The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Operational Definitions
2.2. Search Strategy and Inclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Critical Appraisal
3. Results
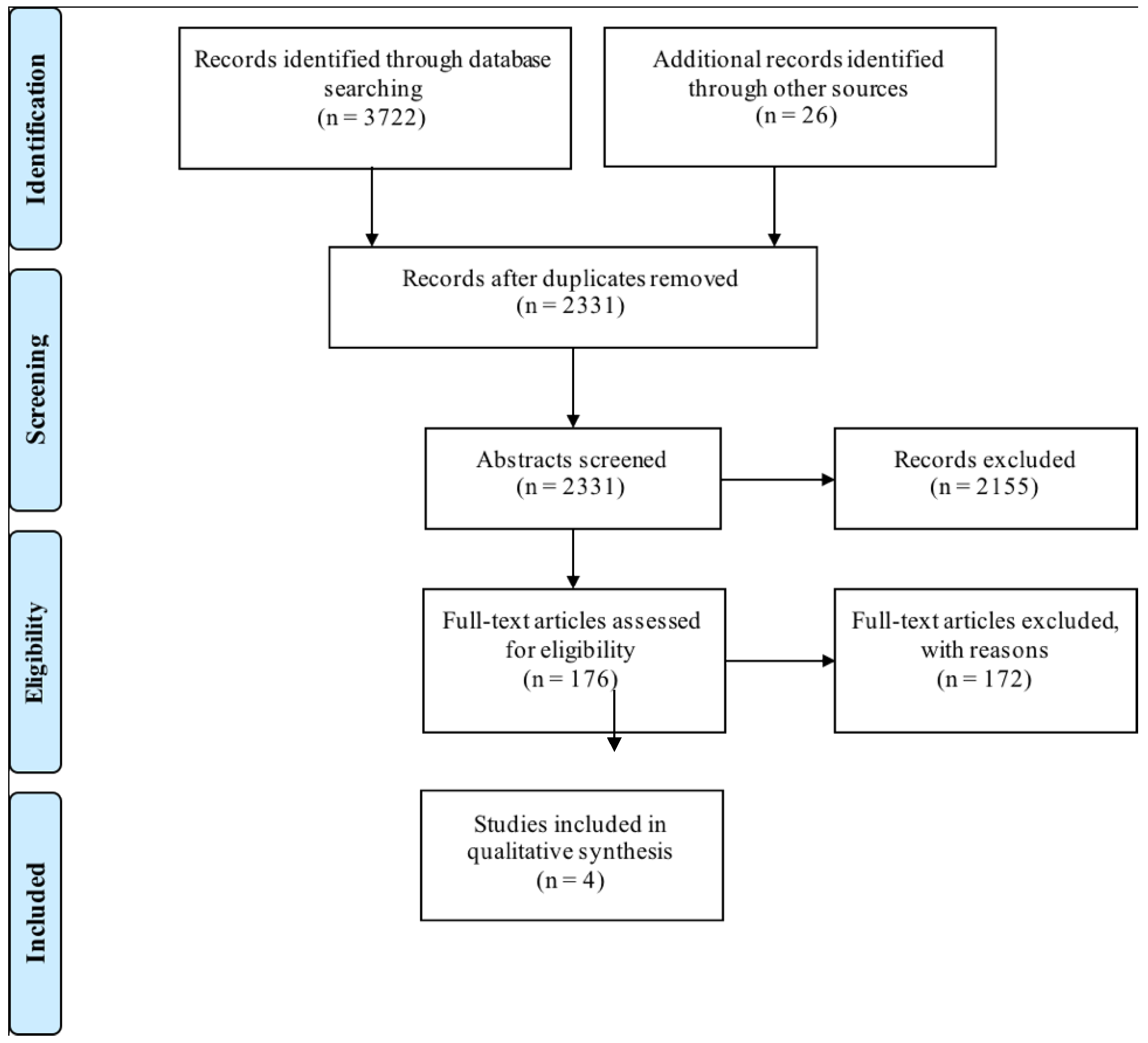
3.1. Literature Retrieval
3.2. Study Characteristics
3.3. Methodological Quality
3.4. Main Findings
4. Discussion
4.1. Limitations of the Systematic Review
4.2. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Search Number | Search Terms |
|---|---|
| 1 | Caregivers/ |
| 2 | (caregiving or “care giving” or caregiver* or care giver* or carer or carers).tw,kw. |
| 3 | 1 or 2 |
| 4 | exp aged/or “aged, 80 and over”/or frail elderly/ |
| 5 | Geriatrics/ |
| 6 | (geriatri* or gerontol* or elder? or elderly or senior* or senescen* or septuagenarian* or octogenarian* or nonagenarian*).tw,kw. |
| 7 | ((old* or aged*) adj2 (adult* or people or patient* or person* or women or men or individual*)).tw,kw. |
| 8 | or/4-7 |
| 9 | 3 and 8 |
| 10 | exp Deglutition Disorders/ |
| 11 | Deglutition/ |
| 12 | dysphagi*.tw,kw. |
| 13 | deglut*.tw,kw |
| 14 | swallow*.tw,kw. |
| 15 | or/10–14 |
| 16 | Nutrition disorders/ |
| 17 | exp Malnutrition/ |
| 18 | Nutritional physiological phenomena/ |
| 19 | Nutritional Status/ |
| 20 | exp Nutrition Therapy/ |
| 21 | Feeding Behavior/ |
| 22 | exp Diet/ |
| 23 | exp Eating/ |
| 24 | exp Food Habits/ |
| 25 | nutrition*.tw,kw. |
| 26 | malnutrition*.tw,kw. |
| 27 | malnourish*.tw,kw. |
| 28 | (meal* or dinning or dinner*1 or supper*1 or lunch*2 or breakfast*1).tw,kw. |
| 29 | (eat or eating).tw,kw. |
| 30 | (feed or feeding).tw,kw. |
| 31 | (drink*1 or drinking).tw,kw. |
| 32 | or/16–31 |
| 33 | Feeding Methods/ |
| 34 | Enteral Nutrition/ |
| 35 | exp Parenteral Nutrition/ |
| 36 | ((enteral or parenteral) adj2 (feed* or nutrition*)).tw,kw. |
| 37 | ((force or tube or intravenous) adj2 feed*).tw,kw. |
| 38 | or/33–37 |
| 39 | 9 and 15 |
| 40 | 9 and 32 |
| 41 | 9 and 38 |
| 42 | Elder Nutritional Physiological Phenomena/ |
| 43 | 3 and 42 |
| 44 | 39 or 40 or 41 or 43 |
| 45 | 44 not (exp animals/not exp humans/) |
| 46 | limit 45 to English language |
References
- Ney, D.M.; Weiss, J.M.; Kind, A.J.; Robbins, J. Senescent swallowing: Impact, strategies, and interventions. Nutr. Clin. Pract. 2009, 24, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Baijens, L.W.; Clave, P.; Cras, P.; Ekberg, O.; Forster, A.; Kolb, G.F.; Leners, J.-C.; Masiero, S.; Mateos-Nozal, J.; Ortega, O.; et al. European society for swallowing disorders—European Union geriatric medicine society white paper: Oropharyngeal dysphagia as a geriatric syndrome. Clin. Interv. Aging 2016, 11, 1403–1428. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.A.; Krishnaswami, S.; Steger, E.; Conover, E.; Vaezi, M.F.; Ciucci, M.R.; Francis, D.O. Economic and survival burden of dysphagia among inpatients in the United States. Dis. Esophagus 2018, 31, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Altman, K.W.; Yu, G.P.; Schaefer, S.D. Consequence of dysphagia in the hospitalized patient: Impact on prognosis and hospital resources. