

Quantitative Assessment of Balance Function Characteristics in Older Patients with Orthostatic Hypotension

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Data Collection
2.3. Laboratory Tests
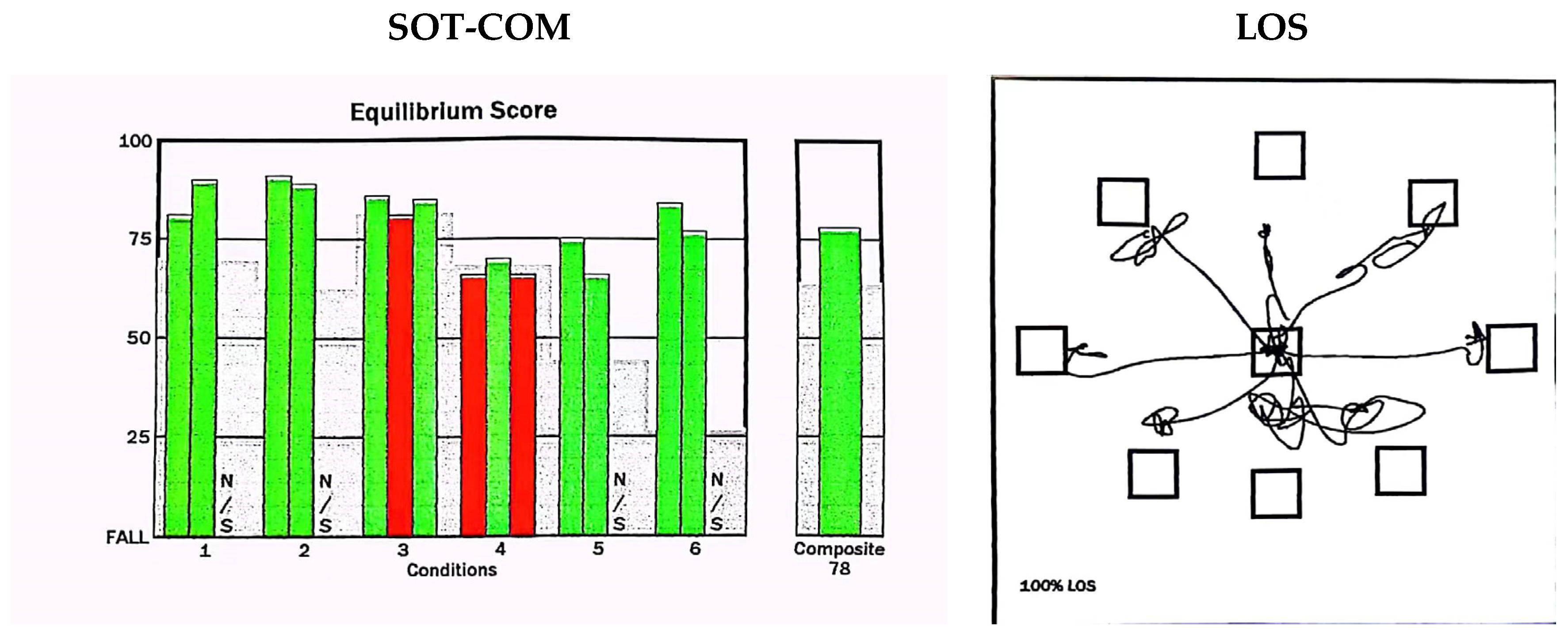
2.4. Computer Dynamic Posturography (CDP)
2.4.1. Sensory Organization Test (SOT)
- Fixed surface, fixed visual surroundings, eyes open.
- Fixed surface, eyes closed.
- Fixed surface, moving visual surroundings, eyes open.
- Moving surface, fixed visual surroundings, eyes open.
- Moving surface, eyes closed.
- Moving surface, moving visual surroundings, eyes open.
2.4.2. Limits-of-Stability Test (LOS)
3. Statistical Analyses
4. Results
- Table 1 shows the characteristics of the study participants. Of 303 older adults, 91 were in the OH group and 212 were in the non-OH group. No significant differences in age, sex, or BMI (p > 0.05) were observed between the groups, and thus, the two groups were essentially matched. Participants with OH had more chronic diseases, including coronary heart disease (p = 0.049) and a history of falls (p < 0.001), than those without OH. A history of multiple medications in the OH group was significantly higher than that in the non-OH group (p = 0.006).
