

Efficiency of Printed Patient Information Leaflets Written for Total Knee and Hip Arthroplasty Patients to Reduce Their Fear of Surgery
 ,
,
Abstract
:1. Introduction
2. Methodology
- -
- The study included patients who had been booked for total knee arthroplasty and total hip arthroplasty surgery, and they had to agree to review our educational material and complete questionnaires about the evaluation of the educational booklet and the SFQ questionnaire, which assesses fear of the surgical process.
- -
- Patients who chose not to complete questionnaires.
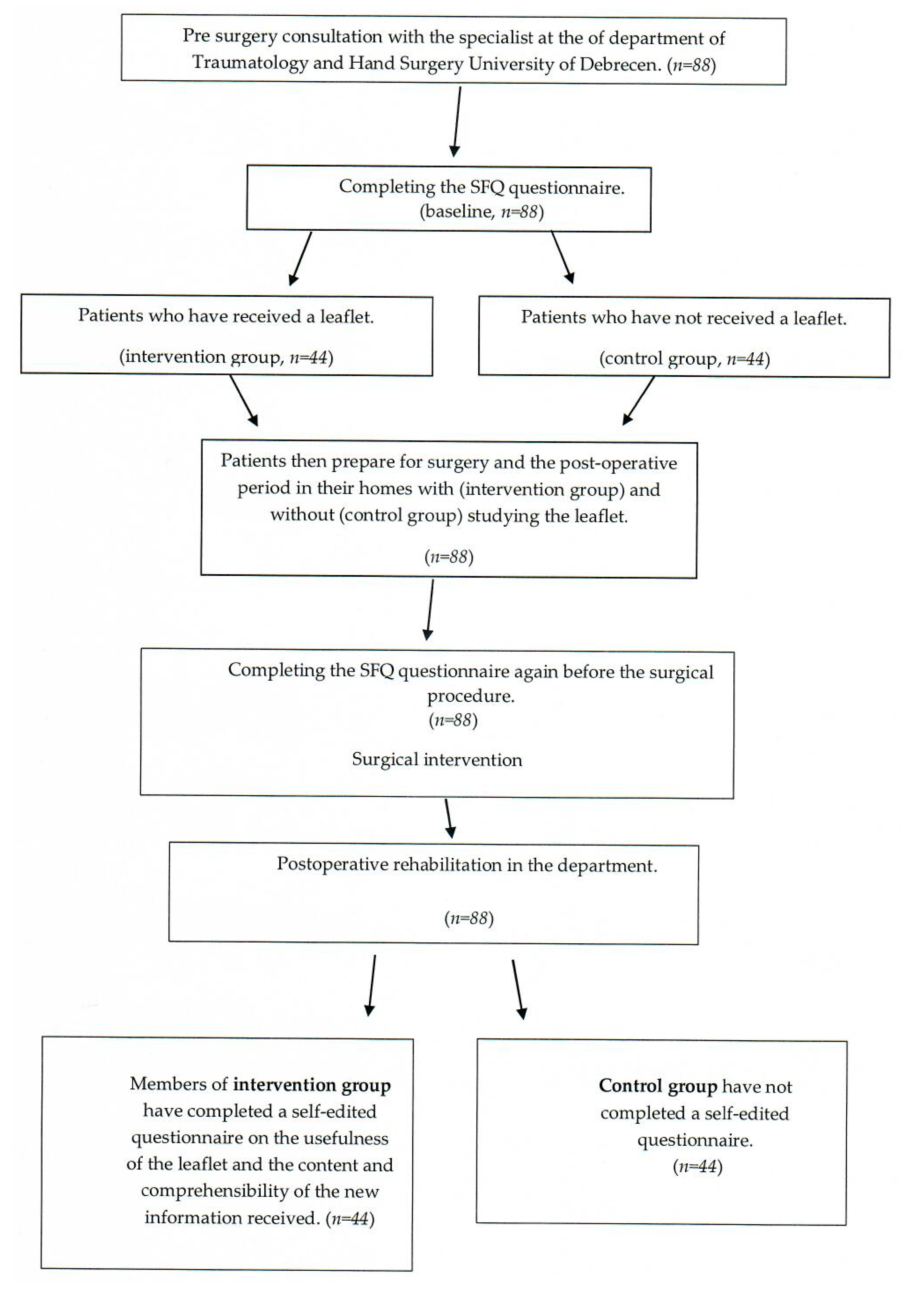
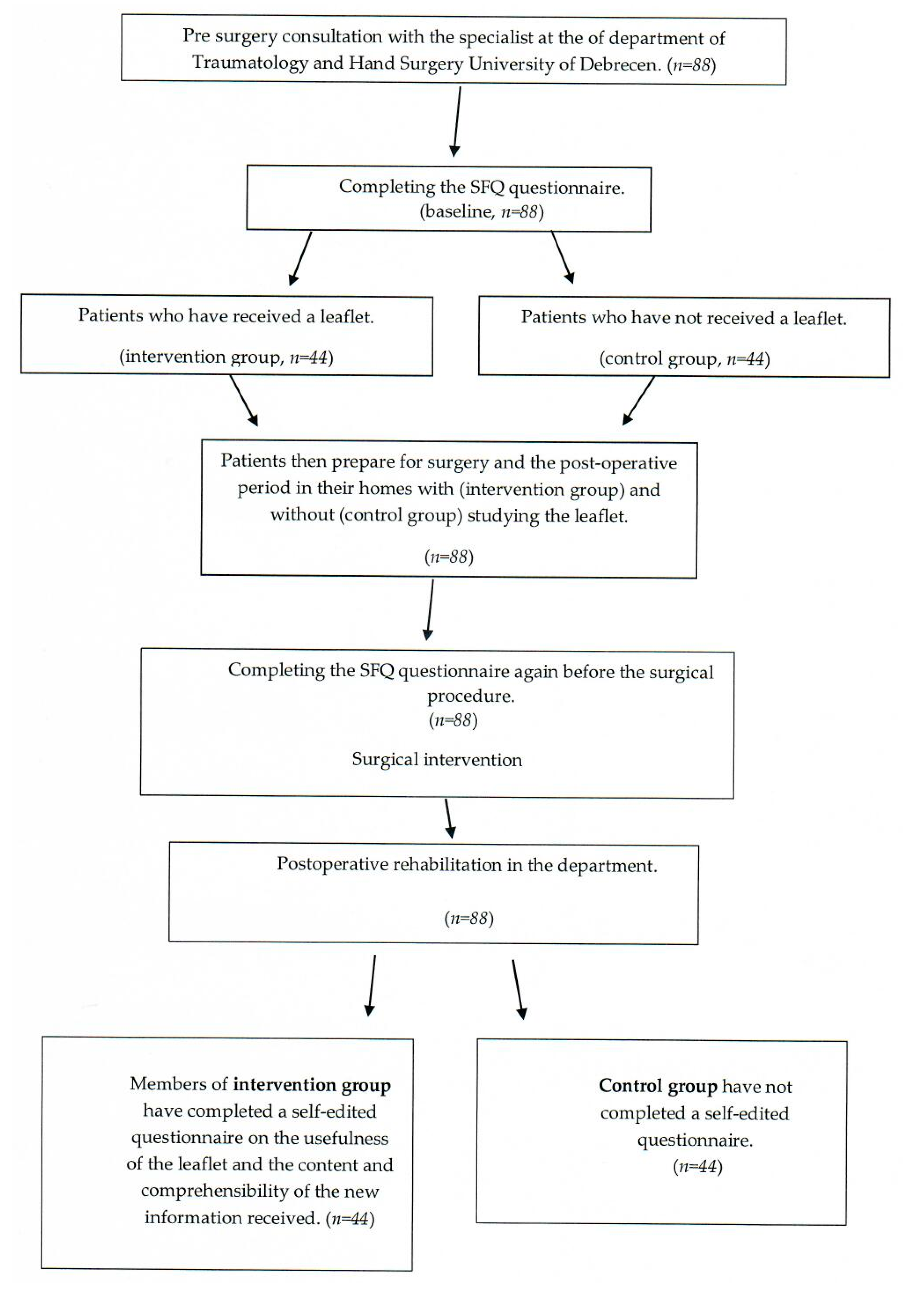
2.1. Study Process
2.2. Patient Information Guide
- The first part described knee and hip prosthesis types, the expected lifetime of replacements, and the factors that affect their lifetime.
- The second part focused on the importance of preoperative programmes. In order to avoid pain, patients load their healthy side more, resulting in a changed posture. Patients do not use the appropriate muscles while walking, which results in a decrease in muscle strength and muscle tone on the painful side, which in turn makes postoperative rehabilitation longer and more difficult. In this part, we also informed patients that preoperative exercises under the supervision of a physiotherapist could help strengthen or, if necessary, relax the affected muscles around the joint to be replaced, which may shorten the rehabilitation period after surgery. They can also learn exercises that we deem important to start immediately after the surgery. Patients were also informed about the walking aids that they would have to use after surgery if they decided to participate in our program. The patient education material also included information on where our preoperative programme would be available for patients waiting for hip and knee arthroplasty surgeries.
