
Factors Affecting Hospitalization and Death of Older Patients Who Need Long-Term Care—The Necessity of the Support for Dysphagia in Home Dental Care

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants’ Characteristics
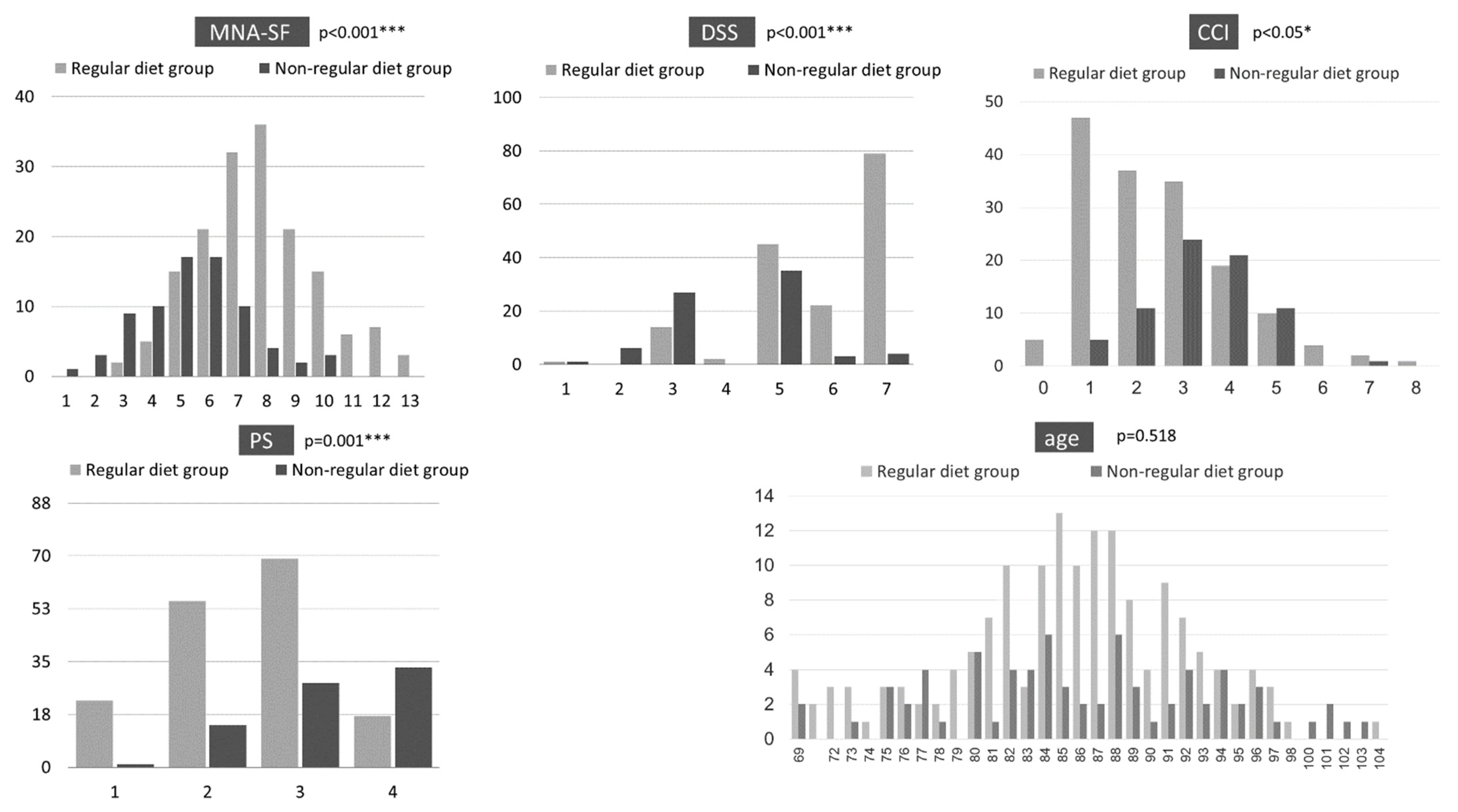
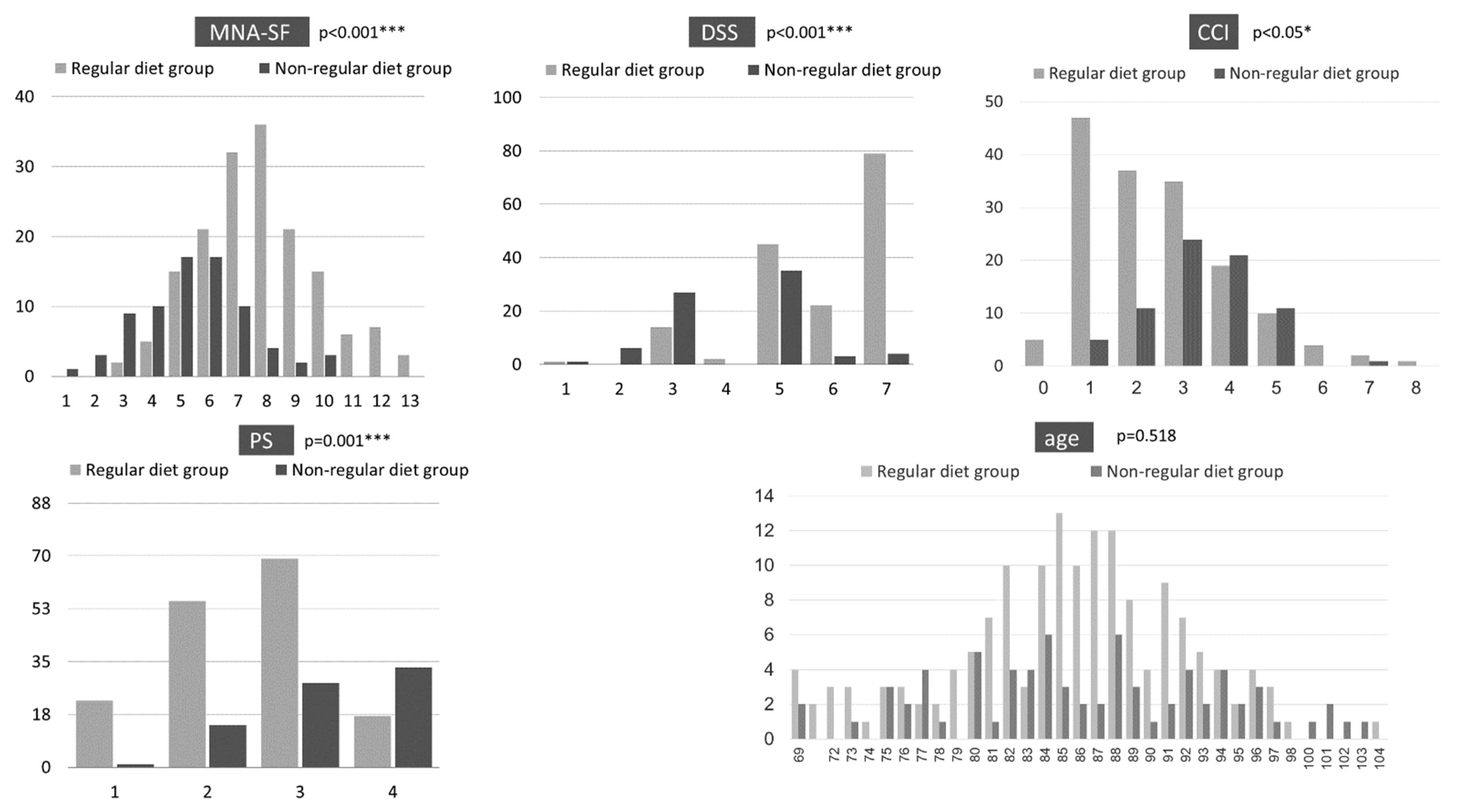
3.2. Cross-Sectional Survey Results
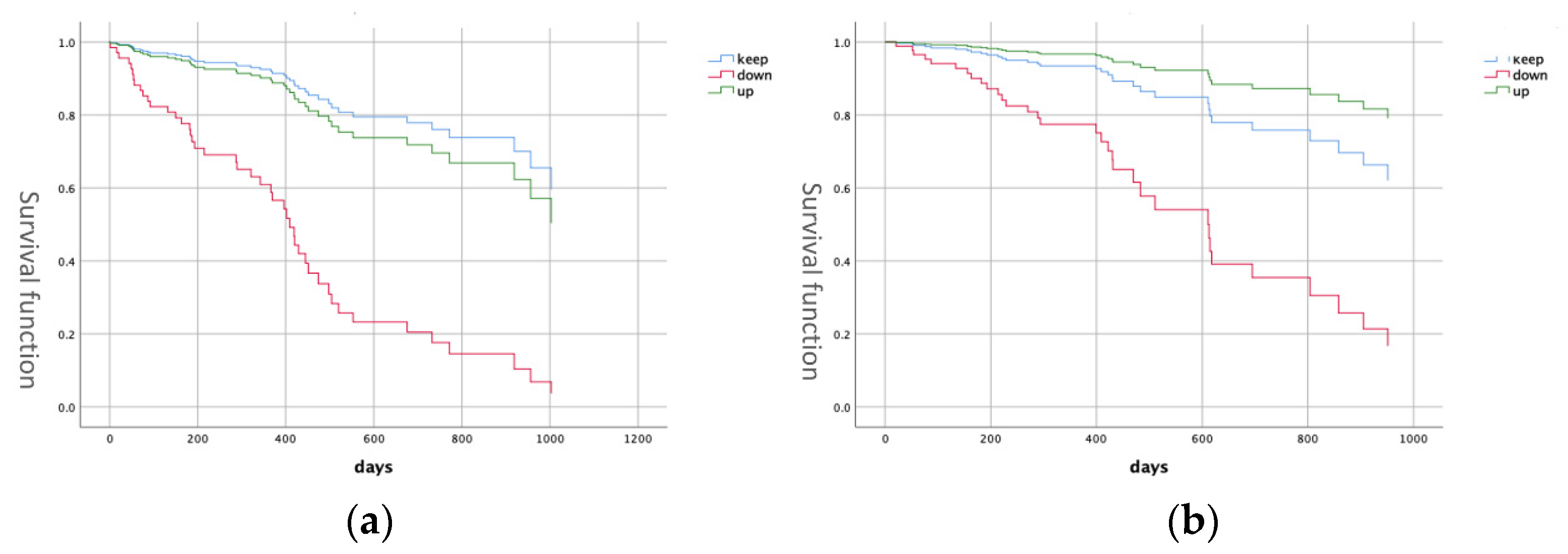
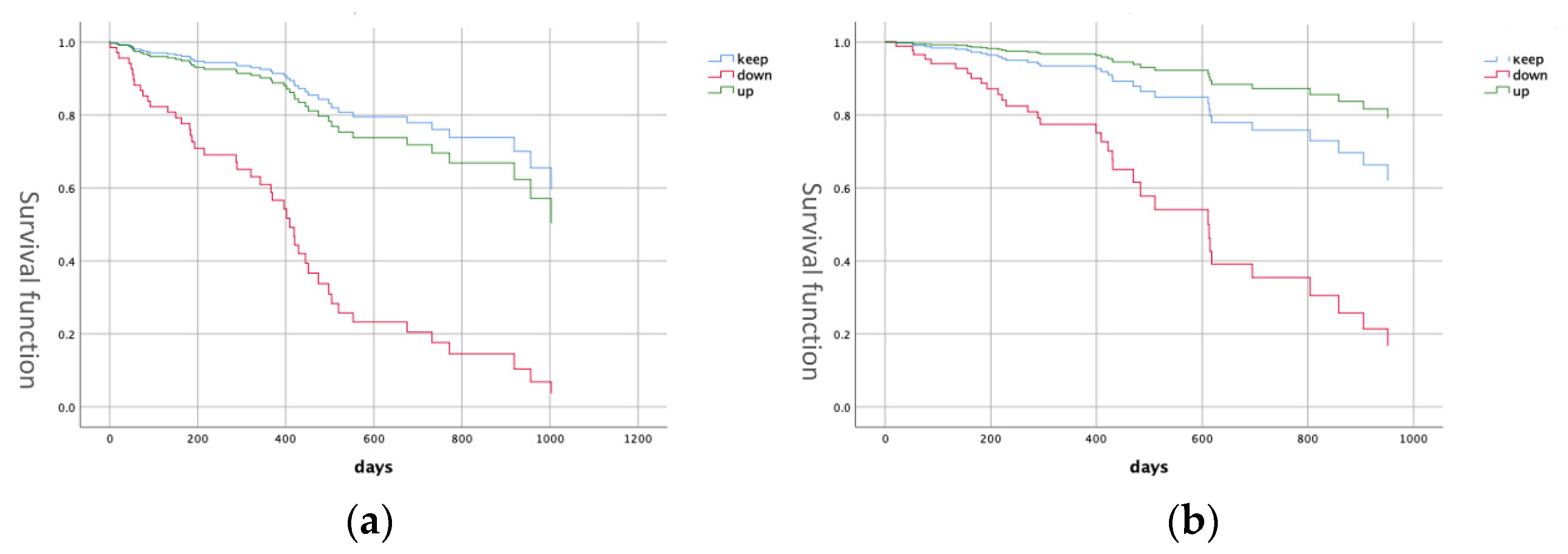
3.3. Prospective Study
4. Discussion
4.1. Comparison of Diet Form
4.2. Factors Influencing Hospitalization and Death
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaitsu, T.; Saito, T.; Kawaguchi, Y. The Oral Healthcare System in Japan. Healthcare 2018, 6, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokobayashi, K.; Matsushima, M.; Fujinuma, Y.; Tazuma, S. Retrospective cohort study of the incidence and risk of fever in elderly people living at home: A pragmatic aspect of home medical management in Japan. Geriatr. Gerontol. Int. 2013, 13, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of independence in activities of daily living in older adults hospitalized with medical illness. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Baba, M.; Saitoh, E.; Okada, S. Dysphagia rehabilitation in Japan. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 929–938. [Google Scholar] [CrossRef]
- Tohara, H.; Iida, T.; Inoue, M.; Sato, M.; Wada, S.; Sanpei, R.; Okada, T.; Shimano, T.; Ebihara, K.; Ueda, K. Dysphagia rehabilitation in visiting home care. Gan Kagaku Ryoho 2010, 37 (Suppl. S2), 159–161. (In Japanese) [Google Scholar]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef]
