Use of Reaction Force to Evaluate Older Adults’ Gait Patterns While Using a Walker to Walk

Abstract
1. Introduction
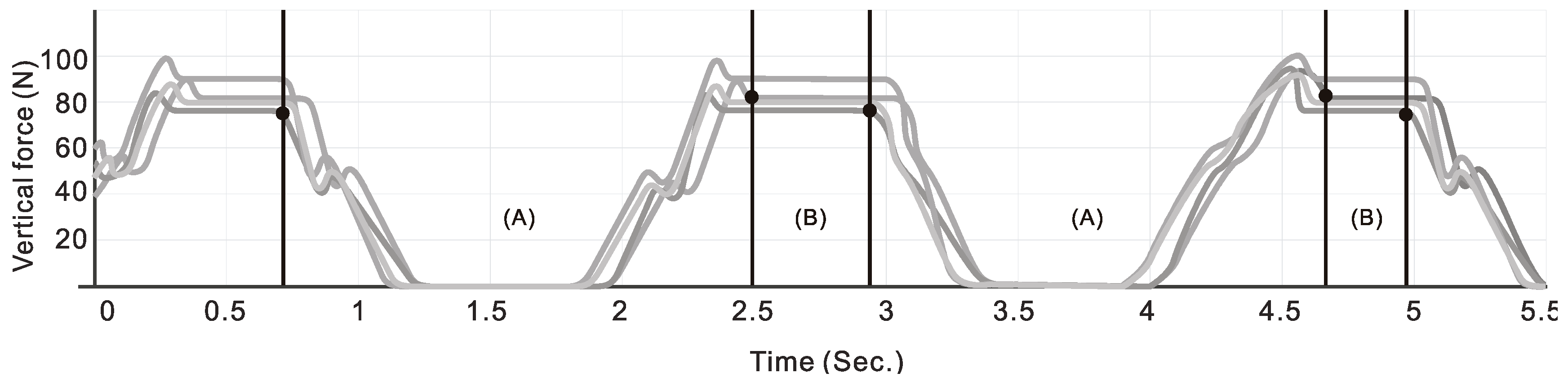
- Decomposing the gait into stance, swing phases, and support force by reaction;
- Whether there are significant differences between two steps in stance, swing phases, and support force while using a walker;
- Whether there are significant differences between two steps in stance, swing phases, and support force between BBS groups while using a walker.
2. Methods
2.1. Participants
2.2. Experimental Walker
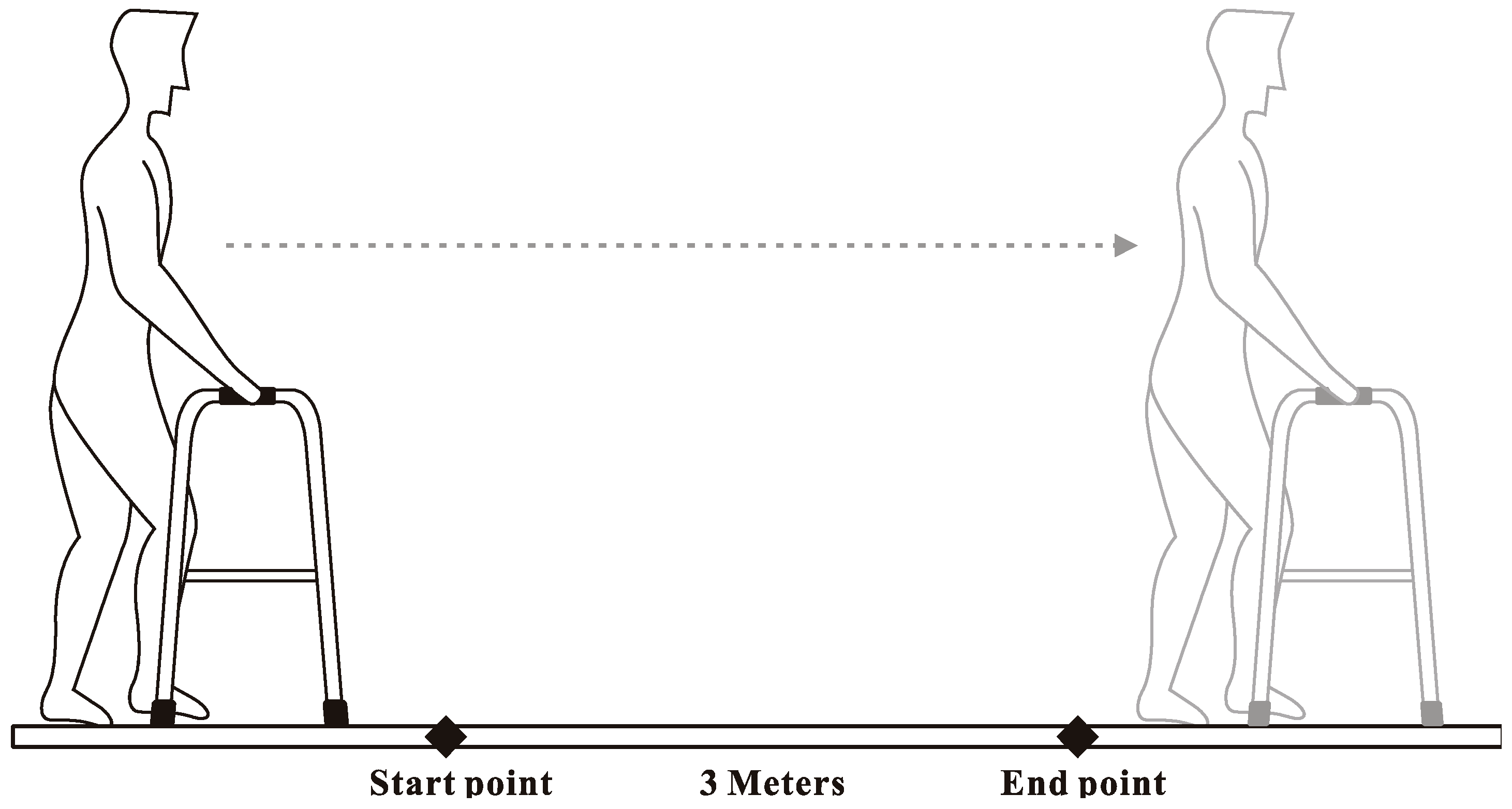
2.3. Task Specification
2.4. Data Analysis
3. Results
4. Discussion
- Stabilization of the gait by stance and swing phases of the walking aid while walking;
- Even if the user can walk stably, the body function can be evaluated by the support force.
Funding
Acknowledgments
Conflicts of Interest
References
- Shurr, D.G.; Cook, T.M. Prosthetic and Orthotics; Appleton and Lange: New York, NY, USA, 1990; p. 225. [Google Scholar]
- Vaughan, C.L.; Davis, B.L.; O’Connor, J.C. Dynamics of Human Gait; Kiboho Publishers: Kape Town, South Africa, 1999; pp. 63–76. [Google Scholar]
- Peat, M.; Dubo, H.I.C.; Winter, D.A.; Quanbury, A.O.; Steinke, T.; Grahame, R. Electromyographic temporal analysis of gait: Hemiplegic locomotion. Arch. Phys. Med. Rehabil. 1976, 57, 421–425. [Google Scholar] [PubMed]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function; Slack Incorporated: Thorofare, NJ, USA, 2010; pp. 152–153. [Google Scholar]
- Kalilani, L.; Asgharnejad, M.; Palokangas, T.; Durgin, T. Comparing the Incidence of Falls/Fractures in Parkinson’s Disease Patients in the US Population. PLoS ONE 2016, 11, e0161689. [Google Scholar] [CrossRef] [PubMed]
- Oppewal, A.; Hilgenkamp, T.I.M.; Wijck, R.; Evenhuis, H.M. Feasibility and outcomes of the berg balance scale in older adults with intellectual disabilities. Res. Dev. Disabil. 2013, 34, 2743–2752. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.A.; Miller, W.C.; Eng, J.J. Effect of stroke on fall rate, location and predictors: A prospective comparison of older adults with and without stroke. PLoS ONE 2011, 6, e19431. [Google Scholar] [CrossRef] [PubMed]