- Table 2 shows that there were no statistically significant differences between the two groups in terms of laboratory indicators.
- As shown in Table 3, there was a significant decrease in SOT-COM (p < 0.001), VIS (p < 0.001), VEST (p < 0.001), and DCL (p = 0.028) in the OH group, compared to the non-OH group, but there were no significant differences in SOM, RT, or MXE between the two groups (p > 0.05).
- A regression analysis was conducted in this study, using various balance indicators as independent variables to analyze the incidence of OH as a binary variable. After adjusting for age, gender, and body mass index, only SOT-COM was found to have a negative correlation with the incidence of OH (OR = 0.904; 95% CI: 0.882–0.927; p < 0.001). Further adjustments for factors such as history of falls, coronary heart disease, history of multiple medications, and laboratory tests revealed that only SOT-COM was negatively correlated with the incidence of OH (OR = 0.884; 95% CI: 0.832–0.940; p < 0.001).
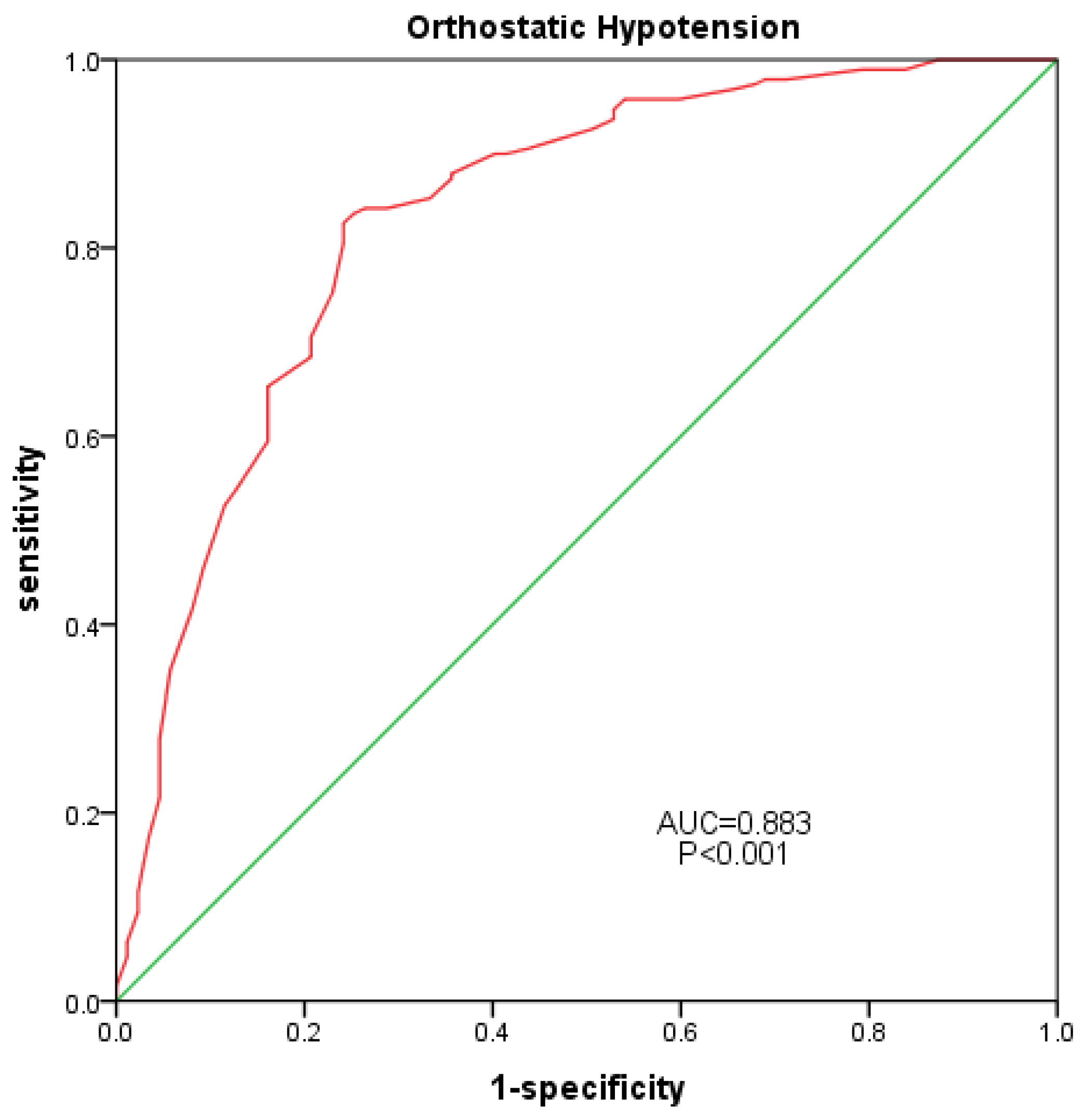
- An ROC curve was plotted for all participants, using the occurrence of OH as the positive rate, and the area under the curve was calculated (Figure 2). The AUC of SOT was 0.833 (95% confidence interval: 0.778–0.887; p < 0.001), with a sensitivity of 0.826 and a specificity of 0.759.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wieling, W.; Kaufmann, H.; Claydon, V.E.; van Wijnen, V.K.; Harms, M.P.; Juraschek, S.P.; Thijs, R.D. Diagnosis and treatment of orthostatic hypotension. Lancet Neurol. 2022, 21, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Claffey, P.; Pérez-Denia, L.; Lavan, A.; Kenny, R.A.; Finucane, C.; Briggs, R. Asymptomatic orthostatic hypotension and risk of falls in community-dwelling older people. Age Ageing 2022, 51, afac295. [Google Scholar] [CrossRef] [PubMed]
- Mol, A.; Reijnierse, E.M.; Bui Hoang, P.T.S. Orthostatic hypotension and physical functioning in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2018, 48, 122–144. [Google Scholar] [CrossRef]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton. Neurosci. Basic 2011, 161, 46–48. [Google Scholar] [CrossRef]
- Shen, S.; He, T.; Chu, J.; He, J.; Chen, X. Uncontrolled hypertension and orthostatic hypotension in relation to standing balance in older hypertensive patients. Clin. Interv. Aging 2015, 10, 897–906. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35 (Suppl. S2), ii7–ii11. [Google Scholar] [CrossRef]
- Ooi, W.L.; Hossain, M.; Lipsitz, L.A. The association between orthostatic hypotension and recurrent falls in nursing home residents. Am. J. Med. 2000, 108, 106–111. [Google Scholar] [CrossRef]
