Natural History of Swallow Function during the Three-Month Period after Stroke

 , and
, and 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Population
2.2. Data Collected
2.3. Clinical Assessment
2.4. Data Analysis and Statistical Methods
3. Results
3.1. Study Population
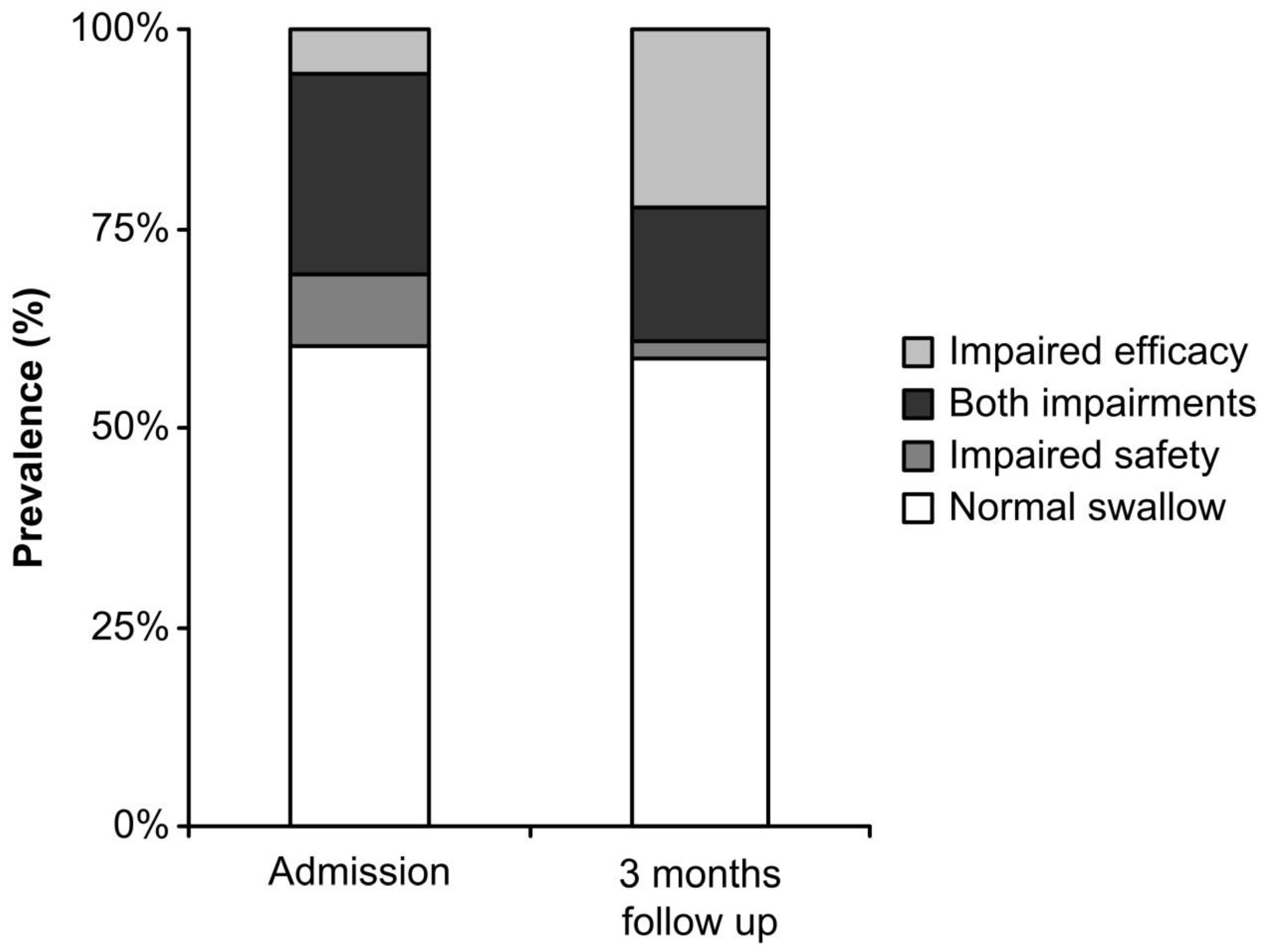
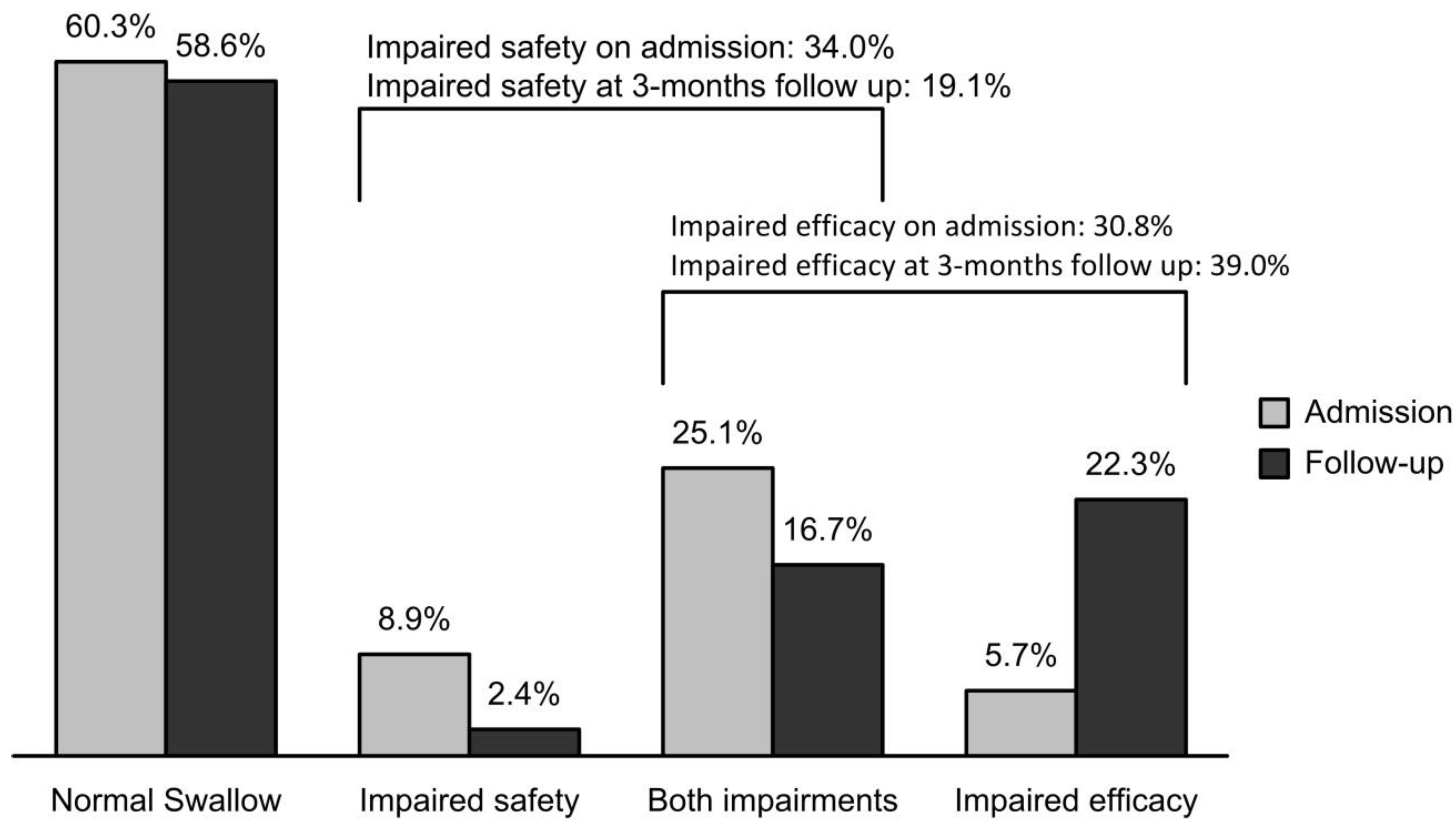
3.2. Prevalence of OD: Admission and the 3-Month Follow-Up
3.3. Factors Associated with the Recovery of Impaired Safety of Swallow
3.4. Factors Associated with the Recovery of Efficacy of Swallow
3.5. Factors Associated with the Worsening of Swallowing Function During Follow up
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Attrill, S.; White, S.; Murray, J.; Hammond, S.; Doeltgen, S. Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review. BMC Health Serv. Res. 2018, 18, 594. [Google Scholar]
- Rofes, L.; Muriana, D.; Palomeras, E.; Vilardell, N.; Palomera, E.; Alvarez-Berdugo, D.; Casado, V.; Clavé, P. Prevalence, risk factors and complications of oropharyngeal dysphagia in stroke patients: A cohort study. Neurogastroenterol. Motil. 2018, 30, e13338. [Google Scholar]
- Vilardell, N.; Rofes, L.; Nascimento, W.V.; Muriana, D.; Palomeras, E.; Clavé, P. Cough reflex attenuation and swallowing dysfunction in sub-acute post-stroke patients: Prevalence, risk factors, and clinical outcome. Neurogastroenterol. Motil. 2017, 29, e12910. [Google Scholar]
- Smithard, D.G.; O’Neill, P.A.; England, R.E.; Park, C.L.; Wyatt, R.; Martin, D.F.; Morris, J. The Natural History of Dysphagia following a Stroke. Dysphagia 1997, 12, 188–193. [Google Scholar]
- Teismann, I.K.; Suntrup, S.; Warnecke, T.; Steinsträter, O.; Fischer, M.; Flöel, A.; Ringelstein, E.B.; Pantev, C.; Dziewas, R. Cortical swallowing processing in early subacute stroke. BMC Neurol. 2011, 11, 34. [Google Scholar]
- Hamdy, S.; Aziz, Q.; Rothwell, J.; Power, M.; Singh, K.; Nicholson, D.; Tallis, R.; Thompson, D.G. Recovery of swallowing after dysphagic stroke relates to functional reorganization in the intact motor cortex. Gastroenterology 1998, 115, 1104–1112. [Google Scholar]
