
Interventions for Nursing Home Residents with Dysphagia—A Scoping Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Knowledge Synthesis
3. Results
3.1. Feeding Intervention
3.2. Oral Hygiene
3.3. Stimulation—Taste and Smell
3.4. Training
3.5. Caregiver Algorithm
3.6. Teaching the Residents Compensatory Strategies
3.7. Mobilization of the Spine
3.8. Positioning, Oral Hygiene, and Swallowing Techniques
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Search Strategies in PubMed

{kind=link}
{kind=link}
| No. | Query | Results |
|---|---|---|
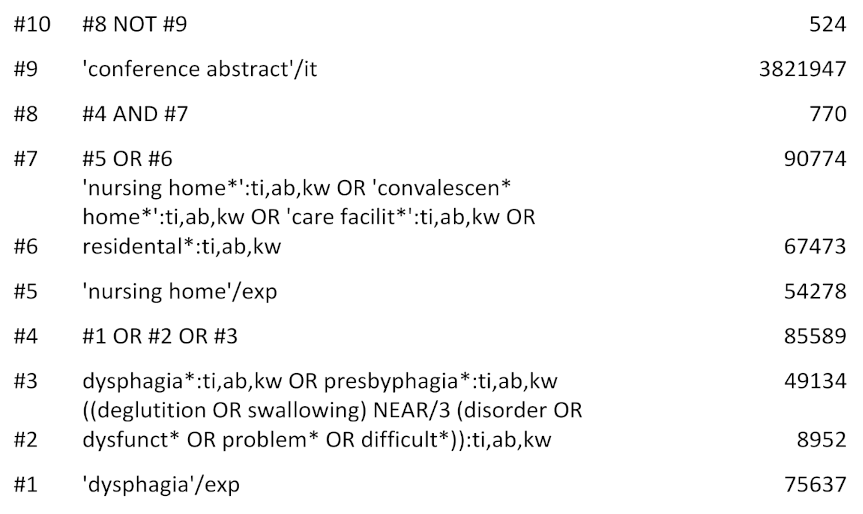
| #10 | #8 NOT #9 | 524 |
| #9 | ‘conference abstract’/it | 3,821,947 |
| #8 | #4 AND #7 | 770 |
| #7 | #5 OR #6 | 90,774 |
| #6 | ‘nursing home*’:ti,ab,kw OR ‘convalescen* home*’:ti,ab,kw OR ‘care facilit*’:ti,ab,kw OR residental*:ti,ab,kw | 67,473 |
| #5 | ‘nursing home’/exp | 54,278 |
| #4 | #1 OR #2 OR #3 | 85,589 |
| #3 | dysphagia*:ti,ab,kw OR presbyphagia*:ti,ab,kw | 49,134 |
| #2 | ((deglutition OR swallowing) NEAR/3 (disorder OR dysfunct* OR problem* OR difficult*)):ti,ab,kw | 8952 |
| #1 | ‘dysphagia’/exp | 75,637 |
| ID | Search | Hits |
|---|---|---|
| #1 | MeSH descriptor: [Nursing Homes] explode all trees | 1334 |
| #2 | (“nursing home*” OR “convalescence home*” OR “convalescent home*” OR “care facilit*” OR residental*):ti,ab,kw | 3363 |
| #3 | #1 OR #2 | 3803 |
| #4 | MeSH descriptor: [Deglutition Disorders] explode all trees | 2834 |
| #5 | (((deglutition OR swallowing) NEAR/3 (disorder OR dysfunct* OR problem* OR difficult*))):ti,ab,kw | 804 |
| #6 | (dysphagia* OR presbyphagia*):ti,ab,kw | 4057 |
| #7 | #4 OR #5 OR #6 | 6590 |
| #8 | #3 AND #7 | 34 |
| Search ID# | Search Terms | Results |
|---|---|---|
| S8 | S4 AND S7 | 415 |
| S7 | S5 OR S6 | 69,092 |
| S6 | “nursing home*” OR “convalescen* home*” OR “care facilit*” OR residental* | 66,004 |
| S5 | (MH “Nursing Homes+”) | 27,595 |
| S4 | S1 OR S2 OR S3 | 13,469 |
| S3 | dysphagia* OR presbyphagia* | 8683 |
| S2 | ((deglutition OR swallowing) N3 (disorder OR dysfunct* OR problem* OR difficult*)) | 9720 |
| S1 | (MH “Deglutition Disorders”) | 8508 |
References
- Baijens, L.W.; Clave, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders—European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clave, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons—From pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging 2016, 11, 189–208. [Google Scholar] [CrossRef]
- Altman, K.W. Oropharyngeal dysphagia pathophysiology, complications and science-based interventions. Nestle Nutr. Inst. Workshop Ser. 2012, 72, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabre, M.; Serra-Prat, M.; Clave, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22, 851–858.e230. [Google Scholar] [CrossRef] [PubMed]
- Namasivayam, A.M.; Steele, C.M. Malnutrition and Dysphagia in long-term care: A systematic review. J. Nutr. Gerontol. Geriatr. 2015, 34, 1–21. [Google Scholar] [CrossRef]
- Sarabia-Cobo, C.M.; Pérez, V.; De Lorena, P.; Domínguez, E.; Hermosilla, C.; Nuñez, M.J.; Vigueiro, M.; Rodríguez, L. The incidence and prognostic implications of dysphagia in elderly patients institutionalized: A multicenter study in Spain. Appl. Nurs. Res. 2016, 30, e6–e9. [Google Scholar] [CrossRef]
- Langmore, S.E.; Olney, R.K.; Lomen-Hoerth, C.; Miller, B.L. Dysphagia in patients with frontotemporal lobar dementia. Arch. Neurol. 2007, 64, 58–62. [Google Scholar] [CrossRef]
- Horner, J.; Alberts, M.J.; Dawson, D.V.; Cook, G.M. Swallowing in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 1994, 8, 177–189. [Google Scholar]
