Effectiveness of the “Mente Sana [Healthy Mind]” Cognitive Training Program for Older Illiterate Adults with Mild Cognitive Impairment


Abstract
1. Introduction
Background
2. Materials and Methods
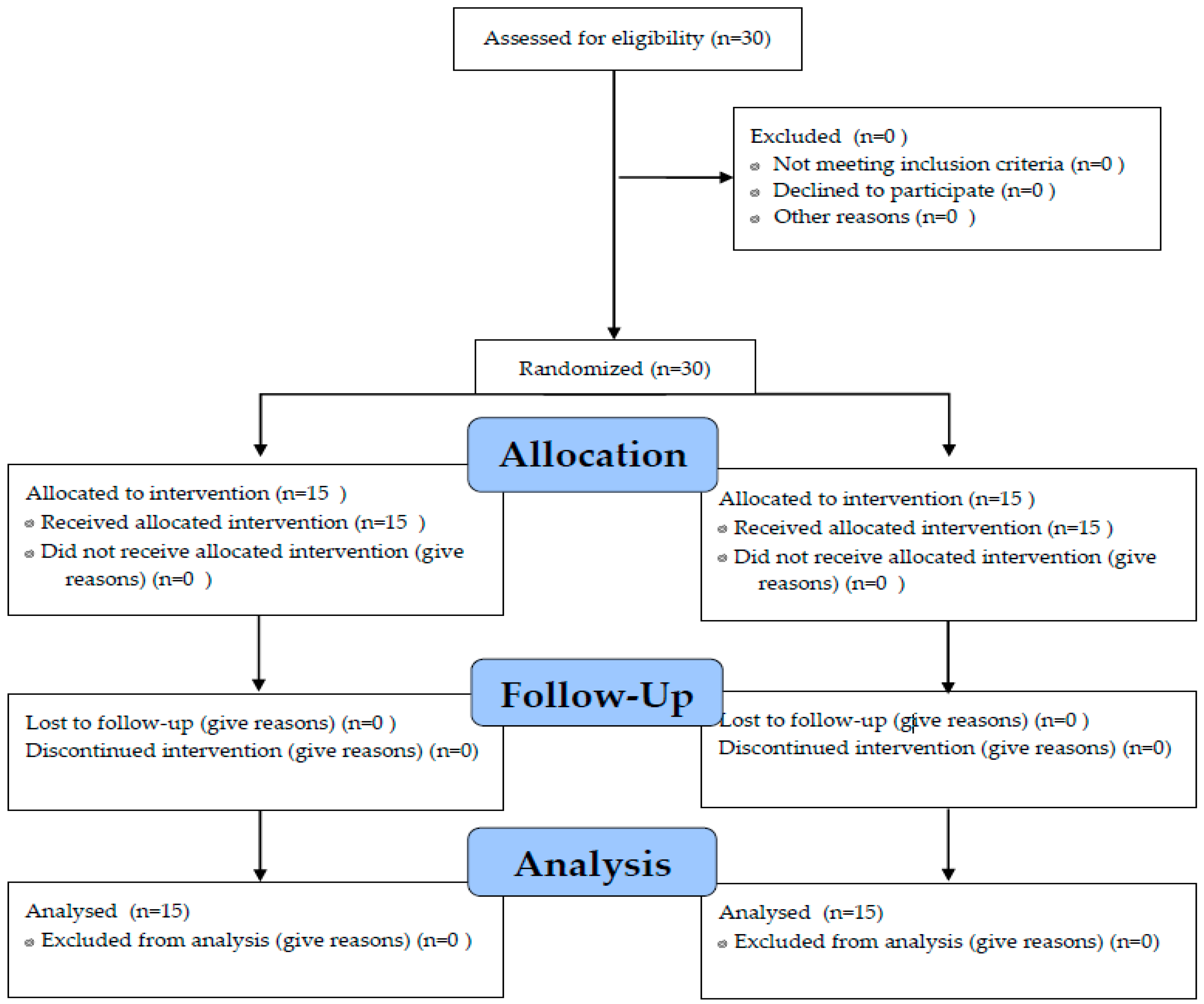
2.1. Participants
2.2. Instruments
2.2.1. Cognitive Impairment
2.2.2. “MENTE SANA [HEALTHY MIND]” Cognitive Training Manual
2.2.3. Procedures
2.3. Method and Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Varela, L.; Chávez, H.; Gálvez, M.; Méndez, F. Cognitive impairment characteristics in the hospitalized Peruvian elderly adults. Rev. Soc. Per. Med. Inter. 2004, 17, 37–42. Available online: http://sisbib.unmsm.edu.pe/bvrevistas/spmi/v17n2/pdf/a02.pdf (accessed on 12 August 2019).
- Abarca, J.C.; Chino, B.N.; Llacho, M.L.V.; Gonzáles, K.; Mucho, K.; Vázquez, R.; Cardens, C.; Soto, M.F. Relationship between education, aging and cognitive decline in a sample of older adults Arequipa. Rev. Chil. Neuropsicol. 2008, 8, 1–9. Available online: https://dialnet.unirioja.es/servlet/articulo?codigo=3987691 (accessed on 12 August 2019).
