
Clinical Factors and Biomarkers Associated with Depressive Disorders in Older Patients Affected by Chronic Kidney Disease (CKD): Does the Advanced Glycation End Products (AGEs)/RAGE (Receptor for AGEs) System Play Any Role?

 ,
,  , , ,
, , , 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection
2.2. Assessment of Depression and Cognitive Impairment
2.3. Frailty Assessment
2.4. Nutritional Status
2.5. AGE Quantification
2.6. sRAGE, esRAGE, and cRAGE Quantification
2.7. Cytokine Quantification
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferrucci, S.M.; Tavecchio, S.; Angileri, L.; Surace, T.; Berti, E.; Buoli, M. Factors Associated with Affective Symptoms and Quality of Life in Patients with Atopic Dermatitis. Acta Derm. Venereol. 2021, 101, adv00590. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Schioppo, T.; Ubiali, T.; Ostuzzi, S.; Bollati, V.; Buoli, M.; Caporali, R. Patient Perception of Depressive Symptoms in Rheumatic Diseases: A Cross-sectional Survey. J. Clin. Rheumatol. 2022, 28, e18–e22. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, Y.; Ma, L. Depression and cardiovascular disease in elderly: Current understanding. J. Clin. Neurosci. 2018, 47, 1–5. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Iodice, S.; Ceresa, A.; Esposito, C.M.; Mucci, F.; Conti, D.M.; Pergoli, L.; Tarantini, L.; Vigna, L.; Bollati, V.; Buoli, M.; et al. The Independent Role of Body Mass Index (BMI) and Severity of Depressive Symptoms on Biological Changes of Women Affected by Overweight/Obesity. Int. J. Environ. Res. Public Health 2021, 18, 2923. [Google Scholar] [CrossRef] [PubMed]
- Bautovich, A.; Katz, I.; Smith, M.; Loo, C.K.; Harvey, S.B. Depression and chronic kidney disease: A review for clinicians. Aust. N. Z. J. Psychiatry 2014, 48, 530–541. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.C.; Zhang, L.X. Prevalence and Disease Burden of Chronic Kidney Disease. Adv. Exp. Med. Biol. 2019, 1165, 3–15. [Google Scholar] [PubMed]
- Hedayati, S.S.; Minhajuddin, A.T.; Afshar, M.; Toto, R.D.; Trivedi, M.H.; Rush, A.J. Association between major depressive episodes in patients with chronic kidney disease and initiation of dialysis, hospitalization, or death. JAMA 2010, 303, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
- Guenzani, D.; Buoli, M.; Carnevali, G.S.; Serati, M.; Messa, P.; Vettoretti, S. Is there an association between severity of illness and psychiatric symptoms in patients with chronic renal failure. Psychol. Health Med. 2018, 23, 970–979. [Google Scholar] [CrossRef]
- Pu, L.; Zou, Y.; Wu, S.K.; Wang, F.; Zhang, Y.; Li, G.S.; Wang, J.W.; Zhang, L.X.; Zhao, M.H.; Wang, L. Prevalence and associated factors of depressive symptoms among chronic kidney disease patients in China: Results from the Chinese Cohort Study of Chronic Kidney Disease (C-STRIDE). J. Psychosom. Res. 2020, 128, 109869. [Google Scholar] [CrossRef]
- Fries, G.R.; Saldana, V.A.; Finnstein, J.; Rein, T. Molecular pathways of major depressive disorder converge on the synapse. Mol. Psychiatry 2023, 28, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ortega, M.; Rayego-Mateos, S.; Lamas, S.; Ortiz, A.; Rodrigues-Diez, R.R. Targeting the progression of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Ochodnicky, P.; Vettoretti, S.; Henning, R.H.; Buikema, H.; Van Dokkum, R.P.; de Zeeuw, D. Endothelial dysfunction in chronic kidney disease: Determinant of susceptibility to end-organ damage and therapeutic response. J. Nephrol. 2006, 19, 246–258. [Google Scholar]