- Clave, P.; Rofes, L.; Carrion, S.; Ortega, O.; Cabre, M.; Serra-Prat, M.; Arreola, V. Pathophysiology, relevance and natural history of oropharyngeal dysphagia among older people. Nestle Nutr. Inst. Workshop Ser. 2012, 72, 57–66. [Google Scholar] [CrossRef]
- Pu, D.; Murry, T.; Wong, M.C.M.; Yiu, E.M.L.; Chan, K.M.K. Indicators of dysphagia in aged care facilities. J. Speech-Lang. Hear. Res. 2017, 60, 2416–2426. [Google Scholar] [CrossRef]
- Park, Y.-H.; Han, H.-R.; Oh, B.-M.; Lee, J.; Park, J.; Yu, S.J.; Chang, H. Prevalence and associated factors of dysphagia in nursing home residents. Geriatr. Nurs. 2013, 34, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Pu, D.; Yiu, E.M.L.; Chan, K.M.K. Factors associated with signs of aspiration in older adults: A prospective study. Geriatr. Nurs. 2020, 41, 635–640. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Palomera, M.; Gomez, C.; Sar-Shalom, D.; Saiz, A.; Montoya, J.G.; Navajas, M.; Palomera, E.; Clave, P. Oropharyngeal dysphagia as a risk factor for malnutrition and lower respiratory tract infection in independently living older persons: A population-based prospective study. Age Ageing 2012, 41, 376–381. [Google Scholar] [CrossRef]
- Ekberg, O.; Hamdy, S.; Woisard, V.; Wuttge-Hannig, A.; Ortega, P. Social and psychological burden of dysphagia: Its impact on diagnosis and treatment. Dysphagia 2002, 17, 139–146. [Google Scholar] [CrossRef]
- Nicolle, L.E.; Strausbaugh, L.J.; Garibaldi, R.A. Infections and antibiotic resistance in nursing homes. Clin. Microbiol. Rev. 1996, 9, 1–17. [Google Scholar] [CrossRef]
- Van der Maarel-Wierink, C.D.; Vanobbergen, J.N.; Bronkhorst, E.M.; Schols, J.M.; de Baat, C. Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J. Dent. Res. 2011, 90, 1398–1404. [Google Scholar] [CrossRef]
- Almirall, J.; Cabré, M.; Clavé, P. Complications of oropharyngeal dysphagia: Aspiration pneumonia. Nestle Nutr. Inst. Workshop Ser. 2012, 72, 67–76. [Google Scholar] [CrossRef]
- Hollaar, V.R.Y.; van der Putten, G.-J.; van der Maarel-Wierink, C.D.; Bronkhorst, E.M.; de Swart, B.J.M.; de Baat, C.; Creugers, N.H.J. Nursing home-acquired pneumonia, dysphagia and associated diseases in nursing home residents: A retrospective, cross-sectional study. Geriatr. Nurs. 2017, 38, 437–441. [Google Scholar] [CrossRef]
- Quagliarello, V.; Ginter, S.; Han, L.; Van Ness, P.; Allore, H.; Tinetti, M. Modifiable risk factors for nursing home-acquired pneumonia. Clin. Infect. Dis. 2005, 40, 1–6. [Google Scholar] [CrossRef]
- Wirth, R.; Pourhassan, M.; Streicher, M.; Hiesmayr, M.; Schindler, K.; Sieber, C.C.; Volkert, D. The impact of dysphagia on mortality of nursing home residents: Results from the nutritionDay project. J. Am. Med. Dir. Assoc. 2018, 19, 775–778. [Google Scholar] [CrossRef]
- Hoshino, D.; Watanabe, Y.; Edahiro, A.; Kugimiya, Y.; Igarashi, K.; Motokawa, K.; Ohara, Y.; Hirano, H.; Myers, M.; Hironaka, S.; et al. Association between simple evaluation of eating and swallowing function and mortality among patients with advanced dementia in nursing homes: 1-year prospective cohort study. Arch. Gerontol. Geriatr. 2020, 87, 103969. [Google Scholar] [CrossRef]
- Jukic Peladic, N.; Orlandoni, P.; Dell’Aquila, G.; Carrieri, B.; Eusebi, P.; Landi, F.; Volpato, S.; Zuliani, G.; Lattanzio, F.; Cherubini, A. Dysphagia in nursing home residents: Management and outcomes. J. Am. Med. Dir. Assoc. 2019, 20, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Forough, A.S.; Wong, S.Y.M.; Lau, E.T.L.; Santos, J.M.S.; Kyle, G.J.; Steadman, K.J.; Cichero, J.A.Y.; Nissen, L.M. Nurse experiences of medication administration to people with swallowing difficulties living in aged care facilities: A systematic review of qualitative evidence. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 71–86. [Google Scholar] [CrossRef]
