Inadequacy of Protein Intake in Older UK Adults

 ,
,  , , and
, , and 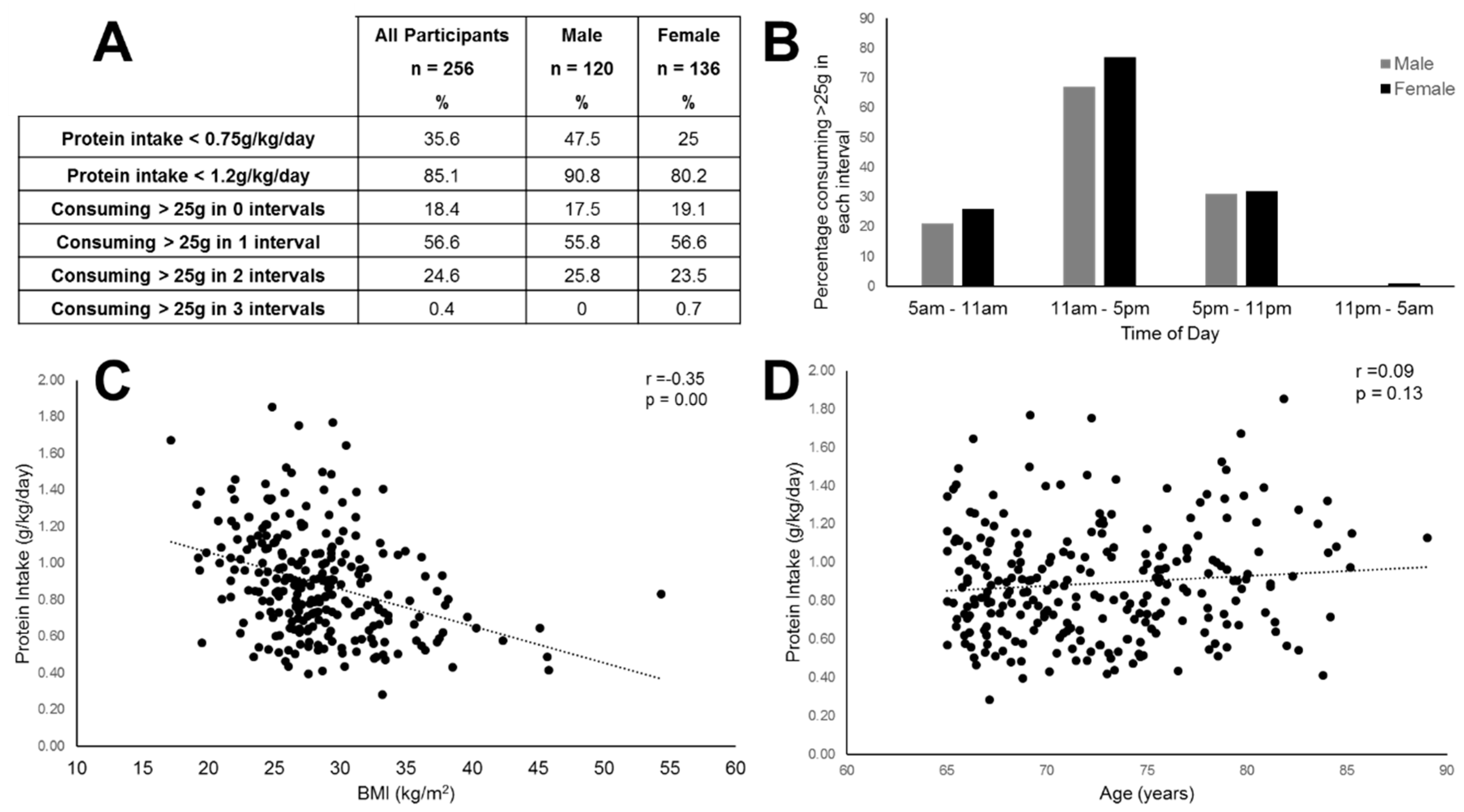{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organisation. World Rep. Ageing Health; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Newman, A.B.; Kupelian, V.; Visser, M.; Simonsick, E.M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Rubion, S.M.; Harris, T.B. Strength but not muscle mass is assoicated with mortality in the Health, Aging and Body composition study cohort. J. Gerontol A Biol. Sci. Med. 2006, 61, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Campbell, W.W.; Jacques, P.F.; Kritchevsky, S.B.; Moore, L.L.; Rodriguez, N.R.; van Loon, L.J. Protein and Healthy Aging. Am. J. Clin. Nutr. 2015, 101, 1339S–1345S. [Google Scholar] [CrossRef] [PubMed]
- Volpi, E.; Campbell, W.W.; Dwyer, J.T.; Johnson, M.A.; Jensen, G.L.; Morley, J.E.; Wolfe, R.R. Is the Optimal Level of Protein Intake for Older Adults Greater than the Recommended Dietary Allowance. J. Gerontol A Biol. Sci. Med. Sci. 2013, 68, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for Optimal Dietary Protein in Older People: A Position Paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef] [PubMed]
- Department of Health Panel on Dietary Reference Values. Dietary Reference values for food and energy for the UK; HMSO: London, UK, 1991; p. 24.