- In the third part, our patients received useful advice on lifestyle, such as how to get out of bed after surgery and how to use a high bed and chair after surgery. The information also highlighted the use of a burlap or elastic bandage. The leaflet also described the near and far aids to use after surgery. It also explained how to transport patients to their homes immediately after surgery or after postoperative rehabilitation. They also described options for patients to continue regular exercise and sports activities (swimming, cycling, or driving) after the postoperative rehabilitation period.
- Intensive stretching of the hip, leaning forward (if it is necessary to bend down, slide your operated leg backwards extended, and bend your healthy leg);
- Crossing legs in any posture;
- Supination and pronation of the operated leg with straight legs;
- Twisting the torso while standing with straight legs (the leg must be moved in the direction of the rotation in sync with the body).
- 4.
- The fourth part offered a general description of postoperative rehabilitation, which is further divided into two stages: early and late rehabilitation. The former begins on the day of the operation at the Department of Traumatology. Based on the recommendations of the surgeon in terms of load, a physiotherapist teaches patients how to do tailored exercises and how to use their mobility aids. In the late rehabilitation stage, when a patient has left the department where the operation was performed, rehabilitation may be continued either at the Department of Rehabilitation or at the patient’s home in the form of home patient care, based on the recommendation of the specialist who performed the surgery. The first phase of late rehabilitation can be carried out more efficiently in a hospital setting because of the availability of equipment that supports the restoration of joint functionality and facilitates a quicker recovery.
2.3. Data Collection
2.3.1. Questionnaires Used for Data Collection
Surgical Fear Questionnaire (SFQ)
Self-Designed Questionnaire to Measure the Effectiveness and Usability of the Patient Information Leaflet
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Demographic Data
3.2. Surgical Fear Questionnaire (SFQ)
3.3. Evaluation of the Patient Information Leaflet in Terms of Clarity, New Information Content, and Usefulness
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hibbard, J.H. Patient activation and the use of information to support informed health decisions. Patient Educ. Couns. 2017, 100, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.; Wainwright, A.; Pereira, L.; Robarts, S.; Dickson, P.; Christian, J.; Webster, F. A qualitative study of patient education needs for hip and knee replacement. BMC Musculoskelet. Disord. 2017, 18, 413. [Google Scholar] [CrossRef] [PubMed]
- O’ Reilly, M.; Mohamed, K.; Foy, D.; Sheehan, E. Educational impact of joint replacement school for patients undergoing total hip and knee arthroplasty: A prospective cohort study. Int. Orthop. 2018, 42, 2745–2754. [Google Scholar] [CrossRef] [PubMed]
- Sinatti, P.; Sánchez Romero, E.A.; Martínez-Pozas, O.; Villafañe, J.H. Effects of Patient Education on Pain and Function and Its Impact on Conservative Treatment in Elderly Patients with Pain Related to Hip and Knee Osteoarthritis: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6194. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F.; Moldovan, L.; Bataga, T. A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania. Healthcare 2023, 11, 1866. [Google Scholar] [CrossRef]
- Pabinger, C.; Geissler, A. Utilization rates of hip arthroplasty in OECD countries. Osteoarthr. Cartil. 2014, 22, 734–741. [Google Scholar] [CrossRef]
- Pabinger, C.; Lothaller, H.; Geissler, A. Utilization rates of knee-arthroplasty in OECD countries. Osteoarthr. Cartil. 2015, 23, 1664–1673. [Google Scholar] [CrossRef]
- Shnaekel, A.; Hadden, K.B.; Moore, T.D.; Prince, L.Y.; Barnes, C.L. Readability of Patient Educational Materials for Total Hip and Knee Arthroplasty. J. Surg. Orthop. Adv. 2018, 27, 72–76. [Google Scholar]
- Doering, S.; Katzlberger, F.; Rumpold, G.; Roessler, S.; Hofstoetter, B.; Schatz, D.S. Videotape Preparation of Patients Before Hip Replacement Surgery Reduces Stress. Psychosom. Med. 2000, 62, 365–373. [Google Scholar] [CrossRef]
- Dekkers, T.; Melles, M.; Groeneveld, B.S.; de Ridder, H. Web-Based Patient Education in Orthopedics: Systematic Review. J. Med. Internet Res. 2018, 20, e143. [Google Scholar] [CrossRef]
- Wittmann, V.; Csabai, M.; Drótos, G.; Lázár, G. Reliability and validity testing of the Hungarian version of the Fear of Surgery Questionnaire among patients who have undergone surgery. Hung. Med. J. 2018, 159, 1988–1993. [Google Scholar]
- Act LXXXI of 1997 on Social Security Pension [Internet]. 1 December 2021. Available online: https://njt.hu/jogszabaly/1997-81-00-00 (accessed on 31 October 2022).