- Loeb, M.B.; Becker, M.; Eady, A.; Walker-Dilks, C. Interventions to prevent aspiration pneumonia in older adults: A systematic review. J. Am. Geriatr. Soc. 2003, 51, 1018–1022. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pr. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Klor, B.M.; Milianti, F.J. Rehabilitation of neurogenic dysphagia with percutaneous endoscopic gastrostomy. Dysphagia 1999, 14, 162–164. [Google Scholar] [CrossRef]
- Lin, L.-C.; Wang, S.-C.; Chen, S.H.; Wang, T.-G.; Chen, M.-Y.; Wu, S.-C. Efficacy of swallowing training for residents following stroke. J. Adv. Nurs. 2003, 44, 469–478. [Google Scholar] [CrossRef]
- Pelletier, C.A.; Lawless, H.T. Effect of citric acid and citric acid-sucrose mixtures on swallowing in neurogenic oropharyngeal dysphagia. Dysphagia 2003, 18, 231–241. [Google Scholar] [CrossRef]
- Ebihara, T.; Ebihara, S.; Maruyama, M.; Kobayashi, M.; Itou, A.; Arai, H.; Sasaki, H. A randomized trial of olfactory stimulation using black pepper oil in older people with swallowing dysfunction. J. Am. Geriatr. Soc. 2006, 54, 1401–1406. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.A.; Barr, S.I. Provision of small, frequent meals does not improve energy intake of elderly residents with dysphagia who live in an extended-care facility. J. Am. Diet. Assoc. 2006, 106, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Bautmans, I.; Demarteau, J.; Cruts, B.; Lemper, J.-C.; Mets, T. Dysphagia in elderly nursing home residents with severe cognitive impairment can be attenuated by cervical spine mobilization. J. Rehabil. Med. 2008, 40, 755–760. [Google Scholar] [CrossRef]
- Quagliarello, V.; Juthani-Mehta, M.; Ginter, S.; Towle, V.; Allore, H.; Tinetti, M. Pilot testing of intervention protocols to prevent pneumonia in nursing home residents. J. Am. Geriatr. Soc. 2009, 57, 1226–1231. [Google Scholar] [CrossRef]
- Hanson, L.C.; Carey, T.S.; Caprio, A.J.; Lee, T.J.; Ersek, M.; Garrett, J.; Jackman, A.; Gilliam, R.; Wessell, K.; Mitchell, S.L. Improving decision-making for feeding options in advanced dementia: A randomized, controlled trial. J. Am. Geriatr. Soc. 2011, 59, 2009–2016. [Google Scholar] [CrossRef]
- Park, Y.; Oh, S.; Chang, H.; Bang, H.L. Effects of the evidence-based nursing care algorithm of dysphagia for nursing home residents. J. Gerontol. Nurs. 2015, 41, 30–39. [Google Scholar] [CrossRef]
- Benigas, J.E.; Bourgeois, M. Using spaced retrieval with external aids to improve use of compensatory strategies during eating for persons with dementia. Am. J. Speech-Lang. Pathol. 2016, 25, 321–334. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, L.L.; Li, H.; Lin, R.; Zheng, J.H.; Wei, Y.P.; Li, J.; Chen, P.; Chen, H.Y. Effects of a feeding intervention in patients with Alzheimer’s disease and dysphagia. J. Clin. Nurs. 2016, 25, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Hollaar, V.R.Y.; van der Putten, G.-J.; Van der Maarel-Wierink, C.D.; Bronkhorst, E.M.; de Swart, B.J.M.; Creugers, N.H.J. The effect of a daily application of a 0.05% chlorhexidine oral rinse solution on the incidence of aspiration pneumonia in nursing home residents: A multicenter study. BMC Geriatr. 2017, 17, 128. [Google Scholar] [CrossRef]
- Jablonski, R.A.; Winstead, V.; Azuero, A.; Ptacek, T.; Jones-Townsend, C.; Byrd, E.; Geisinger, M.L.; Morrow, C. Feasibility of providing safe mouth care and collecting oral and fecal microbiome samples from nursing home residents with dysphagia: Proof of concept study. J. Gerontol. Nurs. 2017, 43, 9–15. [Google Scholar] [CrossRef]
