Pilot of a Charter to Improve Management of Medicines and Oral Care for Residents with Dysphagia in Care Homes

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Charter and Related Website Development
2.2. Feasibility Testing
2.3. Feasibilty (Pilot) Methods
3. Results
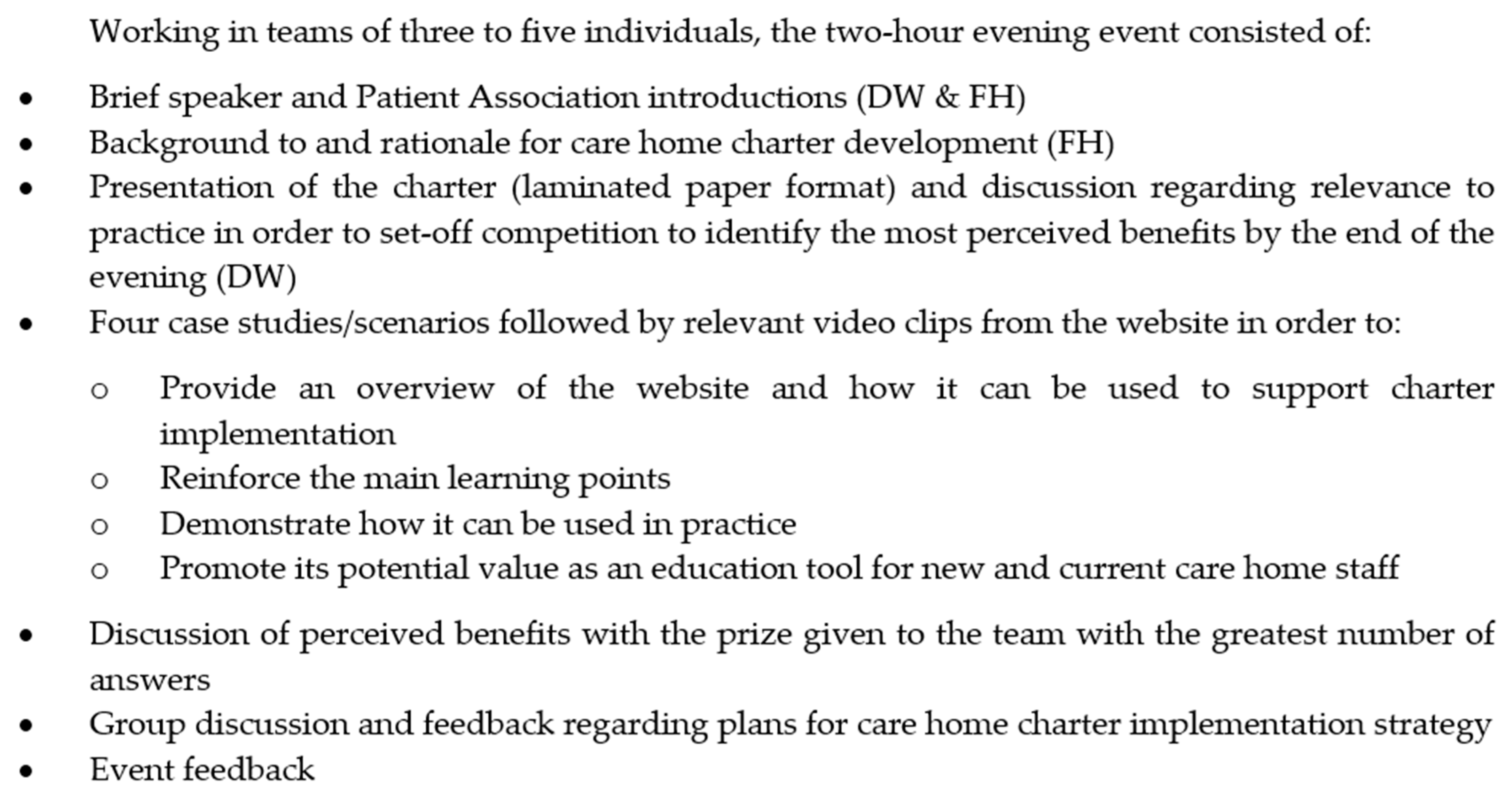
3.1. Launch and Training Event
3.2. Pilot Implementation Feedback (3 Months Post-Implementation)
3.3. Pilot Impact Feedback (Six Months Post-Implementation)
‘This training has been useful. It has made me more aware of how important it is that I involve the multidisciplinary team before making the covert medication decision.’ (Senior Cargiver)‘Very useful information for daily working.’ (Senior Cargiver)‘Being able to identify residents with swallowing difficulties and making referrals to the SALT [Speech and Language Therapist] has ensured safe administration of medication to people with swallowing difficulties.’ (Junior Caregiver)One junior caregiver conversely explained how they were ‘not sure about the charter, as has not been introduced to that but, I am confident in all of the above [confidence statements]’.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Office for National Statistics. 2011 Census Data; Office for National Statistics: London, UK, 2011. [Google Scholar]
- British Geriatrics Society. Guidance on Commissioning and Providing Healthcare Services across the UK; British Geriatrics Society: London, UK, 2016. [Google Scholar]
- Barber, N.D.; Alldred, D.P.; Raynor, D.K.; Dickinson, R.; Garfield, S.; Jesson, B.; Lim, R.; Savage, I.; Standage, C.; Buckle, P.; et al. Care homes’ use of medicines study: Prevalence, causes and potential harm of medication errors in care homes for older people. Qual. Saf. Health Care 2009, 18, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.; Johnston, S.; Mathie, E.; Baron, N.; Machen, I.; Amador, S.; Goodman, C. Potentially inappropriate prescribing in older people with dementia in care homes: A retrospective analysis. Drugs Aging 2012, 29, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.M.; Hughes, C.M.; Crealey, G.; Cardwell, C.; Lapane, K.L. An evaluation of an adapted U.S. model of pharmaceutical care to improve psychoactive prescribing for nursing home residents in Northern Ireland (fleetwood Northern Ireland study). J. Am. Geriatr. Soc. 2010, 58, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Thompson Coon, J.; Abbott, R.; Rogers, M.; Whear, R.; Pearson, S.; Lang, I.; Cartmell, N.; Stein, K. Interventions to reduce inappropriate prescribing of antipsychotic medications in people with dementia resident in care homes: A systematic review. J. Am. Med. Dir. Assoc. 2014, 15, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Carey, I.M.; Harris, T.; DeWilde, S.; Cook, D.G. Quality of prescribing in care homes and the community in england and wales. Br. J. Gen. Pract. J. R. Coll. Gen. Pr. 2012, 62, e329–e336. [Google Scholar] [CrossRef] [PubMed]