- Li, H.; Li, J.; Li, B.; Wang, P.; Zhou, T. Cognitive intervention for persons with mild cognitive impairment: A meta-analysis. Ageing Res. Rev. 2011, 10, 285–296. [Google Scholar] [CrossRef]
- Ajmani, R.S.; Metter, E.J.; Jaykumar, R.; Ingram, D.K.; Spangler, E.L.; Abugo, O.O.; Rifkind, J.M. Hemodynamic changes during aging associated with cerebral blood flow and impaired cognitive function. Neurobiol. Aging 2000, 21, 257–269. [Google Scholar] [CrossRef]
- Navarro, E.; Calero, M.D. Cognitive Plasticity in Young-Old Adults and Old-Old adults and Its Relationship with Successful Aging. Geriatrics 2018, 3, 14. [Google Scholar] [CrossRef]
- Franco, M.; Criado, C. Theoretical Considerations in the Study of Alzheimer’s, Psychotherapeutic intervention in Alzheimer’s Disease Patients with Mild Deterioration, 1st ed.; Ministry of Labor and Social Affairs; General Secretariat for Social Affairs; Institute of Migrations and Social Services (IMSERSO): Madrid, Spain, 2002; Volume 9, p. 9. [Google Scholar]
- Calero, M.D.; Navarro, E. Efficacy of a memory training program in maintaining the elderly with and without cognitive impairment. Clin. Health 2006, 17, 187–202. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1130-52742006000200004&lng=es&nrm=iso (accessed on 10 September 2019).
- Zehnder, F.; Martin, M.; Altgassen, M.; Clare, C. Memory training effects in old age as markers of plasticity: A meta-analysis. Restor. Neurol. Neurosci. 2009, 27, 507–520. [Google Scholar] [CrossRef]
- Bayarre, H.; Fente, A.; Gras, O.; Menéndez, J. Prevalence of mental disability in the elderly of the Playa 1996 Municipality (Part II). Cuba. J. Public Health 1999, 25, 30–38. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34661999000100004&lng=es (accessed on 10 September 2019).
- Camargo-Hernández, K.; Laguado-Jaimes, E. Degree of cognitive impairment of older adults institutionalized in two homes for the elderly in the metropolitan area of Bucaramanga-Santander, Colombia. Rev. Univ. Health 2017, 19, 163–170. Available online: https://revistas.udenar.edu.co/index.php/usalud/article/view/2974 (accessed on 11 September 2019). [CrossRef]
- Peng, Z.; Jiang, H.; Wang, X.; Huang, K.; Zuo, Y.; Wu, X.; Abdullah, A.; Yang, L. The Efficacy of Cognitive Training for Elderly Chinese Individuals with Mild Cognitive Impairment. BioMed Res. Int. 2019, 2019, 10. [Google Scholar] [CrossRef]
- Ardila, A.; Bertolucci, P.; Braga, L.; Castro-Caldas, A.; Judd, T.; Kosmidis, M.; Matute, E.; Nitrini, R.; Ostrosky-Solis, F.; Rosselli, M. Illiteracy: The Neuropsychology of Cognition Without Reading. Arch. Clin. Neuropsychol. 2010, 25, 689–712. [Google Scholar] [CrossRef] [PubMed]
- Organisation Des Nations Unies Pour L’education, La Science Et La Culture. 2019. Available online: https://es.unesco.org/themes/alfabetizacion (accessed on 11 September 2019).
- Calero, M.D.; Garcia-Berbén, T.M. A self-training program in inductive reasoning for low-education elderly: Tutor-guided training vs. self-training. Arch. Gerontol. Geriatr. 1997, 24, 249–259. [Google Scholar] [CrossRef]
- Tak, S.H.; Kim, J.; Ko, H.; Yoo, Y.M. Feasibility of an Integrative Activity Program for Older Adults with Low Education and Mild Dementia. J. Gerontol. Nurs. 2019, 45, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Pedraza, O.L.; Salazar, A.M.; Sierra, F.A.; Soler, D.; Castro, J.; Castillo, P.; Hernández, A.; Piñeros, C. Reliability, criterion and discriminant validity of the Montreal Cognitive Assessment Test (MoCA) in a group of adults from Bogotá. Acta Med. Colomb. 2016, 40, 221–228. Available online: http://www.scielo.org.co/pdf/amc/v41n4/v41n4a04.pdf (accessed on 8 October 2019).