- Singh, S.; Hamdy, S. Dysphagia in stroke patients. Postgrad. Med. J. 2006, 82, 383–391. [Google Scholar]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Muriana, D.; Palomeras, E.; Michou, E.; Clavé, P.; et al. Neurophysiological and Biomechanical Evaluation of the Mechanisms Which Impair Safety of Swallow in Chronic Post-stroke Patients. Transl. Stroke Res. 2019. [Google Scholar] [CrossRef]
- Muriana, D.; Rofes, L.; Sanchez, D.; Palomeras, E.; Vilardell, N.; Palomera, E.; Álvarez-Berdugo, D.; Casado, D.; Clave, P. Incidence, risk factors and early complications of post-stroke oropharyngeal dysphagia. In Proceedings of the 5th Congress of European Society for Swallowing Disorders, Barcelona, Spain, 2–3 October 2015. [Google Scholar]
- Smithard, D.G.; Smeeton, N.C.; Wolfe, C.D. Long-term outcome after stroke: Does dysphagia matter? Age Ageing 2007, 36, 90–94. [Google Scholar]
- Clavé, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar]
- Goldstein, L.B.; Bertels, C.; Davis, J.N. Interrater Reliability of the NIH Stroke Scale. Arch. Neurol. 1989, 46, 660–662. [Google Scholar]
- Bamford, J.; Sandercock, P.; Dennis, M.; Warlow, C.; Burn, J. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 1991, 337, 1521–1526. [Google Scholar]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Bonita, R.; Beaglehole, R. Modification of Rankin Scale: Recovery of motor function after stroke. Stroke 1988, 19, 1497–1500. [Google Scholar]
- Kaiser, M.J.; MNA-International Group; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; et al. Validation of the Mini Nutritional Assessment short-form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar]
- Group, T.E. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Rofes, L.; Arreola, V.; Clavé, P. The volume-viscosity swallow test for clinical screening of dysphagia and aspiration. Nestle. Nutr. Inst. Workshop Ser. 2012, 72, 33–42. [Google Scholar]
- Rofes, L.; Arreola, V.; Mukherjee, R.; Clavé, P. Sensitivity and specificity of the Eating Assessment Tool and the Volume-Viscosity Swallow Test for clinical evaluation of oropharyngeal dysphagia. Neurogastroenterol. Motil. 2014, 26, 1256–1265. [Google Scholar]
