

The Development and Evaluation of an Animated Video for Pre- and Postoperative Instructions for Patients with Osteoarthritis—A Design Science Research Approach




Abstract
1. Introduction
2. Materials and Methods
3. Results: The Rigor Cycle
3.1. Related Work
3.2. Understanding Osteoarthritis and Its Treatments
3.2.1. Osteoarthritis Disease
3.2.2. Osteoarthritis Surgical Treatment and Its Pre- and Post-Arrangements
3.3. Technology Adoption and 3D Interfaces
4. Results: The Relevance Cycle
5. Results: The Design Cycle
5.1. First Design Cycle—Animation Exploration
5.2. Second Design Cycle—Design Validation
5.3. Third Design Cycle—Validation after Implementation
6. Limitations
7. Conclusions and Further Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cope, P.J.; Ourradi, K.; Li, Y.; Sharif, M. Models of osteoarthritis: The good, the bad and the promising. Osteoarthr. Cartil. 2019, 27, 230–239. [Google Scholar] [CrossRef]
- Arden, E.; Arden, N.K.; Hunter, D. Osteoarthritis; Oxford University Press: Oxford, UK, 2008; Volume 93. [Google Scholar]
- Palazzo, C.; Nguyen, C.; Lefevre-Colau, M.M.; Rannou, F.; Poiraudeau, S. Risk factors and burden of osteoarthritis. Ann. Phys. Rehabil. Med. 2016, 59, 134–138. [Google Scholar] [CrossRef]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar]
- Castell, M.V.; Van Der Pas, S.; Otero, A.; Siviero, P.; Dennison, E.; Denkinger, M.; Pedersen, N.; Sanchez-Martinez, M.; Queipo, R.; van Schoor, N.; et al. Osteoarthritis and frailty in elderly individuals across six European countries: Results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet. Disord. 2015, 16, 359. [Google Scholar] [CrossRef] [PubMed]
- Hiscock, J.E. ‘How are you Managing your Arthritis?’: A Qualitative Research Contribution to Self-management Strategies for Osteoarthritis. Int. J. Interdiscip. Soc. Sci. 2010, 5, 467–476. [Google Scholar] [CrossRef]