- Ishimaru, M.; Ono, S.; Morita, K.; Matsui, H.; Yasunaga, H. Domiciliary dental care among homebound older adults: A nested case-control study in Japan. Geriatr. Gerontol. Int. 2019, 19, 679–683. [Google Scholar] [CrossRef]
- Watanabe, K.; Umegaki, H.; Huang, C.; Martins, B.A.; Asai, A.; Kanda, S.; Nomura, H.; Kuzuya, M. Association between dysphagia risk and unplanned hospitalization in older patients receiving home medical care. Geriatr. Gerontol. Int. 2019, 19, 977–981. [Google Scholar] [CrossRef]
- Nishimura, K.; Kagaya, H.; Shibata, S.; Onogi, K.; Inamoto, Y.; Ota, K.; Miki, T.; Tamura, S.; Saitoh, E. Accuracy of Dysphagia Severity Scale rating without using videoendoscopic evaluation of swallowing. Jpn. J. Compr. Rehabil. Sci. 2015, 6, 124–128. [Google Scholar]
- Phillips, M.B.; Foley, A.L.; Barnard, R.; Isenring, E.A.; Miller, M.D. Nutritional screening in community-dwelling older adults: A systematic literature review. Asia Pac. J. Clin. Nutr. 2010, 19, 440–449. [Google Scholar]
- Tamura, B.K.; Bell, C.; Masaki, K.H.; Amella, E. Factors Associated with Weight Loss, Low BMI, and Malnutrition Among Nursing Home Patients: A Systematic Review of the Literature. J. Am. Med. Dir. Assoc. 2013, 14, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Furuta, M.; Komiya-Nonaka, M.; Akifusa, S.; Shimazaki, Y.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Interrelationship of oral health status, swallowing function, nutritional status, and cognitive ability with activities of daily living in Japanese elderly people receiving home care services due to physical disabilities. Community Dent. Oral Epidemiol. 