- Martino, R.; Silver, F.; Teasell, R.; Bayley, M.; Nicholson, G.; Streiner, D.L.; Diamant, N.E. The Toronto Bedside Swallowing Screening Test (TOR-BSST): Development and validation of a dysphagia screening tool for patients with stroke. Stroke 2009, 40, 555–561. [Google Scholar]
- Parker, C.; Power, M.; Hamdy, S.; Bowen, A.; Tyrrell, P.; Thompson, D.G. Awareness of Dysphagia by Patients Following Stroke Predicts Swallowing Performance. Dysphagia 2004, 19, 28–35. [Google Scholar]
- Barer, D.H. The natural history and functional consequences of dysphagia after hemispheric stroke. J. Neurol. Neurosurg. Psychiatry 1989, 52, 236–241. [Google Scholar]
- Hinds, N.P.; Wiles, C.M. Assessment of swallowing and referral to speech and language therapists in acute stroke. QJM Int. J. Med. 1998, 91, 829–835. [Google Scholar]
- Kidd, D.; Nesbitt, R.; MacMahon, J.; Lawson, J. Aspiration in acute stroke: A clinical study with videofluoroscopy. QJM Int. J. Med. 1993, 86, 825–829. [Google Scholar]
- Guillén-Solà, A.; Marco, E.; Martínez-Orfila, J.; Mejías, M.F.D.; Passalacqua, M.D.; Duarte, E.; Escalada, F. Usefulness of the volume-viscosity swallow test for screening dysphagia in subacute stroke patients in rehabilitation income. NeuroRehabilitation 2013, 33, 631–638. [Google Scholar]
- Mann, G.; Hankey, G.J.; Cameron, D. Swallowing function after stroke: Prognosis and prognostic factors at 6 months. Stroke 1999, 30, 744–748. [Google Scholar]
- Broadley, S.; Croser, D.; Cottrell, J.; Creevy, M.; Teo, E.; Yiu, D.; Pathi, R.; Taylor, J.; Thompson, P. Predictors of prolonged dysphagia following acute stroke. J. Clin. Neurosci. 2003, 10, 300–305. [Google Scholar]
- Maeshima, S.; Osawa, A.; Hayashi, T.; Tanahashi, N. Factors Associated with Prognosis of Eating and Swallowing Disability after Stroke: A Study from a Community-based Stroke Care System. J. Stroke Cerebrovasc. Dis. 2013, 22, 926–930. [Google Scholar]
- Nakayama, E.; Tohara, H.; Hino, T.; Sato, M.; Hiraba, H.; Abe, K.; Ueda, K. The effects of ADL on recovery of swallowing function in stroke patients after acute phase. J. Oral REHABIL. 2014, 41, 904–911. [Google Scholar]
