


Efficacy of Health Promotion Interventions Aimed to Improve Health Gains in Middle-Aged Adults—A Systematic Review

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
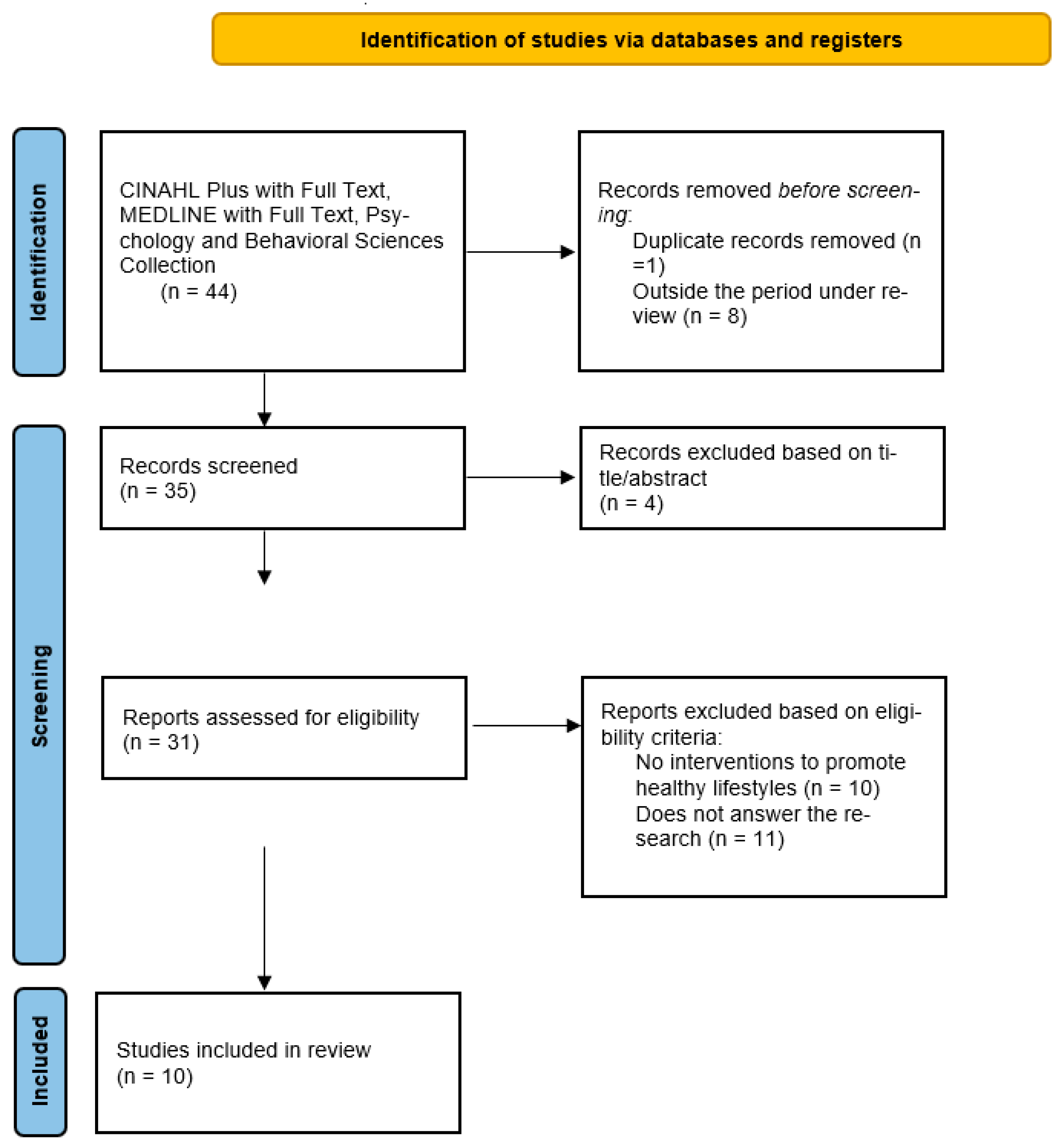
2.1. Research Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Quality Assurance
2.5. Strategy for Data Synthesis
3. Results
4. Discussion
4.1. Interventions That Promote Healthy Lifestyles in Middle-Aged Adults
4.2. Interventions That Translate into Health Gains
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Language selection|European Commission. Archive:Estrutura Populacional E Envelhecimento-Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Archive:Estrutura_populacional_e_envelhecimento&direction=next&oldid=469734 (accessed on 4 February 2023).
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 9 April 2023).