2013, 41, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K.; Furuta, M.; Okabe, Y.; Suma, S.; Takeshita, T.; Akifusa, S.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Swallowing disorders and 1-year functional decline in community-dwelling older adults receiving home care. J. Oral Rehabil. 2017, 44, 982–987. [Google Scholar] [CrossRef]
- Da Silva, A.F.; Moreira, E.A.M.; Barni, G.C.; Panza, V.S.P.; Furkim, A.M.; Moreno, Y.M.F. Relationships between high comorbidity index and nutritional parameters in patients with Oropharyngeal Dysphagia. Clin. Nutr. ESPEN 2020, 38, 218–222. [Google Scholar] [CrossRef]
- Onodera, S.; Furuya, J.; Yamamoto, H.; Tamada, Y.; Kondo, H. Effects of wearing and removing dentures on oropharyngeal motility during swallowing. J. Oral Rehabil. 2016, 43, 847–854. [Google Scholar] [CrossRef]
- Furuya, J.; Tamada, Y.; Sato, T.; Hara, A.; Nomura, T.; Kobayashi, T.; Sakai, M.; Kondo, H. Wearing complete dentures is associated with changes in the three-dimensional shape of the oropharynx in edentulous older people that affect swallowing. Gerodontology 2016, 33, 513–521. [Google Scholar] [CrossRef]
- Yamamoto, H.; Furuya, J.; Tamada, Y.; Kondo, H. Impacts of wearing complete dentures on bolus transport during feeding in elderly edentulous. J. Oral Rehabil. 2013, 40, 923–931. [Google Scholar] [CrossRef]
- Gjestsen, M.T.; Brønnick, K.; Testad, I. Characteristics and predictors for hospitalizations of home-dwelling older persons receiving community care: A cohort study from Norway. BMC Geriatr. 2018, 18, 203. [Google Scholar] [CrossRef]