- Zhang, W.R.; Parikh, C.R. Biomarkers of Acute and Chronic Kidney Disease. Annu. Rev. Physiol. 2019, 81, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Small, D.M.; Coombes, J.S.; Bennett, N.; Johnson, D.W.; Gobe, G.C. Oxidative stress, anti-oxidant therapies and chronic kidney disease. Nephrology 2012, 17, 311–332. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Gu, W.; Hepokoski, M.; Pham, H.; Tham, R.; Kim, Y.C.; Simonson, T.S.; Singh, P. Energy Metabolism Dysregulation in Chronic Kidney Disease. Kidney360 2023, 4, 1080–1094. [Google Scholar] [CrossRef] [PubMed]
- Ting, E.Y.; Yang, A.C.; Tsai, S.J. Role of Interleukin-6 in Depressive Disorder. Int. J. Mol. Sci. 2020, 21, 2194. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M.; Schatzberg, A.F. HPA axis in major depression: Cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef]
- Parekh, A.; Smeeth, D.; Milner, Y.; Thure, S. The Role of Lipid Biomarkers in Major Depression. Healthcare 2017, 5, 5. [Google Scholar] [CrossRef]
- Caldiroli, A.; Capuzzi, E.; Barkin, J.L.; Grassi, S.; Esposito, C.M.; Auxilia, A.M.; Russo, S.; Tagliabue, I.; Carnevali, G.S.; Mucci, F.; et al. Is there an association between inflammatory/anti-oxidant markers and the presence of psychotic symptoms or severity of illness in mood and psychotic disorders? A multi-centric study on a drug-free sample. Brain Behav. Immun. Health 2022, 22, 100453. [Google Scholar] [CrossRef]
- Guenzani, D.; Buoli, M.; Caldiroli, L.; Carnevali, G.S.; Serati, M.; Vezza, C.; Armelloni, S.; Messa, P.; Vettoretti, S. Malnutrition and inflammation are associated with severity of depressive and cognitive symptoms of old patients affected by chronic kidney disease. J. Psychosom. Res. 2019, 124, 109783. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Caldiroli, L.; Guenzani, D.; Carnevali, G.S.; Cesari, M.; Turolo, S.; Barkin, J.L.; Messa, P.; Agostoni, C.; Vettoretti, S. Associations Between Cholesterol and Fatty Acid Profile on the Severity of Depression in Older Persons with Nondialysis Chronic Kidney Disease. J. Ren. Nutr. 2021, 31, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Prasad, C.; Davis, K.E.; Imrhan, V.; Juma, S.; Vijayagopal, P. Advanced Glycation End Products and Risks for Chronic Diseases: Intervening Through Lifestyle Modification. Am. J. Lifestyle Med. 2019, 13, 384–404. [Google Scholar] [CrossRef] [PubMed]
- Garay-Sevilla, M.E.; Rojas, A.; Portero-Otin, M.; Uribarri, J. Dietary AGEs as Exogenous Boosters of Inflammation. Nutrients 2021, 13, 2802. [Google Scholar] [CrossRef] [PubMed]
- Vazzana, N.; Santilli, F.; Cuccurullo, C.; Davì, G. Soluble forms of RAGE in internal medicine. Intern. Emerg. Med. 2009, 4, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Dozio, E.; Briganti, S.; Delnevo, A.; Vianello, E.; Ermetici, F.; Secchi, F.; Sardanelli, F.; Morricone, L.; Malavazos, A.E.; Corsi Romanelli, M.M. Relationship between soluble receptor for advanced glycation end products (sRAGE), body composition and fat distribution in healthy women. Eur. J. Nutr. 2017, 56, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Dozio, E.; Vianello, E.; Sitzia, C.; Ambrogi, F.; Benedini, S.; Gorini, S.; Rampoldi, B.; Rigolini, R.; Tacchini, L.; Romanelli, M.M.C. Circulating Irisin and esRAGE as Early Biomarkers of Decline of Metabolic Health. J. Clin. Med. 2020, 9, 454. [Google Scholar] [CrossRef]
- Dozio, E.; Massaccesi, L.; Corsi Romanelli, M.M. Glycation and Glycosylation in Cardiovascular Remodeling: Focus on Advanced Glycation End Products and O-Linked Glycosylations as Glucose-Related Pathogenetic Factors and Disease Markers. J. Clin. Med. 2021, 10, 4792. [Google Scholar] [CrossRef] [PubMed]
- Caldiroli, L.; Molinari, P.; Dozio, E.; Rigolini, R.; Giubbilini, P.; Romanelli, M.M.C.; Castellano, G.; Vettoretti, S. In Patients with Chronic Kidney Disease Advanced Glycation End-Products Receptors Isoforms (sRAGE and esRAGE) Are Associated with Malnutrition. Antioxidants 2022, 11, 1253. [Google Scholar] [CrossRef]
