
Neglected Dislocation in Adults: A New Therapeutic Strategy for an Uncommon Condition

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
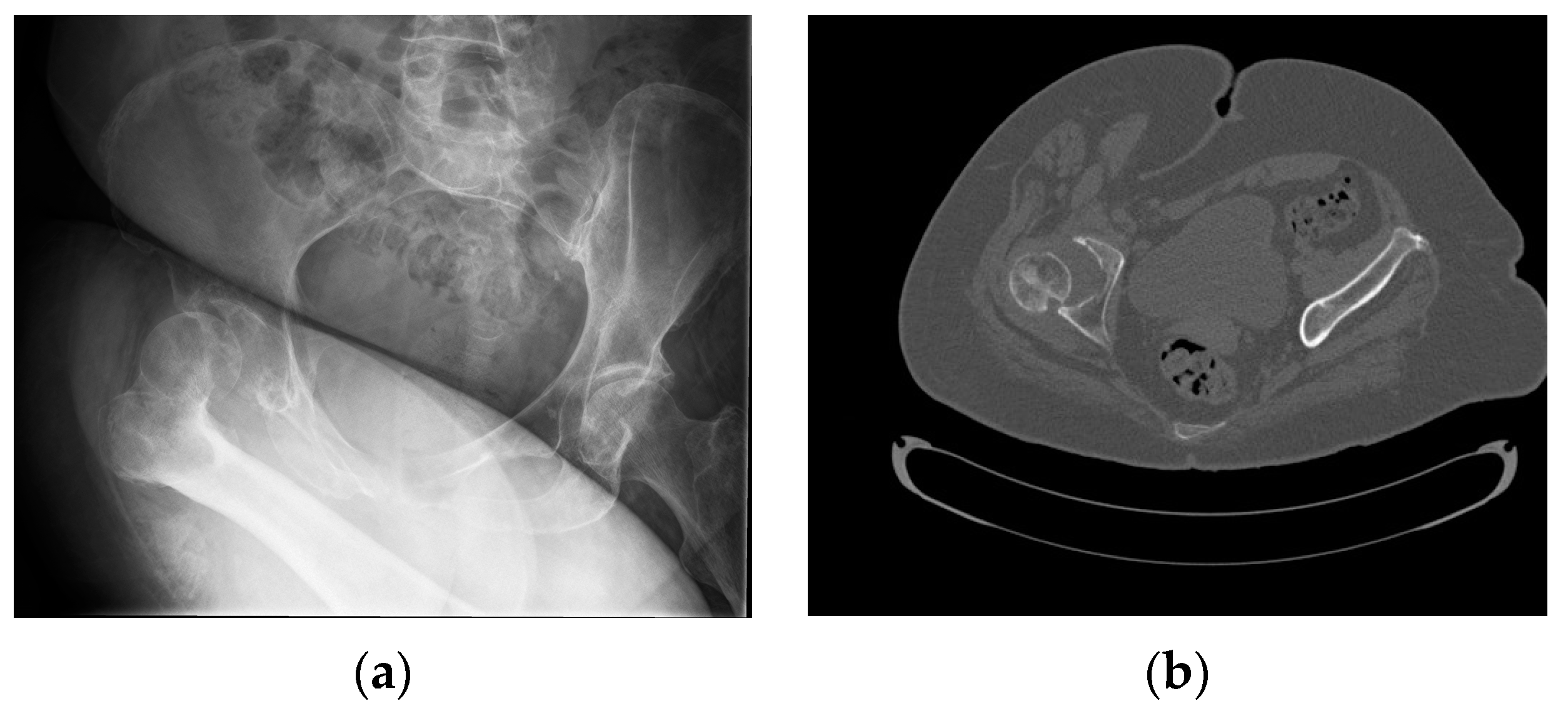
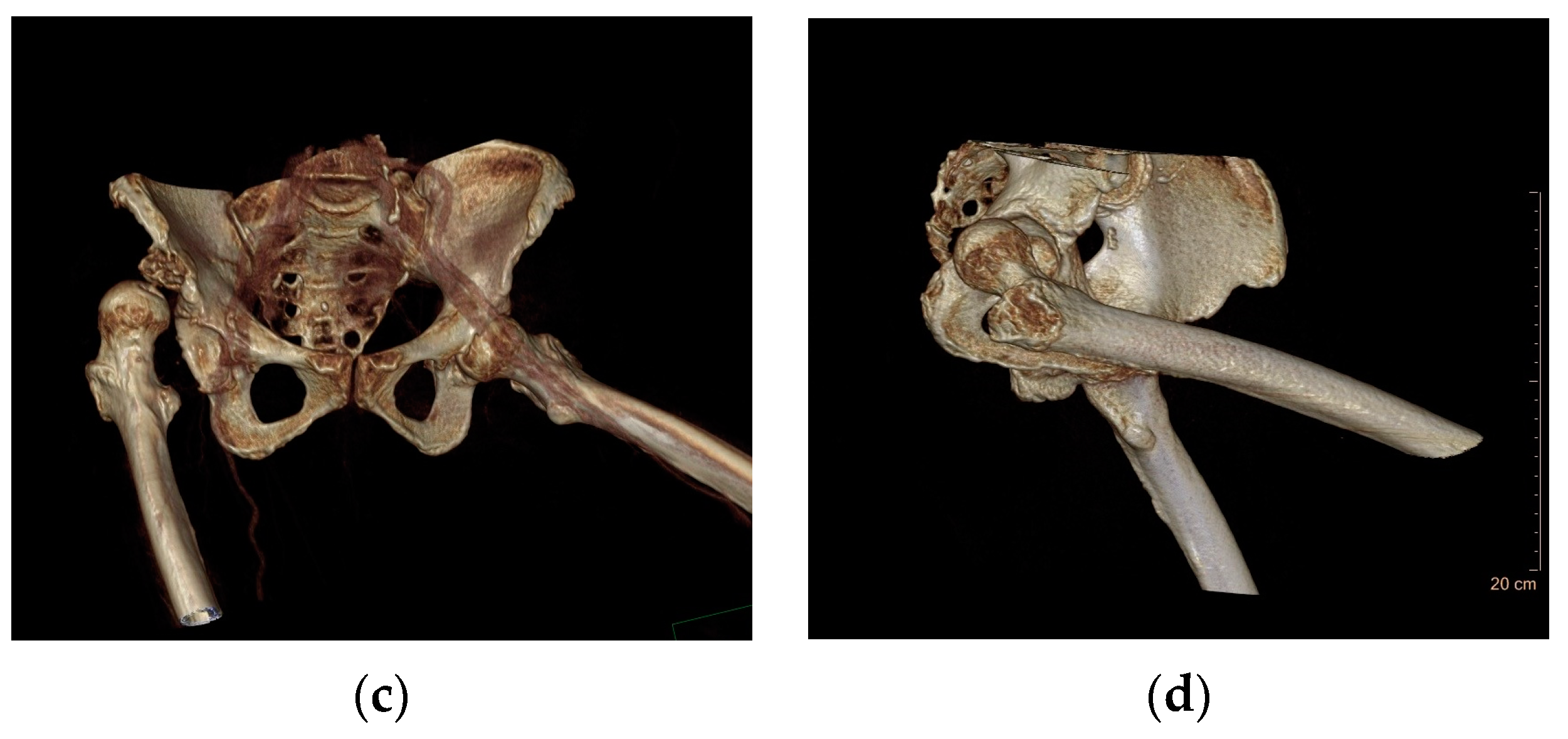
2. Case Presentation
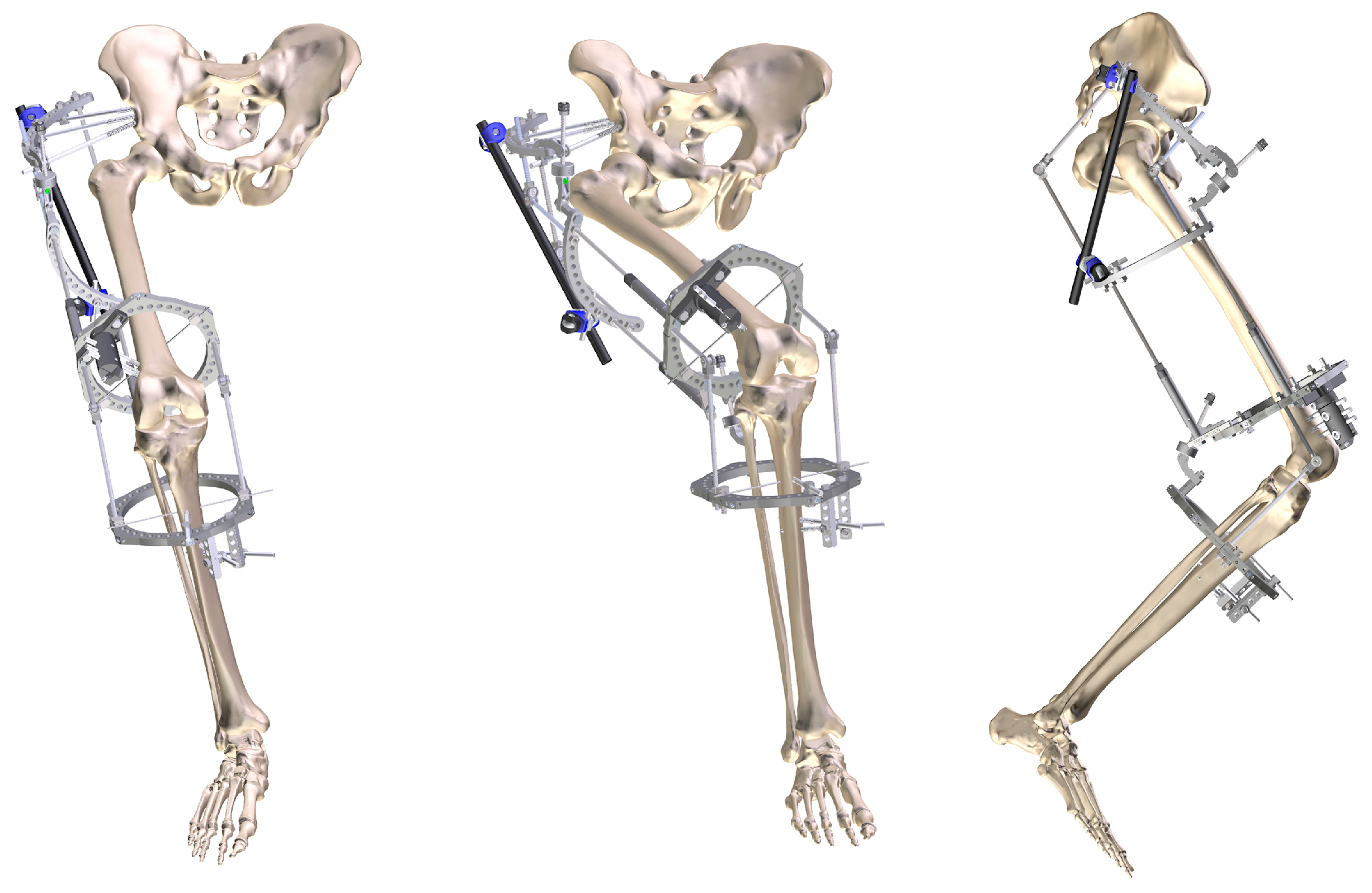
2.1. Two-Stage Open Reduction
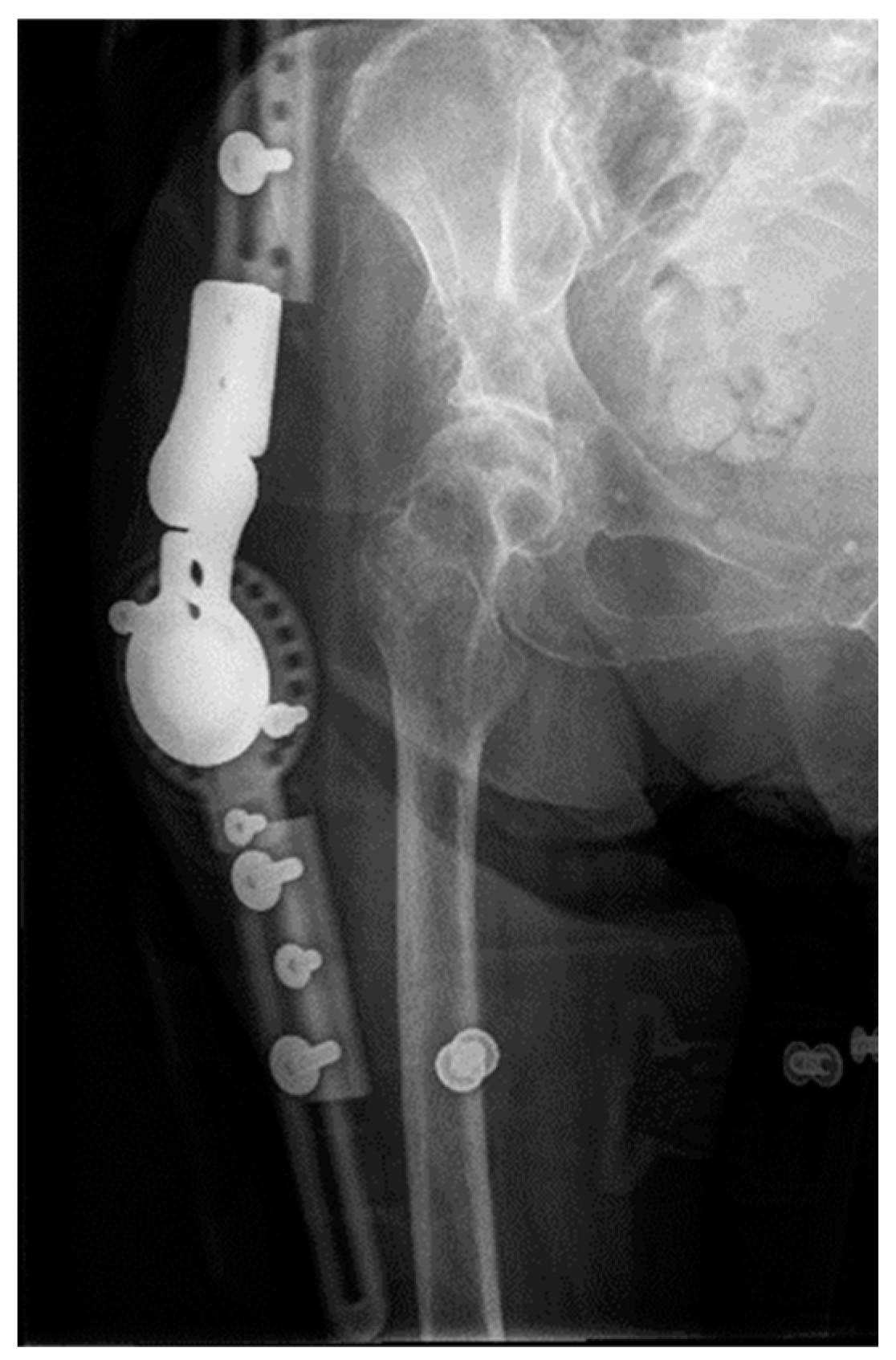
2.2. Complications after Treatment
2.3. Case Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blankenbaker, D.G.; De Smet, A.A. Hip injuries in athletes. Radiol. Clin. N. Am. 2010, 48, 1155–1178. [Google Scholar] [CrossRef]
- Moreta, J.; Foruria, X.; Sánchez, A.; Aguirre, U. Prognostic factors after a traumatic hip dislocation. A long-term retrospective study. Rev. Esp. Cir. Ortop. Traumatol. 2017, 61, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Massoud, E.I.E. Neglected traumatic hip dislocation: Influence of the increased intracapsular pressure. World J. Orthop. 2018, 9, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Hougaard, K.; Thomsen, P.B. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J. Bone Jt. Surg. Am. 1988, 70, 233–239. [Google Scholar] [CrossRef]
- Dawson-Amoah, K.; Raszewski, J.; Duplantier, N.; Waddell, B.S. Dislocation of the Hip: A Review of Types, Causes, and Treatment. Ochsner J. 2018, 18, 242–252. [Google Scholar] [CrossRef]