- Tsuji, T.; Yamamoto, K.; Yamasaki, K.; Hayashi, F.; Momoki, C.; Yasui, Y.; Ohfuji, S.; Fukushima, W.; Habu, D. Lower dietary variety is a relevant factor for malnutrition in older Japanese home-care recipients: A cross-sectional study. BMC Geriatr. 2019, 19, 197. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, S.J.; Choi, Y.H.; Lee, J.H.; Chang, J.H.; Ryu, Y.J. Clinical outcomes and prognostic factors in patients directly transferred to the intensive care unit from long-term care beds in institutions and hospitals: A retrospective clinical study. BMC Geriatr. 2018, 18, 259. [Google Scholar] [CrossRef] [PubMed]
- Vossius, C.; Selbæk, G.; Benth, J.; Bergh, S. Mortality in nursing home residents: A longitudinal study over three years. PLoS ONE 2018, 13, e0203480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkisas, S.; De Cock, A.-M.; Vandewoude, M.; Verhoeven, V. Prevalence of sarcopenia and 9-year mortality in nursing home residents. Aging Clin. Exp. Res. 2019, 31, 951–959. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Regular Diet Group | Non-Regular Diet Group | |||||||
|---|---|---|---|---|---|---|---|---|
| stable | declined | improved | stable | declined | improved | |||
| n = 107 | n = 21 | n = 5 | n = 107 | n = 21 | n = 5 | |||
| (65.6%) | (12.9%) | (3.1%) | (65.6%) | (12.9%) | (3.1%) | |||
| PS | p < 0.001 *** | p = 0.186 | ||||||
| 1 | 16 (15%) | 0 | 1 (20%) | improved-declined | 0 | 1 (20%) | 0 | |
| 2 | 40 (37%) | 3 (14%) | 3 (60%) | p = 0.01 ** | 5 (17%) | 0 | 6 (30%) | |
| 3 | 46 (43%) | 10 (48%) | 0 | stable-declined | 11 (38%) | 1 (20%) | 10 (50%) | |
| 4 | 5 (5%) | 8 (38%) | 1 (20%) | p < 0.001 *** | 13 (45%) | 3 (60%) | 4 (20%) | |
| MNA-SF | p = 0.239 | |||||||