- Dozio, E.; Caldiroli, L.; Molinari, P.; Castellano, G.; Delfrate, N.W.; Romanelli, M.M.C.; Vettoretti, S. Accelerated AGEing: The Impact of Advanced Glycation End Products on the Prognosis of Chronic Kidney Disease. Antioxidants 2023, 12, 584. [Google Scholar] [CrossRef]
- D’Cunha, N.M.; Sergi, D.; Lane, M.M.; Naumovski, N.; Gamage, E.; Rajendran, A.; Kouvari, M.; Gauci, S.; Dissanayka, T.; Marx, W.; et al. The Effects of Dietary Advanced Glycation End-Products on Neurocognitive and Mental Disorders. Nutrients 2022, 14, 2421. [Google Scholar] [CrossRef] [PubMed]
- van Dooren, F.E.; Pouwer, F.; Schalkwijk, C.G.; Sep, S.J.; Stehouwer, C.D.; Henry, R.M.; Dagnelie, P.C.; Schaper, N.C.; van der Kallen, C.J.; Koster, A.; et al. Advanced Glycation End Product (AGE) Accumulation in the Skin is Associated with Depression: The Maastricht Study. Depress. Anxiety 2017, 34, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Skali, H.; Uno, H.; Levey, A.S.; Inker, L.A.; Pfeffer, M.A.; Solomon, S.D. Prognostic assessment of estimated glomerular filtration rate by the new Chronic Kidney Disease Epidemiology Collaboration equation in comparison with the Modification of Diet in Renal Disease Study equation. Am. Heart J. 2011, 162, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G.; Meador, K.G.; Cohen, H.J.; Blazer, D.G. Self-rated depression scales and screening for major depression in the older hospitalized patient with medical illness. J. Am. Geriatr. Soc. 1988, 36, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Dong, J.; Sun, J.; Zhang, Y.; Ma, S.; Li, M.; Zhang, A.; Cheng, B.; Cai, S.; Bao, Q.; et al. Cognitive function assessed by Mini-mental state examination and risk of all-cause mortality: A community-based prospective cohort study. BMC Geriatr. 2021, 21, 524. [Google Scholar] [CrossRef] [PubMed]
- Helmer, C.; Stengel, B.; Metzger, M.; Froissart, M.; Massy, Z.A.; Tzourio, C.; Berr, C.; Dartigues, J.F. Chronic kidney disease, cognitive decline, and incident dementia: The 3C Study. Neurology 2011, 77, 2043–2051. [Google Scholar] [CrossRef] [PubMed]
- Shulman, K.I.; Shedletsky, R.; Silver, I.L. The challenge of time: Clock-drawing and cognitive function in the elderly. Int. J. Geriat. Psychiatry 1986, 1, 135–140. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef]
- Shen, Z.; Ruan, Q.; Yu, Z.; Sun, Z. Chronic kidney disease-related physical frailty and cognitive impairment: A systemic review. Geriatr. Gerontol. Int. 2017, 17, 529–544. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. A malnutrition-inflammation score is correlated with morbidity and mortality in maintenance hemodialysis patients. Am. J. Kidney Dis. 2001, 38, 1251–1263. [Google Scholar] [CrossRef] [PubMed]
- Amparo, F.C.; Kamimura, M.A.; Molnar, M.Z.; Cuppari, L.; Lindholm, B.; Amodeo, C.; Carrero, J.J.; Cordeiro, A.C. Diagnostic validation and prognostic significance of the Malnutrition-Inflammation Score in nondialyzed chronic kidney disease patients. Nephrol. Dial. Transplant. 2015, 30, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Rambod, M.; Bross, R.; Zitterkoph, J.; Benner, D.; Pithia, J.; Colman, S.; Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Association of Malnutrition-Inflammation Score with quality of life and mortality in hemodialysis patients: A 5-year prospective cohort study. Am. J. Kidney Dis. 2009, 53, 298–309. [Google Scholar] [CrossRef]
- Ho, L.C.; Wang, H.H.; Chiang, C.K.; Hung, K.Y.; Wu, K.D. Malnutrition-inflammation score independently determined cardiovascular and infection risk in peritoneal dialysis patients. Blood Purif. 2010, 30, 16–24. [Google Scholar] [CrossRef]