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Crary, M.A.; Humphrey, J.L.; Carnaby-Mann, G.; Sambandam, R.; Miller, L.; Silliman, S. Dysphagia, nutrition, and hydration in ischemic stroke patients at admission and discharge from acute care. Dysphagia 2013, 28, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Shune, S.E.; Karnell, L.H.; Karnell, M.P.; Van Daele, D.J.; Funk, G.F. Association between severity of dysphagia and survival in patients with head and neck cancer. Head Neck 2012, 34, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Namasivayam-MacDonald, A.M.; Morrison, J.M.; Steele, C.M.; Keller, H. How swallow pressures and dysphagia affect malnutrition and mealtime outcomes in long-term care. Dysphagia 2017, 32, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Karvonen-Gutierrez, C.A.; Robis, D.L.; Fowler, K.E.; Terrell, J.E.; Gruber, S.B.; Duffy, S.A. Quality of life scores predict survival among patients with head and neck cancer. J. Clin. Oncol. 2008, 26, 2754–2760. [Google Scholar] [CrossRef] [PubMed]
- Klinke, M.E.; Wilson, M.E.; Hafsteinsdottir, T.B.; Jonsdottir, H. Recognizing new perspectives in eating difficulties following stroke: A concept analysis. Disabil. Rehabil. 2013, 35, 1491–1500. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Frank, C.; Moltz, C.; Vos, P.; Smith, H.; Karlsson, U.; Dutta, S.; Midyett, A.; Barloon, J.; Sallah, S. Impact of dysphagia on quality of life after treatment of head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Rolland, J.S. Families, Illness, & Disability; BasicBooks: New York, NY, USA, 1994. [Google Scholar]
- Johansson, A.E.M.; Johansson, U. Relatives’ experiences of family members’ eating difficulties. Scand. J. Occup. Ther. 2009, 16, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Nund, R.L.; Ward, E.C.; Scarinci, N.A.; Cartmill, B.; Kuipers, P.; Porceddu, S.V. Carers’ experiences of dysphagia in people treated for head and neck cancer—A qualitative study. Dysphagia 2014, 29, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Nund, R.L.; Scarinci, N.A.; Cartmill, B.; Ward, E.C.; Kuipers, P.; Porceddu, S.V. Third-party disability in carers of people with dysphagia following non-surgical management for head and neck cancer. Disabil. Rehabil. 2016, 38, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.M.; Rapley, T.; Carding, P.N.; Wilson, J.A.; McColl, E. Head and neck cancer and dysphagia; caring for carers. Psychooncology 2013, 22, 1815–1820. [Google Scholar] [CrossRef] [PubMed]
- Penner, J.L.; McClement, S.; Lobchuk, M.; Daeninck, P. Family members’ experiences caring for patients with advanced head and neck cancer receiving tube feeding: A descriptive phenomenological study. J. Pain Symptom Manag. 2012, 44, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Nund, R.L.; Scarinci, N.A.; Cartmill, B.; Ward, E.C.; Kuipers, P.; Porceddu, S.V. Application of the international classification of functioning, disability and health (ICF) to people with dysphagia following non-surgical head and neck cancer management. Dysphagia 2014, 29, 692–703. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Manton, K.G.; Land, K.C. Active life expectancy estimates for the U.S. Elderly population: A multidimensional continuous-mixture model of functional change applied to completed cohorts, 1982–1996. Demography 2000, 37, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Spillman, B.C.; Freedman, V.A.; Kasper, J.D. A national profile of family and unpaid caregivers who assist older adults with health care activities. JAMA Intern. Med. 2016, 176, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Gibson, M.J.; Houser, A. Valuing the Invaluable: A New Look at the Economic Value of Family Caregiving; Issue Brief; Public Policy Institute (American Association of Retired Persons): San Francisco, CA, USA, 2007; Volume IB82, pp. 1–12. [Google Scholar]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Zarit, S.H.; Todd, P.A.; Zarit, J.M. Subjective burden of husbands and wives as caregivers: A longitudinal study. Gerontol. 1986, 26, 260–266. [Google Scholar] [CrossRef]
- Torti, F.M.J.; Gwyther, L.P.; Reed, S.D.; Friedman, J.Y.; Schulman, K.A. A multinational review of recent trends and reports in dementia caregiver burden. Alzheimer Dis. Assoc. Disord. 2004, 18, 99–109. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Goodkind, D.; Kowal, P. An Aging World: 2015; United States Census Bureau: Washington, DC, USA, 2016. [Google Scholar]
- O’Connor, D.; Green, S.; Higgins, J. Defining the review question and developing criteria for including studies. In Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; Cochrane Collaboration: London, UK, 2008; pp. 81–94. [Google Scholar]
- Daniels, S.K.; Corey, D.M.; Hadskey, L.D.; Legendre, C.; Priestly, D.H.; Rosenbek, J.; Foundas, A.L. Mechanism of sequential swallowing during straw drinking in health young and older adults. J. Speech Lang. Hear. Res. 2004, 47, 33–45. [Google Scholar] [CrossRef]
- Hiss, S.G.; Treole, K.; Stuart, A. Effects of age, gender, bolus volume, and trial on swallowing apnea duration and swallow/respiratory phase relationships of normal adults. Dysphagia 2001, 16, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Stephen, J.R.; Taves, D.H.; Smith, R.C.; Martin, R.E. Bolus location at the initiation of the pharyngeal stage of swallowing in healthy older adults. Dysphagia 2005, 20, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Tracy, J.F.; Logemann, J.A.; Kahrilas, P.J.; Jacob, P.; Kobara, M.; Krugler, C. Preliminary observations on the effects of age on oropharyngeal deglutition. Dysphagia 1989, 4, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers using meta-aggregation. Int. J. Evid.-Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Bentur, N.; Sternberg, S.; Shuldiner, J.; Dwolatzky, T. Feeding tubes for older people with advanced dementia living in the community in Israel. Am. J. Alzheimers Dis. Demen. 2015, 30, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Choi-Kwon, S.; Kim, H.-S.; Kwon, S.U.; Kim, J.S. Factors affecting the burden on caregivers of stroke survivors in South Korea. Arch. Phys. Med. Rehabil. 2005, 86, 1043–1048. [Google Scholar] [CrossRef] [PubMed]
- Habermann, B.; Shin, J.Y. Preferences and concerns for care needs in advanced Parkinson’s disease: A qualitative study of couples. J. Clin. Nurs. 2017, 26, 1650–1656. [Google Scholar] [CrossRef] [PubMed]