| Malnutrition | 40 (37%) | 14 (67%) | 2 (40%) | p = 0.007 ** | 23 (79%) | 5 (100%) | 18 (90%) | |
| At risk | 59 (55%) | 7 (33%) | 3 (60%) | stable-declined | 6 (21%) | 0 | 2 (10%) | |
| Good | 8 (7%) | 0 | 0 | p = 0.002 ** | 0 | 0 | 0 | |
| PS-1y | p < 0.001 *** | p = 0.101 | ||||||
| 1 | 14 (13%) | 0 | 1 (20%) | improved-declined | 0 | 0 | 0 | |
| 2 | 40 (37%) | 1 (5%) | 3 (60%) | p = 0.04 * | 5 (17%) | 0 | 8 (40%) | |
| 3 | 46 (43%) | 11 (52%) | 0 | stable-declined | 13 (45%) | 2 (40%) | 8 (40%) | |
| 4 | 7 (7%) | 9 (43%) | 1 (20%) | p < 0.001 *** | 11 (38%) | 3 (60%) | 4 (20%) | |
| MNA-SF-1y | p < 0.001 *** | |||||||
| Malnutrition | 45 (42%) | 16 (76%) | 1 (20%) | improved-declined | 23 (79%) | 5 (100%) | 13 (65%) | p = 0.031 * |
| At risk | 55 (51%) | 5 (24%) | 4 (80%) | p = 0.04 * | 6 (21%) | 0 | 6 (30%) | improved-declined |
| Good | 7 (7%) | 0 | 0 | stable-declined | 0 | 0 | 1 (5%) | p = 0.02 * |
| p < 0.001 *** | ||||||||
| No Hospitalization n = 186 (77.8%) | With Hospitalization n = 53 (22.2%) | Univariate | Proportional Hazard | |||
|---|---|---|---|---|---|---|
| p Value | Hazard Ratio | 95% CI | ||||
| MNA-SF |
1:1 2:3 3:9 4:12 5:22 6:27 7:31 8:32 9:20 10:16 11:3 12:7 13:3 |
2:1 3:2 4:3 5:10 6:11 7:10 8:8 9:3 10:2 11:3 | p = 0.111 | p = 0.60 | 0.95 | 0.82–1.13 |
| PS | 1:20 (10.8%) 2:58 (31.2%) 3:76 (40.9%) 4:32 (17.2%) | 1:3 (5.7%) 2:11 (20.8%) 3:21 (39.6%) 4:18 (34.0%) | p = 0.007 ** | p = 0.17 | 1.43 | 0.86–2.37 |
| Age | 84.8 | 83.2 | p = 0.272 | p = 0.89 | 0.99 | 0.97–1.03 |