- He, T.; An, X.; Mao, H.P.; Wei, X.; Chen, J.H.; Guo, N.; Yang, X.; Li, Z.B.; Yu, X.Q.; Li, Z.J. Malnutrition-inflammation score predicts long-term mortality in Chinese PD patients. Clin. Nephrol. 2013, 79, 477–483. [Google Scholar] [CrossRef]
- Molnar, M.Z.; Czira, M.E.; Rudas, A.; Ujszaszi, A.; Lindner, A.; Fornadi, K.; Kiss, I.; Remport, A.; Novak, M.; Kennedy, S.H.; et al. Association of the malnutrition-inflammation score with clinical outcomes in kidney transplant recipients. Am. J. Kidney Dis. 2011, 58, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Afşar, B.; Sezer, S.; Ozdemir, F.N.; Celik, H.; Elsurer, R.; Haberal, M. Malnutrition-inflammation score is a useful tool in peritoneal dialysis patients. Perit. Dial. Int. 2006, 26, 705–711. [Google Scholar] [CrossRef]
- Yanagisawa, K.; Makita, Z.; Shiroshita, K.; Ueda, T.; Fusegawa, T.; Kuwajima, S.; Takeuchi, M.; Koike, T. Specific fluorescence assay for advanced glycation end products in blood and urine of diabetic patients. Metabolism 1998, 47, 1348–1353. [Google Scholar] [CrossRef]
- Guerin-Dubourg, A.; Cournot, M.; Planesse, C.; Debussche, X.; Meilhac, O.; Rondeau, P.; Bourdon, E. Association between Fluorescent Advanced Glycation End-Products and Vascular Complications in Type 2 Diabetic Patients. BioMed Res. Int. 2017, 2017, 7989180. [Google Scholar] [CrossRef]
- Dozio, E.; Vettoretti, S.; Caldiroli, L.; Nerini-Molteni, S.; Tacchini, L.; Ambrogi, F.; Messa, P.; Corsi Romanelli, M.M. Advanced Glycation End Products (AGE) and Soluble Forms of AGE Receptor: Emerging Role as Mortality Risk Factors in CKD. Biomedicines 2020, 8, 638. [Google Scholar] [CrossRef]
- Buoli, M.; Legnani, F.; Nosari, G.; Pan, A.; Ciappolino, V.; Esposito, C.M.; Ceresa, A.; Di Paolo, M.; Surace, T.; Auxilia, A.M.; et al. Which clinical factors and biochemical parameters are associated with late-life major depression. Int. J. Psychiatry Clin. Pract. 2023, 27, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Vecchio, M.; Craig, J.C.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; Pellegrini, F.; Saglimbene, V.; Logroscino, G.; Fishbane, S.; et al. Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int. 2013, 84, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Fabrazzo, M.; De Santo, R.M. Depression in chronic kidney disease. Semin. Nephrol. 2006, 26, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.; Xie, D.; Wang, X.; Jordan, N.; Ricardo, A.C.; Anderson, A.H.; Diamantidis, C.J.; Kusek, J.W.; Yaffe, K.; Lash, J.P.; et al. Depressive Symptoms, Antidepressants, and Clinical Outcomes in Chronic Kidney Disease: Findings from the CRIC Study. Kidney Med. 2024, 6, 100790. [Google Scholar] [CrossRef] [PubMed]
- Jeyasingam, N.; McLean, L.; Mitchell, L.; Wand, A.P.F. Attitudes to ageing amongst health care professionals: A qualitative systematic review. Eur. Geriatr. Med. 2023, 14, 889–908. [Google Scholar] [CrossRef]
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Fracas, E.; Costantino, A.; Vecchi, M.; Buoli, M. Depressive and Anxiety Disorders in Patients with Inflammatory Bowel Diseases: Are There Any Gender Differences. Int. J. Environ. Res. Public Health 2023, 20, 6255. [Google Scholar] [CrossRef]
- García-Montero, C.; Ortega, M.A.; Alvarez-Mon, M.A.; Fraile-Martinez, O.; Romero-Bazán, A.; Lahera, G.; Montes-Rodríguez, J.M.; Molina-Ruiz, R.M.; Mora, F.; Rodriguez-Jimenez, R.; et al. The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective. Nutrients 2022, 14, 1107. [Google Scholar] [CrossRef]
- Heck, A.L.; Handa, R.J. Sex differences in the hypothalamic-pituitary-adrenal axis’ response to stress: An important role for gonadal hormones. Neuropsychopharmacology 2019, 44, 45–58. [Google Scholar] [CrossRef]