- Odderson, I.R.; Keaton, J.C.; McKenna, B.S. Swallow management in patients on an acute stroke pathway: Quality is cost effective. Arch. Phys. Med. Rehabil. 1995, 76, 1130–1133. [Google Scholar]
- Falsetti, P.; Acciai, C.; Palilla, R.; Bosi, M.; Carpinteri, F.; Zingarelli, A.; Pedace, C.; Lenzi, L. Oropharyngeal Dysphagia after Stroke: Incidence, Diagnosis, and Clinical Predictors in Patients Admitted to a Neurorehabilitation Unit. J. Stroke Cerebrovasc. Dis. 2009, 18, 329–335. [Google Scholar]
- Baijens, L.W.; Clavé, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European Society for Swallowing Disorders – European Union Geriatric Medicine Society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar]
- Sporns, P.B.; Muhle, P.; Hanning, U.; Suntrup-Krueger, S.; Schwindt, W.; Eversmann, J.; Warnecke, T.; Wirth, R.; Zimmer, S.; Dziewas, R. Atrophy of Swallowing Muscles Is Associated With Severity of Dysphagia and Age in Patients With Acute Stroke. J. Am. Med. Dir. Assoc. 2017, 18, 635. [Google Scholar]
- Lango, M.N.; Egleston, B.; Fang, C.; Burtness, B.; Galloway, T.; Liu, J.; Mehar, R.; Ebersole, B.; Moran, K.; Ridge, J.A. Baseline health perceptions, dysphagia, and survival in patients with head and neck cancer. Cancer 2014, 120, 840–847. [Google Scholar]
- Terré, R.; Mearin, F. Resolution of Tracheal Aspiration After the Acute Phase of Stroke-Related Oropharyngeal Dysphagia. Am. J. Gastroenterol. 2009, 104, 923–932. [Google Scholar]
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. 2015, 34, 436–442. [Google Scholar]
- Takahata, H.; Tsutsumi, K.; Baba, H.; Nagata, I.; Yonekura, M. Early intervention to promote oral feeding in patients with intracerebral hemorrhage: A retrospective cohort study. BMC Neurol. 2011, 11, 6. [Google Scholar]
- Cabib, C.; Ortega, O.; Vilardell, N.; Mundet, L.; Clavé, P.; Rofes, L. Chronic post-stroke oropharyngeal dysphagia is associated with impaired cortical activation to pharyngeal sensory inputs. Eur. J. Neurol. 2017, 24, 1355–1362. [Google Scholar]



{kind=link}
{kind=link}
| Sample | 247 |
| Age (years) | 72.3 ± 11.9 |
| Sex (male) | 59.5% (147) |
| Previous heart disease | 25.5% (63) |