- Wojciechowski, P.; Kusz, D.J.; Cieliński, Ł.S.; Dudko, S.; Bereza, P.L. Neglected, developmental hip dislocation treated with external iliofemoral distraction, open reduction, and pelvic osteotomy. J. Pediatr. Orthop. B 2012, 21, 209–214. [Google Scholar] [CrossRef]
- Young, S.; Banza, L. Neglected traumatic anterior dislocation of the hip. Open reduction using the Bernese trochanter flip approach—A case report. Acta Orthop. 2017, 88, 348–350. [Google Scholar] [CrossRef]
- Upadhyay, S.S.; Moulton, A.; Burwell, R.G. Biological factors predisposing to traumatic posterior dislocation of the hip. A selection process in the mechanism of injury. J. Bone Jt. Surg. Br. 1985, 67, 232–236. [Google Scholar] [CrossRef]
- Gatin, L.; Khouri, N. Anterior hip dislocation in children with neurological disorders. A retrospective study of ten operated hips. Orthop. Traumatol. Surg. Res. 2015, 101, 55–60. [Google Scholar] [CrossRef]
- Banskota, A.K.; Spiegel, D.A.; Shrestha, S.; Shrestha, O.P.; Rajbhandary, T. Open reduction for neglected traumatic hip dislocation in children and adolescents. J. Pediatr. Orthop. 2007, 27, 187–191. [Google Scholar] [CrossRef]