- Lozano, M.; Hernández, M.; Turró, O.; Pericot, I.; López-Pousa, S.; Vilalta, J. Validación del Montreal Cognitive Assessment (MoCa): Test de cribado para el deterioro cognitivo leve. Datos preliminares. Alzheimer. Real Invest Demenc 2009, 43, 4–11. [Google Scholar]
- Hernández, R.; Fernández, C.; Baptista, M. Metodología de la Investigación, 6th ed.; McGraw-Hill/Interamericana Editores, S.A. de C.V.: Mexico City, Mexico, 2014; ISBN 978-1-4562-2396-0. [Google Scholar]
- Smart, C.M.; Karr, J.E.; Areshenkoff, C.N.; Rabin, L.A.; Hudon, C.; Gates, N.; Hampel, H. Non-pharmacologic interventions for older adults with subjective cognitive decline: Systematic review, meta-analysis, and preliminary recommendations. Neuropsychol. Rev. 2017, 27, 245–257. [Google Scholar] [CrossRef]
- Hill, R.; Wahlin, A.; Winblad, B.; Bäckman, L. The role of demographic and lifestyle variables in utilizing cognitive support for episodic remembering in very old adults. J. Gerontol. 1995, 50, 219–227. [Google Scholar] [CrossRef]
- Calero, D.; Navarro, E. Differences in cognitive performance, level of dependency and quality of life (QoL) related to age and cognitive status in a simple of Spanish old adults under and over 80 years of age. Arch. Gerontol. Geriatr. 2011, 53, 292–297. [Google Scholar] [CrossRef]
- Fan, B.; Wong, R. Effect of Cognitive Training on Daily Function in Older People without Major Neurocognitive Disorder: A Systematic Review. Geriatría 2019, 4, 44. [Google Scholar] [CrossRef]
- Gavelin, H.M.; Lampit, A.; Hallock, H.; Sabates, J.; Bahar-Fuchs, A. Cognition-Oriented Treatments for Older Adults: A Systematic Overview of Systematic Reviews. Neuropsychol. Rev. 2020, 87, 697–707. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control G. | Treatment G | ||||
|---|---|---|---|---|---|
| n = 15 | n = 15 | INTRAGROUP DIF. | INTERGROUPDIF. | ||
| PRETESTMOCA | GROUP | ||||
| M | 18.60 | 17.26 | F = 14.641 ** | F = 20.52 ** | |
| S.D. | 1.24 | 1.66 | ETA = 0.343 | ETA = 0.989 | |
| RANGE | 17–21 | 17–21 | p = 0.958 | p = 1.000 | |
| POSTESTMOCA | INTERACTION MOMENT x GROUP | ||||
| M | 19.00 | 23.87 | F = 45.08 ** | ||
| S.D. | 1.33 | 4.32 | ETA = 0.617 | ||
| RANGE | 15–20 | 19–29 | p = 1.000 |
| Group | Mean | Standard Deviation | t | p | |
|---|---|---|---|---|---|
| Visuo-Spatial/Executive | Control | 2.4667 | 0.63994 | 4.56 | 0.001 |
| Treatment | 4.0000 | 1.13389 | |||
| Identification | Control | 1.8667 | 0.74322 | 3.15 | 0.004 |
| Treatment | 2.6000 | 0.50709 | |||
| Attention | Control | 1.4667 | 0.51640 | ||
| Treatment | 3.1333 | 1.55226 | 3.94 | 0.001 | |
| Language | Control | 1.2667 | 0.59362 | ||
| Treatment | 2.8000 | 0.41404 | 8.20 | 0.0001 | |
| Abstraction | Control | 1.5333 | 0.63994 | ||
| Treatment | 1.8667 | 0.35187 | |||
| Deferred Memory Recall | Control | 3.4667 | 0.63994 | ||
| Treatment | 3.7333 | 1.09978 | |||
| Orientation | Control | 5.2000 | 0.67612 | ||
| Treatment | 5.7333 | 0.45774 | 2.53 | 0.018 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palo Villegas, Y.d.R.; Pomareda Vera, A.E.; Rojas Zegarra, M.E.; Calero, M.D. Effectiveness of the “Mente Sana [Healthy Mind]” Cognitive Training Program for Older Illiterate Adults with Mild Cognitive Impairment. Geriatrics 2020, 5, 34. https://doi.org/10.3390/geriatrics5020034
Palo Villegas YdR, Pomareda Vera AE, Rojas Zegarra ME, Calero MD. Effectiveness of the “Mente Sana [Healthy Mind]” Cognitive Training Program for Older Illiterate Adults with Mild Cognitive Impairment. Geriatrics. 2020; 5(2):34. https://doi.org/10.3390/geriatrics5020034
Chicago/Turabian StylePalo Villegas, Yaneth del Rosario, Andrea Elena Pomareda Vera, María Elena Rojas Zegarra, and M. Dolores Calero. 2020. "Effectiveness of the “Mente Sana [Healthy Mind]” Cognitive Training Program for Older Illiterate Adults with Mild Cognitive Impairment" Geriatrics 5, no. 2: 34. https://doi.org/10.3390/geriatrics5020034
APA StylePalo Villegas, Y. d. R., Pomareda Vera, A. E., Rojas Zegarra, M. E., & Calero, M. D. (2020). Effectiveness of the “Mente Sana [Healthy Mind]” Cognitive Training Program for Older Illiterate Adults with Mild Cognitive Impairment. Geriatrics, 5(2), 34. https://doi.org/10.3390/geriatrics5020034