| NIHSS on admission (mean ± SD) Score ≤6 points (%) | 2(1–4) 87.0% (215) |
| Type of Stroke | |
| Ischemic Hemorrhagic Cerebral venous thrombosis | 95.5% (236) 4.1% (10) 0.4% (1) |
| Stroke Lateralization | |
| Left hemisphere Right hemisphere Bilateral Brain stem Not specified | 44.1% (109) 29.6% (73) 1.2% (3) 6.9% (17) 18.2% (45) |
| Territory Infarction | |
| MCA PCA AChA Watershed Basilar Vertebral | 64.3% (117) 14.8% (27) 8.2% (15) 2.2% (4) 8.8% (16) 1.6% (3) |
| Lesion Location | |
| Supratentorial Infratentorial | 89.6% (163) 10.4% (19) |
| Stroke Diagnosis | |
| PACI TACI POCI LACI Not specified | 41.3% (102) 6.1% (15) 15.8% (39) 32.4% (80) 4.4% (11) |
| Volume of stroke lesion (cc) | 11.8 ± 28.5 |
| Hospital length of stay (days) | 6.5 ± 3.5 |
| Institutionalization on discharge | 21.4% (52) |
| Barthel Index | |
| Pre-stroke event On discharge At follow-up visit | 100 (100–100) 100 (50–100) 100 (80–100) |
| Rankin Scale | |
| Pre-stroke event On discharge At follow-up visit | 0 (0–1) 2 (0–3) 2 (0–2) |
| MNA-sf at follow-up visit (mean ± SD) ≤11points | 13 (12–13) 30% (70) |
| EQ-5D-3L at Follow-Up Visit | |
| Mobility dysfunctions (%) Self-care dependency (%) Dependency in daily life activities (%) Pain/discomfort (%) Anxiety/depression symptoms (%) Perception of healthy status (mean ± SD) | 26.7% (63) 23.7% (56) 26.3% (62) 41.5% (98) 52.1% (123) 68.2 ± 19.2 |
| Factors | Recovery of Impaired Safety of Swallow at 3 Months | Maintained Impaired Safety of Swallow at 3 Months | OR (CI 95%); p-Value |
|---|---|---|---|
| Sample (n) | 36 | 49 | - |
| Age (mean ± SD) | 73.1 ± 11.2 | 78.6 ± 9.4 | 0.009 |
| Sex (male) (%) | 61.1 | 53.1 | 1.4 (0.6–3.3); 0.512 |
| No previous heart disease (%) | 86.1 | 61.2 | 3.9 (1.3–11.9); 0.015 |
| Pre-stroke Rankin score (median (IQ range)) | 0 (0–0) | 0 (0–1) | 0.061 |
| NIHSS on admission (median (IQ range)) | 4 (2–5) | 4 (1–7) | 0.890 |
| Score ≤6 points (%) | 83.3 | 75.5 | 2.2 (0.7–7.0); 0.188 |
| Stroke lateralization | |||
| Left hemisphere (%) Right hemisphere (%) | 62.1 37.9 | 65.0 32.5 | 0.8 (0.3–2.4); 0.806 1.3 (0.5–3.5); 0.798 |
| Territory infarction | |||