- de Bruïne, E.S.; Reijnierse, E.M.; Trappenburg, M.C.; Pasma, J.H. Diminished Dynamic Physical Performance is Associated with orthostatic hypotension in Geriatric Outpatients. J. Geriatr. Phys. Ther. 2019, 42, E28–E34. [Google Scholar] [CrossRef]
- McDonald, C.; Pearce, M.; Kerr, S.R.; Black, D. A prospective study of the association between orthostatic hypotension and falls: Definition matters. Age Ageing 2017, 46, 439–445. [Google Scholar] [CrossRef]
- Shepard, N.T. The clinical use of dynamic posturography in the older. Ear Nose Throat J. 1989, 68, 940–958. [Google Scholar]
- Fiedorová, I.; Mrázková, E.; Zádrapová, M.; Tomášková, H. Receiver Operating Characteristic Curve Analysis of the Somatosensory Organization Test, Berg Balance Scale, and Fall Efficacy Scale-International for Predicting Falls in Discharged Stroke Patients. Int. J. Environ. Res. Public Health 2022, 19, 9181. [Google Scholar] [CrossRef] [PubMed]
- Rossi-Izquierdo, M.; Gayoso-Diz, P.; Santos-Pérez, S.; Del-Río-Valeiras, M.; Faraldo-García, A.; Vaamonde-Sánchez-Andrade, I.; Lirola-Delgado, A. Vestibular rehabilitation in older patients with postural instability: Reducing the number of falls-a randomized clinical trial. Aging Clin. Exp. Res. 2018, 30, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; De Caterina, R.; Fedorowski, A. Orthostatic hypotension: Epidemiology, Prognosis, and Treatment. J. Am. Coll. Cardiol. 2015, 66, 848–860. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A.; Ricci, F.; Hamrefors, V.; Sandau, K.E.; Hwan Chung, T.; Muldowney, J.A.; Gopinathannair, R. Orthostatic hypotension: Management of a Complex, but Common, Medical Problem. Circ. Arrhythmia Electrophysiol. 2022, 15, e010573. [Google Scholar] [CrossRef]
- Press, Y.; Punchik, B.; Freud, T. Orthostatic hypotension and drug therapy in patients at an outpatient comprehensive geriatric assessment unit. J. Hypertens. 2016, 34, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.; Blanke, O. The thalamocortical vestibular system in animals and humans. Brain Res. Rev. 2011, 67, 119–146. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.F.; Darlington, C.L.; Zheng, Y. Move it or lose it--is stimulation of the vestibular system necessary for normal spatial memory? Hippocampus 2010, 20, 36–43. [Google Scholar] [CrossRef]
- Onofrei, R.R.; Amaricai, E. Postural Balance in Relation with Vision and Physical Activity in Healthy Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 5021. [Google Scholar] [CrossRef]
- Hunter, S.W.; Divine, A.; Madou, E.; Omana, H.; Hill, K.D.; Johnson, A.M.; Holmes, J.D.; Wittich, W. Executive function as a mediating factor between visual acuity and postural stability in cognitively healthy adults and adults with Alzheimer’s dementia. Arch. Gerontol. Geriatr. 2020, 89, 104078. [Google Scholar] [CrossRef]