- Burnfield, J.M.; Few, C.D.; Mohamed, O.S.; Perry, J. The influence of walking speed and footwear on plantar pressures in older adults. Clin. Biomech. 2004, 19, 78–84. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Cukowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in parkinson’s disease and huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar]
- Martins, M.; Frizera, A.; Santos, C.; Ceres, R. Assistive mobility devices focusing on smart walkers: Classification and review. Robot. Auton. Syst. 2012, 60, 548–562. [Google Scholar] [CrossRef]
- Bradley, S.; Hernandez, C. Geriatric assistive devices. Am. Fam. Phys. 2011, 84, 405–411. [Google Scholar]
- Kay, B.S.; Hugh, C.M. How to use a walker correctly. Nursing 1998, 28, 32–33. [Google Scholar]
- Aikaterini, P.; Tianjian, J. Frequency & velocity of people walking. Struct. Eng. 2005, 83, 36–40. [Google Scholar]
- Bateni, H.; Heung, E.; Zettel, J.; McLlroy, W.E.; Maki, B.E. Can use of walkers or canes impede lateral compensatory stepping movements? Gait Posture 2004, 20, 74–83. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Muir, S.W.; Berg, K.; Chesworth, B.; Speechley, M. Use of the berg balance scale for predicting multiple falls in community-dwelling elderly people: A prospective study. Phys. Ther. J. 2008, 88, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Kwong, P.W.; Ng, S.S.; Liu, T.W.; Chung, R.C.; Ng, G.Y. Effect of leg selection on the berg balance scale Scores of hemiparetic stroke survivors: A cross-sectional study. Arch. Phys. Med. Rehabil. 2016, 97, 545–551. [Google Scholar] [CrossRef]
- Mohammed, S.; Samé, A.; Oukhellou, L.; Kong, K.; Huo, W.; Amirat, Y. Recognition of gait cycle phases using wearable sensors. Robot. Auton. Syst. 2016, 75, 50–59. [Google Scholar] [CrossRef]
- Pai, Y.C.; Yang, F.; Bhatt, T.; Wang, E. Learning from laboratory-induced falling: Long-term motor retention among older adults. Age 2014, 36, 9640. [Google Scholar] [CrossRef]
- McCrum, C.; Epro, G.; Meijer, K.; Zijlstra, W.; Brüggemann, G.P.; Karamanidis, K. Locomotor stability and adaptation during perturbed walking across the adult female lifespan. J. Biomech. 2016, 49, 1244–1247. [Google Scholar] [CrossRef]