| FOIS Change | stable: 114 (80.3%) declined: 8 (5.6%) improved: 20 (14.1%) | stable: 22 (48.9%) declined: 18 (40.0%) improved: 5 (11.1%) | p < 0.001 *** | p < 0.001 *** stable-improved: p = 0.50 stable-declined: p < 0.001*** | stable-improved: 0.71 stable-declined: 4.63 | stable-improved: 0.26–1.93 stable-declined: 1.65–13.0 |
| DSS |
1:1 (0.5%) 2:3 (1.6%) 3:28 (15.1%) 4:1 (0.5%) 5:63 (33.9%) 6:22 (11.8%) 7:68 (36.6%) |
1:1 (1.9%) 2:3 (1.6%) 3:13 (15.1%) 4:1 (1.9%) 5:17 (32.1%) 6:3 (5.7%) 7:15 (28.3%) | p = 0.024 * | p = 0.12 | 0.83 | 0.65–1.05 |
| CCI |
0:5 (2.7%) 1:46 (24.7%) 2:35 (18.8%) 3:45 (24.2%) 4:31 (16.7%) 5:18 (9.7%) 6:4 (2.2%) 7:1 (0.5%) 8:1 (0.5%) |
0:0 1:7 (13.2%) 2:15 (28.3%) 3:16 (30.2%) 4:10 (18.9%) 5:3 (5.7%) 6:0 7:2 (3.7%) 8:0 | p = 0.188 | p = 0.42 | 0.89 | 0.68–1.05 |
| Survival n = 184 (77.0%) | Death n = 55 (23.0%) | Univariate | Proportional Hazard | |||
|---|---|---|---|---|---|---|
| p Value | Hazard Ratio | 95% CI | ||||
| MNA-SF | 2:2 3:5 4:8 5:23 6:26 7:34 8:36 9:20 10:15 11:6 12:7 13:2 | 1:1 2:1 3:5 4:7 5:9 6:12 7:8 8:5 9: 10:3 13:1 | p < 0.001 *** | p = 0.20 | 0.88 | 0.72–1.07 |
| PS | 1:20 (11.0%) 2:59 (32.6%) 3:74 (40.9%) 4:28 (15.5%) | 1:3 (5.5%) 2:10 (18.2%) 3:23 (41.8%) 4:19 (34.5%) | p = 0.001 ** | p = 0.37 | 1.29 | 0.74–2.28 |
| Age | 83.6 | 87.5 | p = 0.013 * | p = 0.23 | 1.03 | 0.98–1.07 |
| FOIS Change | stable:115 (61.9%) declined: 16 (8.8%) improved: 23 (12.7%) | stable: 21 (63.6%) declined: 10 (30.3%) improved: 2 (6.1%) | p = 0.007 ** | p = 0.005 ** stable-improved: p = 0.34 stable-declined: p = 0.011 * | stable-improved: 2.05 stable-declined: 7.77 | stable-improved: 0.47–8.91 stable-declined: 1.61–37.5 |
| DSS |
1:2 (1.1%) 2:4 (2.2%) 3:22 (11.6%) 5:61 (33.7%) 6:20 (11.0%) 7:75 (40.3%) |