- Zanini, M.; Bagnasco, A.; Catania, G.; Aleo, G.; Sartini, M.; Cristina, M.L.; Ripamonti, S.; Monacelli, F.; Odetti, P.; Sasso, L. A Dedicated Nutritional Care Program (NUTRICARE) to reduce malnutrition in institutionalised dysphagic older people: A quasi-experimental study. J. Clin. Nurs. 2017, 26, 4446–4455. [Google Scholar] [CrossRef]
- Hollaar, V.; van der Maarel-Wierink, C.; Van der Putten, G.-J.; de Swart, B.; de Baat, C. Effect of daily application of a 0.05% chlorhexidine solution on the incidence of (aspiration) pneumonia in care home residents: Design of a multicentre cluster randomised controlled clinical trial. BMJ Open 2015, 5, e007889. [Google Scholar] [CrossRef]
- Rudberg, M.A.; Egleston, B.L.; Grant, M.D.; Brody, J.A. Effectiveness of feeding tubes in nursing home residents with swallowing disorders. J. Parenter. Enter. Nutr. 2000, 24, 97–102. [Google Scholar] [CrossRef]
- Ballesteros-Pomar, M.D.; Cherubini, A.; Keller, H.; Lam, P.; Rolland, Y.; Simmons, S.F. Texture-modified diet for improving the management of oropharyngeal dysphagia in nursing home residents: An expert review. J. Nutr. Health Aging 2020, 24, 576–581. [Google Scholar] [CrossRef]
- Cockburn, N.; Pateman, K.; Taing, M.W.; Pradhan, A.; Ford, P.J. Managing the oral side-effects of medications used to treat multiple sclerosis. Aust. Dent. J. 2017, 62, 331–336. [Google Scholar] [CrossRef]
- NICE. Managing Medicines in Care Homes; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Adhikari, R.; Tocher, J.; Smith, P.; Corcoran, J.; MacArthur, J. A multi-disciplinary approach to medication safety and the implication for nursing education and practice. Nurse Educ. Today 2014, 34, 185–190. [Google Scholar] [CrossRef]
- Iyer, A.; Heathcote, D. Safe Swallowing of Oral Liquid Medications in Patients with Dysphagia A Patient Quality & Safety Initiative—Trillium Health Partners. In Proceedings of the CSHP 2015, San Diego, CA, USA, 8–11 October 2015. [Google Scholar]
- Singh, V.; Brockbank, M.J.; Frost, R.A.; Tyler, S. Multidisciplinary management of dysphagia: The first 100 cases. J. Laryngol. Otol. 1995, 109, 419–424. [Google Scholar] [CrossRef]
- Duval, M.; Black, M.A.; Gesser, R.; Krug, M.; Ayotte, D. Multidisciplinary evaluation and management of dysphagia: The role for otolaryngologists. J. Otolaryngol. Head Neck Surg 2009, 38, 227–232. [Google Scholar]
- Aoki, S.; Hosomi, N.; Hirayama, J.; Nakamori, M.; Yoshikawa, M.; Nezu, T.; Kubo, S.; Nagano, Y.; Nagao, A.; Yamane, N.; et al. The multidisciplinary swallowing team approach decreases pneumonia onset in acute stroke patients. PLoS ONE 2016, 11, e0154608. [Google Scholar] [CrossRef]


| Study Aim(s) | Study Design, Inclusion and Exclusion Criteria, Intervention, Data Collection and Analysis Methods | Study Participants | Primary Outcomes | Results | |
|---|---|---|---|---|---|
| Klor, B M et al., 1999 [28] USA | Determining the effects of swallowing therapy. | Intervention study. Inclusion criteria: PEG tube, nonprogressive neurogenic dysphagia (Modified Barium Swallow), neurological and medical stability, and language and cognitive skills. Intervention: treatment with either swallowing therapy (e.g., tongue-resistance and retraction exercises to minimize vallecular residue) and compensatory techniques (e.g., chin-down posture). Individual treatment/training sessions were 20 min twice daily in a period ranging from 2–16 weeks. | n = 16. All male. | The ability to take oral feeding. | All patients had positive effect of the treatment, and oral feeding was introduced in all patients. PEG tubes were removed in 10 of the 16 patients. A mean weight gain of 5.1 pounds and a mean albumin increase of 0.5 g/dL were reached. |