- Hamel, M.B.; Toth, M.; Legedza, A.; Rosen, M.P. Joint replacement surgery in elderly patients with severe osteoarthritis of the hip or knee: Decision making, postoperative recovery, and clinical outcomes. Arch. Intern. Med. 2008, 168, 1430–1440. [Google Scholar] [CrossRef] [PubMed]
- Moralidou, M.; Di Laura, A.; Henckel, J.; Hothi, H.; Hart, A.J. Three-dimensional pre-operative planning of primary hip arthroplasty: A systematic literature review. EFORT Open Rev. 2020, 5, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Edwards, P.K.; Mears, S.C.; Lowry Barnes, C. Preoperative education for hip and knee replacement: Never stop learning. Curr. Rev. Musculoskelet. Med. 2017, 10, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Westby, M.D.; Backman, C.L. Patient and health professional views on rehabilitation practices and outcomes following total hip and knee arthroplasty for osteoarthritis: A focus group study. BMC Health Serv. Res. 2010, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.P. Patients’ memory for medical information. J. R. Soc. Med. 2003, 96, 219–222. [Google Scholar] [PubMed]
- Lawford, B.J.; Bennell, K.L.; Kasza, J.; Hinman, R.S. Physical Therapists’ Perceptions of Telephone-and Internet Video–Mediated Service Models for Exercise Management of People with Osteoarthritis. Arthritis Care Res. 2018, 70, 398–408. [Google Scholar] [CrossRef]
- Uesugi, Y.; Koyanagi, J.; Takagi, K.; Yamaguchi, R.; Hayashi, S.; Nishii, T. Exercise Therapy Interventions in Patients with Hip Osteoarthritis: Comparison of the Effects of DVD and Website-Based Interventions. JMIR Rehabil. Assist. Technol. 2018, 5, e10. [Google Scholar] [CrossRef]