- Alldred, D.P.; Kennedy, M.C.; Hughes, C.; Chen, T.F.; Miller, P. Interventions to optimise prescribing for older people in care homes. Cochrane Database Syst. Rev. 2016, 2, CD009095. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.S.; Stokes, J.A.; King, M.A.; Lynne, T.A.; Purdie, D.M.; Glasziou, P.P.; Wilson, D.A.; McCarthy, S.T.; Brooks, G.E.; de Looze, F.J.; et al. Outcomes of a randomized controlled trial of a clinical pharmacy intervention in 52 nursing homes. Br. J. Clin. Pharmacol. 2001, 51, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Engle, R.L.; Tyler, D.A.; Gormley, K.E.; Afable, M.K.; Curyto, K.; Adjognon, O.L.; Parker, V.A.; Sullivan, J.L. Identifying barriers to culture change: A qualitative analysis of the obstacles to delivering resident-centered care. Psychol. Serv. 2017, 14, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Scalzi, C.C.; Evans, L.K.; Barstow, A.; Hostvedt, K. Barriers and enablers to changing organizational culture in nursing homes. Nurs. Adm. Q. 2006, 30, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Dibelius, O.; Petzold, C. “We need a new philosophy in the care of elderly people!” Findings about the implementation of the “charter of rights for people needing care and nursing” in senior and nursing homes. Pflege Z. 2007, 60, 564–567. [Google Scholar] [PubMed]
- Namasivayam, A.M.; Steele, C.M. Malnutrition and dysphagia in long-term care: A systematic review. J. Nutr. Gerontol. Geriatr. 2015, 34, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.F.; Altman, K.W. Causes of dysphagia among different age groups: A systematic review of the literature. Otolaryngol. Clin. N. Am. 2013, 46, 965–987. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.H.; Lin, W.C.; Hsu, Y.F.; Lee, I.H.; Hung, Y.C. One-year risk of pneumonia and mortality in patients with poststroke dysphagia: A nationwide population-based study. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2018, 27, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Langmore, S.E.; Skarupski, K.A.; Park, P.S.; Fries, B.E. Predictors of aspiration pneumonia in nursing home residents. Dysphagia 2002, 17, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Hollaar, V.R.Y.; van der Putten, G.J.; van der Maarel-Wierink, C.D.; Bronkhorst, E.M.; de Swart, B.J.M.; de Baat, C.; Creugers, N.H.J. Nursing home-acquired pneumonia, dysphagia and associated diseases in nursing home residents: A retrospective, cross-sectional study. Geriatr. Nurs. 2017, 38, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Popman, A.; Richter, M.; Allen, J.; Wham, C. High nutrition risk is associated with higher risk of dysphagia in advanced age adults newly admitted to hospital. Nutr. Diet. J. Diet. Assoc. Aust. 2018, 75, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Crary, M.A.; Humphrey, J.L.; Carnaby-Mann, G.; Sambandam, R.; Miller, L.; Silliman, S. Dysphagia, nutrition, and hydration in ischemic stroke patients at admission and discharge from acute care. Dysphagia 2013, 28, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Speyer, R.; Kertscher, B.; Denman, D.; Swan, K.; Cordier, R. Health-related quality of life and oropharyngeal dysphagia: A systematic review. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef] [PubMed]
- Seedat, J.; Penn, C. Implementing oral care to reduce aspiration pneumonia amongst patients with dysphagia in a south african setting. S. Afr. J. Commun. Disord. 2016, 63, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dyck, D.; Bertone, M.; Knutson, K.; Campbell, A. Improving oral care practice in long-term care. Can. Nurse 2012, 108, 20–24. [Google Scholar] [PubMed]