- Riviere, S.; Gillette-Guyonnet, S.; Andrieu, S.; Nourhashemi, F.; Lauque, S.; Cantet, C.; Salva, A.; Frisoni, G.; Vellas, B. Cognitive function and caregiver burden: Predictive factors for eating behaviour disorders in Alzheimer’s disease. J. Geriatr. Psychiatry 2002, 17, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Blandford, G.; Watkins, L.B.; Mulvihil, M.N. Assessing abnormal feeding behaviour in dementia: A taxonomy and initial findings. In Weight Loss and Eating Behaviour in Alzheimer’s Patients: Research and Practice in Alzheimer’s Disease; Vellas, B., Riviere, S., Fitten, J., Eds.; SERDI: Paris, France, 1998; pp. 49–66. [Google Scholar]
- Vernooij-Dassen, M.J.; Persoon, J.M.; Felling, A.J. Predictors of sense of competence in caregivers of demented persons. Soc. Sci. Med. 1996, 43, 41–49. [Google Scholar] [CrossRef]
- Arslan, S.S.; Demir, N.; Karaduman, A.A. The anxiety level of caregivers of neurological patients with dysphagia. Dysphagia 2017, 32, 570–574. [Google Scholar] [CrossRef] [PubMed]
- High, D.M. All in the family: Extended autonomy and expectations in surrogate health care decision-making. Gerontol. 1988, 28, 46–51. [Google Scholar] [CrossRef]
- Wolff, J.L.; Kasper, J.D. Caregiving of frail elders: Updating a national profile. Gerontol. 2006, 46, 344–356. [Google Scholar] [CrossRef]
- Riley, L.D.; Bowen, C. The sandwich generation: Challenges and coping strategies of multigenerational families. Fam. J. Couns. Ther. Couples Fam. 2005, 13, 52–58. [Google Scholar] [CrossRef]
- Pinquart, M.; Sorensen, S. Spouses, adult children, and children-in-law as caregivers of older adults: A meta-analytic comparison. Psychol. Aging 2011, 26, 1. [Google Scholar] [CrossRef] [PubMed]
- Melgaard, D.; Rodrigo-Domingo, M.; Mørch, M. The prevalence of oropharyngeal dysphagia in acute geriatric patients. Geriatrics 2018, 3, 15. [Google Scholar] [CrossRef]


| Study | Design | Study Aim(s) | N (CG/CR Dyads) | Mean Age of CRs (years) a | Mean Age of CGs (Years) a | Diagnosis of CRs | Relationship of CGs to CRs |
|---|---|---|---|---|---|---|---|
| Bentur, N., Sternberg, S., Shuldiner, J., & Dwolatzky, T. (2015) [34] | Cross-sectional | To examine the prevalence of feeding tube use among OPAD living in the community in Israel. To describe the demographic, social, and medical characteristics of OPAD and to compare feeding tube users and nonusers. To describe the quality of care of OPAD and the burden of care on their caregivers, and to compare feeding tube users and nonusers. | 117 | 86.5 (7.7) | 61.7 (12.5) | Advanced dementia | 74% children, 22% spouses |
| Choi-Kwon, S., Kim, H-S, Kwon, S. U., & Kim, J. S. (2005) [35] | Cross-sectional | To identify the factors related to caregiver burden in chronic stroke survivors in Seoul, Korea. | 154 | 61.9 (8.1) b | 54.5 (13.1) | Chronic ischemic stroke | 70% spouses, 14% children, 14% daughters-in-law |
| Habermann, B., & Shin, J. Y. (2017) [36] | Qualitative | To explore the needs, concerns, and preferences of couples with advanced PD in the United States of America as they plan the care needed for the future. | 14 | 73.31 (9.3) | 72.13 (8.8) | Advanced Parkinson’s disease | 100% partner or spouse |
| Riviere, S., Gillette-Guyonette, S., Andrieu, S., Nourhashemi, F., Lauque, S., Cantet, C., Salva, A., Frisoni, G., & Vellas, B. (2002) [37] | Cohort | To investigate predictors of aversive feeding behaviors which occurred during a one-year interval among AD patients living at home with a caregiver in France, Spain and Italy. | 193 | 76 (8.1) | 61.1 (13.4) and 62.5 (12.5)—study divided CGs into 2 groups | Alzheimer’s disease | 54% spouses, 35% another relative |