- Gregório, J.; Reis, L.; Peyroteo, M.; Maia, M.; da Silva, M.M.; Lapão, L.V. The role of Design Science Research Methodology in developing pharmacy eHealth services. Res. Soc. Adm. Pharm. 2021, 17, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Storey, V.; Baskerville, R. Computational Science: A Field of Inquiry for Design Science Research. In Proceedings of the 55th Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2022. [Google Scholar]
- Hevner, A.R. A three cycle view of design science research. Scand. J. Inf. Syst. 2007, 19, 4. [Google Scholar]
- Hevner, A.R.; March, S.T.; Park, J.; Ram, S. Design science in information systems research. MIS Q. 2004, 28, 75–105. [Google Scholar] [CrossRef]
- Bider, I.; Perjons, E.; Johannesson, P. Just Finished a Cycle of a Design Science Research Project: What’s Next? Complex Syst. Inform. Model. Q. 2020, 22, 60–86. [Google Scholar] [CrossRef]
- Baskerville, R.; Kaul, M.; Storey, V. Unpacking the duality of design science. In Proceedings of the Thirty Second International Conference on Information Systems, Shanghai, China, 4–7 December 2011. [Google Scholar]
- Hevner, A.; Chatterjee, S. Design science research in information systems. In Design Research in Information Systems; Springer: Boston, MA, USA, 2010; pp. 9–22. [Google Scholar]
- Baskerville, R.; Baiyere, A.; Gregor, S.; Hevner, A.; Rossi, M. Design science research contributions: Finding a balance between artifact and theory. J. Assoc. Inf. Syst. 2018, 19, 3. [Google Scholar] [CrossRef]
- Pai, F.-Y.; Huang, K.-I. Applying the Technology Acceptance Model to the introduction of healthcare information systems. Technol. Forecast. Soc. Change 2011, 78, 650–660. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Marangunić, N.; Granić, A. Technology acceptance model: A literature review from 1986 to 2013. Univers. Access Inf. Soc. 2014, 14, 81–95. [Google Scholar] [CrossRef]