| Lin L et al., 2003 [29] Taiwan | Examining the functional swallowing and nutritional outcomes of swallowing training. | Quasi-experimental parallel cluster design. 7 nursing homes. Inclusion criteria: stroke, dysphagia (FEES), oral intake, mentally and linguistically able to participate. Intervention: the intervention group received a structured swallowing training program, 30 min of swallowing training each day for 6 days per week for 8 weeks. The control group: no training. | Control group n = 14 and intervention group n = 35. | Swallowing volume and swallowing speed. | Mean differences in volume per second, volume per swallow, mid-arm circumference and body weight between pre- and post-training of the experimental group were significantly higher than for the control group, while mean differences in neurological examination and choking frequency during meals for the experimental group were significantly lower than in the control group. |
| Pelletier C A et al., 2003 [30] USA | Investigate the effect of sour (citric acid) and sweet-sour taste. | Controlled clinical trial. Inclusion criteria: neurologic dysphagia (FEES), thickened liquids, stable medical condition. Intervention: during FEES examination, initially presented with water, sour liquid (2.7% citric acid), and sweet-sour mixture (1.11% citric acid 8% sucrose) in 5 mL and cup drinking. | n = 11 | Swallowing impairment (PAS scale), stage transition duration, and frequency of spontaneous swallows. | Citric acid improved swallowing (i.e., less aspiration and penetration) compared with water. Teaspoon delivery of liquids significantly reduced aspiration and penetration compared with natural cup drinking. |
| Ebihara et al., 2006 [31] Japan | Determine the effect of olfactory stimulation with volatile black pepper oil (BPO). | Randomized, controlled study. Inclusion criteria were nursing home residents with physical symptoms and cognitive impairment being stable for the preceding three months, dysphagia (assessment not defined). Exclusion criteria were unstable health conditions. Intervention: (1) BPO-treated group, (2) a lavender oil group, and (3) odorless group. | n = 105 | Latency of the swallowing reflex (LTSR), the number of swallowing movements, serum substance P, and regional cerebral blood flow. | Nasal inhalation of BPO for 1-min shortened LTSR, compared with that of lavender oil and distilled water (p < 0.03). Compared with the period before the study, the 1-month intervention using BPO improved LTSR with an increase of SP (p < 0.01). The number of swallowing movements for 1 min during the nasal inhalation of BPO increased (p < 0.001). |
| Taylor, K A et al., 2006 [32] Canada | Assessing energy content in five vs. three daily meals would improve energy intake. | Crossover study. Inclusion criteria: ≥65 years, dysphagia (prior dysphagia symptoms based on bedside evaluation by an experienced swallowing team) and receiving a texture- modified diet. Exclusion criteria: tube-fed, medically unstable, or receiving a diabetic diet. Intervention: the residents were randomly assigned to three or five meals during an initial 4-day study period, followed by the opposite meal pattern in a second period. | n = 31 | Energy intake. | Average energy intakes were similar between the three- and five-meal patterns (1325 ± 207 kcal/day vs. 1342 ± 177 kcal/day, respectively; p = 0.565); fluid intake was higher with five meals (698±156 mL/day) vs. three (612 ± 176 mL/day;p = 0.003). |