- Yildiz, S.; Heybeli, C.; Smith, L.; Soysal, P.; Kazancioglu, R. The prevalence and clinical significance of loss of appetite in older patients with chronic kidney disease. Int. Urol. Nephrol. 2023, 55, 2295–2302. [Google Scholar] [CrossRef]
- Feng, L.; Yap, K.B.; Ng, T.P. Depressive symptoms in older adults with chronic kidney disease: Mortality, quality of life outcomes, and correlates. Am. J. Geriatr. Psychiatry 2013, 21, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Lis, M.; Miłuch, T.; Majdowski, M.; Zawodny, T. A link between ghrelin and major depressive disorder: A mini review. Front. Psychiatry 2024, 15, 1367523. [Google Scholar] [CrossRef] [PubMed]
- Graterol Torres, F.; Molina, M.; Soler-Majoral, J.; Romero-González, G.; Rodríguez Chitiva, N.; Troya-Saborido, M.; Socias Rullan, G.; Burgos, E.; Paúl Martínez, J.; Urrutia Jou, M.; et al. Evolving Concepts on Inflammatory Biomarkers and Malnutrition in Chronic Kidney Disease. Nutrients 2022, 14, 4297. [Google Scholar] [CrossRef] [PubMed]
- Drew, D.A.; Weiner, D.E.; Sarnak, M.J. Cognitive Impairment in CKD: Pathophysiology, Management, and Prevention. Am. J. Kidney Dis. 2019, 74, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Sejunaite, K.; Gaucher, F.; Lanza, C.; Riepe, M.W. Clock Drawing Test: Types of Errors and Accuracy in Early Cognitive Screening. J. Alzheimers Dis. 2023, 95, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Darcet, F.; Gardier, A.M.; Gaillard, R.; David, D.J.; Guilloux, J.P. Cognitive Dysfunction in Major Depressive Disorder. A Translational Review in Animal Models of the Disease. Pharmaceuticals 2016, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Pitsillou, E.; Bresnehan, S.M.; Kagarakis, E.A.; Wijoyo, S.J.; Liang, J.; Hung, A.; Karagiannis, T.C. The cellular and molecular basis of major depressive disorder: Towards a unified model for understanding clinical depression. Mol. Biol. Rep. 2020, 47, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Capuzzi, E.; Caldiroli, A.; Ceresa, A.; Esposito, C.M.; Posio, C.; Auxilia, A.M.; Capellazzi, M.; Tagliabue, I.; Surace, T.; et al. Clinical and Biological Factors Are Associated with Treatment-Resistant Depression. Behav. Sci. 2022, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.; Sohan, M.; Daria, S.; Masud, A.A.; Ahmed, M.U.; Roy, A.; Shahriar, M. Evaluation of inflammatory cytokines in drug-naïve major depressive disorder: A systematic review and meta-analysis. Int. J. Immunopathol. Pharmacol. 2023, 37, 3946320231198828. [Google Scholar] [CrossRef]
- Proma, M.A.; Daria, S.; Nahar, Z.; Ashraful Islam, S.M.; Bhuiyan, M.A.; Islam, M.R. Monocyte chemoattractant protein-1 levels are associated with major depressive disorder. J. Basic Clin. Physiol. Pharmacol. 2022, 33, 735–741. [Google Scholar] [CrossRef]
- Lehto, S.M.; Niskanen, L.; Herzig, K.H.; Tolmunen, T.; Huotari, A.; Viinamäki, H.; Koivumaa-Honkanen, H.; Honkalampi, K.; Ruotsalainen, H.; Hintikka, J. Serum chemokine levels in major depressive disorder. Psychoneuroendocrinology 2010, 35, 226–232. [Google Scholar] [CrossRef]
- Mélik-Parsadaniantz, S.; Rostène, W. Chemokines and neuromodulation. J. Neuroimmunol. 2008, 198, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.A.; McColl, A.; Graham, G.J.; Cavanagh, J. Sustained exposure to systemic endotoxin triggers chemokine induction in the brain followed by a rapid influx of leukocytes. J. Neuroinflammation 2020, 17, 94. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Anshita, D.; Ravichandiran, V. MCP-1: Function, regulation, and involvement in disease. Int. Immunopharmacol. 2021, 101, 107598. [Google Scholar] [CrossRef]