| Joanna Briggs Guidelines | Bentur, N., Sternberg, S., Shuldiner, J., & Dwolatzky, T. (2015) [34] | Choi-Kwon, S., Kim, H-S, Kwon, S. U., & Kim, J. S. (2005) [35] |
|---|---|---|
| Were the criteria for inclusion in the sample clearly defined? | Yes | Yes |
| Were the study subjects and the setting described in detail? | Subjects—yes; setting—no | Subjects—yes; setting—no |
| Was the exposure measured in a valid and reliable way? | N/A | N/A |
| Were objective, standard criteria used for measurement of the condition? | Yes | Unclear |
| Were confounding factors identified? | Yes | Yes |
| Were strategies to deal with confounding factors stated? | Yes | Yes |
| Were the outcomes measured in a valid and reliable way? | No | No |
| Was appropriate statistical analysis used? | Yes | Yes |
| Joanna Briggs Guidelines | Riviere, S., Gillette-Guyonette, S., Andrieu, S., Nourhashemi, F., Lauque, S., Cantet, C., Salva, A., Frisoni, G., & Vellas, B. (2002) [37] |
|---|---|
| Were the two groups similar and recruited from the same population? | Yes |
| Were the exposures measured similarly to assign people to both exposed and unexposed groups? | N/A |
| Was the exposure measured in a valid and reliable way? | Yes |
| Were confounding factors identified? | No |
| Were strategies to deal with confounding factors stated? | No |
| Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? | N/A |
| Were the outcomes measured in a valid and reliable way? | Yes |
| Joanna Briggs Guidelines | Habermann, B., & Shin, J. Y. (2017) [36] |
|---|---|
| Is there congruity between the stated philosophical perspective and the research methodology? | Unclear |
| Is there congruity between the research methodology and the research question or objectives? | Yes |
| Is there congruity between the research methodology and the methods used to collect data? | Yes |
| Is there congruity between the research methodology and the representation and analysis of data? | Yes |
| Is there congruity between the research methodology and the interpretation of results? | Yes |
| Is there a statement locating the researcher culturally or theoretically? | No |
| Is the influence of the researcher on the research, and vice-versa, addressed? | No |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namasivayam-MacDonald, A.M.; Shune, S.E. The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review. Geriatrics 2018, 3, 30. https://doi.org/10.3390/geriatrics3020030
Namasivayam-MacDonald AM, Shune SE. The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review. Geriatrics. 2018; 3(2):30. https://doi.org/10.3390/geriatrics3020030
Chicago/Turabian StyleNamasivayam-MacDonald, Ashwini M., and Samantha E. Shune. 2018. "The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review" Geriatrics 3, no. 2: 30. https://doi.org/10.3390/geriatrics3020030
APA StyleNamasivayam-MacDonald, A. M., & Shune, S. E. (2018). The Burden of Dysphagia on Family Caregivers of the Elderly: A Systematic Review. Geriatrics, 3(2), 30. https://doi.org/10.3390/geriatrics3020030