| Bautmans, I et al., 2008 [33] Belgium | Investigating the feasibility of cervical spine mobilization in elderly dementia nursing home residents with dysphagia | A randomized controlled trial with crossover design. Inclusion criteria: ≥65 years, Alzheimer’s dementia (MMSE < 24/30), cervical anterior position, extension or kyphosis and dysphagia (speech therapy report in the medical record). Exclusion criteria: central nervous conditions that could influence swallowing, acute illness or fed by a tube. Intervention: a physiotherapist mobilized the head and cervical spine to correct the patient’s posture. Three sessions were performed during the mobilization week (every 2 days), each session lasting approximately 20 min. Control sessions were identical in planning and duration but consisted of a socializing visit by the physical therapist. | n = 15 | Feasibility (attendance, hostility to therapy, complications) and dysphagia limit (maximal volume of water (0–20 mL) that can be swallowed in a single movement) | 90% of cervical spine mobilization sessions were completed successfully, and no complications were observed. Swallowing capacity improved significantly from 3 mL to 5 mL after one session (p = 0.01) and to 10 mL after the one-week treatment (p = 0.03). |
| Quaglia- rello, V et al., 2009 [34] USA | Identify the feasibility of a multi-component intervention protocol consisting of three different interventions. | Randomized feasibility study. Inclusion criteria: nursing home residents, >age 65 years, swallowing difficulties (cough during swallowing). Exclusion criteria were residents <4 weeks; residents for short-term rehabilitation only; estimated to survive <6 months, tube-fed or had a tracheostomy. Intervention: participants were assigned to three groups: (1) upright feeding positioning, (2) teaching swallowing techniques, or (3) manual oral brushing. | n = 22 | Reduction in the frequency of cough during swallowing— quantified by the number of episodes of coughing while eating in the previous week as follows: never, sometimes (<50% of time), frequently (>50% of time), always. | Episodes of cough during swallowing were reduced at the end of 3 months in 6 of 8 (75%) participants assigned to manual brushing, 3 of 7 (43%) of participants assigned to feeding positioning, and 3 of 7 (43%) of participants assigned to instruction in swallowing techniques. Manual brushing was not significantly more effective than the other two intervention protocols (p = 0.31). |
| Hanson, L C et al., 2011 [35] USA | Testing whether a decision aid, compared to usual care, could improve the quality of decision-making by next-of-kins for nursing home residents with advanced dementia. | Randomised controlled study in 24 nursing homes. Inclusion criteria: nursing home resident, > 65 years, advanced dementia, feeding problems (difficulty swallowing, choking on food or liquid, dehydration, dysphagia, or aspiration). Exclusion criteria: feeding tube, enrolled in hospice, or had weight loss associated with diuresis. Intervention: Next of kins in intervention sites received a structured decision aid providing information about dementia and feeding options. Next of kins in the control group received usual care, including any information from health care providers. Next of kins had in-person interviews with trained research assistants at enrolment and telephone interviews at 1 and 3 months. Structured nursing home chart reviews were completed at enrolment, 1 and 3 months. | n = 256 | Next of kins decisional conflict at 3 months, knowledge about dementia and feeding options, frequency of communication with health care providers, and use of feeding treatments. | Next of kins in both groups experienced the same level of decisional conflict at the time of study enrollment. After 3 months next of kins who received the decision aid had significantly lower (better) scores on the Decisional Conflict Scale than surrogates receiving usual care (1.65 vs. 1.97, p < 0.001), and lower scores on each subscale. Examining within-group change, both groups of next of kins experienced reduced decisional conflict over 3-month follow-up. However, those in the intervention arm had a significantly greater reduction of decisional conflicts (p < 0.001). |