- Puthumana, J.; Thiessen-Philbrook, H.; Xu, L.; Coca, S.G.; Garg, A.X.; Himmelfarb, J.; Bhatraju, P.K.; Ikizler, T.A.; Siew, E.D.; Ware, L.B.; et al. Biomarkers of inflammation and repair in kidney disease progression. J. Clin. Investig. 2021, 131, e139927. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, K.; Xiang, Y.; Ma, B.; Li, H.; Li, Y.; Shi, Y.; Li, S.; Bai, Y. Role of MCP-1 as an inflammatory biomarker in nephropathy. Front. Immunol. 2023, 14, 1303076. [Google Scholar] [CrossRef]
- Maldonado-Ruiz, R.; Trujillo-Villarreal, L.A.; Montalvo-Martínez, L.; Mercado-Gómez, O.F.; Arriaga-Ávila, V.; Garza-Ocañas, L.; Ortiz-López, R.; Garza-Villarreal, E.A.; Guevara-Guzmán, R.; Camacho-Morales, A. MCP-1 Signaling Disrupts Social Behavior by Modulating Brain Volumetric Changes and Microglia Morphology. Mol. Neurobiol. 2022, 59, 932–994. [Google Scholar] [CrossRef] [PubMed]
- Molinari, P.; Caldiroli, L.; Dozio, E.; Rigolini, R.; Giubbilini, P.; Romanelli, M.M.C.; Messa, P.; Vettoretti, S. AGEs and sRAGE Variations at Different Timepoints in Patients with Chronic Kidney Disease. Antioxidants 2021, 10, 1994. [Google Scholar] [CrossRef]
- Koska, J.; Gerstein, H.C.; Beisswenger, P.J.; Reaven, P.D. Advanced Glycation End Products Predict Loss of Renal Function and High-Risk Chronic Kidney Disease in Type 2 Diabetes. Diabetes Care 2022, 45, 684–691. [Google Scholar] [CrossRef]
- Lotan, R.; Ganmore, I.; Livny, A.; Itzhaki, N.; Waserman, M.; Shelly, S.; Zacharia, M.; Moshier, E.; Uribarri, J.; Beisswenger, P.; et al. Effect of Advanced Glycation End Products on Cognition in Older Adults with Type 2 Diabetes: Results from a Pilot Clinical Trial. J. Alzheimers Dis. 2021, 82, 1785–1795. [Google Scholar] [CrossRef]
- Bär, K.J.; Franke, S.; Wenda, B.; Müller, S.; Kientsch-Engel, R.; Stein, G.; Sauer, H. Pentosidine and N(epsilon)-(carboxymethyl)-lysine in Alzheimer’s disease and vascular dementia. Neurobiol. Aging 2003, 24, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, D.A.; Hardas, S.S.; Lange, M.L. Oxidatively modified glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and Alzheimer’s disease: Many pathways to neurodegeneration. J. Alzheimers Dis. 2010, 20, 369–393. [Google Scholar] [CrossRef] [PubMed]
- Berends, E.; van Oostenbrugge, R.J.; Foulquier, S.; Schalkwijk, C.G. Methylglyoxal, a highly reactive dicarbonyl compound, as a threat for blood brain barrier integrity. Fluids Barriers CNS 2023, 20, 75. [Google Scholar] [CrossRef] [PubMed]
- Smit, A.J.; Hartog, J.W.; Voors, A.A.; van Veldhuisen, D.J. Advanced glycation endproducts in chronic heart failure. Ann. N. Y. Acad. Sci. 2008, 1126, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Koetsier, M.; Lutgers, H.L.; de Jonge, C.; Links, T.P.; Smit, A.J.; Graaff, R. Reference values of skin autofluorescence. Diabetes Technol. Ther. 2010, 12, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Yue, X.; Hu, H.; Koetsier, M.; Graaff, R.; Han, C. Reference values for the Chinese population of skin autofluorescence as a marker of advanced glycation end products accumulated in tissue. Diabet. Med. 2011, 28, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Tani, Y.; Asai, J.; Nemoto, F.; Kusano, Y.; Suzuki, H.; Hayashi, Y.; Asahi, K.; Nakayama, M.; Miyata, T.; et al. Skin autofluorescence is associated with severity of vascular complications in Japanese patients with Type 2 diabetes. Diabet. Med. 2012, 29, 492–500. [Google Scholar] [CrossRef]
- Mook-Kanamori, M.J.; Selim, M.M.E.-D.; Takiddin, A.H.; Al-Homsi, H.; Al-Mahmoud, K.a.S.; Al-Obaidli, A.; Zirie, M.A.; Rowe, J.; Gherbi, W.S.; Chidiac, O.M.; et al. Ethnic and gender differences in advanced glycation end products measured by skin auto-fluorescence. Dermato-Endocrinology 2013, 5, 325–330. [Google Scholar] [CrossRef]