- Davis, F. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Park, N.; Rhoads, M.; Hou, J.; Lee, K.M. Understanding the acceptance of teleconferencing systems among employees: An extension of the technology acceptance model. Comput. Hum. Behav. 2014, 39, 118–127. [Google Scholar] [CrossRef]
- Bagozzi, R. The legacy of the Technology Acceptance Model and a proposal for a paradigm shift. J. Assoc. Inf. Syst. 2007, 8, 243–254. [Google Scholar] [CrossRef]
- Vogelsang, K.; Steinhüser, M.; Hoppe, U. A qualitative approach to examine technology acceptance. Res. Methods Philos. 2013, 17. [Google Scholar]
- Schuir, J.; Anton, E.; Eleks, M.; Teuteberg, F. Tell Me and I Forget, Involve Me and I Learn: Design and Evaluation of a Multimodal Conversational Agent for Supporting Distance Learning. In Proceedings of the 17th International Conference on Wirtschaftsinformatik, Nürnberg, Germany, 21–23 February 2022. [Google Scholar]
- Drechsler, A.; Hevner, A.R. A Four-Cycle Model of IS Design Science Research: Capturing the Dynamic. In Proceedings of the 11th International Conference on Design Science Research in Information Systems and Technology (DESRIST), St. John, NL, Canada, 23–25 May 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part | What We See (Imagery) | What We Hear (Dialogue) |
|---|---|---|
| A | The operation will be performed with either spinal anaesthesia, where only the lower part of the body is numb… | |
| B | …or under general anaesthesia where you are sedated during the procedure. | |
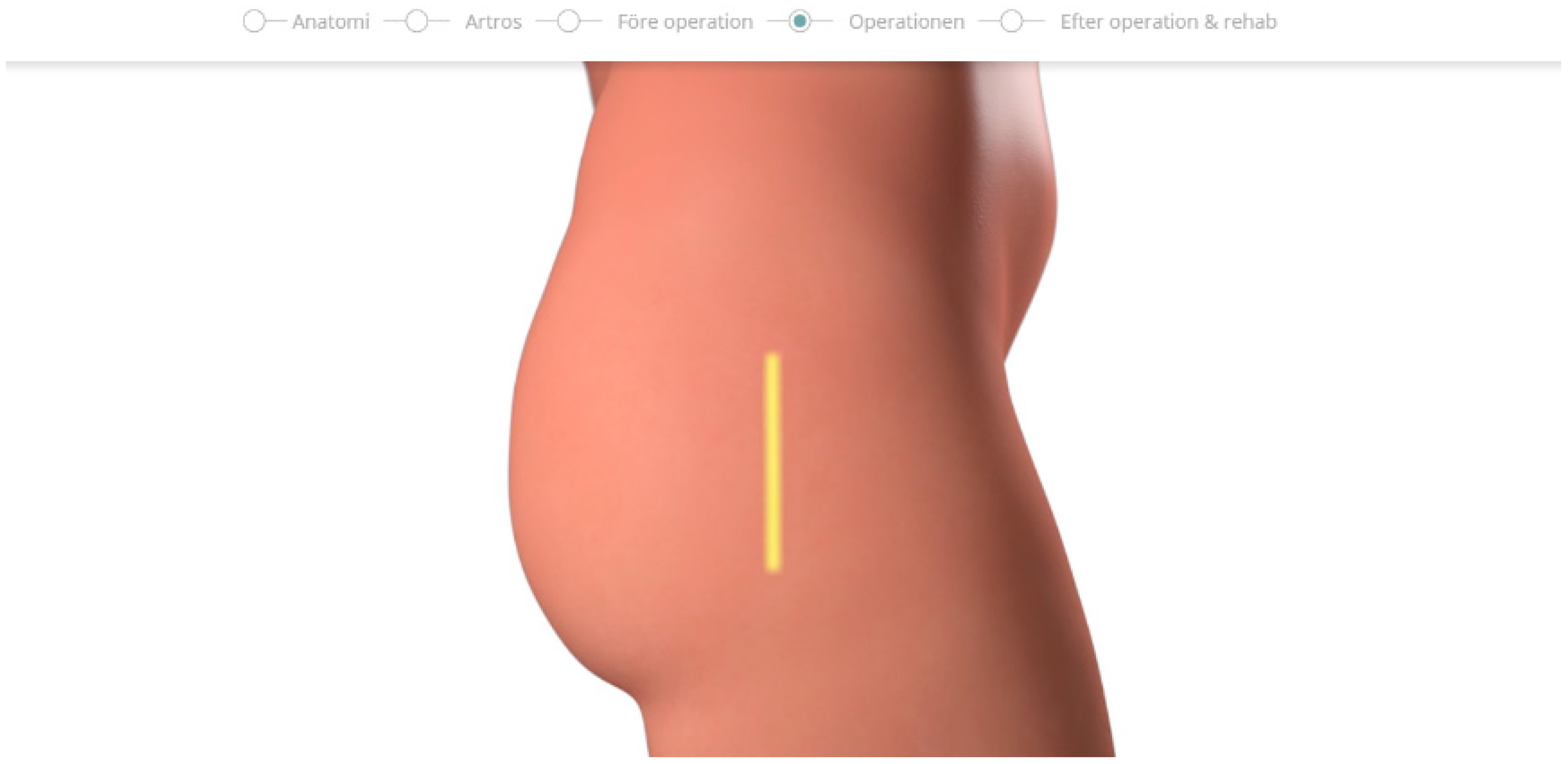
| C | The incision is approximately 15 cm long and will leave a visible scar. | |
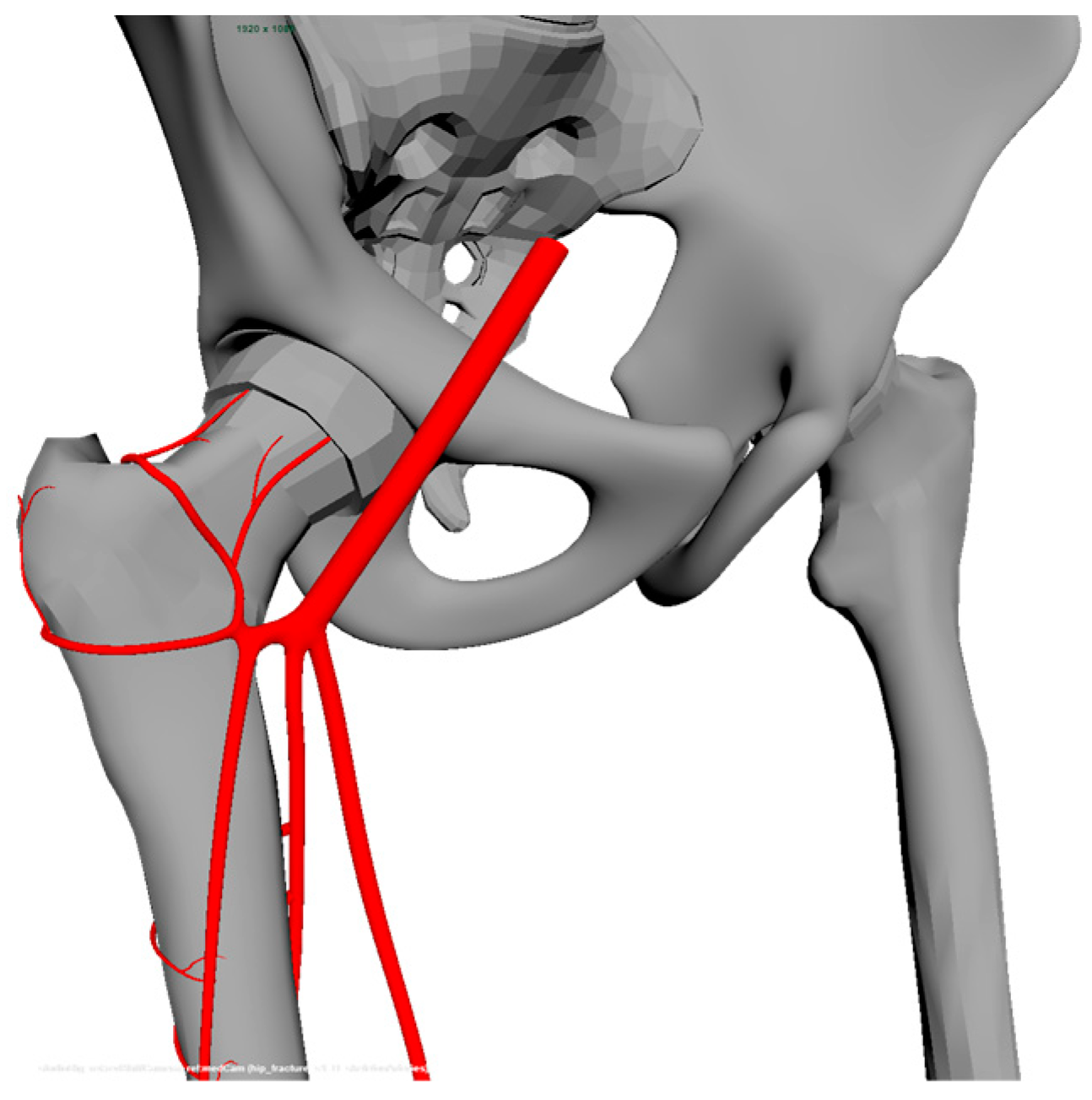
| D | The thigh bone is dislocated from the acetabulum. | |