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. National Diet. and Nutrition Survey Results from Years 7 and 8 (combined) of the rolling programme (2014/2015) to (2015/2016); PHE Publications: London, UK, 2018.
- Lonnie, M.; Hooker, E.; Brunstrom, J.M.; Corfe, B.M.; Green, M.A.; Watson, A.W.; Williams, E.A.; Stevenson, E.J.; Penson, S.; Johnstone, A.M. Protein for Life: Review of Optimal Protein Intake, Sustainable Dietary Sources and the Effect on Appetite in Ageing Adults. Nutrients 2018, 103, 360. [Google Scholar] [CrossRef] [PubMed]
- Astell, A.J.; Hwang, F.; Brown, L.J.; Timon, C.; Maclean, L.M.; Smith, T.; Adlam, T.; Khadra, H.; Williams, E.A. Validation of the NANA (Novel Assessment of Nutrition and Aging) touch screen system for use at home by older adults. Exp. Gerontol 2014, 60, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Forster, S.E.; Powers, H.J.; Foulds, G.A.; Flower, D.J.; Hopkinson, K.; Parker, S.G.; Young, T.A.; Saxton, J.; Pockley, A.G.; Williams, E.A. Improvement in Nutritional Status reduces the clinical impact of infections in older adults. J. Am. Ger. Soc. 2012, 60, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Franssen, R.; Dullemeijer, C.; van Dronkelaar, C.; Kyung, K.H.; Ispoglou, T.; Zhu, K.; Prince, R.L.; van Loon, L.J.C.; de Groot, L.C.P.G.M. The Impact of Dietary Protein or Amino Acid Supplementation on Muscle Mass and Strength in Elderly People: Individual Participant data and Meta-Analysis of RCT’s. J. Nutr. Health Aging 2017, 21, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Jyväkorpi, S.K.; Pitkälä, K.H.; Puranen, T.M.; Björkman, M.P.; Kautiainen, H.; Strandberg, T.E.; Soini, H.H.; Suominen, M.H. High Proportions of older people with normal nutritional status have low protein intake and low diet quality. Arch. Gerontol Geriatr. 2016, 67, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Molino, S.; Dossena, M.; Buonocore, D.; Verri, M. Sarcopenic Obesity: An Appriasal of the Current Status of Knowledge and Management in Elderly People. J. Nutr Health Aging 2015, 20, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Berner, L.A.; Becker, G.; Wise, M.; Doi, J. Characterization of Dietary Protein among Older Adults in the United States, Amount, Animal Sources, and Meal Patterns. J. Acad Nutr Diet. 2013, 113, 809–815. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morris, S.; Cater, J.D.; Green, M.A.; Johnstone, A.M.; Brunstrom, J.M.; Stevenson, E.J.; Williams, E.A.; Corfe, B.M. Inadequacy of Protein Intake in Older UK Adults. Geriatrics 2020, 5, 6. https://doi.org/10.3390/geriatrics5010006
Morris S, Cater JD, Green MA, Johnstone AM, Brunstrom JM, Stevenson EJ, Williams EA, Corfe BM. Inadequacy of Protein Intake in Older UK Adults. Geriatrics. 2020; 5(1):6. https://doi.org/10.3390/geriatrics5010006
Chicago/Turabian StyleMorris, Susan, James D. Cater, Mark A. Green, Alexandra M. Johnstone, Jeffrey M. Brunstrom, Emma J. Stevenson, Elizabeth A. Williams, and Bernard M. Corfe. 2020. "Inadequacy of Protein Intake in Older UK Adults" Geriatrics 5, no. 1: 6. https://doi.org/10.3390/geriatrics5010006
APA StyleMorris, S., Cater, J. D., Green, M. A., Johnstone, A. M., Brunstrom, J. M., Stevenson, E. J., Williams, E. A., & Corfe, B. M. (2020). Inadequacy of Protein Intake in Older UK Adults. Geriatrics, 5(1), 6. https://doi.org/10.3390/geriatrics5010006