| Park et al., 2015 [36] Korea | To examine the effect of an evidence-based nursing care algorithm | Control intervention study.Inclusion criteria were ≥65 years, living on the same floor, remained min. 6 months in the nursing home and oral intake, dysphagia (Gugging Swallowing Screen). A control period of 6 months was followed by an algorithm period of 6 months. Intervention: nursing care algorithm consisting of (1) screening for dysphagia, (2) grouping by the degree of dysphagia risk, and (3) nursing care for each group (checking for OD signs, positioning, instructing in exercises, oral hygiene, meal assisting and modified diet) | n = 40 | Dysphagia-related quality of life and risk of aspiration | Improvement of dysphagia-related quality of life and reducing the risk of aspiration |
| Benigas, J et al., 2016 [37] USA | Determine the effect of teaching persons with dementia to use compensatory swallowing strategies paired with an external memory aid. | Pilot study. Inclusion criteria: dementia and dysphagia (FEES). 65 to 99 years, sixth grade or higher level of education, ability to sit at 90° during the sessions, agreement to eat in a quiet environment when working with the investigator, be a verbal communicator. Exclusion criteria: diagnosis of psychiatric illness. Intervention: 30- to 45-min treatment sessions five times weekly in a quiet room, and compensatory strategies were trained using a yellow card with the responses printed. | n = 5 | The response was considered correct only if all the responses were performed in the correct order. | The use of a visual aid was functionally related to improvements in 2–3 compensatory swallowing behaviors for each of the 5 participants. |
| Chen L L et al., 2016 [38] China | Investigate the effects of an optimal feeding intervention in nursing home residents with Alzheimer’s disease and dysphagia. | Prospective cohort study. Inclusion criteria >60 years, dementia, gagging, dysphagia (Kubota water swallow test), able to take food. Exclusion criteria: severe liver, kidney, or blood diseases, other diseases that may have affected swallowing function, dependent on gastric tube or feeding tube for nutrition or unstable vital signs. Intervention: The residents were prepared for the meal; surroundings were optimized in a three-month period. Observations and assessments of the patients were performed pre- and post-intervention | n = 30 | Swallowing function measured with the Kubota water swallow test, type and amount of food intake, and nutritional status. | Patients’ eating/feeding abilities improved overall, including significantly increased food intake (p < 0.001), improvement in the Kubota water swallow test (p < 0.001) and significant improvements in skinfold thickness, arm circumference, serum albumin and hemoglobin (all p < 0.01), indicating improved nutritional status. Among 22 patients who initially required assisted feeding, 5 patients resumed self-feeding after the intervention (p = 0.06). |