| MCA infarction (%) | 81.5 | 52.5 | 3.4 (1.0–10.8); 0.058 |
| Lesion location | |||
| Supratentorial (%) Infratentorial (%) | 88.9 11.1 | 81.1 18.9 | 1.9 (0.4–8.0); 0.498 |
| Stroke diagnosis | |||
| PACI (%) TACI (%) POCI (%) LACI (%) | 54.5 15.2 12.1 18.2 | 37.0 17.4 21.7 23.9 | 2.1 (0.8–5.1); 0.169 0.8 (0.3–2.9); 1.000 0.5 (0.1–1.7); 0.374 0.7 (0.2–2.2); 0.591 |
| Volume of stroke lesion (cc) (mean ± SD) | 21.2 ± 40.8 | 13.1 ± 23.0 | 0.305 |
| Institutionalization on discharge (%) | 30.6 | 40.2 | 0.6 (0.3–1.6); 0.490 |
| Barthel Index on discharge (median (IQ range)) | 70 (40–100) | 80 (40–100) | 0.864 |
| Barthel Index at follow-up visit (median (IQ range)) | 100 (80–100) | 70 (70–100) | 0.057 |
| Barthel ≥90 points (%) | 60.0 | 35.4 | 2.9 (1.2–7.3); 0.039 |
| MNA-sf at follow-up visit (median (IQ range)) | 11 (11–14) | 12 (11–14) | 0.668 |
| EQ-5D-3L: | |||
| Mobility dysfunctions (%) | 39.4 | 52.4 | 0.6 (0.2–1.5); 0.352 |
| Self-care dependency (%) | 42.4 | 40.5 | 1.1 (0.4–2.7); 1.000 |
| Dependency in daily life activities (%) | 36.3 | 52.4 | 0.5 (0.2–1.3); 0.243 |
| Pain/discomfort (%) | 54.5 | 52.4 | 1.1 (0.4–2.7); 1.000 |
| Anxiety/depression symptoms (%) | 51.5 | 64.3 | 0.6 (0.2–1.5); 0.346 |
| Perception of healthy status (mean ± SD) | 68.0 ± 19.7 | 67.4 ± 19.1 | 0.886 |
| Factors | Recovery of Efficacy of Swallow at 3 Months | Maintained Impaired Efficacy of Swallow at 3 Months | OR (CI 95%); p-Value |
|---|---|---|---|
| Sample (n) | 23 | 54 | - |
| Age (mean ± SD) | 75.1 ± 8.5 | 77.6 ± 10.1 | 0.106 |
| Sex (male) (%) | 60.9 | 55.5 | 1.2 (0.5–3.4); 0.803 |
| No previous heart disease (%) | 87.0 | 59.3 | 4.6 (1.2–17.3); 0.019 |
| Pre-stroke Rankin score (median (IQ range)) | 0 (0–2) | 0 (0–1) | 0.947 |
| NIHSS on admission (median (IQ range)) Score ≤6 points (%) | 2 (1–5) 86.9 | 3 (1–11) 74.1 | 0.205 3.3 (0.7–16.2); 0.207 |
| Stroke lateralization | |||
| Left hemisphere (%) Right hemisphere (%) | 60.0 40.0 | 61.3 36.4 | 0.9 (0.3–2.7); 1.000 1.2 (0.4–3.7); 0.788 |
| Territory infarction | |||
| MCA infarction (%) | 75.0 | 59.1 | 1.7 (0.5–5.7); 0.402 |
| Lesion location | |||