2:2 (3.6%) 3:17 (30.9%) 4:2 (3.6%) 5:19 (34.5%) 6:5 (9.1%) 7:10 (18.2%) | p < 0.001 *** | p = 0.19 | 0.83 | 0.64–1.09 |
| CCI |
0:5 (2.7%) 1:41 (22.2%) 2:44 (23.9%) 3:45 (24.5%) 4:32 (17.4%) 5:14 (7.6%) 6:3 (1.6%) 7:0 8:0 |
0:0 1:12 (21.8%) 2:7 (12.7%) 3:16 (29.1%) 4:9 (16.3%) 5:6 (10.9%) 6:1 (1.8%) 7:3 (5.5%) 8:1 (1.8%) | p = 0.026 * | p = 0.75 | 0.95 | 0.70–1.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakasugi, Y.; Susa, C.; Murata, S.; Aida, J.; Sasaki, J.; Furuya, J.; Tohara, H. Factors Affecting Hospitalization and Death of Older Patients Who Need Long-Term Care—The Necessity of the Support for Dysphagia in Home Dental Care. Geriatrics 2022, 7, 37. https://doi.org/10.3390/geriatrics7020037
Wakasugi Y, Susa C, Murata S, Aida J, Sasaki J, Furuya J, Tohara H. Factors Affecting Hospitalization and Death of Older Patients Who Need Long-Term Care—The Necessity of the Support for Dysphagia in Home Dental Care. Geriatrics. 2022; 7(2):37. https://doi.org/10.3390/geriatrics7020037
Chicago/Turabian StyleWakasugi, Yoko, Chiaki Susa, Shino Murata, Jun Aida, Jun Sasaki, Junichi Furuya, and Haruka Tohara. 2022. "Factors Affecting Hospitalization and Death of Older Patients Who Need Long-Term Care—The Necessity of the Support for Dysphagia in Home Dental Care" Geriatrics 7, no. 2: 37. https://doi.org/10.3390/geriatrics7020037
APA StyleWakasugi, Y., Susa, C., Murata, S., Aida, J., Sasaki, J., Furuya, J., & Tohara, H. (2022). Factors Affecting Hospitalization and Death of Older Patients Who Need Long-Term Care—The Necessity of the Support for Dysphagia in Home Dental Care. Geriatrics, 7(2), 37. https://doi.org/10.3390/geriatrics7020037