| E | The acetabulum is resurfaced so that the prosthesis will fit. | |
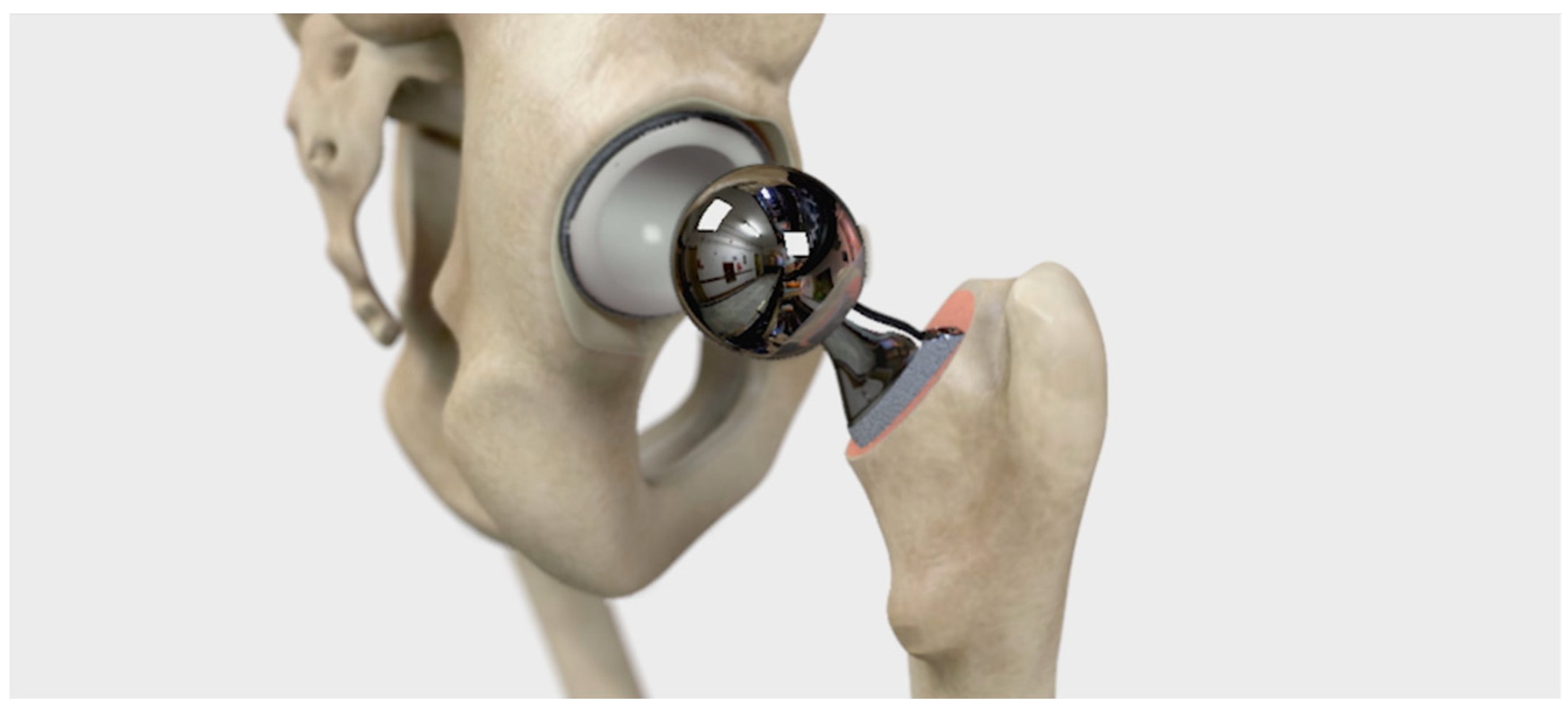
| F | The artificial hip component is then fitted to the acetabulum. | |
| G | A hole is made in the thigh bone to fit the thigh component. | |
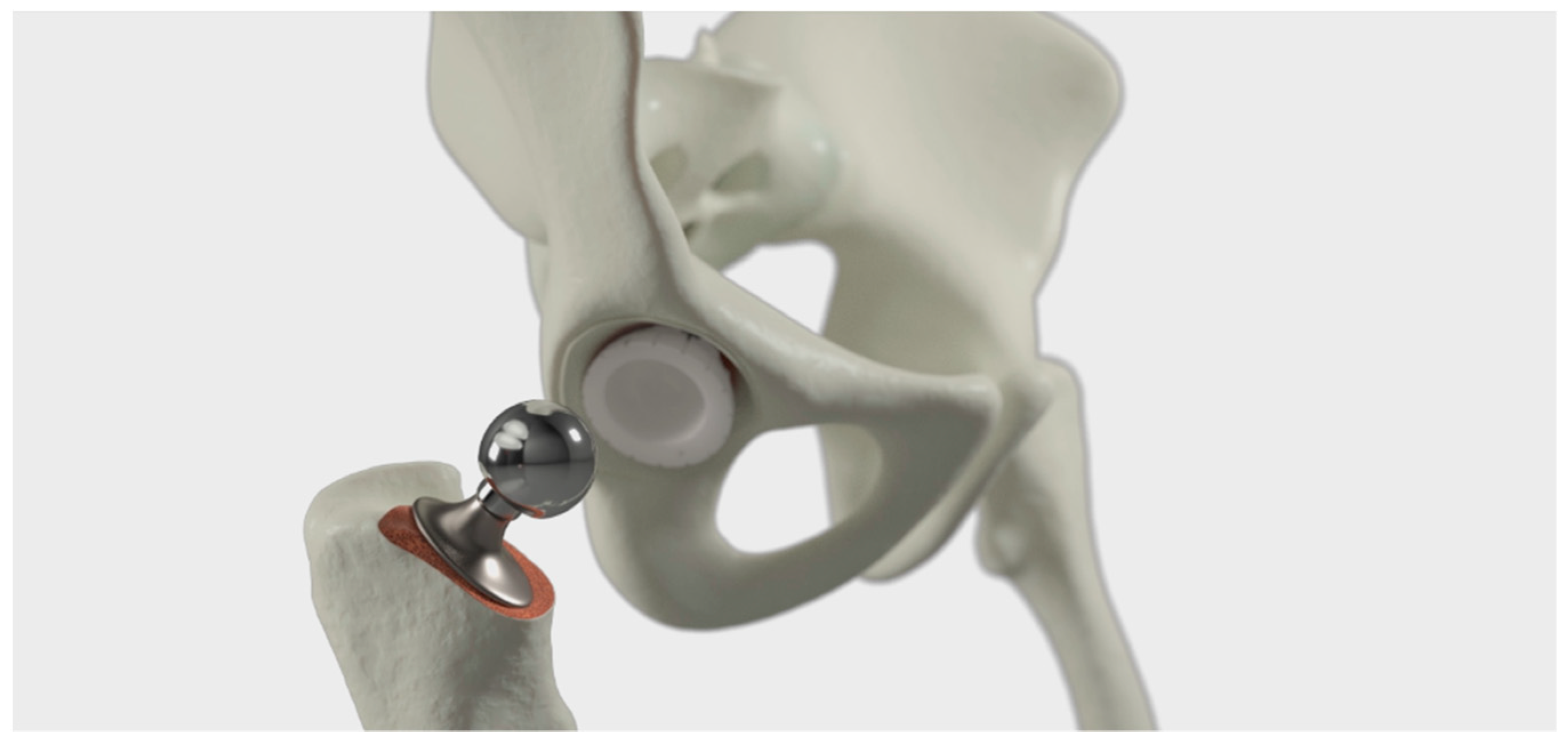
| H | The thigh component is then fitted in place. | |
| I | The components are fastened in place with or without the help of bone cement. | |
| J | The artificial ball joint is then placed onto the thigh component to complete the artificial hip. | |
| K | The incision is then closed and the wound is dressed. |
| Part | What We See (Imagery) | What We Hear (Dialogue) |
|---|---|---|
| A | Before surgery, you will receive spinal anaesthesia. You lie on your side and bring your elbows and knees together. | |
| B | When the lower part of your back is washed off with alcohol, the anaesthetist gives you an injection into the spine containing a local anaesthetic through a thin needle. | |
| C | The nerves in the lower part of your body are now anesthetized. | |
| D | The sting itself is hardly felt, but when the anaesthetic strikes, you will begin to feel warm in the legs and you will not be able to move them. | |
| E | During the operation, you can listen to music through headphones. You can also get a sedative so that you fall asleep during the procedure. | |
| F | It is not always possible to administer spinal anaesthesia. Instead, in these cases, we can give you a general anaesthesia. | |
| G | The type of anaesthetic we choose is determined after a consultation with your anaesthetist. | |
| H | The incision is around 15 cm long and will leave a visible scar. | |
| I | The thigh bone is dislocated from the acetabulum. | |
| J | The acetabulum is resurfaced so that the prosthesis will fit. | |