- Veres, D. Hundreds of Thousands of Hungarian Pensioners Forced to Work They have Devastating Opportunities. Available online: https://www.portfolio.hu/gazdasag/20191028/tobb-szazezer-magyar-nyugdijas-kenytelen-dolgozni-lesujto-lehetosegeik-vannak-404899# (accessed on 31 October 2022).
- Weiss, B.D.; Blanchard, J.S.; McGee, D.L.; Hart, G.; Warren, B.; Burgoon, M.; Smith, K.J. Illiteracy among Medicaid Recipients and its Relationship to Health Care Costs. J. Health Care Poor Underserved 1994, 5, 99–111. [Google Scholar] [CrossRef]
- Majid, N.; Lee, S.; Plummer, V. The effectiveness of orthopedic patient education in improving patient outcomes: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 122–133. [Google Scholar] [CrossRef]
- Yi, M.M.; Yi, P.H.; Hussein, K.I.; Cross, M.B.; Della Valle, C.J. Readability of Patient Education Materials From the Web Sites of Orthopedic Implant Manufacturers. J. Arthroplast. 2017, 32, 3568–3572. [Google Scholar] [CrossRef]
- Rackwitz, L.; Reyle-Hahn, S.-M.; Nöth, U. Präoperatives Management und Patientenschulung in der Fast-Track-Endoprothetik. Orthopäde 2020, 49, 299–305. [Google Scholar] [CrossRef]
- Rohringer, M.; Kellerer, J.D.; Fink, C.; Schulc, E. The role of health literacy in orthopaedic rehabilitation after total knee and hip arthroplasty: A scoping review. Int. J. Orthop. Trauma Nurs. 2021, 40, 100793. [Google Scholar] [CrossRef]
- Bitzer, E.M.; Spörhase, U. Gesundheitskompetenz in der medizinischen Rehabilitation und die Bedeutung für die Patientenschulung. Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 983–988. [Google Scholar] [CrossRef]
- Clarius, M.; Rackwitz, L.; Nöth, U.; Clarius, J.; Clarius, L.M. Prästationäres Management in der Fast-Track-Endoprothetik. Orthopäde 2022, 51, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Badarudeen, S.; Sabharwal, S. Assessing Readability of Patient Education Materials: Current Role in Orthopaedics. Clin. Orthop. Relat. Res. 2010, 468, 2572–2580. [Google Scholar] [CrossRef] [PubMed]
- Stenquist, D.S.; Ready, L.V.; Ghazinouri, R.; Beagan, C.; Wisdom, A.; Katz, J.N. Development of Patient Education Materials for Total Joint Replacement During an International Surgical Brigade. JAAOS Glob. Res. Rev. 2020, 4, e20.00074. [Google Scholar] [CrossRef] [PubMed]
- Koivisto, J.-M.; Saarinen, I.; Kaipia, A.; Puukka, P.; Kivinen, K.; Laine, K.-M.; Haavisto, E. Patient education in relation to informational needs and postoperative complications in surgical patients. Int. J. Qual. Health Care 2020, 32, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Doinn, T.Ó.; Broderick, J.M.; Abdelhalim, M.M.; Quinlan, J.F. Readability of Patient Educational Materials in Hip and Knee Arthroplasty: Has a Decade Made a Difference? J. Arthroplast. 2020, 35, 3076–3083. [Google Scholar] [CrossRef] [PubMed]
- Oroszi, J. Professional Protocol of the Ministry of Health on Nurse-Infection Control, National Spine Centre. Available online: https://gerinces.hu/kezeles/konzervativ-kezeles/betegoktatasrol/ (accessed on 4 November 2022).