- Hansson, E.E.; Beckman, A.; Håkansson, A. Effect of vision, proprioception, and the position of the vestibular organ on postural sway. Acta Oto-Laryngol. 2010, 130, 1358–1363. [Google Scholar] [CrossRef]
- Wingert, J.R.; Welder, C.; Foo, P. Age-related hip proprioception declines: Effects on postural sway and dynamic balance. Arch. Phys. Med. Rehabil. 2014, 95, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Ogliari, G.; Ryg, J.; Qureshi, N.; Andersen-Ranberg, K.; Scheel-Hincke, L.L.; Masud, T. Subjective vision and hearing impairment and falls among community-dwelling adults: A prospective study in the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur. Geriatr. Med. 2021, 12, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, Y.; Carey, J.P.; Della Santina, C.C.; Schubert, M.C.; Minor, L.B. Disorders of balance and vestibular function in US adults: Data from the National Health and Nutrition Examination Survey, 2001–2004. Arch. Int. Med. 2009, 169, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Donovan, J.; De Silva, L.; Cox, H.; Palmer, G.; Semciw, A.I. Vestibular dysfunction in people who fall: A systematic review and meta-analysis of prevalence and associated factors. Clin. Rehabil. 2023, 37, 2692155231162423. [Google Scholar] [CrossRef] [PubMed]
- Batuecas-Caletrio, A.; Trinidad-Ruiz, G.; Zschaeck, C.; del Pozo de Dios, J.C.; de Toro Gil, L.; Martin-Sanchez, V.; Martin-Sanz, E. Benign paroxysmal positional vertigo in the older. Gerontology 2013, 59, 408–412. [Google Scholar] [CrossRef]
- Villarroel, M.; Ciudin, A.; Hernández, C.; Simó, R. Neurodegeneration: An early event of diabetic retinopath. World J. Diabetes 2010, 1, 57–64. [Google Scholar] [CrossRef]
- Takahashi, M.; Miyai, N.; Nagano, S.; Utsumi, M.; Oka, M.; Yamamoto, M. Orthostatic blood pressure changes and subclinical markers of atherosclerosis. Am. J. Hypertens. 2015, 28, 1134–1140. [Google Scholar] [CrossRef]
- Nakamura, T.; Suzuki, M.; Ueda, M.; Hirayama, M. Lower body mass index is associated with orthostatic hypotension in Parkinson’s disease. J. Neurol. Sci. 2017, 372, 14–18. [Google Scholar] [CrossRef]
- Veronese, N.; Trevisan, C.; Bolzetta, F.; Zambon, S. Hypovitaminosis D predicts the onset of orthostatic hypotension in older adults. J. Am. Soc. Hypertens. 2016, 10, 724–732. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| OH Group (91 Cases) | Non-OH Group (212 Cases) | |X2/T/Z| | p | |
|---|---|---|---|---|
| Age (years) | 80.10 ± 8.12 | 79.04 ± 8.74 | 0.989 | 0.323 |
| Sex (male, %) | 67.03 | 73.58 | 1.345 | 0.246 |
| BMI | 24.02 ± 3.30 | 23.86 ± 2.87 | 0.439 | 0.661 |
| Hypertension (Yes, %) | 74.73 | 68.57 | 1.155 | 0.283 |
| Coronary heart disease (Yes, %) | 52.75 | 40.48 | 3.876 | 0.049 * |