| Supratentorial (%) Infratentorial (%) | 95.0 5.0 | 85.4 14.6 | 3.3 (0.4–29.1); 0.410 |
| Stroke diagnosis | |||
| PACI (%) TACI (%) POCI (%) LACI (%) | 52.2 4.3 26.1 17.4 | 41.2 15.7 23.5 19.6 | 1.6 (0.6–4.2); 0.452 0.3 (0.0–2.3); 0.267 1.3 (0.4–4.1); 0.766 0.9 (0.3–3.5); 1.000 |
| Volume of stroke lesion (cc) (mean ± SD) | 26.0 ± 48.7 | 18.7 ± 36.2 | 0.990 |
| Institutionalization on discharge (%) | 21.7 | 40.7 | 0.126 |
| Barthel Index on discharge (median (IQ range)) | 90 (70-100) | 80 (50-90) | 0.441 |
| Barthel Index at follow-up visit (median (IQ range)) Barthel ≥90 points (%) | 90 (80–100) 54.5 | 90 (50–100) 43.3 | 0.210 1.6 (0.6–4.3); 0.450 |
| MNA-sf at follow-up visit (median (IQ range)) | 12 (10–14) | 12 (11–14) | 0.928 |
| EQ-5D-3L: | |||
| Mobility dysfunctions (%) | 45.5 | 46.0 | 0.9 (0.4–2.7); 1.000 |
| Self-care dependency (%) | 45.5 | 36.0 | 1.5 (0.5–4.1); 0.600 |
| Dependency in daily life activities (%) | 45.5 | 48.0 | 0.9 (0.3–2.5); 1.000 |
| Pain/discomfort (%) | 50.0 | 46.0 | 1.2 (0.4–3.2); 0.802 |
| Anxiety/depression symptoms (%) | 36.4 | 66.0 | 3.6 (1.3–10.3); 0.021 |
| Perception of healthy status (mean ± SD) | 63.8 ± 16.4 | 66.9 ± 19.3 | 0.523 |
| Factors | No Impaired Efficacy of Swallow at 3 Months | New Diagnosis of Impaired Efficacy of Swallow at 3 Months | OR (CI 95%); p-Value |
|---|---|---|---|
| Sample (n) | 126 | 44 | - |
| Age (mean ± SD) | 69.3 ± 12.8 | 72.8 ± 10.7 | 0.106 |
| Sex (male) (%) | 65.1 | 47.7 | 2.0 (1.0–4.1); 0.050 |
| No previous heart disease (%) | 78.6 | 75.0 | 0.8 (0.4–1.8); 0.676 |
| Pre-stroke Rankin score (median (IQ range)) | 0 (0–0) | 0 (0–0) | 0.045 |
| NIHSS on admission (median (IQ range)) Score ≤6 points (%) | 2 (1–3) 86.5 | 2 (1–3) 93.2 | 0.544 1.2 (0.3–4.9); 0.720 |
| Stroke lateralization | |||
| Left hemisphere (%) Right hemisphere (%) | 65.0 32.5 | 62.1 37.9 | 0.9 (0.4–2.0); 1.000 1.0 (0.5–2.2); 1.000 |
| Territory infarction | |||
| MCA infarction | 49.2 | 33.3 | 1.9 (0.9–4.0); 0.104 |
| Lesion location | |||
| Supratentorial (%) Infratentorial (%) | 85.3 14.7 | 76.5 23.5 | 1.8 (0.7–4.7); 0.289 |
| Stroke diagnosis | |||