- Fast, A.; Wang, F.S.; Adrezin, R.S.; Cordaro, M.A.; Ramis, J.; Sosner, J. The instrumented walker: Usage patterns and forces. Arch. Phys. Med. Rehabil. 1995, 76, 484–491. [Google Scholar] [CrossRef]
- Deschamps, K.; Eerdekens, M.; Desmet, D.; Matricali, G.A.; Wuite, S.; Staes, F. Estimation of foot joint kinetics in three and four segment foot models using an existing proportionality scheme: Application in paediatric barefoot walking. J. Biomech. 2017, 61, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, P.B.; MacWilliams, A.; Davis, R.B.; D’Astous, J.L. A multi-segment foot model based on anatomically registered technical coordinate systems: Method repeatability and sensitivity in pediatric planovalgus feet. Gait Posture 2013, 37, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Bruening, D.A.; Cooney, K.M.; Buczek, F.L. Analysis of a kinetic multi-segment foot model part II: Kinetics and clinical implications. Gait Posture 2012, 35, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.Y.; Yeh, P.C. Vertical force and wrist deviation angle in a sample of elderly people using walkers. Percept. Mot. Skills 2013, 116, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Alwan, M.; Wasson, G.; Sheth, P.; Ledoux, A.; Huang, C. Passive derivation of basic walker-assisted gait characteristics from measured forces and moments. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004. [Google Scholar]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. J. Am. Med. Assoc. 2011, 305, 50–58. [Google Scholar] [CrossRef]
- Callisaya, M.; Blizzard, L.; Schmidt, M.; McGinley, J.; Srikanth, V.K. Sex modifies the relationship between age and gait: A population-based study of older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L.B.; Johnson, R.B.; Turner, L.A. Research Methods, Design, and Analysis, 12th ed.; Pearson Education: Harlow, UK, 2013; pp. 36–39. [Google Scholar]