- Nixon, J.R. Late open reduction of traumatic dislocation of the hip. Report of three cases. J. Bone Jt. Surg. Br. 1976, 58, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Clegg, T.E.; Roberts, C.S.; Greene, J.W.; Prather, B.A. Hip dislocations—Epidemiology, treatment, and outcomes. Injury 2010, 41, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.; Tejwani, N.; Egol, K.A. Traumatic hip dislocation—A review. Bull. NYU Hosp. Jt. Dis. 2010, 68, 91–96. [Google Scholar] [PubMed]
- Pai, V.S. The management of unreduced traumatic dislocation of the hip in developing countries. Int. Orthop. 1992, 16, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.C.; Shravat, B.P. Reduction of neglected traumatic dislocation of the hip by heavy traction. J. Bone Jt. Surg. Am. 1977, 59, 249–251. [Google Scholar] [CrossRef]
- Beebe, M.J.; Bauer, J.M.; Mir, H.R. Treatment of Hip Dislocations and Associated Injuries: Current State of Care. Orthop. Clin. N. Am. 2016, 47, 527–549. [Google Scholar] [CrossRef] [PubMed]
- Symeonides, P.P.; Pournaras, J.; Petsatodes, G.; Christoforides, J.; Hatzokos, I.; Pantazis, E. Total hip arthroplasty in neglected congenital dislocation of the hip. Clin. Orthop. Relat. Res. 1997, 341, 55–61. [Google Scholar] [CrossRef]