| Diabetes (Yes, %) | 47.25 | 38.10 | 2.203 | 0.138 |
| Cerebrovascular disease (Yes, %) | 23.08 | 18.57 | 0.808 | 0.369 |
| Chronic kidney disease (Yes, %) | 8.79 | 8.57 | 0.004 | 0.950 |
| History of falls (Yes, %) | 73.63 | 32.10 | 44.498 | <0.001 * |
| Multiple medication history (≥5, %) | 63.74 | 46.67 | 7.409 | 0.006 * |
| OH Group (91 Cases) | Non-OH Group (212 Cases) | |X2/T/Z| | p | |
|---|---|---|---|---|
| Hgb (g/L) | 132.15 ± 16.54 | 135.13 ± 13.32 | 1.430 | 0.154 |
| ALB (g/L) | 41.40 ± 6.61 | 40.56 ± 3.87 | 1.075 | 0.285 |
| SCr (µmol/L) | 93.83 ± 58.90 | 86.20 ± 32.02 | 1.113 | 0.268 |
| BUN (mmol/L) | 6.47 ± 2.35 | 6.13 ± 1.89 | 1.232 | 0.219 |
| UA (µmol/L) | 356.17 ± 98.83 | 349.41 ± 85.08 | 0.570 | 0.569 |
| TG (mmol/L) | 1.35 ± 0.98 | 1.36 ± 0.75 | 0.073 | 0.942 |
| TC (mmol/L) | 4.06 ± 0.93 | 4.26 ± 0.94 | 1.643 | 0.102 |
| HDL-C (mmol/L) | 1.29 ± 0.43 | 1.39 ± 0.44 | 1.684 | 0.093 |
| LDL-C (mmol/L) | 2.22 ± 0.81 | 2.33 ± 0.80 | 1.039 | 0.300 |
| AI | 2.41 ± 1.19 | 2.30 ± 1.03 | 0.800 | 0.425 |
| HbA1C (%) | 7.20 ± 1.59 | 6.90 ± 1.97 | 0.985 | 0.326 |
| 25(OH)D3 (ng/mL) | 24.49 ± 12.43 | 25.58 ± 12.30 | 0.589 | 0.556 |
| eGFR (mL/min/1.73 m2) | 71.99 ± 20.20 | 73.18 ± 17.34 | 0.488 | 0.626 |
| OH Group (91 Cases) | Non-OH Group (212 Cases) | |X2/T/Z| | p | |
|---|---|---|---|---|
| SOM (M (Q1, Q3)) | 98 (95, 100) | 98 (95, 100) | 1.205 | 0.228 |
| VIS (M (Q1, Q3)) | 70 (52, 80) | 80 (70, 85) | 6.088 | <0.001 * |
| VEST (M (Q1, Q3)) | 15 (5, 60) | 65 (60, 80) | 8.173 | <0.001 * |
| SOT-COM (M (Q1, Q3)) | 53 (42, 66) | 76 (69, 80) | 8.898 | <0.001 * |
| RT (s) | 0.95 ± 0.22 | 0.90 ± 0.26 | 1.357 | 0.176 |
| MXE (%) | 66.60 ± 13.01 | 68.80 ± 11.45 | 1.386 | 0.167 |
| DCL (%) | 67.35 ± 9.41 | 70.26 ± 9.82 | 2.210 | 0.028 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Liu, B.; Zhou, J.; Liu, Q.; Ye, H. Quantitative Assessment of Balance Function Characteristics in Older Patients with Orthostatic Hypotension. Geriatrics 2023, 8, 103. https://doi.org/10.3390/geriatrics8050103
Cui Y, Liu B, Zhou J, Liu Q, Ye H. Quantitative Assessment of Balance Function Characteristics in Older Patients with Orthostatic Hypotension. Geriatrics. 2023; 8(5):103. https://doi.org/10.3390/geriatrics8050103
Chicago/Turabian StyleCui, Yao, Bo Liu, Jian Zhou, Qian Liu, and Hui Ye. 2023. "Quantitative Assessment of Balance Function Characteristics in Older Patients with Orthostatic Hypotension" Geriatrics 8, no. 5: 103. https://doi.org/10.3390/geriatrics8050103
APA StyleCui, Y., Liu, B., Zhou, J., Liu, Q., & Ye, H. (2023). Quantitative Assessment of Balance Function Characteristics in Older Patients with Orthostatic Hypotension. Geriatrics, 8(5), 103. https://doi.org/10.3390/geriatrics8050103