- Loureiro, H. Cuidar na “entrada na reforma”: Uma Intervenção Conducente À Promoção da Saúde de Indivíduos E de Famílias; Tese de Doutoramento, Universidade de Aveiro: Aveiro, Portugal, 2011. [Google Scholar]
- Lopes, M.; Fonseca, C.; Guedes Pinho, L.; Margarida Goes, M.; Maria Rodrigues, A. Cuidados à Pessoa com Multimorbilidade e Dependência: A Mudança de Paradigma Necessária. In Desafios do Envelhecimento Para a Saúde, a Economia e A Sociedade; Princípia: Cascais, Portugal, 2022; pp. 14–39. [Google Scholar]
- Virtual Health Library. DeCS/MeSH Health Sciences Descriptors. Available online: https://decs.bvsalud.org/en/ths/resource/?id=9062&filter=ths_termall&q=middle%20aged (accessed on 9 April 2023).
- Solhi, M.; Pirouzeh, R.; Zanjari, N. Middle-aged preparation for healthy aging: A qualitative study. BMC Public Health 2022, 22, 274. [Google Scholar] [CrossRef] [PubMed]
- Cabral, M.; Ferreira, P.; Silva, P. Processos de Envelhecimento em Portugal. Homepage|Fundação Francisco Manuel dos Santos. 2013. Available online: https://www.ffms.pt/FileDownload/b45aa8e7-d89b-4625-ba91-6a6f73f4ecb3/processos-de-envelhecimento-em-portugal (accessed on 4 February 2023).
- World Health Organization (WHO). WHO’s Work on the UN Decade of Healthy Ageing (2021–2030). Available online: https://www.who.int/initiatives/decade-of-healthy-ageing (accessed on 4 February 2023).
- IRIS PAHO Home. 2019. Available online: https://iris.paho.org/bitstream/handle/10665.2/52902/OPASWBRAFPL20120_por.pdf?sequence=1&isAllowed=y (accessed on 4 February 2023).
- WHO. The Decade of Healthy Ageing (2020–2030). 2020. Available online: https://cdn.who.int/media/docs/default-source/decade-of-healthy-ageing/final-decade-proposal/decade-proposal-final-apr2020-en.pdf?sfvrsn=b4b75ebc_25&download=true (accessed on 5 February 2023).
- Canhestro, A. Envelhecer Com Saúde: Promoção de Estilos de Vida Saudáveis no Baixo Alentejo. Repositório da Universidade de Lisboa: Página principal. 2018. Available online: https://repositorio.ul.pt/handle/10451/34565 (accessed on 4 February 2023).
- WHO/Europe | Home. Strategy and Action Plan for Healthy Ageing in Europe, 2012–2020. 2012. Available online: https://www.euro.who.int/__data/assets/pdf_file/0008/175544/RC62wd10Rev1-Eng.pdf (accessed on 4 February 2023).
- Bosch-Farré, C.; Garre-Olmo, J.; Bonmatí-Tomàs, A.; Malagón-Aguilera, M.C.; Gelabert-Vilella, S.; Fuentes-Pumarola, C.; Juvinyà-Canal, D. Prevalence and related factors of Active and Healthy Ageing in Europe according to two models: Results from the Survey of Health, Ageing and Retirement in Europe (SHARE). PloS ONE 2018, 13, e0206353. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2019, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Home Page|JBI. 2020. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Case_Series2017_0.pdf (accessed on 10 February 2023).
- World Health Organization. World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1&isAllowed=y (accessed on 10 February 2023).
- van Keulen, H.M.; van Breukelen, G.; de Vries, H.; Brug, J.; Mesters, I. A randomized controlled trial comparing community lifestyle interventions to improve adherence to diet and physical activity recommendations: The VitalUM study. Eur. J. Epidemiol. 2020, 36, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.; Chiang, S.; Liu, H.; Chiang, L. Effects of Individualized Aerobic Exercise Training on Physical Activity and Health-Related Physical Fitness among Middle-Aged and Older Adults with Multimorbidity: A Randomized Controlled Trial. MDPI. 2020. Available online: https://www.mdpi.com/1660-4601/18/1/101 (accessed on 10 February 2023).