| K | The artificial hip component is then fitted to the acetabulum. | |
| L | A hole is made in the thigh bone to fit the thigh component. | |
| M | The thigh component is then fitted in place. | |
| N | The components are fastened in place with or without the help of bone cement. | |
| O | The artificial ball joint is then placed onto the thigh component to complete the artificial hip. | |
| P | The incision is then closed and the wound is dressed. | |
| Q | A hip replacement takes on average 60–90 min. Longer operating times may occur. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kylén, E.; Stenholm, J.; Johansson, M.; Aggestam, L.; Svensson, A. The Development and Evaluation of an Animated Video for Pre- and Postoperative Instructions for Patients with Osteoarthritis—A Design Science Research Approach. Geriatrics 2024, 9, 19. https://doi.org/10.3390/geriatrics9010019
Kylén E, Stenholm J, Johansson M, Aggestam L, Svensson A. The Development and Evaluation of an Animated Video for Pre- and Postoperative Instructions for Patients with Osteoarthritis—A Design Science Research Approach. Geriatrics. 2024; 9(1):19. https://doi.org/10.3390/geriatrics9010019
Chicago/Turabian StyleKylén, Erik, Joel Stenholm, Madeleine Johansson, Lena Aggestam, and Ann Svensson. 2024. "The Development and Evaluation of an Animated Video for Pre- and Postoperative Instructions for Patients with Osteoarthritis—A Design Science Research Approach" Geriatrics 9, no. 1: 19. https://doi.org/10.3390/geriatrics9010019
APA StyleKylén, E., Stenholm, J., Johansson, M., Aggestam, L., & Svensson, A. (2024). The Development and Evaluation of an Animated Video for Pre- and Postoperative Instructions for Patients with Osteoarthritis—A Design Science Research Approach. Geriatrics, 9(1), 19. https://doi.org/10.3390/geriatrics9010019