- Nishdia, Y.; Kitamura, K.; Yamamoto, H.; Takahashi, Y.; Mizoguchi, H. Living function resilient service using a mock living lab and real living labs: Development of balcony-IoT and handrail-IoT for healthcare. Procedia Comput. Sci. 2017, 113, 121–129. [Google Scholar] [CrossRef]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in Stroke Rehabilitation: A Systematic Review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]
- Gay, L.R.; Mills, G.E.; Airasian, P. Educational Research Competencies for Analysis and Application, 10th ed.; Pearson: Boston, MA, USA, 2012; pp. 203–226. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Step/Berg | M (SD) | SS | df | MS | F | Effect Size | Post hoc |
|---|---|---|---|---|---|---|---|---|
| Two steps | ||||||||
| Stance phases | 1 | 2.92 (1.05) | 1.04 | 1 | 1.04 | 0.83 | 0.01 | - |
| 2 | 3.11 (1.18) | |||||||
| Swing phases | 1 | 2.01 (0.84) | 0.00 | 1 | 0.00 | 0.00 | 0.00 | - |
| 2 | 2.01 (0.78) | |||||||
| Support force | 1 | 137.01 (68.49) | 937.44 | 1 | 937.44 | 0.20 | 0.00 | - |
| 2 | 142.60 (68.97) | |||||||
| Berg group | ||||||||
| Stance phases | H | 3.54 (0.51) | 100.60 | 2 | 50.30 | 123.78* | 0.68 | H, M > L |
| M | 3.73 (0.81) | |||||||
| L | 2.08 (0.73) | |||||||
| Swing phases | H | 1.28 (0.42) | 37.94 | 2 | 18.97 | 54.41* | 0.48 | H < M > L |
| M | 2.64 (0.60) | |||||||
| L | 2.08 (0.72) | |||||||
| Support force | H | 189.14 (67.89) | 159,826.81 | 2 | 79913.40 | 23.46* | 0.29 | H > M > L |
| M | 127.62 (43.96) | |||||||
| L | 101.34 (61.41) | |||||||
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeh, P.-C. Use of Reaction Force to Evaluate Older Adults’ Gait Patterns While Using a Walker to Walk. Geriatrics 2019, 4, 43. https://doi.org/10.3390/geriatrics4030043
Yeh P-C. Use of Reaction Force to Evaluate Older Adults’ Gait Patterns While Using a Walker to Walk. Geriatrics. 2019; 4(3):43. https://doi.org/10.3390/geriatrics4030043
Chicago/Turabian StyleYeh, Po-Chan. 2019. "Use of Reaction Force to Evaluate Older Adults’ Gait Patterns While Using a Walker to Walk" Geriatrics 4, no. 3: 43. https://doi.org/10.3390/geriatrics4030043
APA StyleYeh, P.-C. (2019). Use of Reaction Force to Evaluate Older Adults’ Gait Patterns While Using a Walker to Walk. Geriatrics, 4(3), 43. https://doi.org/10.3390/geriatrics4030043