{kind=link}
| Baseline | Control Group | Intervention Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgery | Group | Median | IQR | p-value (age under 70 vs. 70 and over) | Median | IQR | p-value (age under 70 vs. 70 and over) | p-value (baseline vs. intervention group) | Median | IQR | p-value (age under 70 vs. 70 and over) | p-value (baseline vs. intervention group) |
| Total knee arthroplasty | under 70 | 38.00 | 30.00–40.00 | 0.835 | 54.00 | 20.00–69.00 | 0.097 | 0.379 | 22.50 | 19.00–28.00 | 0.298 | 0.058 |
| 70 and over | 36.50 | 31.50–39.50 | 75.00 | 63.00–84.00 | 0.002 | 17.50 | 15.50–23.50 | 0.001 | ||||
| total | 37.50 | 30.00–40.00 | 64.50 | 54.00–82.00 | 0.005 | 20.00 | 16.00–24.00 | <0.001 | ||||
| Total hip arthroplasty | under 70 | 35.00 | 28.00–42.00 | 0.992 | 56.00 | 31.00–71.00 | 0.008 | 0.016 | 20.00 | 16.00–22.00 | 0.719 | <0.001 |
| 70 and over | 33.50 | 27.50–43.00 | 77.00 | 73.00–86.00 | <0.001 | 20.00 | 15.50–23.50 | <0.001 | ||||
| total | 34.50 | 28.00–42.00 | 73.00 | 56.00–81.00 | <0.001 | 20.00 | 16.00–22.00 | <0.001 | ||||
| Total Hip Arthroplasty | Total Knee Arthroplasty | |||
|---|---|---|---|---|
| coeff [95% CI] | p | coeff [95% CI] | p | |
| Age (years) | −0.05 [−0.34–0.23] | 0.711 | 1.23 [0.02–2.44] | 0.046 |
| Gender (female/male) | 4.71 [−1.4–10.81] | 0.128 | 17.34 [2.19–32.48] | 0.027 |
| Group (control/intervention) | 55.15 [50.14–60.16] | <0.001 | 49.5 [34.92–64.08] | <0.001 |
| Comprehensibility | New Information | Usefulness | |||||
|---|---|---|---|---|---|---|---|
| Surgery | Group | Median | IQR | Median | IQR | Median | IQR |
| Total knee arthroplasty | total | 12.00 | 12.00–12.00 | 12.00 | 11.25–12.00 | 12.00 | 12.00–12.00 |
| below 70 | 12.00 | 12.00–12.00 | 12.00 | 10.50–12.00 | 12.00 | 11.25–12.00 | |
| over 70 | 12.00 | 12.00–12.00 | 12.00 | 11.00–12.00 | 12.00 | 12.00–12.00 | |
| Total hip arthroplasty | total | 12.00 | 11.25–12.00 | 11.50 | 10.00–12.00 | 12.00 | 11.00–12.00 |
| below 70 | 12.00 | 12.00–12.00 | 12.00 | 11.00–12.00 | 12.00 | 11.00–12.00 | |
| over 70 | 12.00 | 11.00–12.00 | 10.00 | 9.75–12.00 | 11.00 | 10.25–12.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szilágyiné Lakatos, T.; Lukács, B.; Nagy, A.C.; Jenei, Z.; Veres-Balajti, I. Efficiency of Printed Patient Information Leaflets Written for Total Knee and Hip Arthroplasty Patients to Reduce Their Fear of Surgery. Geriatrics 2023, 8, 89. https://doi.org/10.3390/geriatrics8050089
Szilágyiné Lakatos T, Lukács B, Nagy AC, Jenei Z, Veres-Balajti I. Efficiency of Printed Patient Information Leaflets Written for Total Knee and Hip Arthroplasty Patients to Reduce Their Fear of Surgery. Geriatrics. 2023; 8(5):89. https://doi.org/10.3390/geriatrics8050089
Chicago/Turabian StyleSzilágyiné Lakatos, Tünde, Balázs Lukács, Attila Csaba Nagy, Zoltán Jenei, and Ilona Veres-Balajti. 2023. "Efficiency of Printed Patient Information Leaflets Written for Total Knee and Hip Arthroplasty Patients to Reduce Their Fear of Surgery" Geriatrics 8, no. 5: 89. https://doi.org/10.3390/geriatrics8050089
APA StyleSzilágyiné Lakatos, T., Lukács, B., Nagy, A. C., Jenei, Z., & Veres-Balajti, I. (2023). Efficiency of Printed Patient Information Leaflets Written for Total Knee and Hip Arthroplasty Patients to Reduce Their Fear of Surgery. Geriatrics, 8(5), 89. https://doi.org/10.3390/geriatrics8050089