- Latina, J.; Fernandez-Jimenez, R.; Bansilal, S.; Sartori, S.; Vedanthan, R.; Lewis, M.; Kofler, C.; Hunn, M.; Martin, F.; Bagiella, E.; et al. Grenada Heart Project–Community Health ActioN to EncouraGe healthy BEhaviors (GHP-CHANGE): A randomized control peer group–based lifestyle intervention. Am. Heart J. 2020, 220, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Blom, E.E.; Aadland, E.; Skrove, G.K.; Solbraa, A.K.; Oldervoll, L.M. Health-related quality of life and physical activity level after a behavior change program at Norwegian healthy life centers: A 15-month follow-up. Qual. Life Res. 2020, 29, 3031–3041. [Google Scholar] [CrossRef] [PubMed]
- Webel, A.R.; Moore, S.M.; Longenecker, C.T.; Currie, J.; Horvat Davey, C.; Perazzo, J.; Sattar, A.; Josephson, R. A randomizes controlled trial of the systemCHANGE intervention on behaviors related to cardiovascular risk in HIV + Adults. J. Acquir. Immune Defic. Syndr. 2018, 78, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.-Y. Smart wearable devices as a psychological intervention for healthy lifestyle and quality of life: A randomized controlled trial. Qual. Life Res. 2020, 30, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Ghayomzadeh, M.; Etesami, M.S.; Earnest, C.P.; Rezaei, S.; Navalta, J.W.; Taj, L.; SeyedAlinaghi, S.; Mohraz, M.; Gharakhanlou, R.; Voltarelli, F.A. Effect of a Short-term Lifestyle Modification Program on Quality of Life, Anthropometric Characteristics and CD4+T Cell Count of HIV Infected Patients in Tehran/Iran: A Randomized Controlled Trial. Explore 2019, 15, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K.; Mason, S.T.; Vail, T.A.; Rogers, G.V.; Livingston, K.A.; Whelan, J.G.; Chin, M.K.; Blanchard, C.M.; Turgiss, J.L.; Roberts, S.B. Effectiveness of an Energy Management Training Course on Employee Well-Being: A Randomized Controlled Trial. Am. J. Health Promot. 2018, 33, 118–130. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, C.S.; Nielsen, S.M.; Bjørner, J.; Johansen, M.Y.; Christensen, R.; Vaag, A.; Lieberman, D.E.; Pedersen, B.K.; Langberg, H.; Ried-Larsen, M.; et al. One-year intensive lifestyle intervention and improvements in health-related quality of life and mental health in persons with type 2 diabetes: A secondary analysis of the U-TURN randomized controlled trial. BMJ Open Diabetes Res. Care 2021, 9, e001840. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Cartmel, B.; Gottlieb, L.; Ercolano, E.A.; Li, F.; Harrigan, M.; McCorkle, R.; Ligibel, J.A.; von Gruenigen, V.E.; Gogoi, R.; et al. Randomized Trial of Exercise on Quality of Life in Women With Ovarian Cancer: Women’s Activity and Lifestyle Study in Connecticut (WALC). JNCI J. Natl. Cancer Inst. 2017, 109, djx072. [Google Scholar] [CrossRef] [PubMed]
- Virtual Health Library. DeCS/MeSH Health Sciences Descriptors. Available online: https://decs.bvsalud.org/ths/resource/?id=57934&filter=ths_termall&q=\%22health%20gain\%22 (accessed on 9 April 2023).
- George, E.S.; Masri, E.M.; Kwasnicka, D.; Romeo, A.; Cavallin, S.; Bennie, A.; Kolt, G.; Guagliano, J. Effectiveness of Adult Health Promotion Interventions Delivered Trought Professional Sport: Systematic Review and Meta-Analysis. Sport. Med. 2022, 52, 2637–2655. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Mei, S.; Yang, R.; Chen, L.; Gao, H.; Li, L. Effects of lifestyle intervention using patient-centered cognitive behavioral therapy among patients with cardio-metabolic syndrome: A randomized, controlled trial. BMC Cardiovasc. Disorders 2016, 16, 227. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Interventions to Promote Healthy Lifestyles | Studies | |
|---|---|---|
| Educational | Healthy eating | [18,20,21,22,24,25] |
| Physical exercise | [18,19,20,21,22,24,25,26,27] | |
| Change in habits and lifestyles away from harmful behaviors (smoking, excess carbohydrates, sedentary lifestyle, and stress) | [20,21,22,24] | |
| Motivational | Motivational interviewing | [19,21] |
| Cognitive behavioral therapy | [25] | |
| Acceptance and commitment therapy | [25] | |
| Personalized communication letters | [18] | |
| Use of electronic equipment | Accelerometers | [21,22] |
| Smartwatch/bracelet | [23] | |
| Polar Watch V800 | [24] | |
| Individuals | Performed individually by the person | [18,19,22,23,27] |
| In group | Performed in interactions with other people in a group | [20,21,22,24,25,26] |
| Intervention | Impact of the Intervention | Studies |
|---|---|---|
| Intervention over 12 months consisting of the transmission of information about healthy lifestyles (fruit and vegetable consumption and physical exercise) by sending 4 personalized communication letters (TPC) | Physical and psychological | [18] |
| Intervention implemented across 12 weeks that consisted of a multidisciplinary, individualized aerobic exercise training program, 30 to 50 min per session, combined with motivational telephone interviews, once a week, with duration of 15 to 30 min | Physical and psychological | [19] |
| Health education conducted by peers over 12 months | Physical, psychological, and social | [20] |