| PACI (%) TACI (%) POCI (%) LACI (%) | 44.2 3.3 14.2 38.3 | 41.7 5.5 0 52.8 | 1.1 (0.5–2.4); 0.850 0.6 (0.1–3.3); 0.622 12.3 (0.7–210.6); 0.013 0.6 (0.3–1.2); 0.130 |
| Volume of stroke lesion (cc) (mean ± SD) | 6.9 ± 16.2 | 9.1 ± 27.3 | 0.367 |
| Institutionalization on discharge (%) | 11.3 | 25.0 | 2.6 (1.1–6.3); 0.046 |
| Barthel Index on discharge (median (IQ range)) | 90 (90–100) | 90 (80–100) | 0.046 |
| Barthel Index at follow-up visit (median (IQ range)) ≥90 points (%) | 100 (90–100) 82.8 | 100 (80–100) 65.2 | 0.004 9.0 (3.4–24.0); <0.001 |
| MNA-sf at follow-up visit (median (IQ range)) | 13 (12–14) | 12 (11–13) | 0.033 |
| EQ-5D-3L: | |||
| Mobility dysfunctions (%) | 14.2 | 30.9 | 2.7 (1.2–6.2); 0.021 |
| Self-care dependency (%) | 13.3 | 28.6 | 2.6 (1.1–6.1); 0.033 |
| Dependency in daily life activities (%) | 14.2 | 26.2 | 0.5 (0.2–1.1); 0.096 |
| Pain/discomfort (%) | 33.3 | 54.8 | 2.4 (1.2–5.0); 0.017 |
| Anxiety/depression symptoms (%) | 46.7 | 62.0 | 0.5 (0.3–1.1); 0.108 |
| Perception of healthy status (mean ± SD) | 72.8 ± 16.8 | 60.0 ± 21.0 | < 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arreola, V.; Vilardell, N.; Ortega, O.; Rofes, L.; Muriana, D.; Palomeras, E.; Álvarez-Berdugo, D.; Clavé, P. Natural History of Swallow Function during the Three-Month Period after Stroke. Geriatrics 2019, 4, 42. https://doi.org/10.3390/geriatrics4030042
Arreola V, Vilardell N, Ortega O, Rofes L, Muriana D, Palomeras E, Álvarez-Berdugo D, Clavé P. Natural History of Swallow Function during the Three-Month Period after Stroke. Geriatrics. 2019; 4(3):42. https://doi.org/10.3390/geriatrics4030042
Chicago/Turabian StyleArreola, Viridiana, Natàlia Vilardell, Omar Ortega, Laia Rofes, Desiree Muriana, Ernest Palomeras, Daniel Álvarez-Berdugo, and Pere Clavé. 2019. "Natural History of Swallow Function during the Three-Month Period after Stroke" Geriatrics 4, no. 3: 42. https://doi.org/10.3390/geriatrics4030042
APA StyleArreola, V., Vilardell, N., Ortega, O., Rofes, L., Muriana, D., Palomeras, E., Álvarez-Berdugo, D., & Clavé, P. (2019). Natural History of Swallow Function during the Three-Month Period after Stroke. Geriatrics, 4(3), 42. https://doi.org/10.3390/geriatrics4030042