- Martin, F.; Trebilcock, R.; Best, L. Effects of cyclosporin a on induced hit cell alkalinization. Life Sci. 1992, 51, 607–613. [Google Scholar] [CrossRef]
- Eriksson, M.D.; Eriksson, J.G.; Kautiainen, H.; Salonen, M.K.; Mikkola, T.M.; Kajantie, E.; Wasenius, N.; Von Bonsdorff, M.; Laine, M.K. Advanced glycation end products measured by skin autofluorescence are associated with melancholic depressive symptoms—Findings from Helsinki Birth Cohort Study. J. Psychosom. Res. 2021, 145, 110488. [Google Scholar] [CrossRef]
- Goodwin, R.D.; Dierker, L.C.; Wu, M.; Galea, S.; Hoven, C.W.; Weinberger, A.H. Trends in U.S. depression prevalence from 2015 to 2020: The widening treatment gap. Am. J. Prev. Med. 2022, 63, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Kogon, A.J.; Matheson, M.B.; Flynn, J.T.; Gerson, A.C.; Warady, B.A.; Furth, S.L.; Hooper, S.R.; Chronic Kidney Disease in Children (CKiD) Study Group. Depressive Symptoms in Children with Chronic Kidney Disease. J. Pediatr. 2016, 168, 164–170.e1. [Google Scholar] [CrossRef] [PubMed]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Gambaro, G.; Yabarek, T.; Graziani, M.S.; Gemelli, A.; Abaterusso, C.; Frigo, A.C.; Marchionna, N.; Citron, L.; Bonfante, L.; Grigoletto, F.; et al. Prevalence of CKD in northeastern Italy. Clin. J. Am. Soc. Nephrol. 2010, 5, 1946–1953. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total Sample | Depression − | Depression + | χ2 or t | OR (95% CI) | p | |
|---|---|---|---|---|---|---|---|
| N = 115 | N = 72 (62.6%) | N = 43 (37.4%) | |||||
| Sex | Male | 80 (69.6%) | 59 (81.9%) | 21 (48.8%) | 13.94 | 4.76 (2.04–11.10) | <0.01 |
| Female | 35 (30.4%) | 13 (18.1%) | 22 (51.2%) | ||||
| Age (years) | 79.7 ± 6.4 | 79.2 ± 6.9 | 80.6 ± 5.3 | 1.12 | N.A. | 0.27 | |
| Years of education | 10.8 ± 4.2 | 11.2 ± 4.4 | 10.1 ± 3.8 | 1.36 | N.A. | 0.18 | |
| BMI (kg/m2) | 28.1 ± 4.8 | 28.1 ± 4.4 | 27.0 ± 5.5 | 0.14 | N.A. | 0.89 | |
| Presence of a caregiver | Yes | 86 (74.8%) | 55 (76.4%) | 31 (72.1%) | 0.26 | 0.80 (0.34–1.89) | 0.61 |
| No | 29 (25.2%) | 17 (23.6%) | 12 (27.9%) | ||||
| Diabetes | Yes | 65 (56.5%) | 43 (59.7%) | 22 (51.2%) | 0.8 | 0.71 (0.33–1.51) | 0.37 |
| No | 50 (43.5%) | 29 (40.3%) | 21 (48.8%) | ||||
| Hypertension | Yes | 104 (90.4%) | 66 (91.7%) | 38 (88.4%) | 0.34 | 0.69 (0.20–2.42) | 0.56 |
| No | 11 (9.6%) | 6 (8.3%) | 5 (11.6%) | ||||
| Previous cardiovascular events | Yes | 63 (55.3%) | 40 (56.3%) | 23 (53.5%) | 0.09 | 0.89 (0.42–1.91) | 0.77 |
| No | 51 (44.7%) | 31 (43.7%) | 20 (46.5%) | ||||
| MIS | 6.24 ± 4.46 | 5.35 ± 3.28 | 7.74 ± 5.66 | 2.53 | N.A. | 0.02 | |
| Frailty status | Yes | 52 (45.2%) | 25 (34.7%) | 27 (62.8%) | 11.51 | N.A. | <0.01 |
| No | 15 (13.0%) | 14 (19.5%) | 1 (2.3%) | ||||
| Pre-frailty | 48 (41.8%) | 33 (45.8%) | 15 (34.9%) | ||||
| MMSE | 25.8 ± 3.1 | 25.0 ± 3.1 | 25.9 ± 3.1 | 0.08 | N.A. | 0.94 | |
| CDT | 3.3 ± 2.0 | 3.6 ± 1.9 | 2.8 ± 2.0 | 2.16 | N.A. | 0.03 | |
| Variables | Total Sample | Depression − | Depression + | t | p |
|---|---|---|---|---|---|
| N = 115 | N = 72 (62.6%) | N = 43 (37.4%) | |||
| Biochemical variables | |||||
| eGFR (mL/min/1.73 m2) | 24 ± 10 | 23 ± 10 | 25 ± 10 | 0.77 | 0.44 |
| Creatinine clearance (mL/min) | 27 ± 14 | 26 ± 13 | 28 ± 17 | 0.48 | 0.63 |
| Albumin (g/dL) | 4.0 ± 0.3 | 4.1 ± 0.4 | 4.0 ± 0.3 | 0.71 | 0.48 |
| Total cholesterol (mg/dL) | 166 ± 37 | 165 ± 36 | 170 ± 38 | 0.62 | 0.54 |
| HDL (mg/dL) | 53 ± 18 | 52 ± 18 | 54 ± 16 | 0.76 | 0.45 |
| LDL (mg/dL) | 113 ± 31 | 112 ± 29 | 114 ± 35 | 0.36 | 0.72 |
| Vitamin D (ng/mL) | 29 ± 17 | 28 ± 15 | 31 ± 19 | 0.95 | 0.35 |
| Systemic inflammation | |||||
| CRP (mg/L) * | 0.2 (0.1–0.4) | 0.2 (0.1–0.5) | 0.2 (0.1–0.4) | 0.55 | 0.59 |
| Leukocytes (cells/mm3) | 6920 ± 1704 | 6951 ± 1856 | 6866 ± 1424 | 0.26 | 0.78 |