| Design of a personalized plan for behavior change | Physical, psychological, and social | [21] |
| Education about healthy lifestyles complemented by telephone calls | Physical and psychological | [22] |
| Intervention implemented over 3 months that consisted of the use of 2 different commercial smart devices (bracelet and watch) | Physical and psychological | [23] |
| Promotion of physical and mental exercise and healthy eating (increased consumption of fruit and vegetables) and adoption of healthier habits (physical, mental, and cognitive), over 8 weeks | Physical, psychological, and social | [24] |
| Implementation of an intensive 2.5-day group program to promote well-being (combining cognitive behavioral theory and acceptance and commitment therapy), followed by periodic follow-up at 6, 12, and 18 months | Physical, psychological, and social | [25] |
| Implementation of an intensive intervention on lifestyle (physical exercise, nutrition, sleep, management of chronic disease) over 1 year | Physical, psychological, and social | [26] |
| Program of moderate-intensity aerobic exercises, performed at home, facilitated by weekly telephone calls, over 6 months | Physical and psychological | [27] |
| Intervention | Health Gains | Studies |
|---|---|---|
| Intervention over 12 months consisting of the transmission of information about healthy lifestyles (fruit and vegetable consumption and physical exercise) by sending 4 personalized communication letters (TPC) | Adherence to physical exercise; adherence to the consumption of fruits and vegetables | [18] |
| Intervention implemented across 12 weeks that consisted of a multidisciplinary, individualized aerobic exercise training program, 30 to 50 min per session, combined with motivational telephone interviews, once a week, with duration of 15 to 30 min | Improvement in physical condition; increased handgrip strength; increased cardiorespiratory fitness | [19] |
| Health education conducted by peers over 12 months | Increase in healthy behaviors | [20] |
| Design of a personalized plan for behavior change | Improved health-related quality of life (in all dimensions) | [21] |
| Education about healthy lifestyles complemented by social telephone calls | Weight decrease | [22] |
| Intervention implemented over 3 months that consisted of the use of 2 different commercial smart devices (bracelet and watch) | Stress management; increased knowledge (self-actualization); increased quality of life. | [23] |
| Promotion of physical and mental exercise, healthy eating (increased consumption of fruit and vegetables), and adoption of healthier habits (physical, mental, and cognitive) over 8 weeks | Increased quality of life (in all subscales) | [24] |
| Implementation of an intensive 2.5-day group program to promote well-being (combining cognitive behavioral theory and acceptance and commitment therapy), followed by periodic follow-ups at 6, 12, and 18 months | Increased quality of life; increased well-being | [25] |
| Implementation of an intensive intervention on lifestyle (physical exercise, nutrition, sleep, management of chronic disease) over 1 year | Increased health-related quality of life | [26] |
| Program of moderate-intensity aerobic exercises, performed at home, facilitated by weekly telephone calls, over 6 months | Increased quality of life | [27] |
| Interventions’ Themes | Health Gains |
|---|---|
| Mental health | Increased knowledge (self-actualization) |
| Physical activity and physical condition | Adherence to physical exercise |
| Improvement in physical condition | |
| Nutrition habits | Adherence to the consumption of fruits and vegetables |
| Quality of life | Increased quality of life |
| Well-being | Increased well-being |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, E.M.C.P.; Canhestro, A.M.G.D.S.; Rosário, J.M.O.A.; Fonseca, C.J.V.; Pinho, L.M.G.; Arco, H.M.S.L.R. Efficacy of Health Promotion Interventions Aimed to Improve Health Gains in Middle-Aged Adults—A Systematic Review. Geriatrics 2023, 8, 50. https://doi.org/10.3390/geriatrics8030050
Santos EMCP, Canhestro AMGDS, Rosário JMOA, Fonseca CJV, Pinho LMG, Arco HMSLR. Efficacy of Health Promotion Interventions Aimed to Improve Health Gains in Middle-Aged Adults—A Systematic Review. Geriatrics. 2023; 8(3):50. https://doi.org/10.3390/geriatrics8030050
Chicago/Turabian StyleSantos, Eunice M. C. P., Ana M. G. D. S. Canhestro, Jorge M. O. A. Rosário, César J. V. Fonseca, Lara M. G. Pinho, and Helena M. S. L. R. Arco. 2023. "Efficacy of Health Promotion Interventions Aimed to Improve Health Gains in Middle-Aged Adults—A Systematic Review" Geriatrics 8, no. 3: 50. https://doi.org/10.3390/geriatrics8030050
APA StyleSantos, E. M. C. P., Canhestro, A. M. G. D. S., Rosário, J. M. O. A., Fonseca, C. J. V., Pinho, L. M. G., & Arco, H. M. S. L. R. (2023). Efficacy of Health Promotion Interventions Aimed to Improve Health Gains in Middle-Aged Adults—A Systematic Review. Geriatrics, 8(3), 50. https://doi.org/10.3390/geriatrics8030050