| Hollaar, V et al., 2017 [39] Netherlands | Assessing the effect of a 0.05% chlorhexidine-containing solution in addition to daily oral hygiene care. | Controlled clinical trial. 17 nursing homes. Inclusion criteria: ≥65 years, physically disabled, dysphagia (assessed by a speech therapist). Exclusion criteria: cognitively impaired, vegetative state, terminally ill, dependent on mechanical ventilation or using an additional oral hygiene care solution. Intervention: for 1 year, participants in the intervention group received the usual oral hygiene care with the addition of a 0.05% chlorhexidine oral rinse solution, and participants in the control group received only oral hygiene care. | n = 103 | Episodes of pneumonia | Survival analysis showed no significant difference in the incidence of pneumonia between both groups. After adjustment for group and FOIS-level, regression analysis showed that the variables age, gender, CDS score, number of diseases, medication use, number of teeth, and the presence of dental implants or removable dentures were not significantly associated with the incidence of pneumonia. |
| Jablonski R A et al., 2017 [40] USA | Determine the safety of a mouth care protocol for nursing home care residents with dysphagia and no access to suction equipment. | Feasibility study. Inclusion criteria were nursing home residents, ≥65 years, dysphagia (diagnosis of dysphagia in medical record), dementia, dependent on others for mouth care and having min. two teeth. The oral health assessment tool, the Katz index of independence of activity in daily living, and the global deterioration scale was used to collect information. Intervention: mouth care was provided twice daily for 5 days and once for day 6. | n = 4 | Microbe abundance | The mouth care protocol resulted in improved oral hygiene without aspiration. |
| Zanini, M et al., 2017 [41] Italy | Assess changes in daily food intake following the introduction of meals with modified textures and an adequate content of proteins, calories, balanced nutritional and bromatological properties. | Intervention study in 20 nursing homes. Inclusion criteria: nursing home residents ≥ 65 years, CIRS-score < 6 and diagnosed with dysphagia (diagnosis of dysphagia in medical record). Exclusion criteria: clinical instability, terminally ill, chronic or cancer diseases, severe dysphagia, DOSS ≥ 2 or tube feeding. Intervention: meals without nutritional supplementation, but with personalised levels of density, viscosity, texture. | n = 479 | Nutritional status (anthropometric parameters, plasmatic biochemical nutritional parameters, and nutritional screening tools) | The total mean BMI of the sample increased from 17.88 to 19.00; body weight averagely improved by 7.19%. There was a progressive improvement of total protein and serum albumin values. No side effects were reported. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melgaard, D.; Westergren, A.; Skrubbeltrang, C.; Smithard, D. Interventions for Nursing Home Residents with Dysphagia—A Scoping Review. Geriatrics 2021, 6, 55. https://doi.org/10.3390/geriatrics6020055
Melgaard D, Westergren A, Skrubbeltrang C, Smithard D. Interventions for Nursing Home Residents with Dysphagia—A Scoping Review. Geriatrics. 2021; 6(2):55. https://doi.org/10.3390/geriatrics6020055
Chicago/Turabian StyleMelgaard, Dorte, Albert Westergren, Conni Skrubbeltrang, and David Smithard. 2021. "Interventions for Nursing Home Residents with Dysphagia—A Scoping Review" Geriatrics 6, no. 2: 55. https://doi.org/10.3390/geriatrics6020055
APA StyleMelgaard, D., Westergren, A., Skrubbeltrang, C., & Smithard, D. (2021). Interventions for Nursing Home Residents with Dysphagia—A Scoping Review. Geriatrics, 6(2), 55. https://doi.org/10.3390/geriatrics6020055