- Soufiane, B.; Naserddine, H.; Atif, M.; Abdelhamim, E.I.; Mohemmed, S.; Abdelmjide, E. Neglected traumatic dislocation of the hip treated with total hip arthroplasty: Report of 2 cases. Pan. Afr. Med. J. 2015, 20, 313. [Google Scholar]
- Kumar, S.; Dahuja, A.; Narula, M.S.; Garg, S.; Kaur, R. Neglected hip dislocation: An unusual presentation, its management and review of the literature. Strateg. Trauma Limb Reconstr. 2017, 12, 189–192. [Google Scholar] [CrossRef]
- Zajc, J.; Fokter, S.K. Bimodular femoral stems in primary total hip arthroplasty. Expert Rev. Med. Devices 2023, 20, 1051–1064. [Google Scholar] [CrossRef]
- Ko, L.M.; Hozack, W.J. The dual mobility cup. Bone Jt. J. 2016, 98, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Sharma, H.; Dreghorn, C.R.; Gardner, E.R. Girdlestone resection arthroplasty of the hip: Current perspectives. Curr. Orthop. 2005, 19, 385–392. [Google Scholar] [CrossRef]
- Alva, A.; Shetty, M.; Kumar, V. Old unreduced traumatic anterior dislocation of the hip. BMJ Case Rep. 2013, 2013, bcr2012008068. [Google Scholar] [CrossRef] [PubMed]
- Gomez, J.A.; Matsumoto, H.; Roye, D.P.; Vitale, M.G.; Hyman, J.E.; van Bosse, H.J.P.; Marangoz, S.; Sala, D.A.; Stein, M.I.; Feldman, D.S. Articulated hip distraction: A treatment option for femoral head avascular necrosis in adolescence. J. Pediatr. Orthop. 