- National Institute for Health and Care Excellence. Guidance NG34; Oral Health for Adults in Care Homes; National Institute for Health and Care Excellence: London, UK, 2016. [Google Scholar]
- Kwok, C.; McIntyre, A.; Janzen, S.; Mays, R.; Teasell, R. Oral care post stroke: A scoping review. J. Oral Rehabil. 2015, 42, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Durgude, Y.; Cocks, N. Nurses’ knowledge of the provision of oral care for patients with dysphagia. Br. J. Community Nurs. 2011, 16, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Miarons Font, M.; Rofes Salsench, L. Antipsychotic medication and oropharyngeal dysphagia: Systematic review. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1332–1339. [Google Scholar] [CrossRef] [PubMed]
- Tiisanoja, A.; Syrjala, A.M.; Komulainen, K.; Lampela, P.; Hartikainen, S.; Taipale, H.; Knuuttila, M.; Ylostalo, P. Anticholinergic burden and dry mouth among finnish, community-dwelling older adults. Gerodontology 2018, 35, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Serrano Santos, J.M.; Poland, F.; Wright, D.; Longmore, T. Medicines administration for residents with dysphagia in care homes: A small scale observational study to improve practice. Int. J. Pharm. 2016, 512, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Fodil, M.; Nghiem, D.; Colas, M.; Bourry, S.; Poisson-Salomon, A.S.; Rezigue, H.; Trivalle, C. Assessment of clinical practices for crushing medication in geriatric units. J. Nutr. Health Aging 2017, 21, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Van Welie, S.; Wijma, L.; Beerden, T.; van Doormaal, J.; Taxis, K. Effect of warning symbols in combination with education on the frequency of erroneously crushing medication in nursing homes: An uncontrolled before and after study. BMJ Open 2016, 6, e012286. [Google Scholar] [CrossRef] [PubMed]
- Haw, C.; Stubbs, J. Covert administration of medication to older adults: A review of the literature and published studies. J. Psychiatr. Mental Health Nurs. 2010, 17, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Patients Association. Medicines Related Care of Residents with Dysphagia. Available online: https://www.patients-association.org.uk/blog/medicines-dysphagia-care-home-residents (accessed on 28 August 2018).
- National Institute for Health and Care Excellence. Managing Medicines in Care Homes. Nice Social Care Guideline 1; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Patients Association. Care Home Charter for Swallowing and Medicines. Available online: www.carehomecharter.org (accessed on 28 August 2018).
- Identifying Dysphagia in Residents in Care Homes. Available online: http://www.carehomecharter.org/identifying-dysphagia (accessed on 24 October 2018).
- Edwards, P.J.; Roberts, I.; Clarke, M.J.; Diguiseppi, C.; Wentz, R.; Kwan, I.; Cooper, R.; Felix, L.M.; Pratap, S. Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst. Rev. 2009, 3, Mr000008. [Google Scholar] [CrossRef] [PubMed]
- Care Quality Commission. Care Quality Commission: Independent Regulation of Health and Social Care in England. Available online: https://www.cqc.org.uk/ (accessed on 28 August 2018).



