18] | |
| Administration Cost | 1.553 | 1.009 | Gamma | [18] | |
| Utilities | QoL GIR Responder | 0.272 | 0.211 | Beta | [21] |
| QoL GIR No Responder | 0.256 | 0.202 | Beta | [21] |
| Parameter | Deterministic Value | Probabilistic Value | Distribution | Source | |
|---|---|---|---|---|---|
| Transition Probabilities | Group/Individual Rehabilitation (GIR-Soc) | 0.800 | 0.792 | Beta | Experts’ Opinion |
| Group/Individual Rehabilitation (GIR-Int) | 0.000 | 0.000 | Beta | Expert Opinion | |
| GIR Response | 0.400 | 0.399 | Beta | [25] | |
| GIR No Response | 0.600 | 0.601 | Beta | [25] | |
| Costs (GBP) | Physiotherapy Cost | 48.000 | 55.851 | Gamma | [24] |
| Secondary Care Costs | 57.000 | 49.387 | Gamma | [24] | |
| Follow-Up Cost | 0.000 | 0.000 | Gamma | [24] | |
| Administration Cost | 2.329 | 2.366 | Gamma | [24] | |
| Utilities | QoL GIR Responder | 0.272 | 0.201 | Beta | [25] |
| QoL GIR No Responder | 0.256 | 0.342 | Beta | [25] |
| Parameter | Deterministic Value | Probabilistic Value | Distribution | Source | |
|---|---|---|---|---|---|
| Transition Probabilities | GaitSmart Rehabilitation (GSR) | 1.000 | 1.000 | Beta | Assumption |
| GSR Response | 0.800 | 0.812 | Beta | [25] | |
| GSR No Response | 0.200 | 0.188 | Beta | [25] | |
| Primary Care | 0.000 | 0.000 | Beta | [25] | |
| Costs (GBP) | GaitSmart Intervention Cost Per Patient per Session | 10 | – | – | Manufacturer |
| Secondary Care Costs Per Patient per Session | 6.75 | 6.73 | Gamma | [24] | |
| Follow-Up Cost | 0.000 | 0.000 | Gamma | [24] | |
| Number of Sessions | 4 | – | [25] | ||
| Utilities | QoL GSR Responder | 0.285 | 0.314 | Beta | [25] |
| QoL GSR No Responder | 0.249 | 0.205 | Beta | [25] |
| Interventions | Mean Cost—£ | Incremental Cost—£ | Mean (QALYs) | Incremental (QALYs) | ICER—£ |
|---|---|---|---|---|---|
| SoC | 517.56 | - | 0.26 | - | - |
| GS | 67.00 | −450.56 | 0.28 | 0.02 | Dominant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanghelini, F.; Ponzo, A.; Xydopoulos, G.; Fordham, R.; Khanal, S. Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom. Geriatrics 2024, 9, 129. https://doi.org/10.3390/geriatrics9050129
Zanghelini F, Ponzo A, Xydopoulos G, Fordham R, Khanal S. Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom. Geriatrics. 2024; 9(5):129. https://doi.org/10.3390/geriatrics9050129
Chicago/Turabian StyleZanghelini, Fernando, Aisling Ponzo, Georgios Xydopoulos, Richard Fordham, and Saval Khanal. 2024. "Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom" Geriatrics 9, no. 5: 129. https://doi.org/10.3390/geriatrics9050129
APA StyleZanghelini, F., Ponzo, A., Xydopoulos, G., Fordham, R., & Khanal, S. (2024). Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom. Geriatrics, 9(5), 129. https://doi.org/10.3390/geriatrics9050129