2009, 29, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Lee, C.W.; Kim, H.J.; Kim, H.H.; Wang, L. Treatment of Late-Onset Legg-Calve-Perthes Disease by Arthrodiastasis. Clin. Orthop. Surg. 2016, 8, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Aguado-Maestro, I.; Abril, J.C.; Bañuelos Diaz, A.; García Alonso, M. Hip arthrodiastasis in Legg-Calvé-Perthes disease. Rev. Esp. Cir. Ortop. Traumatol. 2016, 60, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Amer, A.R.A.L.; Khanfour, A.A. Arthrodiastasis for late onset Perthes’ disease using a simple frame and limited soft tissue release: Early results. Acta Orthop. Belg. 2011, 77, 472–479. [Google Scholar] [PubMed]
- Gutiérrez Carbonell, P. Arthrodiastasis followed by open reduction associated with pelvic and femoral osteotomies for the treatment of high inveterate congenital hip dislocation. J. Pediatr. Orthop. B 2018, 27, 479–484. [Google Scholar] [CrossRef]
- Flynn, J.M.; Miller, F. Management of hip disorders in patients with cerebral palsy. J. Am. Acad. Orthop. Surg. 2002, 10, 198–209. [Google Scholar] [CrossRef]
- Ilizarov, G.A. The tension-stress effect on the genesis and growth of tissues. Part I. The influence of stability of fixation and soft-tissue preservation. Clin. Orthop. Relat. Res. 1989, 238, 249–281. [Google Scholar] [CrossRef]