{kind=link}
{kind=link}
| Resident Charter | Care Home Worker Charter |
|---|---|
| When I am staying in a care home, I expect people responsible for my care to: | As a professional working in a care home I must have the requisite knowledge and skills to: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Question | Response | ||
|---|---|---|---|
| Junior Staff (%) | Senior Staff (%) | Resident/Relative (%) | |
| Copy of charter available to you (Senior n = 18. Junior n = 18) | 17 (94.4) | 16 (89.9) | |
| Did you access the website (Senior n = 17, Junior n = 17) | 16 (94.1) | 8 (47.1) | |
| Did you commit to the charter using the on-line quiz (Senior n = 15, Junior n = 15) | 7 (46.7) | 3 (20) | |
| Which of the following tools from the website have you used? | N = 16 | N = 8 | |
| Tips for embedding the charter in your home | 11 (68.8) | 5 (62.50 | |
| On-line course on Dysphagia: Swallowing difficulties and medicines | 7 (43.8) | 2 (25) | |
| Guidelines in practice | 11 (68.8) | 4 (50) | |
| Dysphagia identification checklist | 10 (62.5) | 5 (62.5) | |
| Care plan reminder template | 10 (62.5) | 3 (37.5) | |
| Audit checklist | 9 (56.3) | 5 (62.5) | |
| Which of the Resources from the website have you used? | N = 16 | N = 16 | |
| NHS advice on swallowing difficulties | 10 (62.5) | 6 (75.0) | |
| Learning advice on disabilities for people with swallowing difficulties | 7 (43.8) | 5 (62.5) | |
| NEWT guidelines for the administration of medication to patients with enteral feeding tubes or swallowing difficulties | 4 (25.0) | 1 (12.5) | |
| Swallowing difficulties website | 11 (68.8) | 6 (75.0) | |
| Prescribing decision support website | 6 (37.5) | 3 (37.5) | |
| Advanced decisions and general information | 7 (43.8) | 2 (25.0) | |
| General medicine-related support and advice | 8 (50.0) | 4 (50.0) | |
| Overall usefulness of the charter within the role | N = 17 | N = 15 | N = 7 |
| Very negative effect | 0 | 0 | |
| Negative effect | 0 | 0 | |
| No effect | 5.9 | 0 | |
| Useful | 58.8 | 66.7 | |
| Very useful | 35.3 | 33.3 | |
| Overall usefulness of the charter in improving the quality of care for residents (%): | N = 17 | N = 15 | N = 7 |
| Very negative effect | 0 | 0 | 0 |
| Negative effect | 0 | 0 | 0 |
| No effect | 0 | 50.0 | 50.0 |
| Useful | 80.0 | 33.3 | 33.3 |
| Very useful | 20.0 | 16.7 | 16.7 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morris, J.E.; Hollwey, F.; Hansjee, D.; Power, R.A.; Griffith, R.; Longmore, T.; Smithard, D.G.; Dann-Reed, E.; Wright, D.J. Pilot of a Charter to Improve Management of Medicines and Oral Care for Residents with Dysphagia in Care Homes. Geriatrics 2018, 3, 78. https://doi.org/10.3390/geriatrics3040078
Morris JE, Hollwey F, Hansjee D, Power RA, Griffith R, Longmore T, Smithard DG, Dann-Reed E, Wright DJ. Pilot of a Charter to Improve Management of Medicines and Oral Care for Residents with Dysphagia in Care Homes. Geriatrics. 2018; 3(4):78. https://doi.org/10.3390/geriatrics3040078
Chicago/Turabian StyleMorris, Jacqueline E., Frances Hollwey, Dharinee Hansjee, Rachel A. Power, Richard Griffith, Timothy Longmore, David G. Smithard, Eleanor Dann-Reed, and David J. Wright. 2018. "Pilot of a Charter to Improve Management of Medicines and Oral Care for Residents with Dysphagia in Care Homes" Geriatrics 3, no. 4: 78. https://doi.org/10.3390/geriatrics3040078
APA StyleMorris, J. E., Hollwey, F., Hansjee, D., Power, R. A., Griffith, R., Longmore, T., Smithard, D. G., Dann-Reed, E., & Wright, D. J. (2018). Pilot of a Charter to Improve Management of Medicines and Oral Care for Residents with Dysphagia in Care Homes. Geriatrics, 3(4), 78. https://doi.org/10.3390/geriatrics3040078