| NLR | 2.7 ± 1.4 | 2.8 ± 1.3 | 2.7± 1.4 | 0.37 | 0.71 |
| IL-10 (pg/mL) [3.6; 0–14.1] * | 1.9 (0.9–11.1) | 1.9 (0.9–13.9) | 1.8 (0.5–10.6) | 0.21 | 0.83 |
| Missing n = 10 | |||||
| IL-6 (pg/mL) [43; 0–149] | 3.9 ± 2.8 | 4.1 ± 2.7 | 3.6 ± 2.9 | 0.9 | 0.37 |
| Missing n = 7 | |||||
| IL-17 (pg/mL) [<31.3] | 0.4 ± 1.1 | 0.2 ± 0.7 | 0.7 ± 1.6 | 1.57 | 0.13 |
| Missing n = 9 | |||||
| IL-12p70 (pg/mL) [<7.8] | 1.7 ± 3.0 | 1.5 ± 2.3 | 1.9 ± 3.9 | 0.64 | 0.52 |
| Missing n = 8 | |||||
| TNF-α (pg/mL) [<2] | 15.2 ± 8.2 | 15.0 ± 8.6 | 15.5 ± 7.6 | 0.32 | 0.75 |
| Missing n = 8 | |||||
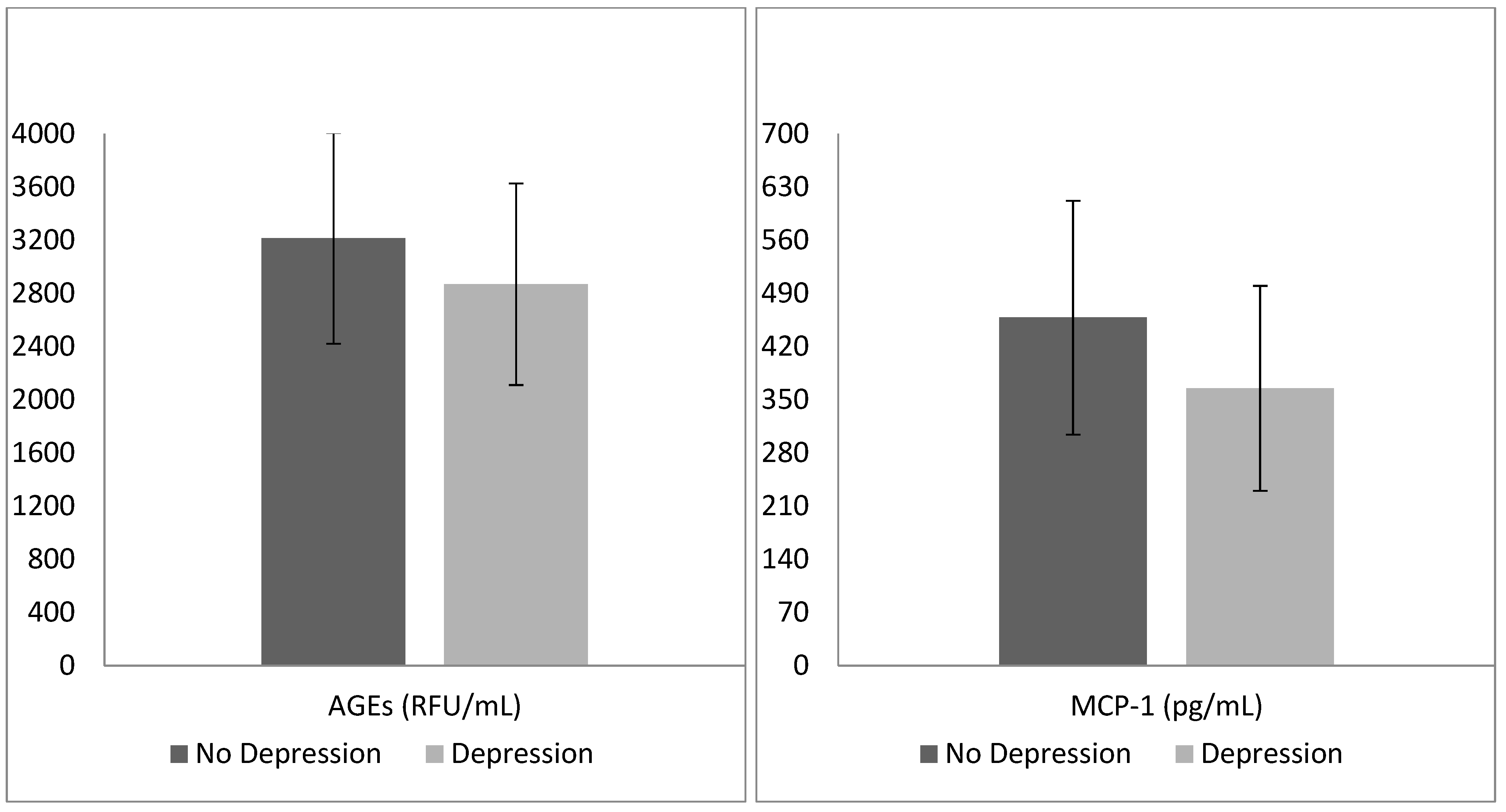
| MCP-1 (pg/mL) | 425 ± 154 | 458 ± 154 | 365 ± 135 | 2.99 | <0.01 |
| [423; 280.2–501.2] | |||||
| Missing n = 18 | |||||
| Advanced glycation end products | |||||
| AGEs (RFU/mL) | 3083 ± 794 | 3215 ± 793 | 2869 ± 759 | 2.2 | 0.03 |
| Missing n = 10 | |||||
| sRAGEs (pg/mL) | 2346 ± 1305 | 2416 ± 1263 | 2232 ± 1380 | 0.7 | 0.48 |
| [640; 365.5–1028] | |||||
| Missing n = 10 | |||||
| esRAGEs (pg/mL) | 663 ± 478 | 664 ± 470 | 662 ± 498 | 0.02 | 0.98 |
| [338.7; 121.8–796.2] | |||||
| Missing n = 11 | |||||
| cRAGEs (pg/mL) | 1692 ± 961 | 1753 ± 969 | 1592 ± 953 | 0.82 | 0.41 |
| [286.3; 2.23–564.7] | |||||
| Missing n = 11 | |||||
| AGEs/sRAGEs | 1.70 ± 0.99 | 1.69 ± 0.96 | 1.73 ± 1.04 | 0.18 | 0.86 |
| Missing n = 10 | |||||
| Variables | B | SE | Wald | p | EXP(B) | 95% CI for OR | |
|---|---|---|---|---|---|---|---|
| Sex | 2.38 | 0.79 | 9.05 | <0.01 | 10.77 | 2.29–50.71 | |
| Frailty | Pre-frail | 1.83 | 1.38 | 1.76 | 0.18 | 6.23 | 0.42–92.69 |
| Frail | 1.09 | 1.23 | 0.79 | 0.38 | 2.98 | 0.27–33.24 | |
| MIS | 0.16 | 0.1 | 2.71 | 0.1 | 1.17 | 0.97–1.42 | |
| CDT score | 0.03 | 0.16 | 0.05 | 0.83 | 1.03 | 0.76–1.41 | |
| Missing n = 2 | |||||||
| MCP-1 (pg/mL) | −0.01 | <0.01 | 8.85 | <0.01 | 0.99 | 0.98–0.99 | |
| Missing n = 18 | |||||||
| AGEs (RFU/mL) | <−0.01 | <0.01 | 8.87 | <0.01 | 0.1 | 0.997–0.999 | |
| Missing = 10 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buoli, M.; Dozio, E.; Caldiroli, L.; Armelloni, S.; Vianello, E.; Corsi Romanelli, M.; Castellano, G.; Vettoretti, S. Clinical Factors and Biomarkers Associated with Depressive Disorders in Older Patients Affected by Chronic Kidney Disease (CKD): Does the Advanced Glycation End Products (AGEs)/RAGE (Receptor for AGEs) System Play Any Role? Geriatrics 2024, 9, 99. https://doi.org/10.3390/geriatrics9040099
Buoli M, Dozio E, Caldiroli L, Armelloni S, Vianello E, Corsi Romanelli M, Castellano G, Vettoretti S. Clinical Factors and Biomarkers Associated with Depressive Disorders in Older Patients Affected by Chronic Kidney Disease (CKD): Does the Advanced Glycation End Products (AGEs)/RAGE (Receptor for AGEs) System Play Any Role? Geriatrics. 2024; 9(4):99. https://doi.org/10.3390/geriatrics9040099
Chicago/Turabian StyleBuoli, Massimiliano, Elena Dozio, Lara Caldiroli, Silvia Armelloni, Elena Vianello, Massimiliano Corsi Romanelli, Giuseppe Castellano, and Simone Vettoretti. 2024. "Clinical Factors and Biomarkers Associated with Depressive Disorders in Older Patients Affected by Chronic Kidney Disease (CKD): Does the Advanced Glycation End Products (AGEs)/RAGE (Receptor for AGEs) System Play Any Role?" Geriatrics 9, no. 4: 99. https://doi.org/10.3390/geriatrics9040099
APA StyleBuoli, M., Dozio, E., Caldiroli, L., Armelloni, S., Vianello, E., Corsi Romanelli, M., Castellano, G., & Vettoretti, S. (2024). Clinical Factors and Biomarkers Associated with Depressive Disorders in Older Patients Affected by Chronic Kidney Disease (CKD): Does the Advanced Glycation End Products (AGEs)/RAGE (Receptor for AGEs) System Play Any Role? Geriatrics, 9(4), 99. https://doi.org/10.3390/geriatrics9040099