- Ciobanu, I.; Stanculescu (Badea), D.I.; Iliescu, A.; Popescu, A.M.; Seiciu, P.L.; Mikolajczyk, T.; Moldovan, F.; Berteanu, M. The usability pilot study of a mechatronic system for gait rehabilitation. Procedia Manuf. 2018, 22, 864–871. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García de la Blanca, J.C.; Cuarental García, J.; Luengo, G.; Martí, R.; Ramos, L.R. Neglected Dislocation in Adults: A New Therapeutic Strategy for an Uncommon Condition. Geriatrics 2023, 8, 117. https://doi.org/10.3390/geriatrics8060117
García de la Blanca JC, Cuarental García J, Luengo G, Martí R, Ramos LR. Neglected Dislocation in Adults: A New Therapeutic Strategy for an Uncommon Condition. Geriatrics. 2023; 8(6):117. https://doi.org/10.3390/geriatrics8060117
Chicago/Turabian StyleGarcía de la Blanca, Juan Carlos, Javier Cuarental García, Gonzalo Luengo, Rafael Martí, and Luis Rafael Ramos. 2023. "Neglected Dislocation in Adults: A New Therapeutic Strategy for an Uncommon Condition" Geriatrics 8, no. 6: 117. https://doi.org/10.3390/geriatrics8060117
APA StyleGarcía de la Blanca, J. C., Cuarental García, J., Luengo, G., Martí, R., & Ramos, L. R. (2023). Neglected Dislocation in Adults: A New Therapeutic Strategy for an Uncommon Condition. Geriatrics, 8(6), 117. https://doi.org/10.3390/geriatrics8060117